
Purpose
This study examined the relationships of health literacy, physical activity, and grip strength with self-care compliance in older male patients with chronic heart failure.
Methods
A cross-sectional descriptive was conducted, and 106 older male outpatients with chronic HF were recruited from a veterans’ hospital in Seoul. Data were collected from February 7, 2022 to April 10, 2022 using a self-reported questionnaire and were analyzed using SPSS/WIN 23.0.
Results
The average age of the participants was 76.3±4.5 years, and the average time elapsed since the heart failure diagnosis was 3.22±2.01 years. The mean self-care compliance score was 42.21±6.03 out of 60 points.
In the univariate analysis, grip strength was not significantly correlated with self-care compliance. The hierarchical regression analysis indicated that health literacy (β=.33, p<.001), physical activity (β=.32, p=.001), and alcohol drinking (β=-.28, p=.001) had statistically significant effects on self-care compliance, collectively explaining 34% of the variance (adjusted R2 =.34, F=12.00, p<.001).
Conclusion
The study highlights the necessity of periodically assessing and considering health literacy and the level of physical activity when developing educational strategies to promote self-care compliance among older male patients with heart failure in outpatient nursing practice.
This study examined the relationships of health literacy, physical activity, and grip strength with self-care compliance in older male patients with chronic heart failure.
A cross-sectional descriptive was conducted, and 106 older male outpatients with chronic HF were recruited from a veterans’ hospital in Seoul. Data were collected from February 7, 2022 to April 10, 2022 using a self-reported questionnaire and were analyzed using SPSS/WIN 23.0.
The average age of the participants was 76.3±4.5 years, and the average time elapsed since the heart failure diagnosis was 3.22±2.01 years. The mean self-care compliance score was 42.21±6.03 out of 60 points. In the univariate analysis, grip strength was not significantly correlated with self-care compliance. The hierarchical regression analysis indicated that health literacy (β=.33, p<.001), physical activity (β=.32, p=.001), and alcohol drinking (β=-.28, p=.001) had statistically significant effects on self-care compliance, collectively explaining 34% of the variance (adjusted R2=.34, F=12.00, p<.001).
The study highlights the necessity of periodically assessing and considering health literacy and the level of physical activity when developing educational strategies to promote self-care compliance among older male patients with heart failure in outpatient nursing practice.
Heart Failure (HF) affects approximately 26 million people globally [1] and is characterized by shortness of breath, swelling, fatigue, and depression [2]. It can be classified as acute or chronic based on the speed of symptom onset [2]. HF imposes a significant burden on patients, resulting in poor quality of life, increased mortality, more frequent hospital admissions, and higher healthcare costs [1]. In Korea, the prevalence of HF is expected to increase due to an aging population and risk factors such as hypertension and diabetes [3]. By 2040, it is projected that over 1.72 million people in South Korea will have HF, accounting for more than 3.0% of the population [3, 4]. The prevalence of HF has steadily increased from 0.77% in 2002 to 2.24% in 2018, with a more pronounced rise in men (115.8%) than in women (70.5%) [4]. HF presents differently in men and women due to differences in pathophysiology, clinical presentation, and diagnosis [5]. Additionally, HF is most prevalent among older adults [6]. Consequently, there is a pressing need to prioritize the management of HF in older male patients.
The European Society of Cardiology's HF guidelines emphasize the importance of patient education on adhering to treatment, taking medications regularly, engaging in tailored physical activity, and monitoring symptoms through regular check-ups [2]. Effective self-care among HF patients is linked to improved health outcomes [7]. Improved self-care, symptom recognition, and treatment have been shown to reduce readmission rates among HF patients [8]. Self-care involves naturalistic decision-making, which includes actions to maintain physiological balance (self-care maintenance) and responses to symptoms and indicators (self-care management) [9]. Despite its importance, many patients with HF struggle with self-care due to various factors, including a lack of understanding of their symptoms, difficulty accessing medical information, inadequate healthcare support systems, physical limitations, emotional stress, and a lack of social support [2]. Given the significant impact of self-care compliance on the prognosis of HF, it is crucial to identify the factors that influence self-care compliance. Health literacy, defined as the ability to access, understand, and apply health information, plays a key role in medication adherence and health management among patients. It is particularly important in effective communication between patients and healthcare providers and in self-care compliance among those with HF [10]. Higher health literacy facilitates smoother communication and enhances the effectiveness of self-care. The American Heart Association recommends assessing patients' health literacy to improve their understanding of self-care instructions [6]. Patients with higher health literacy are more likely to understand their condition, make informed decisions, and adhere to treatment plans [10]. Therefore, health literacy is a vital factor influencing self-care in patients with HF.
Physical activity, which includes daily movements such as exercise and housework, serves as a diagnostic, prognostic, and therapeutic tool for chronic HF [2, 11]. Grip strength is a simple measure for assessing muscle strength and physical performance in older adults and serves as a predictive factor in HF diagnosis [12, 13]. Although grip strength has been linked to cardiovascular mortality and disease occurrence, its association with HF remains unclear and is subject to ongoing debate [12]. Promoting physical activity and grip strength in HF patients has proven to be cost-effective, reducing hospitalization and mortality rates while enhancing quality of life [12]. While patients with HF tend to gradually increase their physical activity at the individual level, these changes are often limited by factors such as age-related muscle weakness, exercise intolerance, and symptoms like dyspnea and fatigue [2, 14]. Therefore, it is necessary to evaluate both the understanding of health-related information and physical activity levels, which include tasks such as adhering to medication and engaging in exercise. This approach is likely to be effective in increasing self-care compliance among older male patients with HF. The quality of life in HF patients is influenced by both physical and cognitive abilities, highlighting the importance of further research on various factors affecting self-care [2, 9]. Previous studies have suggested a relationship between grip strength, health literacy, and cognitive preservation [15], emphasizing the need for ongoing research to further clarify these connections. The aim of this study was to examine the impact of health literacy, physical activity, and grip strength on self-care compliance among older male patients with chronic HF. It is hoped that the findings of this study will contribute to the development of effective interventions to promote healthy adaptation based on an understanding of the characteristics associated with self-care adherence in older male patients with HF.
This cross-sectional descriptive study aimed to identify the influences of health literacy, physical activity, and grip strength on self-care compliance among older male patients with chronic HF.
The participants in this study were patients with chronic HF who attended the cardiology department at a Veterans Health Service Medical Center in Seoul, Korea. The inclusion criteria specified that participants must be: 1) male, aged 65 or older; 2) diagnosed with chronic HF by a physician and receiving outpatient treatment; 3) capable of communicating and independently responding to questionnaires; 4) able to live independently; and 5) fully understanding of the study's purpose and voluntarily consenting to participate. The exclusion criteria included: 1) patients with a history of cognitive impairments such as Alzheimer's disease or vascular dementia; 2) patients classified as New York Heart Association (NYHA) class IV with mobility limitations; 3) individuals with psychiatric diagnoses or those receiving psychiatric medications; 4) individuals with visual or hearing impairments.
The G*Power 3.1.9.4 program was utilized to determine the appropriate sample size for the multiple regression analysis. The effect size for this study was estimated at 0.30, based on a coefficient of determination (R2) of 0.23, which was confirmed in a prior study examining factors that influence self-care compliance in patients with chronic HF [15]. For the multiple regression analysis, an effect size of f2=0.30, a power of 95%, a significance level of 0.05, and 10 independent variables were considered, necessitating a sample size of 91 patients. Given an anticipated dropout rate of 20%, 113 patients were initially recruited. However, the final analysis included only 106 patients after excluding four due to insufficient responses.
The general characteristics were evaluated by 11 questions covering age, marital status, economic activity, cohabitation, caregiver status, education level, monthly household income, smoking habits, drinking habits, body mass index, and regular exercise. The disease-related characteristics section included four questions regarding the duration of diagnosis, educational experience, hospitalization history, and NYHA class.
The health literacy measurement tool for patients with cardiovascular disease, developed by Shim [16], was utilized in this study to assess health literacy, with the author's permission obtained via email. This instrument comprises 22 items, each rated on a 4-point Likert scale that ranges from 1 ("not at all") to 4 ("very much so"), with possible scores varying from 22 to 88. Higher scores reflect a greater capacity to comprehend health information. Initially, when the tool was developed, it demonstrated a Cronbach's α of .89 [16]; in the current study, Cronbach's α was .79.
The reliability and validity of the Korean version of the Global Physical Activity Questionnaire, developed by the World Health Organization (WHO), have been confirmed [17]. This questionnaire is publicly available and free to use. It covers the previous seven days and includes 16 questions that ask about the frequency and duration of moderate-intensity and high-intensity physical activities in various domains, as well as the average time spent in sedentary activities. Responses are converted into minutes, and the Metabolic Equivalents of Task (METs) were calculated by multiplying the time spent on activities by the number of days exercised, adjusted for intensity. According to WHO-recommended standards, exercise intensities are categorized as follows: 4.0 METs for walking or cycling for transportation, 4.0 METs for moderate-intensity activities, and 8.0 METs for high-intensity activities [17]. The total physical activity is calculated by summing the activities related to transportation, moderate-intensity, and high-intensity efforts.
Grip strength was measured using a Grip Dynamometer (T.K.K.-5401, Japan). Participants were seated upright with their arms, torso, and palms aligned perpendicularly to the shoulder line, maintaining this position for at least 2 seconds. The Asian Working Group on Sarcopenia (AWGS) considers grip strength to be a key indicator of muscle strength, specifically focusing on the maximum value from the dominant hand [18]. In this study, the grip strength value was determined by averaging the maximum measurements obtained from the dominant hand, in accordance with methodologies from previous studies [19]. Sarcopenia was defined as having a grip strength of less than 26 kg in men, following the criteria set by the AWGS [18].
For assessing self-care compliance, we utilized the Korean version of the European Heart Failure Self-care Behavior Scale (EHFScBS-12), developed by Jaarsma et al. [20]. Permission to use this scale was granted by the authors via email. Although the self-care compliance tool was adapted from the EHFScBS-12 to the EHFScBS-9, this study employed the original EHFScBS-12 to explore various dimensions of self-care compliance. The tool comprises 12 items, each rated on a 5-point Likert scale from 1 ("never") to 5 ("always"). The total scores range from a minimum of 5 to a maximum of 60, with higher scores indicating greater self-care compliance. At the time of its development [20], the tool's reliability was shown by a Cronbach's α of 0.81; in the current study, Cronbach's α was .72.
This study was approved by our Institutional Review Board of the hospital where the researcher was affiliated and where data collection occurred (IRB No. 2022-01-006-006). Participants were fully informed about the research objectives, the questionnaire completion process, and the steps taken to protect their personal information, maintain confidentiality, and restrict data usage to research purposes only. They were also informed that their participation was voluntary and that they could withdraw from the study at any time without any repercussions. To safeguard confidentiality, each set of collected data was assigned a unique serial number and stored on an encrypted security device to prevent the identification of personal information.
The data collection period of this study was from February 7 to April 10, 2022. Patients who met the inclusion criteria were pre-selected from electronic medical records. Data collection was conducted with the assistance of cardiology specialists at the Veterans Health Service Medical Center. Eligible patients were invited to complete a self-reported structured questionnaire, which took approximately 20 minutes to finish. If a participant encountered difficulties with the questionnaire, the researcher would read the questions aloud and record their verbal responses. The grip strength of all participants was measured by the researcher during a one-on-one interview in a quiet room.
The collected data were analyzed using SPSS/WIN 23.0. We examined general and disease-related characteristics, as well as research variables, using descriptive statistics. To explore the relationship with self-care compliance, we employed an independent t-test and one-way ANOVA (analysis of variance). We calculated the means and standard deviations for the participant's health literacy, physical activity, grip strength, and self-care compliance. Pearson's correlation coefficients were used to analyze correlations between variables. A hierarchical multiple regression analysis determined the impact of general and disease-related characteristics and independent variables on self-care compliance. The statistical significance level for testing between variables was set at .05.
All participants were men and retired veterans. The average age was 76.32±4.51 years, with 74 participants (69.8%) being over 75 years old. Eighty-seven participants (82.1%) were married, and 66 (62.3%) had at least a high school education. Twenty participants (18.9%) were engaged in economic activities. Regarding household composition, 18 participants (17.0%) lived alone, while 81 (76.4%) had a caregiver. Fourteen participants (13.2%) were current smokers, and 27 (25.5%) reported consuming alcohol once a week.
Regarding disease-related characteristics, the average time elapsed since the HF diagnosis was 3.22±2.01 years. Eighty-three patients (78.3%) had been hospitalized due to HF had been hospitalized due to HF. All participants presented with comorbidities; hypertension was the most common, affecting 99 individuals (93.4%), followed by dyslipidemia, which affected 63 patients (59.4%). A total of 97 participants (91.5%) were classified as NYHA Class II (Table 1).
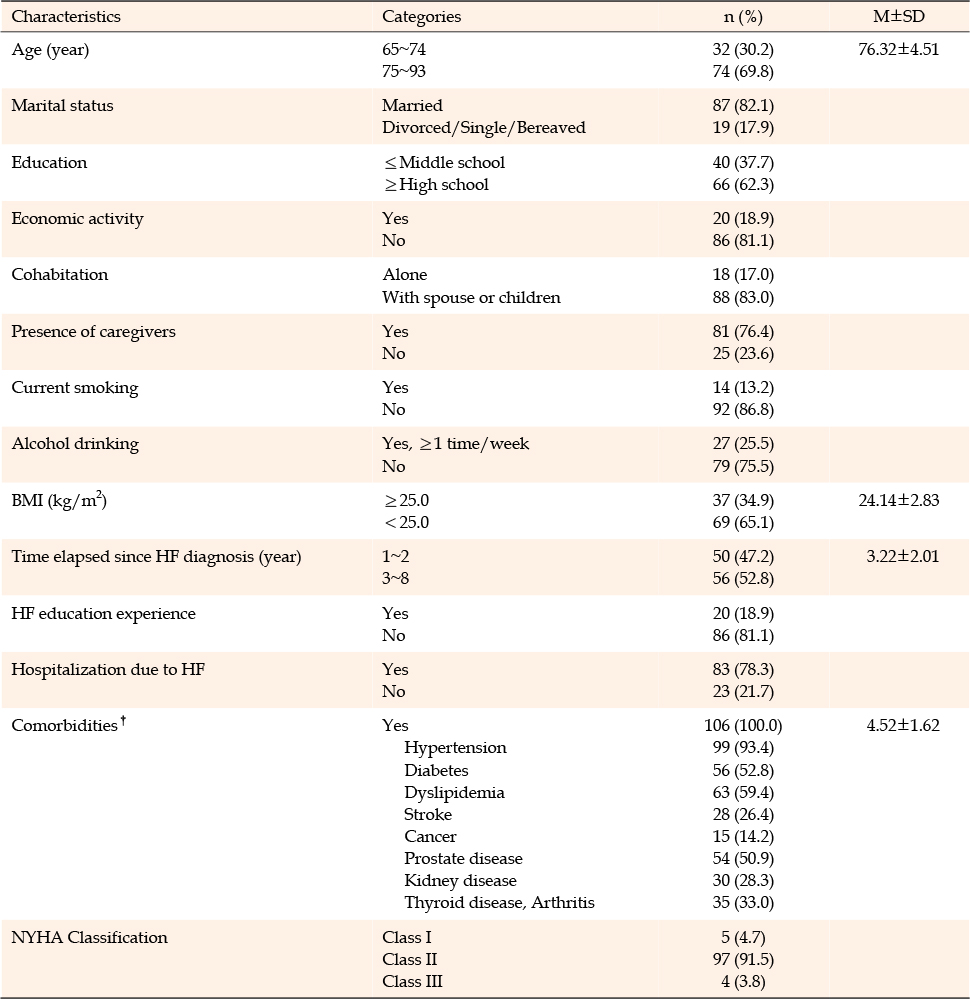
Table 1
General and Disease-related Characteristics of the Participants (N=106)
The average health literacy score was 67.55±8.25 out of a possible 88. The average scores for each subcategory were as follows: understanding and exploring health information, 12.76±2.22 out of 16; interactions with medical staff, 13.50±2.43 out of 16; use of health information support resources, 18.22±3.13 out of 24; and selection and evaluation of active health information, 23.07±3.50 out of 30. Physical activity levels averaged 1,676.42±1,596.94 METs, with a maximum of 7,200 METs. According to the WHO's physical activity guidelines [17], the participants were categorized as follows: 18.9% in the high-intensity group, 54.7% in the moderate-intensity group, and 26.4% in the low-intensity group. The average grip strength among the participants was 25.72±7.08 kg. Notably, 46.2% of participants fell into the sarcopenia category, with grip strengths of less than 26 kg, as defined by a previous study [18]. Self-care compliance averaged 42.21±6.03 out of 60. Within this category, adherence to prescribed medications had the highest score (4.52±0.59), while limiting fluid intake had the lowest (2.39±1.00) (Table 2).
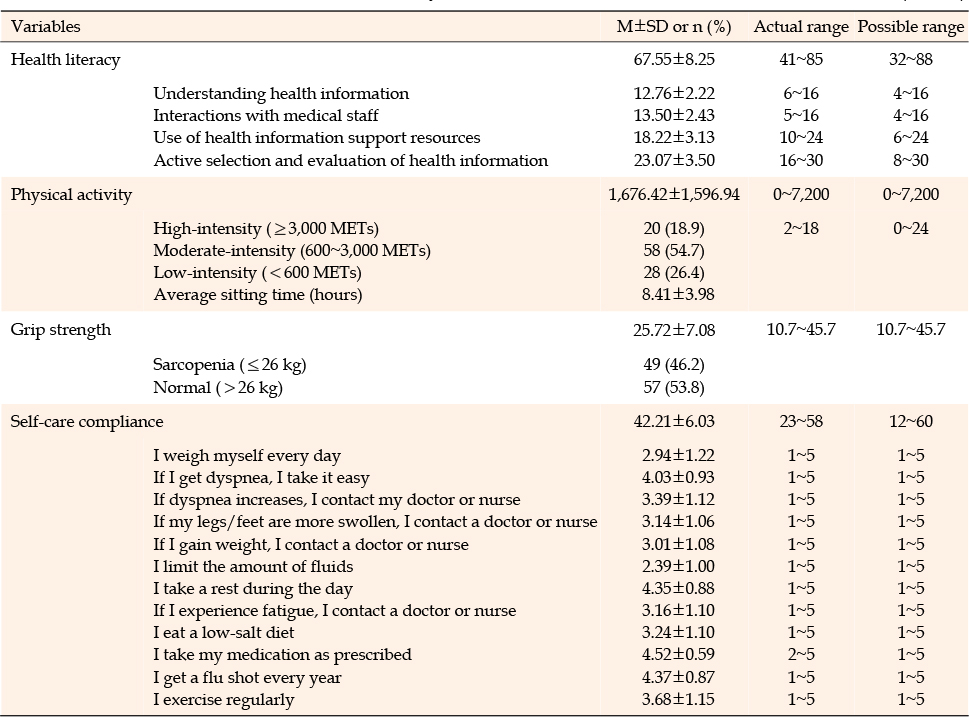
Table 2
Scores for the Research Variables of this Study (N=106)
Significant differences in self-care compliance were found according to some of the participants' general and disease-related characteristics-namely, economic activity (t=−2.19, p=.031), presence of caregivers (t=3.57, p<.001), and alcohol drinking (t=2.65, p=.009). In other words, self-care compliance was higher in participants who did not engage in economic activities, had a caregiver, or did not drink alcohol (Table 3).
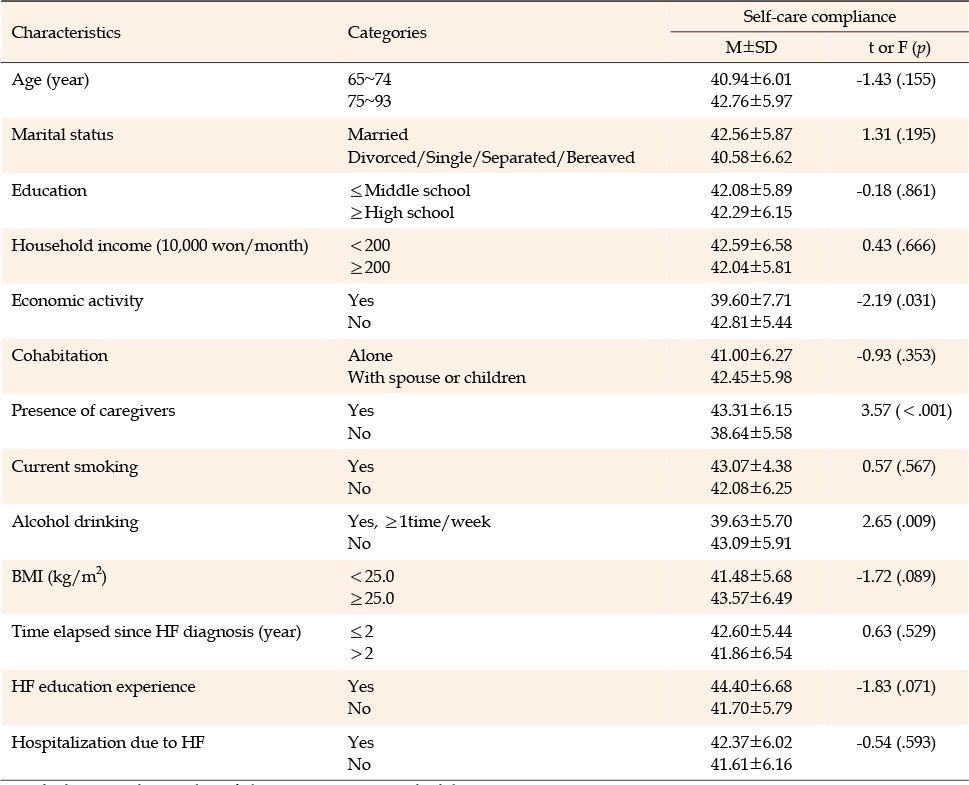
Table 3
Differences in Self-care Compliance According to Participants' Characteristics (N=106)
Health literacy (r=.43, p<.001) and physical activity (r=.28, p=.004) were significantly correlated with self-care compliance. However, there was no correlation between grip strength and self-care compliance (r=.02, p=.804) (Table 4).
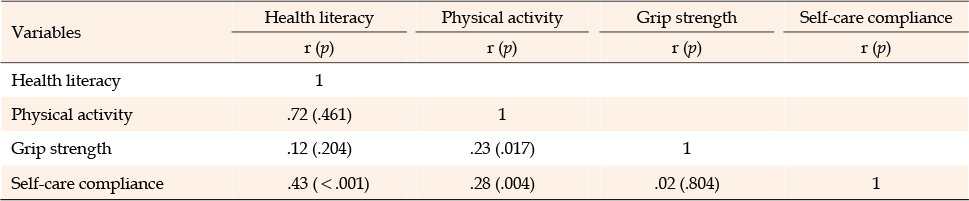
Table 4
Correlations among Health Literacy, Physical Activity, Grip Strength, and Self-care Compliance (N=106)
A hierarchical multiple regression analysis was conducted to identify the factors influencing self-care compliance among older male patients with chronic HF. Initially, the impact of control variables such as economic activity, caregiver support, and alcohol consumption on self-care compliance was examined (Model 1). Subsequently, the effects of health literacy and physical activity on self-care compliance were assessed, controlling for economic activity, caregiver support, and alcohol consumption (Model 2). The variance inflation factor (VIF) values ranged from 1.04 to 1.16, all below 10, indicating an absence of multicollinearity issues. Additionally, the Durbin-Watson value was 1.99, close to 2, suggesting no autocorrelation issues. The results of the residual analysis confirmed that the model met the criteria for linearity, normality, and homoscedasticity.
In the hierarchical regression analysis, the presence of a caregiver (β=.27, p=.005) and alcohol drinking (β=-.19, p=.037) were found to be significant factors in model 1, explaining 14.0% of the variance in self-care compliance (F=6.88, p<.001). In Model 2, which incorporated health literacy and physical activity, both variables exhibited significantly positive regression coefficients (health literacy: β=.33, p<.001; physical activity: β=.32, p=.001). These two variables added 20.0% to the explanatory power, and the three variables, including alcohol drinking, accounted for 34.0% of the total variance in self-care compliance (adjusted R2=0.34, F=12.00, p<.001) (Table 5).
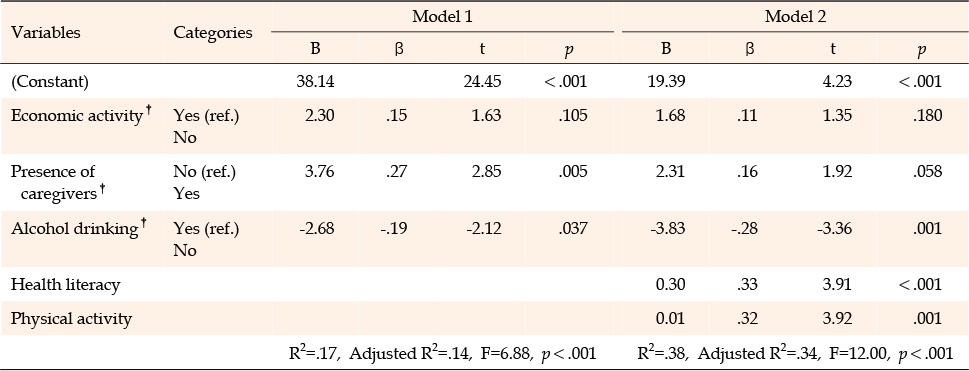
Table 5
Hierarchical Multiple Regression Analysis on Factors Influencing Self-care Compliance (N=106)
This study investigated self-care compliance in older male patients with chronic HF and aimed to identify the influence of health literacy, physical activity, and grip strength on their self-care compliance. The average self-care compliance score for patients with chronic HF was 42.21 (out of 60), which is substantially higher than the score of 33.2 observed in other chronic HF patients [21]. In this study, medication adherence and influenza vaccination rates were notably high, whereas weight monitoring exhibited the lowest compliance, as indicated by the EHFScBS items. This contrasts with previous research suggesting that the majority of HF patients exhibit the lowest levels of exercise [7]. This discrepancy may be attributed to the fact that the participants were retired veterans who benefited from various forms of social support. There was no reported burden associated with influenza vaccinations, treatments, or hospital visits. The literature suggests that self-care compliance may be lower in men than in women [22]. Studies indicate that social support and self-care confidence are crucial factors influencing self-care in male patients [23], which corresponds with the high levels of self-care observed among the participants in our study. Monitoring symptoms based on self-care compliance levels is vital for prognosis, highlighting the importance of nursing interventions to improve these behaviors. Self-care may be influenced by the perceived need and the long-term nature of the behavioral changes required [1]. Therefore, understanding these influences on self-care compliance is critical for developing effective nursing interventions.
A hierarchical multiple regression analysis indicated that health literacy, physical activity, and alcohol consumption significantly influenced self-care compliance in older male patients with chronic HF. The observation that self-care compliance was higher among participants who abstained from alcohol aligns with previous research, which found elevated levels of self-care compliance among older HF patients who did not consume alcohol [15]. In this study, approximately one-quarter of the participants reported drinking more than once a week, suggesting a need for health education on alcohol abstinence and enhanced monitoring of self-care practices among heavy drinkers in outpatient nursing practice.
Health literacy significantly affected self-care compliance in this study, consistent with previous studies on older adults with HF [10] and patients with diabetes [24]. Shin et al. [25] focused on older adults with chronic HF and observed a generally low level of health literacy. Prior research on cardiovascular patients has demonstrated their ability to gather and understand essential information through health literacy [26]. Effective HF treatment and the prevention of adverse outcomes necessitate patient engagement and access to reliable health information [2]. Patients must understand advice and health information to develop adequate self-care skills, as health literacy has been associated with both the capability and interest in engaging in self-care behaviors [9, 26]. A study on HF patients [27] highlighted the significant impact of education and perceived control on self-care compliance. Tailoring health literacy management to consider age and cognitive type is crucial for improving self-care compliance. Our findings strongly suggest that health literacy is a key factor in self-care compliance among HF patients.
Physical activity was identified as a significant factor influencing self-care compliance in this study. This observation is consistent with research on physical activity among octogenarians in living care facilities, which shows a correlation between activity time and self-care [28]. The participants in this study demonstrated higher levels of physical activity compared to those in a previous study involving older adults with HF [29]. This difference may be due to the fact that all participants were classified as NYHA classes I to II, reflecting relatively mild HF severity, and had been diagnosed with HF for an average of three years. Higher levels of physical activity have been associated with a significant decrease in HF risk [30], underscoring the potential benefits of promoting physical activity in HF prevention. The physical activity level of patients with chronic HF often changes due to complex symptoms and the effects of aging [10], which can pose challenges to maintaining self-care compliance. Consequently, it is crucial for healthcare providers to regularly monitor the physical abilities of patients throughout their treatment to address any declines in activity levels. Developing nursing interventions that encourage effective physical activity strategies is vital for improving self-care compliance.
No significant correlation was observed between grip strength and self-care compliance in this study. In contrast, a study on stroke patients found that grip strength was a major predictor of self-care compliance, particularly in relation to physical symptoms and daily living activities [31]. Stroke often results in muscle paralysis or impaired bodily functions, which can hinder self-care abilities. However, the patients in this study, being veterans, generally maintained moderate to high levels of physical activity and possessed good physical capabilities, which likely mitigated such effects. The average grip strength recorded in this study was 25.7 kg, compared to 26.5 kg in a previous study involving older French male adults with HF [32]. Given the demographic differences, the grip strength observed in this study was somewhat lower. This suggests that self-care compliance may be influenced by a variety of factors beyond just grip strength. Future research should aim to elucidate the impact of grip strength on self-care compliance and explore the mechanisms underlying this relationship.
The significance of this study lies in its use of physical activity and grip strength as indicators of physical health influencing self-care compliance. We confirmed that physical activity impacted self-care compliance in older male patients with chronic HF. Additionally, the study is noteworthy for its use of a newly developed health literacy tool that incorporated characteristics specific to patients with cardiovascular disease and the roles of patients with chronic diseases, such as information utilization and communication skills with medical staff. However, the study has several limitations. First, the sample was drawn from a single medical institution and consisted only of older male veterans, which limits the generalizability of the findings to other HF patients. Second, health literacy, physical activity, and self-care compliance were evaluated using self-reported measures, which may have introduced errors based on participants' interpretations. Therefore, future research should aim to overcome these limitations by increasing the sample size and ensuring consistent and thorough data collection methods.
In this study of older male patients with chronic HF, not drinking alcohol, higher health literacy, and higher physical activity were found to positively influence self-care compliance. It is necessary to periodically evaluate these characteristics in outpatient nursing practice and provide educational interventions to increase patients' self-care compliance. In addition to assessing grip strength, future research could explore the influence of overall physical fitness, exercise capacity, and engagement in specific physical activities on self-care compliance in older male patients with chronic HF.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conceptualization and design acquisition - MSM and HSY.
Data collection, data analysis & drafting - MSM.
Critical review and editing, supervision - HSY.
This paper is part of the first author's master's thesis from Hanyang University Graduate School of Clinical Nursing.
 E-SUBMISSION
E-SUBMISSION