
Purpose
This study was conducted to investigate the moderating effect of physical activity on the relationship between perceived stress and depression in patients newly diagnosed with ischemic heart disease.
Methods: This study had a cross-sectional design. Data were collected using a structured self-report questionnaire, which covered demographic characteristics, perceived stress, depression, and physical activity. Multiple linear regression was used to determine whether perceived stress and physical activity influenced depression, after controlling for demographic characteristics. The moderating effect of physical activity on the relationship between perceived stress and depression was analyzed using model 1 of the PROCESS macro (bootstrap sample size=5,000).
Results: The findings revealed that the level of depression was higher in women (p=.003), individuals without a spouse (p=.004), and those with an average monthly income of less than 3 million won (p=.045). The regression results showed that perceived stress was associated with a significant increase in the level of depression (β=.53, p<.001), and low physical activity was also a significant predictor of depression (β=.16, p=.013). The moderating effect of physical activity on the relationship between perceived stress and depression was confirmed, indicating that when physical activity was high, the impact of perceived stress on depression was weaker than when physical activity was low (B=-0.37, p=.038).
Conclusion: The findings suggest the need to implement a nursing program that can enhance physical activity and early screening for stress and depression in patients with ischemic heart disease.
This study was conducted to investigate the moderating effect of physical activity on the relationship between perceived stress and depression in patients newly diagnosed with ischemic heart disease.
This study had a cross-sectional design. Data were collected using a structured self-report questionnaire, which covered demographic characteristics, perceived stress, depression, and physical activity. Multiple linear regression was used to determine whether perceived stress and physical activity influenced depression, after controlling for demographic characteristics. The moderating effect of physical activity on the relationship between perceived stress and depression was analyzed using model 1 of the PROCESS macro (bootstrap sample size=5,000).
The findings revealed that the level of depression was higher in women (p=.003), individuals without a spouse (p=.004), and those with an average monthly income of less than 3 million won (p=.045). The regression results showed that perceived stress was associated with a significant increase in the level of depression (β=.53, p<.001), and low physical activity was also a significant predictor of depression (β=.16, p=.013). The moderating effect of physical activity on the relationship between perceived stress and depression was confirmed, indicating that when physical activity was high, the impact of perceived stress on depression was weaker than when physical activity was low (B=-0.37, p=.038).
The findings suggest the need to implement a nursing program that can enhance physical activity and early screening for stress and depression in patients with ischemic heart disease.
Ischemic Heart Disease (IHD) is a leading cause of death among chronic diseases [1]. In Korea, the mortality rate due to IHD has continued to increase, reaching 27.5 deaths per 100,000 individuals in 2021 [2]. This represents a 0.5% increase from the previous year. IHD is characterized by symptoms caused by atherosclerotic plaques in the coronary arteries, which can lead to coronary artery spasms and microvascular dysfunction [3]. Both physiological and psychological factors have been reported to exacerbate these causes [4].
The impact of psychological distress on IHD is widely acknowledged [4]. Stress and depression are key health concerns that not only are prevalent among patients with IHD, but also adversely affect its prognosis [5, 6, 7, 8]. The prevalence of depression is at least three times higher among individuals with IHD than among the general population [7], and these patients often exhibit inadequate self-management, harming their prognosis [8]. Perceived stress is considered a major negative factor that can trigger depression [8, 9], while Physical Activity (PA) is known to help alleviate depression [10]. Physically active adults have a lower risk of developing depression compared to individuals leading sedentary lifestyles [11], and PA has been shown to mitigate depressive symptoms [12, 13, 14].
As a strategy to improve health outcomes among patients with IHD, it is essential to develop interventions aimed at reducing depression by minimizing the impact of perceived stress. However, given the challenges associated with reducing stress in daily life, it is also important to investigate strategies that can mitigate the severity of depression even under stressful circumstances. Previous studies of patients with IHD have demonstrated a negative correlation of stress and depression with PA levels [15, 16].
Little research has investigated how PA moderates the association between perceived stress and depression in patients with IHD. Enhancing our understanding of how PA can regulate depression resulting from perceived stress in individuals with IHD can offer valuable evidence for the development of interventions centered on PA.
In this study, we aimed to investigate perceived stress and depression in patients newly diagnosed with IHD, as well as to explore the impact of perceived stress on depression and the regulatory effect of PA in this relationship. By doing so, we hope to provide foundational data for nursing interventions, highlighting the relevance of PA in managing stress and depression and in preventing IHD.
This correlational cross-sectional study was designed to explore the moderating effect of PA on the relationship between perceived stress and depression in patients with IHD.
This study included participants aged 19 years or older who had recently been diagnosed with IHD. These individuals were recruited from the cardiovascular center of a university hospital while hospitalized. A cardiologist, who agreed to assist in participant recruitment after learning about the purpose of the study, recommended that patients who met specific criteria participate in the research. These included individuals diagnosed with stenosis of 50% or more on coronary angiography, those undergoing percutaneous coronary intervention, and those who had confirmed positive results on the ergonovine provocation test for the initial diagnosis of IHD. Among the recommended participants, those who voluntarily agreed to participate were selected as the target population. The exclusion criteria included diagnosed depression and difficulties with cooperation due to mental illness or communication disorders.
The sample size was calculated using G*Power 3.1.9.2 (University of Dusseldorf, Dusseldorf, Germany). Based on a previous study [17], we gathered a total of 118 samples for a multiple regression analysis of the factors influencing depression in patients with IHD. We planned to include eight variables, which comprised both independent and control variables. A post hoc analysis established the effect size at 0.15, indicating a medium effect size, with five input variables. The significance level (α) was set at .05 and the power at .91.
Data for this study were collected between February 2020 and March 2021. The researcher visited patients' hospital rooms and administered a structured self-reported questionnaire. On average, the questionnaire took about 20 minutes to complete.
The researcher thoroughly explained the study's purpose, methodology, and content to the participants. Before participating, each individual provided written informed consent. Participants were made aware of their right to withdraw from the study or decline participation at any time. They were also assured that the data collected, including survey responses, would be used exclusively for research purposes. To determine the specific type of IHD (coronary artery spasm or coronary artery stenosis) for each participant, the researcher examined their electronic medical records.
Regarding general patient characteristics, seven items were surveyed: gender, age, religion, marital status, occupation, monthly income (either less than or more than 3 million won), and education level (either less than high school or college and above). Lifestyle habits included smoking and drinking, which were assessed based on whether the patient had never smoked or drank, had quit, or currently smokes or drinks. Disease-related characteristics included comorbidities and type of IHD. Comorbidities were evaluated by asking whether the patient had been diagnosed with diabetes or hypertension by a doctor and whether they had any other comorbidities. The type of IHD was classified as either coronary artery spasm or coronary artery stenosis.
To measure perceived stress, we utilized an open-source tool created by Lee et al. [18]. This tool was originally developed for the Stress Questionnaire of the Korean National Health and Nutrition Examination Survey, a scientific research project initiated by the Korea Centers for Disease Control and Prevention in 2010. As such, it was employed in this study without the need for a separate approval procedure. The version of the tool used in this study was a shortened one, comprising nine items selected from the original 20 [18]. The questionnaire examined the degree of perception of essential stress reactions, such as distress, anger, aggression, and tension. Responses were collected on a Likert scale ranging from 1 ("not at all") to 5 ("very much"). The scoring ranged from 9 to 45, with higher scores signifying greater levels of perceived stress. Based on a cutoff of 23 points, stress levels were categorized into high and low-stress groups [18]. In the study conducted by Lee et al. [18], Cronbach's α value was .91, while in this study, it was .88.
In this study, we utilized the Korean version of the Beck Depression Inventory, second edition (K-BDI-II), which was translated by Lee et al. [19] from the original Beck Depression Inventory developed by Beck in 1996. This open-access tool was directly purchased and used by the researcher. The K-BDI-II consists of 21 items, each reflecting major symptoms of depression such as sadness, guilt, suicidal ideation, and loss of pleasure. The scoring is based on a 4-point Likert scale, with the total score calculated by summing the scores of each item. Higher scores indicate higher levels of depression. The reliability of the tool has been reported to be high in previous research, with a Cronbach's α value of .89 in the studies of both Beck and Lee et al. [19]. In the present study, the Cronbach's α value was .88.
In this study, we utilized the Korean version of the International Physical Activity Questionnaire (IPAQ), a tool that facilitates international comparisons of PA [20]. The reliability and validity of the Korean version of the IPAQ were previously validated by Oh et al. [21]. The survey included questions about regular exercise, types of exercise, and the dates and times of vigorous exercise, moderate-intensity PA, and walking for a minimum of 10 minutes, all within the past week. The energy requirements for each type of activity were defined in Metabolic Equivalents (METs), and PA was quantified in MET-min/week.
PA levels were originally classified into three categories: active, minimally active, and inactive, based on the amount of PA performed [16]. However, for this study, we utilized two levels. The high-activity group consisted of individuals who engaged in high-intensity activities at least 3 days a week, achieving 1,500 MET-min/week of activity, or those who participated in a combination of PAs totaling at least 3,000 MET-min/week over a 7-day period. The low-activity group includes those classified as minimally active and inactive, which includes individuals who engage in activities that are below the level of activity required for the high-activity group. We applied weights based on the IPAQ guidelines.
This study received approval from the institutional review board of a university hospital in S city, with which the researcher is affiliated (approval number: 1911-163-1082).
The study was conducted in a way that safeguarded the privacy of the participants, ensuring the confidentiality of their personal information. It was explicitly stated that the data collected would be used exclusively for research purposes. Participants were given the freedom to withdraw their consent at any time without repercussions. Moreover, the collected data would be preserved for 3 years and then deleted, as specified in the consent form.
The collected data were analyzed using SPSS 23.0 (IBM Corp., Armonk, NY, USA). The general characteristics, lifestyle habits, disease-related characteristics, perceived stress, and PA level of the participants were analyzed using descriptive statistics. Differences in depression according to independent variables were analyzed using the independent t-test and one-way analysis of variance. Relationships involving perceived stress and depression were assessed using Pearson correlations. Multiple linear regression was conducted, with variables that exhibited significant relationships with depression considered as independent variables. Due to the non-normal distribution of METs in this study, PA was classified as a categorical variable and analyzed as either high or low. The moderating effect of PA on the relationship between perceived stress and depression was analyzed using model 1 of the PROCESS macro (bootstrap sample size=5,000).
Out of the 118 participants, 68 (57.6%) were under the age of 65 years, and 92 (78.0%) were male. Additionally, 95 participants (80.5%) had a spouse, and 68 participants (57.6%) had attained a high school education or less. In terms of employment, 89 participants (75.4%) were employed. Regarding religious beliefs, 69 participants (58.5%) did not follow any religion. Finally, 69 participants (58.5%) reported a monthly income of 3 million Korean won or more.
Of the individuals surveyed, 56 (47.5%) reported that they had quit smoking, while 24 (20.3%) indicated that they were current smokers. Regarding alcohol consumption, 60 (50.8%) of the respondents confirmed that they were current drinkers, and 34 (28.8%) stated that they had quit drinking.
The comorbidities present included diabetes in 24 patients (20.3%) and hypertension in 55 patients (46.6%). Among all patients, 102 (86.4%) had two or fewer comorbidities. In total, regarding the type of IHD, 58 patients (49.2%) had coronary artery spasms, while 60 patients (50.8%) had coronary artery stenosis. PA levels were high in 31 patients (26.3%) and low in 87 patients (73.7%). Perceived stress levels were low in 80 participants (67.8%) and high in 38 participants (32.2%).
The level of depression was found to be higher in women (15.77±6.68) compared to men (11.21±6.85) (t=3.01, p=.003) and in individuals without a spouse (15.98±8.37) compared to those with a spouse (11.31±6.41) (t=-2.95, p=.004). Individuals with a monthly income of ≥3 million won exhibited lower depression levels (11.12±7.07) than those earning <3 million won (13.76±6.78) (t=2.03, p=.045). While the level of depression was higher in the low-activity group (12.89±7.21) than in the high-activity group (10.32±6.30), this difference was not statistically significant (t=1.76, p=.081). A significant difference in depression levels was observed based on the perceived stress level (t=5.38, p<.001) (Table 1).
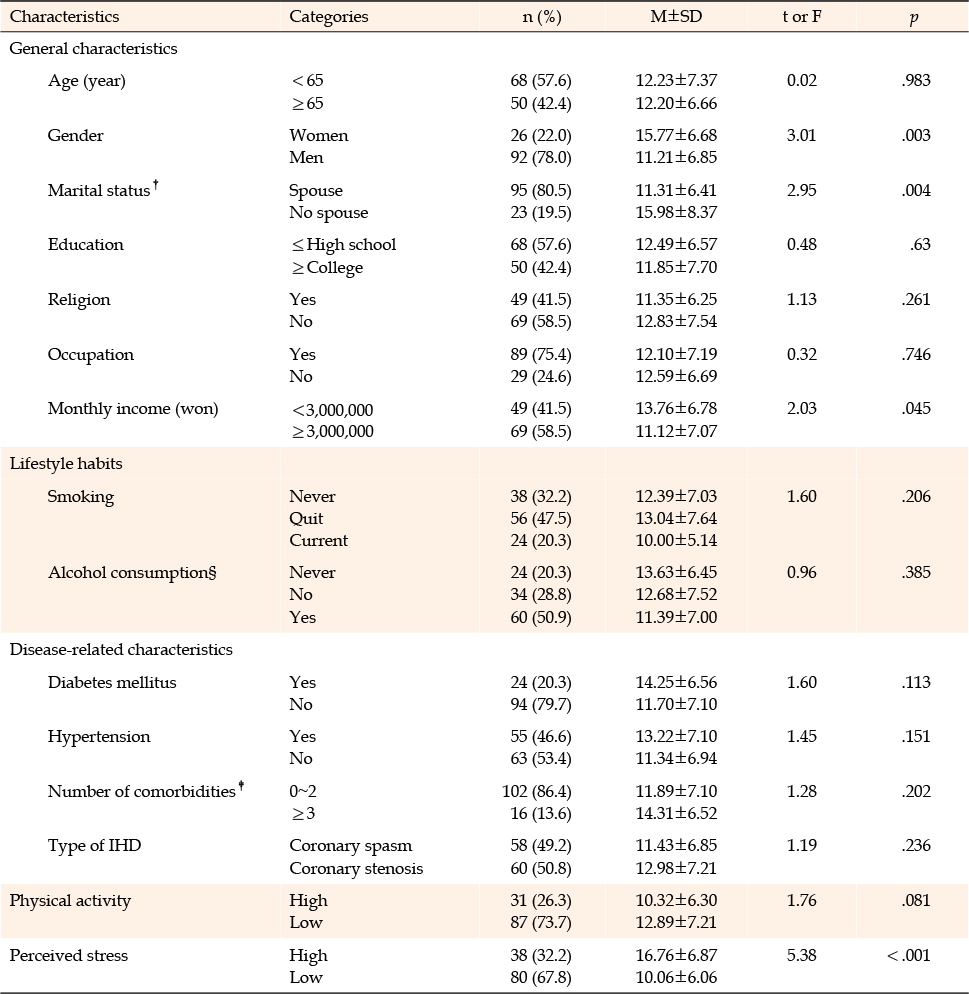
Table 1
Depression According to General Characteristics, Lifestyle Habits, and Disease-related Characteristics (N=118)
The data revealed a positive correlation between perceived stress and depression (r=.57, p<.001). To evaluate the potential impact of perceived stress, a linear regression analysis was conducted. The Durbin-Watson value of 2.06 confirmed the absence of autocorrelation among the independent variables. Furthermore, depression, serving as the dependent variable, met the assumption of normality. The tolerance limits, which ranged from 0.90 to 0.97, and the variance inflation factor, which ranged from 1.05 to 1.12, indicated the absence of multicollinearity.
After adjusting for factors such as gender, marital status, and monthly income, the regression analysis assessed the impact of perceived stress and PA level on depression. The regression model yielded significant results (F=20.52, p<.001), suggesting that the model was a strong fit for the data. This model explained 35.7% of the variation in depression. Consequently, we found that perceived stress was associated with a significant increase in depression levels (β=.53, p<.001), and low PA was also a significant predictor of depression (β=.16, p=.013) (Table 2).
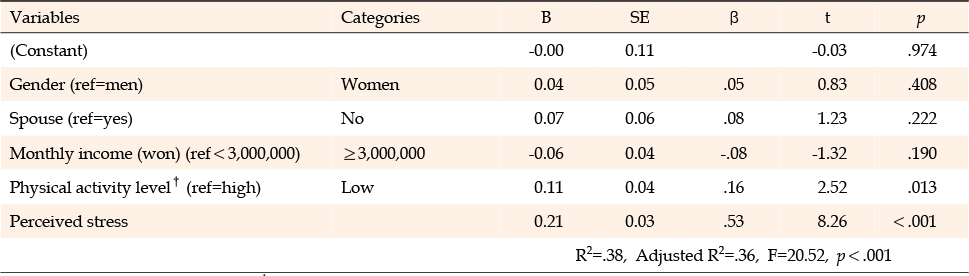
Table 2
Impact of Perceived Stress on Depression (N=118)
To confirm the moderating effect of PA on the relationship between perceived stress and depression, we conducted an analysis using model 1 of the PROCESS macro (Table 3). The F-value, which signifies the goodness of fit of the analysis model, was significant at 9.28 (p=.001). The explanatory power was 33, and the R2 value shifted to 0.03 (F=4.42, p=.038) after the inclusion of the interaction term. This interaction term (B=-0.37, p=.038) was statistically significant, indicating that PA moderates the relationship between perceived stress and depression (Table 3).

Table 3
Moderating Effect of Physical Activity on the Relationship between Perceived Stress and Depression (N=118)
The positive relationship between perceived stress and depression was significantly decreased when the level of PA was high, thus confirming the moderating effect of PA. This was evident as the slope of the high-activity group was less steep than that of the low-activity group, as shown in Figure 1. In other words, the strong positive correlation between perceived stress and depression could be mitigated by a high PA level. Therefore, the increase in depression in response to stress exhibited a varying pattern based on the level of PA.
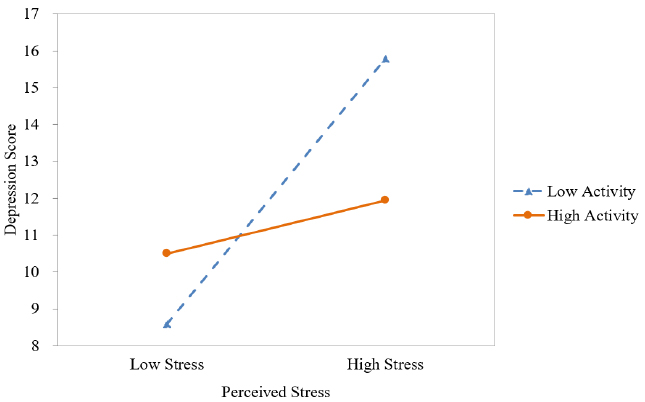
Figure 1
Moderating effect of physical activity on the relationship between perceived stress and depression score.
In this study, we explored the impact of perceived stress on depression in patients newly diagnosed with IHD, and we examined whether PA levels had a moderating effect on this relationship. We found that women exhibited higher levels of depression than men. This observation aligns with a prior study [22] that also reported elevated depression levels in women with IHD. Given the detrimental effect of depression on the prognosis of IHD [23], it is particularly important to closely monitor depression in women patients, who may exhibit especially pronounced symptoms of depression.
After controlling for gender, marital status, and monthly income, perceived stress was found to significantly affect depression levels. This finding aligns with the outcomes of prior research [9, 24, 25]. Moreover, the observation that individuals who endure higher levels of stress also experience more severe depression [26] corroborates these results. This underscores the importance of identifying and addressing the stress experienced by patients with IHD.
Upon analyzing the moderating effect of PA level on the relationship between perceived stress and depression, we found that higher levels of PA could help alleviate the impact of perceived stress on depression. This analysis aligns with previous research [12], concurrently illustrating that even under heightened stress conditions, PA can lessen the severity of depression.
It is well-established that depression tends to increase as stress levels rise [27]. However, this finding that PA can potentially modulate the relationship between stress and depression is highly meaningful. This suggests that engaging in active PA can help mitigate the strong negative impact of stress on depression. These results align with previous studies showing that PA can be as effective as pharmacotherapy in reducing depression [10] and can enhance resilience to stress [28]. As a result, these findings highlight the importance of intervention programs designed to minimize negative responses to perceived stress in patients with IHD, thereby reducing depression. Therefore, it is crucial for nurses to emphasize the importance of regularly engaging in moderate-to-high-intensity PA for patients with IHD.
However, in this study, exercise intensity was classified based on METs, and factors such as exercise preference or the type of exercise were not considered. Therefore, given that the moderating effects of stress and depressive symptoms may vary between aerobic and resistance exercises, it is crucial to conduct separate studies to investigate the different types and intensities of PA [29].
This study has a few limitations that should be considered. First, the use of convenience sampling from a single university hospital in Seoul may restrict the generalizability of the findings. Second, despite the measurement of PA in METs, the broad spectrum of activities posed a challenge for analysis as a continuous variable and for conducting an in-depth evaluation based on exercise intensity. These limitations may stem from the small sample size. Future studies should strive to expand the sample size to overcome these limitations.
This study revealed that perceived stress exacerbates depression, while PA moderates the relationship between perceived stress and depression. Therefore, it is crucial to underscore the importance of enhancing PA in patients with IHD. This will not only improve their physical health but also alleviate negative psychological symptoms.
Therefore, we recommend the development and implementation of PA programs specifically designed for patients with IHD, with the aim of effectively reducing negative emotions. This can be accomplished by conducting systematic reviews or experimental studies to pinpoint the specific types and methods of PA that can lessen negative emotions. This will enable the provision of personalized intervention strategies for each patient.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - YY-H and LSJ.
Data collection - YY-H.
Analysis and interpretation of the data - YY-H and LSJ.
Drafting and critical revision of the manuscript - YY-H and LSJ.
This article is a revision of the first author's master's thesis from Chung-Ang University.
 E-SUBMISSION
E-SUBMISSION