
Purpose
This study investigated the mediating effect of sleep discomfort in the relationship between tinnitus distress and depression.
Methods
This cross-sectional study used the Tinnitus Handicap Inventory, the Korean Screening Tool for Depressive Disorders, and the Korean version of the Pittsburgh Sleep Quality Index to examine a convenience sample of 139 individuals with tinnitus who were selected from an online patient community in January 2023. Data were analyzed using the independent t-test, Pearson's correlation coefficients, and the PROCESS macro with 95% bootstrap confidence intervals. All statistical analyses were performed using IBM SPSS/WIN 25.0.
Results
Tinnitus distress exhibited a positive correlation with depression (r=.70, p<.001) and sleep discomfort (r=.33, p<.001), and depression showed a positive correlation with sleep discomfort (r=.52, p<.001). Further, sleep discomfort had a statistically significant partial mediating effect in the relationship between tinnitus distress and depression (β=.11; 95% CI, 0.05~0.18).
Conclusion
The findings of this study indicate that sleep discomfort plays a partial mediatory role in the relationship between tinnitus distress and depression.
Intervention programs for improving sleep discomfort among individuals with tinnitus are recommended to reduce depression in this population. In addition, screenings for sleep discomfort and depression should be routinely carried out as part of the treatment strategy for individuals with tinnitus.
This study investigated the mediating effect of sleep discomfort in the relationship between tinnitus distress and depression.
This cross-sectional study used the Tinnitus Handicap Inventory, the Korean Screening Tool for Depressive Disorders, and the Korean version of the Pittsburgh Sleep Quality Index to examine a convenience sample of 139 individuals with tinnitus who were selected from an online patient community in January 2023. Data were analyzed using the independent t-test, Pearson's correlation coefficients, and the PROCESS macro with 95% bootstrap confidence intervals. All statistical analyses were performed using IBM SPSS/WIN 25.0.
Tinnitus distress exhibited a positive correlation with depression (r=.70, p<.001) and sleep discomfort (r=.33, p<.001), and depression showed a positive correlation with sleep discomfort (r=.52, p<.001). Further, sleep discomfort had a statistically significant partial mediating effect in the relationship between tinnitus distress and depression (β=.11; 95% CI, 0.05~0.18).
The findings of this study indicate that sleep discomfort plays a partial mediatory role in the relationship between tinnitus distress and depression. Intervention programs for improving sleep discomfort among individuals with tinnitus are recommended to reduce depression in this population. In addition, screenings for sleep discomfort and depression should be routinely carried out as part of the treatment strategy for individuals with tinnitus.
Tinnitus, which is defined as the subjective perception of sound in the absence of external auditory stimuli and with no known exact cause, is a prevalent symptom among Koreans. In 2022, the prevalence of subjective tinnitus among individuals aged 40 and older was 9.5%, indicating that approximately one in 10 people in Korea is affected [1]. The number of medical visits due to tinnitus has increased annually, except for 2020 when the COVID-19 pandemic occurred; moreover, the number of visits steadily rises with age up to 69 years [2].
Tinnitus is strongly associated with negative emotions, including anxiety and depression, and it contributes to the development of psychological symptoms [3]. A previous study reported that high tinnitus distress was significantly associated with higher depression scores and lower health-related quality of life [4], and a systematic review also reported that 33% of patients with tinnitus develop depression [5]. Furthermore, Trevis et al., reporting high levels of negative coping with tinnitus in patients with chronic depression, emphasized the significance of managing depression in patients with tinnitus [6].
Sleep disorders are prevalent conditions characterized by insufficient sleep duration and quality, with adverse impacts on next-day activities. In South Korea, they affect 17~23% of adults, and the total number of patients has increased at an average annual growth rate of 4.7% from 2018 to 2022 [7]. Sleep discomfort has a significant effect on mental health, and individuals with poor sleep quality show a higher prevalence of depressive symptoms than those with good sleep quality [8]. Additionally, sleep disorders have been identified as modifiable risk factors for depression [9].
A meta-analysis found that 53.5% of patients with tinnitus experienced sleep discomfort, with women reporting more sleep difficulties than men [10]. A recent study [11] reported that >70% of patients with tinnitus developed sleep disorders; in particular, most patients with chronic tinnitus, regardless of tinnitus severity or personal characteristics, stated that they experienced difficulty falling asleep and staying asleep due to tinnitus. Wang et al. [12] also reported that 54.2% of patients with tinnitus were diagnosed with sleep disorders and found that sleep disorders mediated the relationship between tinnitus severity and anxiety. Therefore, our study aimed to examine whether sleep discomfort similarly plays a mediating role in the relationship between tinnitus distress and depression.
The specific objectives of this study were to 1) determine the general characteristics of participants and assess their levels of tinnitus distress, sleep discomfort, and depression; 2) explore differences in tinnitus distress, sleep discomfort, and depression scores based on the general characteristics of the participants; 3) examine correlations among tinnitus distress, sleep discomfort, and depression; and 4) investigate the mediating role of sleep discomfort in the relationship between tinnitus distress and depression among participants. The insights gained from this mediation analysis could contribute to a deeper understanding of the complex interactions between tinnitus distress, sleep discomfort, and depression. Additionally, these findings may guide nurses in prioritizing specific aspects of care for individuals with tinnitus in clinical settings.
This study was designed as a cross-sectional survey to examine the mediating effect of sleep discomfort in the relationship between tinnitus distress and depression. Based on the previous research findings, the following hypotheses were derived regarding the relationship among tinnitus distress, sleep discomfort, and depression:
Proposition 1: Tinnitus distress has a significant impact on depression
Proposition 2: Sleep discomfort has a significant impact on depression
Proposition 3: Tinnitus distress has a significant impact on sleep discomfort
Based on these hypotheses, we predicted that sleep distress might be a mediator in the relationship between tinnitus distress and depression.
Data were collected through an online survey in January 2023. The study participants were individuals aged ≥19 years who were members of an online tinnitus support group, had experienced continuous or intermittent tinnitus for at least 3 months, and were able to read the questionnaire and indicate their intentions. Individuals with a neurological or psychiatric condition, or chronic pain other than tinnitus were excluded. To prevent duplicate responses, community staff verified participants' phone numbers, which were collected for survey payments, and confirmed that participants met the inclusion criteria, including membership status. Only those who passed these checks and consented to participate voluntarily were allowed to proceed with the survey. There is an interdependent relationship between significance level (α), statistical power (the minimum acceptable level of power for a study is .80, or 80%), effect size (nursing variables are moderately correlated with one another), and sample size. Fixing any three of these factors determines the fourth [13]. To determine the number of participants, the G*Power 3.1.9.7 software [14] was utilized, based on a two-tailed test with a significance level (α) of .05, a statistical power of .85, and a medium effect size of .15. With 10 independent variables, 131 participants were initially selected. Out of 150 survey responses received, 139 were analyzed after excluding 11 responses identified as either dishonest or duplicates. The number of participants was deemed adequate as it surpassed the number calculated using the G*Power 3.1 software program.
This study was approved by the Institutional Review Board of Kyungpook National University (Approval Number: 2023-0012), and informed consent was obtained from all participants before the commencement of the study. All participants received a recruitment document describing the purpose of the study, the number of survey questions, and the survey response method. Information regarding voluntary participation, patients' ability to withdraw from the study at any time, and their rights to anonymity, privacy, and strict confidentiality were also provided. Furthermore, it was stated that all collected data would be securely stored in a locked laboratory computer and deleted 3 years after study completion.
Based on the findings of a previous study [15], the general characteristics of the participants were assessed using seven questions. Three of these questions focused on socioeconomic factors such as sex, age, and occupation. The remaining four questions addressed aspects of tinnitus, including its direction, duration, pattern, and subjective perception.
The Tinnitus Handicap Inventory (THI) was developed by Newman et al. [16] and was translated and validated for Korean conditions by Kim et al. [17]. The THI consists of 25 items, with 11, 9, and 5 items for the functional, emotional, and catastrophizing subscales, respectively. Each item is scored on a scale of 0~4, where 0 indicates "no," 2 indicates "sometimes," and 4 indicates "yes." The total score ranges from 0 to 100 points, with higher scores indicating greater tinnitus distress. Zeman et al. [18] categorized the THI score into five grades of tinnitus severity: slight (0~16), mild (18~36), moderate (38~56), severe (58~76), and catastrophic (78~100). The reliability for the translated version was shown by a Cronbach's α value of .95, with .89, .91, and .79 for the functional, emotional, and catastrophizing subscales, respectively [17]. In this study, Cronbach's α for the THI total score was .93, with values of .88, .90, and .67 for the functional, emotional, and catastrophizing subscales, respectively.
Sleep discomfort was measured using the Korean version of the Pittsburgh Sleep Quality Index developed by Buysse et al. [19] and translated into Korean by Sohn et al. [20]. This 18-item self-report instrument assesses sleep quality over the past month using the following seven factors: subjective sleep discomfort, sleep latency, sleep duration, sleep efficiency, sleep discomfort, use of sleep medication, and daytime dysfunction. Each factor is rated on a scale of 0~3 (total range, 0~21), with a score of ≥8.5 points indicating poor sleep discomfort and sleep problems. Cronbach's α was .84 for the Korean version of the Sleep discomfort Index tool [20] and .69 in this study.
Depression was measured using the Korean Screening Tool for Depressive Disorders developed by Choi et al. [21]. This 12-item instrument is a 5-point Likert scale that scores the symptoms corresponding to each question in the past 2 weeks, with 0 points assigned for "never" and 4 points for "very much." The total score was calculated according to the developer's instructions. Since items 10 and 11 are oppositely worded (appetite vs. anorexia), only the higher score of the two was included. The raw scores of each of the 11 items were then multiplied by their assigned weights and summed for analysis. The score ranges from 0 to 51.64 points, with higher scores indicating more severe depression. Scores above the cutoff point of 14 indicate moderate to severe depression. At the time of development, the instrument reliability was shown by a Cronbach's α of .95 [21]. In this study, Cronbach's α was .90.
Data were collected during January 2023 using a Google online survey. Prior to data collection, the study purpose, requirements, and methodology were explained to the representative of an online tinnitus support group, from whom cooperation was sought in recruiting participants. The participant recruitment document was then provided to the patient representative, who shared it with the online community members. Those who read the notice and wanted to participate in the survey could freely access the link and respond to the survey. Before the survey, patients were asked to indicate whether they agreed to participate voluntarily and whether they met the inclusion criteria. The survey was initiated after confirming their voluntary participation and eligibility.
Data were analyzed using IBM SPSS/WIN 25.0 [22]. The general characteristics of participants, as well as their tinnitus distress, sleep discomfort, and depression scores, were evaluated using descriptive statistics. The independent t-test was used to analyze the differences in tinnitus distress, sleep discomfort, and depression scores according to the general characteristics of the participants. Pearson correlation coefficients were used to analyze the correlation among tinnitus distress, sleep discomfort, and depression. The mediating effect of sleep discomfort in the relationship between tinnitus distress and depression was evaluated using Hayes's PROCESS Macro Model 4 (version 4.2) [22]. Bootstrapping with 5000 iterations was used to test the significance of the indirect effect of sleep discomfort in the relationship between tinnitus distress and depression [23].
Of 139 participants, 70 (50.4%) were men, with a mean age of 44.46 years (range, 20~67 years) (Table 1). Overall, 82.7% of participants were employed, and 48.9% of participants reported the presence of unilateral tinnitus. The mean tinnitus duration was 62.89 months (range, 3~432 months). Furthermore, 83.5% of the participants had continuous tinnitus, and 23.7% reported that their subjective perception of tinnitus was unbearable. Tinnitus distress was significantly higher in participants who were not employed than those who were employed (t=−2.34, p=.023). Furthermore, tinnitus distress was statistically significantly higher in participants who reported that their subjective perception of tinnitus was unbearable (t=−6.99, p<.001). Sleep discomfort was also statistically significantly higher in women than in men (t=−2.97, p=.004), in those who were unemployed than in those who were employed (t= −2.25, p=.026), and in those who subjectively reported tinnitus as unbearable than in those who reported it as tolerable (t=−5.28, p<.001). Depression scores were statistically significantly higher in women than in men (t=−2.21, p=.029) and in those who subjectively reported tinnitus as unbearable than in those who reported it as tolerable (t=−4.98, p<.001) (Table 1).
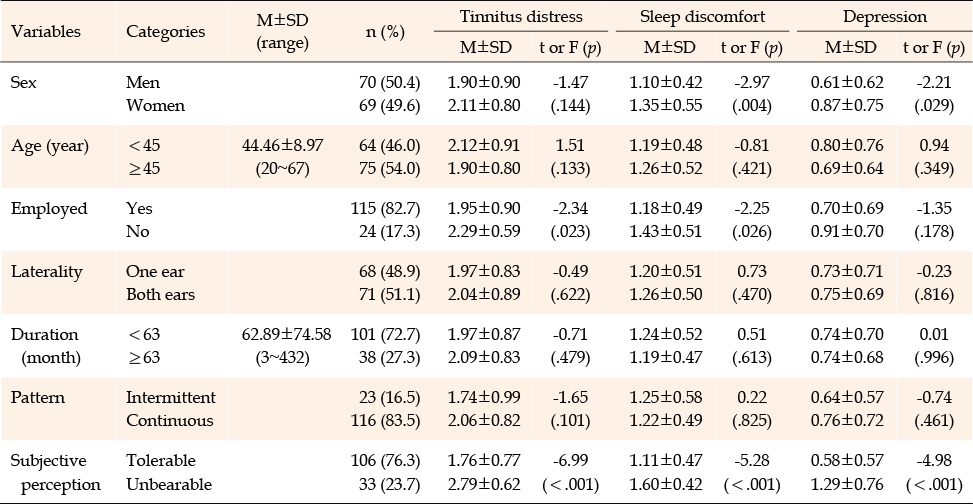
Table 1
Differences in Tinnitus Distress, Sleep Discomfort, and Depression Scores by General Characteristics (N=139)
The average tinnitus distress score in this study was 50.10±21.46 (of 100 points). The functional subscale score was 20.14±9.68 (range, 0~44) points, the emotional subscale score was 16.91±9.45 (range, 0~36) points, and the catastrophizing subscale score was 13.05±4.90 (range, 0~20) points. When the total tinnitus score was categorized into score bands, 8 (5.8%) patients had slight tinnitus with scores between 0 and 16, 34 (24.4%) had mild tinnitus with scores between 18 and 36, 44 (31.7%) had moderate tinnitus with scores between 38 and 56, 36 (25.9%) had severe tinnitus with a score between 58 and 76, and 17 (12.2%) had catastrophic tinnitus with a score between 78 and 100. Each of the seven subcomponents of sleep discomfort was rated on a scale of 0~3, for a total of 0~21 points. The overall mean score was 8.59±3.53 points (range, 2~19 points). Furthermore, 42.4% of participants had a total sleep discomfort score of ≥8.5 points, indicating poor sleep. For each subcomponent on a scale of 0~3, the scores for subjective sleep discomfort, sleep latency, sleep duration, sleep efficiency, sleep discomfort, use of sleep medication, and daytime dysfunction were 1.69±0.70, 1.70±0.94, 1.14±0.85, 0.51±0.89, 1.54±0.58, 0.61±1.12, and 1.40±0.80, respectively. The depression score ranged from 0 to 51.64 points, with a mean score of 8.14±7.63 points (range, 0~32 points), and 23% of all participants scored above the cutoff point of 14 points for depression treatment (Table 2).
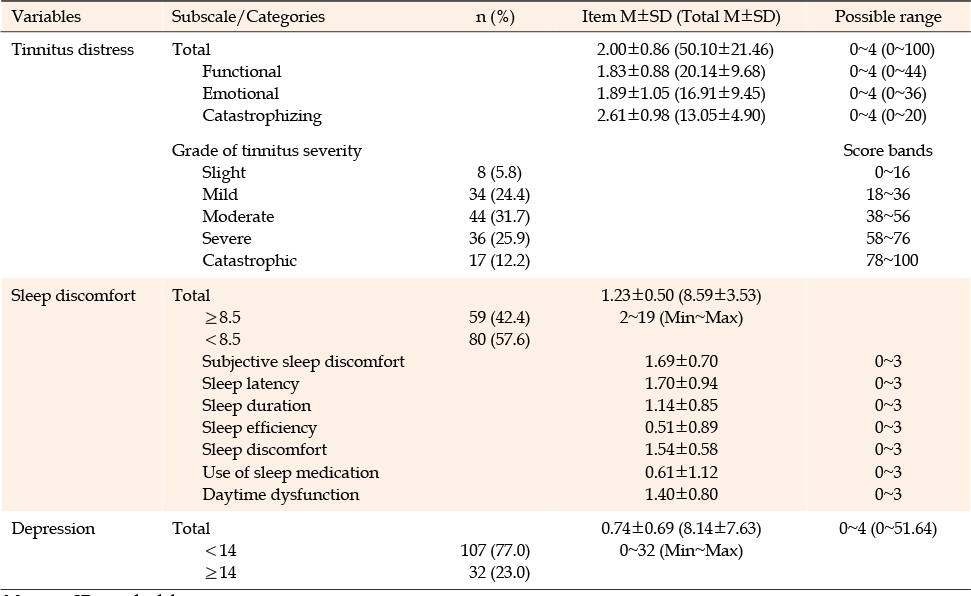
Table 2
Tinnitus Distress, Sleep Discomfort, and Depression (N=139)
Tinnitus distress showed positive correlations with depression (r=.70, p<.001) and sleep discomfort (r=.33, p<.001). The depression score was positively correlated with sleep discomfort (r=.52, p<.001). All tinnitus distress subscales were correlated with depression, with the emotional subscale score having the highest correlation (r=.70, p<.001), followed by the functional subscale (r=.64, p<.001) and catastrophizing subscale (r=.44, p<.001). Among the tinnitus distress subscales, only the functional (r=.35 p<.001) and emotional (r=.31, p<.001) subscales were correlated with sleep discomfort (Table 3).

Table 3
Correlations among Tinnitus Distress, Sleep Discomfort, and Depression (N=139)
Before testing the mediation effect, we verified that the Durbin-Watson value was close to 2, and the correlation coefficients of all variables were less than 0.8. The tolerance was above 0.1 and the variation inflation factor was below 10, suggesting no multicollinearity. Finally, the residuals were checked for normality. The results revealed that tinnitus distress significantly affected sleep discomfort (β=.33, t=4.07, p<.001) and depression (β=.59, t=10.14, p<.001). Furthermore, sleep discomfort had a statistically significant effect on depression (β=.33, t=5.63, p<.001; Table 4). Bootstrapping with 5,000 iterations was performed to examine the mediating role of sleep discomfort in the pathway from tinnitus distress to depression, and the findings were statistically significant (β=.11; 95% CI, 0.05~0.18) as the 95% confidence intervals did not include 0. Therefore, the partial mediating effect of sleep discomfort in the relationship between tinnitus discomfort and depression was confirmed (Table 4, Figure 1).
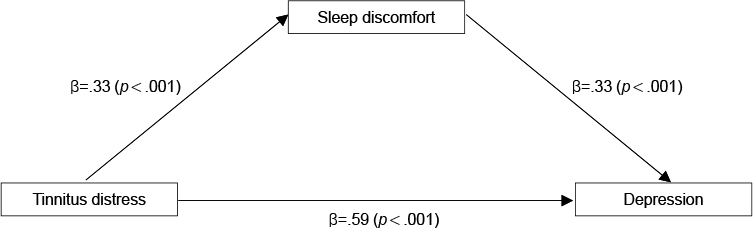
Figure 1
Path diagram of the model.
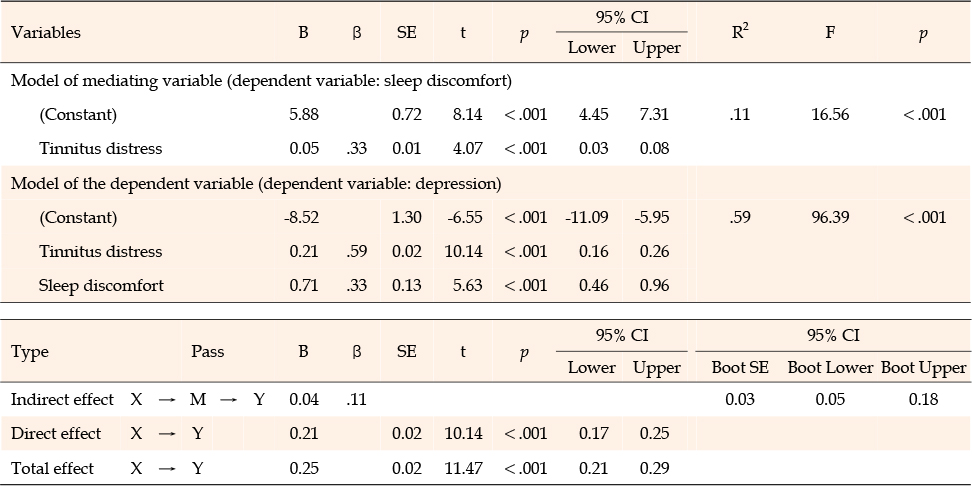
Table 4
Indirect Mediation Effect of Sleep Discomfort in the Relationship between Tinnitus Distress and Depression (N=139)
This study investigated the mediating effect of sleep discomfort in the relationship between tinnitus distress and depression.
In this study, the average tinnitus distress score was 50.1±21.5 out of 100, which is slightly higher than the scores reported in international (44.3±23.0) [4] and Korean studies (49.2±26.2) [24], but lower than the score of 54.2±26.0 in a study using the Japanese version of the same instrument [25]. A total of 5.8% of participants in the current study reported slight tinnitus distress; this proportion is lower than reported in previous studies [4, 24, 25]. Conversely, 69.8% reported moderate or high tinnitus distress, similar to findings in a Korean study (65.6%) [24], but differing from those of international studies (58.2% and 71.1%) [4, 25]. The previous two studies [4, 24] included subjects with average ages of 46.8 years and 47 years, respectively, similar to this study's participants. However, Wakabayashi et al. [25], with participants who were approximately 14 years older than those in this study, reported higher tinnitus distress scores and the highest proportion of moderate or higher distress perception. These findings are consistent with those of big data statistics and previous research [2, 26], indicating that tinnitus distress increases with age. Comparing tinnitus durations across studies is challenging. The duration was unspecified in one study [25], while it was 65.8 months in another [4], similar to the current study, and significantly shorter at 26.4 months in yet another [24], despite similar tinnitus distress scores. These discrepancies underscore the need for future research to explore potential differences in tinnitus distress among various age groups and according to the duration of tinnitus.
In this study, tinnitus patients had a sleep quality score of 8.6±3.5, notably higher than the general population with an average age of 40.6 years, which scored 5.7±3.2 [27], and adults aged 19 years and older, who scored 5.6±3.2 [28], using the same measurement tool. The score in the current study also exceeded the 7.9±3.4 observed in patients with asthma [29]. Higher scores indicate poorer sleep quality; therefore, the participants in this study, with an average age of 45, exhibited significantly worse sleep quality than average Korean adults without tinnitus and asthma patients with an average age of 63 years. The PSQI-K uses a cutoff score of 8.5 to classify sleep quality as poor, and 42.4% of the study participants scored 8.5 or above, indicating poor sleep quality. Previous research using the PSQI-K has employed the original tool's cutoff score of 5 instead of the PSQI-K's cutoff score of 8.5. In those studies, 44.7% and 41% of the general population [27, 28], and 71.2% of asthma patients [29] scored 5 or higher. For comparison, when applying a cutoff score of 5 or higher in this study, 90% of the participants exceeded this threshold, highlighting that individuals with tinnitus experience significantly worse sleep quality.
In this study, we found a positive correlation between sleep discomfort and depression in patients with tinnitus, consistent with previous research that identified a strong bidirectional correlation between depression and sleep discomfort [30]. The average depression score among participants was 8.1±7.6, based on a scale of 0 to 51.6 points, with 23% scoring above the clinical cutoff of 14. This result is comparable to a prior study that reported a 25.6% rate of depression among tinnitus patients [3] and aligns with a meta-analysis showing an overall depression prevalence of 33%, with severe depression in 23% of cases [5]. However, a cohort study on tinnitus patients found that only 5.5% required clinical treatment for depression, which contrasts with our findings [31]. Additionally, Weidt et al. [4] reported that 11.5% of tinnitus patients with less severe symptoms met the criteria for clinical depression using a BDI cutoff of 18 or more, lower than the 23% in our study with a cutoff of 14 or more. These findings indicate a positive correlation between the severity of tinnitus symptoms and the prevalence of depression.
The findings of the current study suggest a link between tinnitus and depressive disorders, especially when accompanied by sleep discomfort. According to a previous qualitative study [32], individuals with tinnitus often experience increased distress at night when ambient noise levels are lower. This leads to difficulties in falling asleep and frequently results in shallow sleep. To manage these sleep disturbances, many individuals resort to neuroleptic medications, while others seek psychiatric counseling or hospitalization for severe insomnia. The current study quantitatively confirms the results obtained from the earlier qualitative study [32].
It is worth noting that the prevalence rates of tinnitus, sleep disorders, and depression in Korea, as well as the number of hospital visits related to these conditions, are all increasing [2, 7]. This combination can significantly impair daily functioning and reduce physical and psychological quality of life. Additionally, tinnitus is strongly associated with suicidal ideation [26]. Given that life expectancy in Korea has risen from 76.2 years in 2,000 to 83.8 years in 2021 [33], and considering the still unidentified cause of tinnitus and its challenging treatment options, it is likely that tinnitus may persist into old age due to increased life spans. Therefore, healthcare providers should take into account sleep discomfort and depression when managing individuals with tinnitus, and further research into the risk factors of tinnitus should be conducted to help alleviate its symptoms. Moreover, since existing research [9] indicates that sleep discomfort is a modifiable risk factor for depression, health researchers should develop and implement interventions aimed at reducing sleep discomfort in individuals with tinnitus.
This study confirmed the mediating effect of sleep discomfort in the relationship between tinnitus distress and depression. Although the effect size was small (β=.11; 95% CI, 0.05~0.18), sleep discomfort partially mediated the relationship between tinnitus distress and depression. According to Baron and Kenny [34], the inadequate reliability of the tool used to measure a mediator can result in underestimating the mediator's effect on the dependent variable and overestimating the effect of the independent variable on the dependent variable. In this study, the modest partial mediation effect size of sleep discomfort in the tinnitus distress-depression relationship might be attributed to the low reliability of the sleep discomfort measurement instrument, as indicated by a Cronbach's α value of .69. Therefore, replicating the study with an alternative tool to assess sleep quality would be beneficial. Additionally, this study has several limitations. The participants were recruited through convenience sampling, targeting adults aged 19 and older, including middle-aged and older adults. Consequently, the findings cannot be generalized to the entire population of patients with tinnitus. The study also did not determine whether the participants had been diagnosed with clinical depression or were taking antidepressant medication. Therefore, it is necessary to confirm the use of antidepressant medication in patients with tinnitus in follow-up studies.
This study confirmed that sleep discomfort plays a partial mediatory role in the relationship between tinnitus distress and depression. Therefore, healthcare professionals, especially nurses, should consider this interplay among tinnitus distress, sleep discomfort, and depression when managing individuals with tinnitus. Based on the results of the current study, we suggest an experimental study design to determine the effectiveness of developing and implementing a nursing intervention aimed at improving sleep quality in individuals with tinnitus and reducing the occurrence of depression. Additionally, a population-wide survey should be conducted on individuals with tinnitus who are taking antidepressants. Furthermore, in the clinical care of individuals with tinnitus, routine screening for sleep discomfort and depression is necessary.
CONFLICTS OF INTEREST:The author declared no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - JWJ.
Analysis, or interpretation of the data - JWJ.
Drafting or critical revision of the manuscript for important intellectual content - JWJ.
 E-SUBMISSION
E-SUBMISSION