
Purpose
This study identified the mediating effect of resilience on the relationship between job stress and the professional quality of life of hospice and palliative care nurses.
Methods
The participants included 136 hospice and palliative care nurses from 13 inpatient hospice and palliative care wards at a tertiary hospital in a metropolitan city in South Korea. Data were collected from February 2022 to March 2022. Hayes' PROCESS macro 3.5 was used to test the significance of the parameter's indirect effects. Professional quality of life was divided into three subdomains: compassion satisfaction, secondary traumatic stress, and burnout.
Results
As a mediator, resilience had both direct and indirect effects on the relationship between job stress and the compassion satisfaction of hospice and palliative care nurses. Furthermore, there were both direct and indirect effects on the relationship between job stress and secondary traumatic stress. Finally, although there was no direct effect on the relationship between job stress and burnout, there was an indirect mediating effect.
Conclusion
This study confirmed the direct effect of compassion satisfaction on job stress and the professional quality of life of hospice and palliative care nurses, as well as the mediating effect of resilience on job stress and burnout. To improve the professional quality of life of hospice and palliative care nurses, it is necessary to develop and apply programs that enhance resilience in order to promote its mediating effects on compassion satisfaction and burnout.
This study identified the mediating effect of resilience on the relationship between job stress and the professional quality of life of hospice and palliative care nurses.
The participants included 136 hospice and palliative care nurses from 13 inpatient hospice and palliative care wards at a tertiary hospital in a metropolitan city in South Korea. Data were collected from February 2022 to March 2022. Hayes' PROCESS macro 3.5 was used to test the significance of the parameter's indirect effects. Professional quality of life was divided into three subdomains: compassion satisfaction, secondary traumatic stress, and burnout.
As a mediator, resilience had both direct and indirect effects on the relationship between job stress and the compassion satisfaction of hospice and palliative care nurses. Furthermore, there were both direct and indirect effects on the relationship between job stress and secondary traumatic stress. Finally, although there was no direct effect on the relationship between job stress and burnout, there was an indirect mediating effect.
This study confirmed the direct effect of compassion satisfaction on job stress and the professional quality of life of hospice and palliative care nurses, as well as the mediating effect of resilience on job stress and burnout. To improve the professional quality of life of hospice and palliative care nurses, it is necessary to develop and apply programs that enhance resilience in order to promote its mediating effects on compassion satisfaction and burnout.
Hospice and palliative care refer to professional medical care that improves the Quality of Life (QoL) of patients with terminal diseases by relieving their pain and physical, psychological, social, and spiritual suffering [1]. Beyond medical care that delays the death of the patient, hospice and palliative care actively work to relieve pain and uncomfortable symptoms and address the patient's psychological, social, and spiritual needs [2]. Hospice and palliative care nurses provide integrated holistic care to improve QoL for terminally ill patients who may fear the physical changes of their illness as well as death. In addition, hospice and palliative care nurses provide direct care to patients and play an important role as team coordinators [3].
Job stress refers to the discomfort, pressure, and tension felt by employees due to working conditions, including the work environment, job complexity, workload, workplace conflict, role ambiguity, job instability, and an irrational and authoritarian organizational culture [4]. Nurses experience job stress during the nursing process. For hospice and palliative care nurses, major stressors include a lack of confidence in the pain management of patients with terminal cancer, time pressures, difficulty delivering bad news, and end-of-life care [5].
Job stress affects an organization by negatively impacting workers' physical or mental health and increasing turnover [6]. As caregivers of dying patients, hospice and palliative care nurses can experience a decline in their Professional QoL (ProQOL) due to physical and emotional exhaustion [7]. Thus, hospice and palliative care nurses require both physical and mental measures to relieve stress.
ProQOL is a subjective assessment of the QoL of people in professions that provide services to a target population, particularly how they experience their jobs [8]. Compassion fatigue can also be described as burnout and secondary traumatic stress. Thus, ProQOL is comprised of three aspects: compassion satisfaction, burnout, and secondary traumatic stress [8]. Compassion fatigue is experienced as a loss of motivation, indifference toward patients, and inability to cope. However, compassion satisfaction moderates compassion fatigue and enables nurses to continue caring for patients [9, 10]. As a highly sensitive group, hospice and palliative care nurses can experience compassion fatigue because they internalize anger, anxiety, fear, and sadness, much like the patients and their caregivers going through the pain, terminal symptoms, and eventual dying process [11]. Thus, a supportive environment in which hospice and palliative care nurses can perform their work is required to maintain a positive mindset and reduce compassion fatigue.
Nurses play an important role in hospice and palliative care as members of multidisciplinary teams. They participate in various programs for pain management, symptom control, end-of-life care, and bereavement care to improve the QoL of patients [12]. The pressure experienced by hospice and palliative care nurses depends on the difficulty of the care required (i.e., this varies with the type of cancer or disease), mental exhaustion, conflict with the hospice team [8], and the high stress of delays during end-of-life care [13]. As the symptoms of hospice patients worsen, their physical and psychological demands increase, and their families experience various degrees of death anxiety [14]. The high levels of stress experienced by hospice and palliative care nurses differ from those experienced by general ward nurses [15], as they are expected to take on emotionally stressful tasks [16].
In previous studies, oncology nurses with high resilience reported low burnout and job stress, high job satisfaction, and a strong ability to cope [17]. Resilience is the ability to adapt to situations and overcome adversity [18] and can help nurses perform well in their jobs, thereby reducing the prevalence of post-traumatic stress and emotional burnout [19]. The higher the job satisfaction and the lower the job stress and burnout, the more influence nurses' resilience and ProQOL were shown to have on caregiving [20, 21].
Nursing care seeks to restore and promote the health of patients [22] by paying attention to patients' needs while providing care. Because a decline in the ProQOL of nurses can negatively impact patient care, enhancing the ProQOL of nurses is important [23]. Recent studies of the ProQOL of nurses in general, as care providers focused on their patients' health and recovery, showed that hospice and palliative care nurses have high levels of job stress and psychological burnout, because they are required to care for patients who are dying [15, 16]. However, to our knowledge, no study has identified the mediating effect of resilience, which can mitigate job stress and improve QoL, on the relationship between job stress and ProQOL in hospice and palliative care nurses. Thus, the present study aimed to confirm the mediating effect of resilience on the relationship between job stress and the ProQOL of hospice and palliative care nurses. This study can facilitate the creation of policies that improve ProQOL and strengthen the resilience of hospice and palliative care nurses.
To determine the degree of job stress, resilience, and ProQOL among hospice and palliative care nurses and explore the mediating effect of resilience on the relationship between job stress and ProQOL, we performed the following:
Examined the differences in job stress, resilience, and ProQOL based on demographic characteristics.
Assessed the degree of job stress, resilience, and ProQOL among hospice and palliative care nurses.
Identified correlations between job stress, resilience, and ProQOL.
Determined the mediating effect of resilience on the relationship between job stress and ProQOL.
This descriptive, multicenter, and cross-sectional study was performed from February 1, 2022, to March 20, 2022. Data was collected using a questionnaire.
The participants included hospice and palliative care nurses who worked across 13 inpatient hospice and palliative care Jeonbuk State, South Jeolla Province, North Chungcheong Province, South Chungcheong Province, Gwangju metropolitan city, Gyeonggi Province. province in South Korea for more than a year and oversaw nursing practice, education, and consultations for hospice patients.
Prior to data collection, the researchers obtained permission to use the measurement tools from the original developers via email and explained the purpose of the study to the department head of the hospital. Participation was voluntary and participants responded to the researcher's email and phone number disclosed in the recruitment announcement. The questionnaires were delivered to participants by email or post and were completed by the individual participants. The questionnaire took approximately 10~15 minutes to complete, and a small gift was provided to the participants.
The number of subjects was calculated using the G*Power 3.1 program (Heinrich-Heine-Universitat Dusseldorf, Dusseldorf, Germany) for multiple regression analysis, with a medium effect size of .15, significance level (α) of .05, power (1−β) of .85, and 10 independent variables. The calculated minimum sample size was 131 participants. After accounting for a 10% dropout rate [24], the total number of participants required was 146. Of the 146 questionnaires, 136 were analyzed after excluding 10 incomplete questionnaires.
Permission to use the Job Stress measurement tool was obtained from the original developer, Mi Ok Gu, via email. Permission to use the Resilience measurement tool was granted by the developer, Jonathan Davidson, via email on June 20, 2021, and permission for the ProQOL measurement tool was granted by the ProQOL office on the same date.
A tool developed by Kim et al. [25] to measure the work stress experienced by nurses in the clinical field was modified by Kang [26] to target hospice ward nurses. The tool comprised 43 questions in nine areas, which could be scored on a 6-point Likert scale (1 indicating "I do not feel it at all" and 6 indicating "I feel it strongly"). Higher scores were observed with higher stress levels. The reliability of the tool was shown by a Cronbach's α of .94, .94, and .95 in Kim et al. [25], Kang [26], and the present study, respectively.
To measure the degree of resilience in oncology nurses, the Korean Connor-Davidson Resilience Scale was developed by Connor and Davidson [27] and validated after translation by Baek [28]. The resilience tool included 25 questions across five dimensions, scored on a 5-point Likert scale (0 indicating "not at all" to 4 indicating "very much so"). High scores indicated high levels of resilience. The reliability of the tool was shown by a Cronbach's α of .89, .91, and .94 in Connor and Davidson [27], Baek [28], and the present study, respectively.
This study employed Korean version 5 of the ProQOL tool developed by Stamm [8]. It included 30 questions (10 questions across the three subdomains of compassion satisfaction, secondary traumatic stress, and burnout) scored on a 5-point Likert scale (1 indicating "not at all" to 5 indicating "very much so"). High scores indicated a high ProQOL. A score distribution of 10~50 points was possible in each subdomain, with higher scores indicating higher degrees of compassion satisfaction, secondary traumatic stress, and burnout as represented by an average value on a 5-point scale. According to Stamm's classification criteria [8], ≤22 points (22 points on a 5-point scale for 10 questions; ≤2.2 points by converting 22 points to the average value of the questions) was low, 23~41 points (10 questions, 5-point scale, item average value 2.3~4.1 points) was average, and ≥42 points (10 questions, 5-point scale, item average value ≥4.2 points) was high. According to Stamm [8], the tool reliabilities were shown by a Cronbach's α of .88, .81, and .75 for compassion satisfaction, secondary traumatic stress, and burnout, respectively. The corresponding values in this study were .93, .77, and .68, respectively.
This study obtained approval from the Institutional Bioethics Committee/Public Review Committee (IRB NO: P01-202112-21-017) of the Ministry of Health and Welfare. The participants completed a consent form after the purpose and methods of the study were explained and they were told that participation could be withdrawn at any time without penalties. Furthermore, it was explained that the collected data would not be used for any purpose other than research and that anonymity was guaranteed. The data were coded and managed to prevent personal identification and were stored in a password-protected file in a locked location to prevent leakage.
Data analysis was performed using SPSS version 23.0 (IBM Corp., Armonk, NY, USA). The general participant characteristics were analyzed using descriptive statistics. Job stress, resilience, and ProQOL were expressed as averages and standard deviations. Differences in general characteristics, job stress, resilience, and ProQOL were analyzed using the independent t-test and one-way analysis of variance, with the post hoc Scheffé test. The correlation between job stress, resilience, and ProQOL was calculated using Pearson correlation coefficients (p<.05, p<.001). This study was designed to confirm the Durbin-Watson value, which examines autocorrelation, under the basic assumptions that must be examined to confirm the mediating effect of resilience on the relationship between job stress and ProQOL. An analysis was performed with a mediation model (model 4) using SPSS PROCESS macro-3.5 to confirm the mediating effect. The statistical significance of the indirect effect was determined by performing 10,000 bias-adjusted bootstrapping tests at a 95% confidence interval (CI).
The general characteristics of the participants are listed in Table 1. Of the 146 questionnaires retrieved, 10 were incomplete, leaving 136 questionnaires to be analyzed.
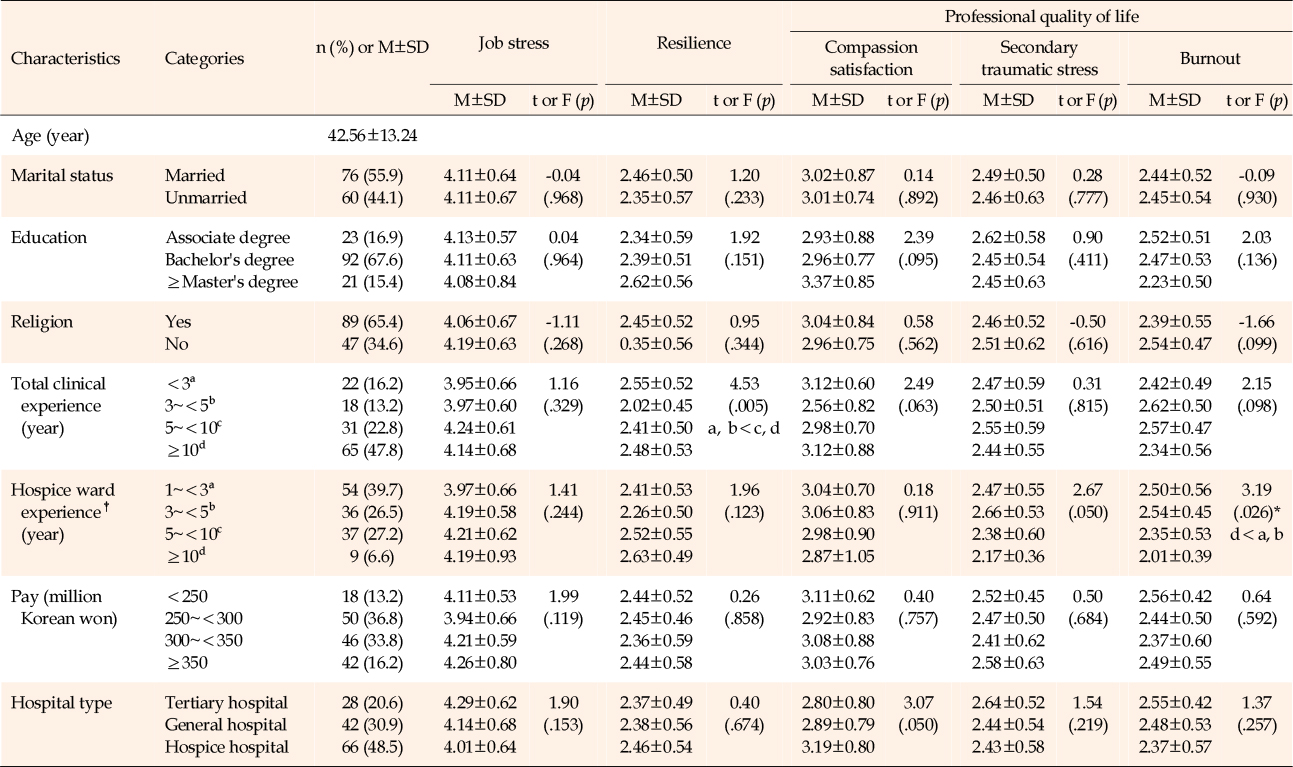
Table 1
Differences in Job Stress, Resilience, and Professional Quality of Life according to General Characteristics (N=136)
No statistically significant differences were observed in the general characteristics and job stress of the participants. A significant difference was observed in the resilience scores of nurses with different years of clinical experience (F=4.53, p=.005). The post hoc analysis revealed that nurses with 5–10 years or >10 years of clinical experience exhibited significantly higher resilience than those with <5 years of experience. Among the general characteristics and ProQOL of the participants, compassion satisfaction and secondary traumatic stress did not exhibit statistically significant differences. A significant difference (F=3.19, p=.026) in burnout was observed according to the years of experience in a hospice ward, and the post hoc analysis revealed that burnout was significantly higher for nurses with 1–3 and 3–5 years of experience than for nurses with ≥10 years of experience (Table 1).
The average job stress score in this study was 4.11±0.65 (out of 6 points), and the average resilience score was 2.41±2.41 (out of 4 points). Regarding ProQOL, compassion satisfaction scores averaged 3.02±0.08 (out of 5 points), secondary traumatic stress scores averaged 2.48±0.56 (out of 5 points), and burnout scores averaged 2.44±0.53 (out of 5 points) (Table 2).
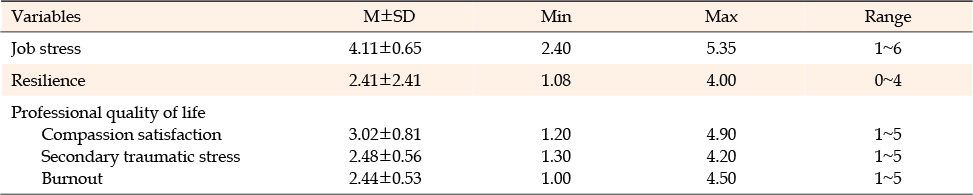
Table 2
Descriptive Statistics of Research Variables (N=136)†
Correlations between job stress, resilience, and ProQOL (compassion satisfaction, secondary traumatic stress, and burnout) were analyzed. Job stress was negatively correlated with resilience (r=−.18, p=.035) and compassion satisfaction (r=−.27, p=.002). Conversely, job stress was positively correlated with secondary traumatic stress (r=.26, p=.002) and burnout (r=.18, p=.036).
Resilience was positively correlated with compassion satisfaction (r=.46, p<.001). However, it was negatively correlated with secondary traumatic stress (r=−.23, p=.007) and burnout (r=-.14, p<.001). Compassion satisfaction was negatively correlated with secondary traumatic stress (r=−.04, p=.358) and exhaustion (r=−.37, p<.001). A positive correlation was observed between secondary traumatic stress and burnout (r=.56, p<.001) (Table 3).
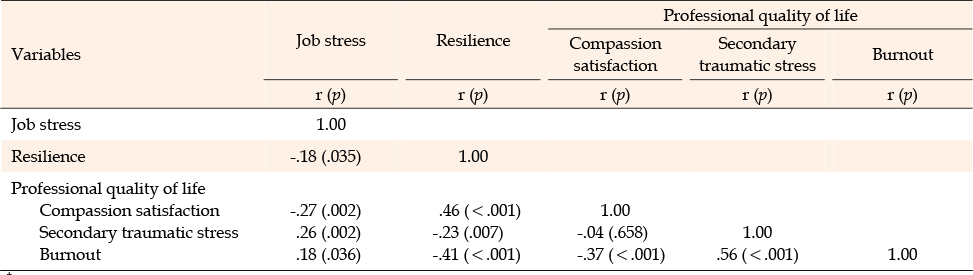
Table 3
Correlations among Research Variables (N=136)†
The regression analysis of compassion satisfaction, a dependent variable, revealed a Durbin-Watson value of 1.92. The Durbin-Watson value of secondary traumatic stress was 1.91, therefore dependent. For the regression analysis of hospice ward experience, 1~3 years was treated as a dummy variable to control for significant differences in burnout; the Durbin-Watson value was 1.09 (close to 2) and, therefore, dependent. The variables were independent, without autocorrelation. Multicollinearity was investigated, and the tolerance limit range was 0.87~0.97 (<1.0). The variance inflation index range was 1.03~1.09 (<10); therefore, the problem of multicollinearity was not observed. Normality was examined using a p-p plot, and the points were confirmed to be close to a 45° straight line, indicating a normal distribution of the error term. The standardized residual scatterplot confirmed the homoscedasticity of the residuals, as they were irregularly distributed without any trend or cycle centered at the mean of 0 (Table 4).
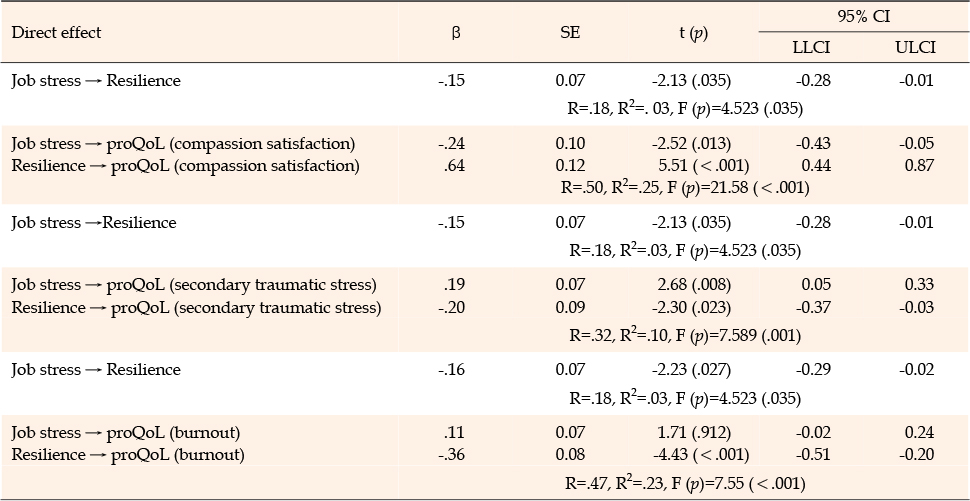
Table 4
Mediating Effects of Resilience on the Relationship between Job Stress and Professional Quality of Life (N=136)†
An analysis was conducted using the PROCESS macro model 4.0 (Table 4) to examine the mediating effect of resilience on the relationship between job stress and compassion satisfaction in hospice nurses. The independent variable, job stress, had a significant negative effect on the mediating variable, resilience (β=−.15, p=.035). Job stress (β=−.24, p=.013) and resilience (β=.64, p<.001) exerted a positive effect on the dependent variable, compassion satisfaction. The explanatory power was 25% (Table 4).
The total effect of the relationship between job stress and compassion satisfaction was −.33 (95% CI, −0.60 to −0.13), and the direct effect was −.24 (95% CI, −0.43 to −0.15). It was statistically significant with a bootstrapped CI of −0.43 to −0.15. The indirect effect of job stress on compassion satisfaction mediated by resilience was −.10, with a bootstrapped CI of −0.20 to −0.01, indicating a statistically significant mediating effect (Table 5).
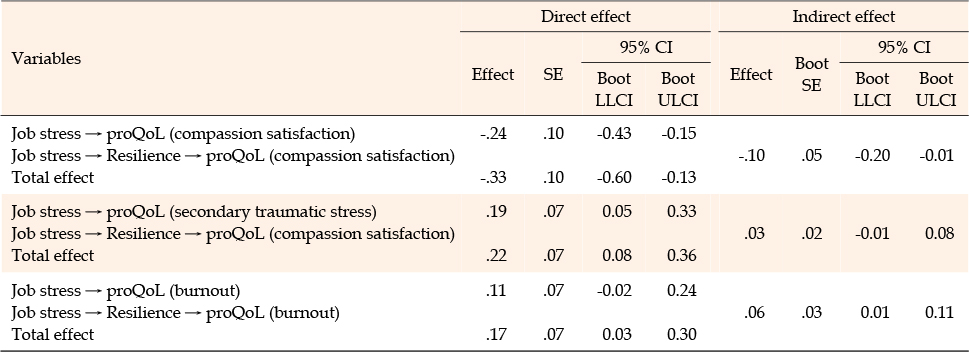
Table 5
Significance Test of the Mediation of Professional Quality of Life (N=136)
Job stress had a significant negative effect on resilience (β=−15, p=.035). Furthermore, job stress (β=.19, p=.008) and resilience (β=−.20, p=.023) had a negative effect on secondary traumatic stress, with an explanatory power of 10% (Table 4).
The total effect of the relationship between job stress and secondary traumatic stress was .22 (95% CI, 0.08~0.36), and the direct effect of job stress on secondary traumatic stress was .19 (95% CI, 0.05~0.33). Both were statistically significant as the CIs did not include zero. The indirect effect of job stress on secondary traumatic stress through resilience was not statistically significant at .03 (95% CI, −0.01~0.08), as the interval included zero (Table 5).
The analysis revealed that job stress had a significant negative effect on resilience (β=−.16, p=.027). The independent variable, job stress (β=.11, p=.912), was not significant for the dependent variable, burnout. The mediator, resilience (β=−.36, p<.001), had a negative effect on the dependent variable, burnout, with an explanatory power of 23% (Table 4).
The total effect of resilience on the relationship between job stress and burnout among hospice nurses was .17, with a bootstrapped CI of 0.03 to 0.30, which was statistically significant. The direct effect of resilience on job stress and burnout was .11, with a bootstrapped CI of −0.02 to 0.24, which was not statistically significant. The statistically significant mediating effect of resilience on job stress and burnout was .06, with a bootstrapped CI of 0.01 to 0.11 (Table 5).
This study determined the mediating effect of resilience on the relationship between job stress and ProQOL among hospice and palliative care nurses. In the three aspects of ProQOL, compassion satisfaction averaged 3.02±0.08 points, secondary traumatic stress averaged 2.48±0.56 points, and burnout averaged 2.44±0.53 points. A study of nurses working with COVID-19 patients, using the same instrument [29], found a score of 3.22 for compassion satisfaction, 2.72 for secondary traumatic stress, and 2.89 for burnout, much like the present results. Nurses experience physical and emotional exhaustion while serving as caregivers of dying patients, causing a deteriorating ProQOL [7]. Furthermore, nurses can experience high levels of stress due to the difficulties of caring for different types of cancer. This can lead to feeling overwhelmed and experiencing mental burnout, emotional distress [12], and delays in end-of-life care-related tasks [13]. To improve the ProQOL of hospice and palliative care nurses who care for patients facing death, measures should be taken to increase compassion satisfaction, as well as reduce the levels of burnout and secondary traumatic stress by identifying their causes.
In this study, differences in resilience were observed according to the nurses' years of clinical experience. A similar study observed that nurses with over 7 years of clinical experience exhibited higher resilience than nurses with 1~4 years of clinical experience [30]. It was found that skilled clinical experience can help nurses overcome difficult situations and successfully adapt, and that resilience can also be improved through education [31]. Thus, educational programs that improve resilience should be developed.
When considering the differences in ProQOL according to the participants' general characteristics, burnout was significantly different based on hospice ward experience. In post hoc analysis, burnout was significantly higher among those with 1~3 and 3~5 years of hospice unit experience than those with 10+ years of experience. A similar study found that burnout varied by the length of time caring for patients with COVID-19 [29]. Since shorter work experience showed higher rates of burnout, a burnout management intervention program tailored to work experience should be introduced. Furthermore, to improve ProQOL by increasing compassion satisfaction and reducing burnout, hospice nurses should also be empowered to choose the hospice ward they work on.
Job stress was negatively related to resilience and compassion satisfaction, and positively related to secondary traumatic stress and burnout. Resilience was positively related to compassion satisfaction, and negatively related to secondary traumatic stress and burnout.
Regarding ProQOL, compassion satisfaction was negatively associated with secondary traumatic stress and burnout, and positively associated with resilience. This differs from previous studies that examined the relationship between resilience and ProQOL in healthcare workers, where resilience had a statistically significant association with all three subscales of ProQOL [32]. A study of generalist nurses [33] also found that higher resilience was associated with lower burnout. The likely reason for this variation in findings was that these studies did not include hospice and palliative care nurses. Applying a stress reduction program that actively manages job stress and enhances resilience may help hospice and palliative care nurses view the last days of their patients' lives positively and enhance their ability to provide quality care to dying patients.
This study found a direct effect of job stress on compassion satisfaction in hospice and palliative care nurses, and an indirect mediation effect through resilience. Although resilience had no mediating effect on job stress and secondary traumatic stress, resilience did have a mediating effect on job stress and burnout. Direct comparisons were difficult to achieve because only a few studies investigated the same research subjects, research variables, and relationships to be confirmed as the present study. However, the mediating effect of resilience in our study did reveal results like those in a study of patients with multiple sclerosis, which found the moderating effect of resilience on depression and health-related QoL [34]. In a separate study involving patients on hemodialysis, the findings mirrored the mediation effect of resilience on the relationship between symptom experience and QoL [35]. Resilience is the ability to use adversity and difficulties as a springboard to leap forward [18]; the application of resilience-building programs can be an effective alternative to improve ProQOL. This study was significant because it showed the relationship between hospice and palliative care nurses' job stress and compassion satisfaction, a subdomain of ProQOL. The direct effect of job stress on compassion satisfaction was confirmed, as well as the indirect effect of resilience on burnout. Therefore, it is necessary to improve resilience to improve the ProQOL of hospice and palliative care nurses. This study showed that resilience had no mediating effect on the relationship between job stress and secondary traumatic stress in hospice and palliative care nurses. Therefore, repeated studies are needed to validate this result. Based on this study, the active development and application of resilience enhancement programs are needed to improve the ProQOL of hospice and palliative care nurses. Hospice and palliative care nurses should not feel that they are expected to sacrifice for their patients as part of their profession. Resilience-building programs that include psychological support must be applied to enable them to provide the holistic and individualized care that dying patients need and allow them to view dying more comfortably.
This study is significant since it was conducted among nurses who care for hospice patients nationwide. Moreover, it identified resilience as an important variable for reducing job stress in hospice and palliative care nurses to improve their ProQOL. Based on this study, we made the following recommendations. First, in an era where healthcare providers are increasingly aware of providing a comfortable death rather than life-sustaining treatment, hospice and palliative care nurses must identify their level of job stress and apply regular counseling programs to reduce mental and psychological burdens. Second, it is necessary to develop a customized resilience-building program that caters specifically to hospice and palliative care nurses. Third, active nursing policies should be supported that enable nurses to choose the hospice and palliative care department they wish to work in.
A limitation of this study was that it did not consider other variables, such as the satisfaction of hospice and palliative care nurses with working conditions. The indirect mediation effect of resilience on secondary traumatic stress, a subdomain of ProQOL, was not found; therefore, future studies are needed to confirm the relationship between secondary traumatic stress and resilience
CONFLICTS OF INTEREST:The authors declare that no known competing financial interests or personal relationships influenced the work reported in this paper.
AUTHORSHIP:
Conceptualization, methodology, formal analysis, writing-original draft, writing-review and editing - JE.
Conceptualization, writing-original draft, writing-review and editing - HSJ.
Conceptualization, data curation, writing-original draft - KHS.
The authors gratefully acknowledge the scholars whose articles are cited and referenced in this manuscript. The authors are also grateful to the authors, editors, and publishers of the articles, journals, and books included in the literature review conducted for this study. We also want to thank the nurses who participated in this study.
This work was supported by the Basic Science Research Program of the National Research Foundation of Korea, funded by the Ministry of Education (grant no. 2021R1F1A104945411). The sponsors had no role in the study design; the collection, analysis, and interpretation of data; writing of the report; or in the decision to submit the article for publication.
 E-SUBMISSION
E-SUBMISSION