
Purpose
This study aims to identify factors affecting the Health-Related Quality of Life (HRQoL) in patients with atrial fibrillation.
Methods
The study subjects were 158 outpatients with atrial fibrillation at a university hospital in Metropolitan City B. Data were collected from March 18, 2022 to July 1, 2022 and were analyzed using descriptive statistics, independent t-test, one-way ANOVA, Pearson’s correlation coefficient, and hierarchical multiple regression with SPSS 22.
Results
Self-management behaviors (β=.27, p<.001), self-efficacy (β=.30, p<.001), and grit (β=.33, p<.001) were found to have statistically significant effects on HRQoL. Hierarchical regression analysis showed that age, employment status, and monthly household income explained 23.6% of the variance in HRQoL, while subjective health status and perceived stress added 18.6% of the variance. Self-management behaviors, self-efficacy, and grit had an explanatory power of 32.4%, and the overall explanatory power was 74.6%.
Conclusion
Self-management behaviors, self-efficacy, and grit were identified as factors affecting HRQoL in patients with atrial fibrillation. These results will be used as important fundamental data to develop nursing interventions in order to improve the HRQoL of patients with atrial fibrillation.
This study aims to identify factors affecting the Health-Related Quality of Life (HRQoL) in patients with atrial fibrillation.
The study subjects were 158 outpatients with atrial fibrillation at a university hospital in Metropolitan City B. Data were collected from March 18, 2022 to July 1, 2022 and were analyzed using descriptive statistics, independent t-test, one-way ANOVA, Pearson’s correlation coefficient, and hierarchical multiple regression with SPSS 22.
Self-management behaviors (β=.27, p<.001), self-efficacy (β=.30, p<.001), and grit (β=.33, p<.001) were found to have statistically significant effects on HRQoL. Hierarchical regression analysis showed that age, employment status, and monthly household income explained 23.6% of the variance in HRQoL, while subjective health status and perceived stress added 18.6% of the variance. Self-management behaviors, self-efficacy, and grit had an explanatory power of 32.4%, and the overall explanatory power was 74.6%.
Self-management behaviors, self-efficacy, and grit were identified as factors affecting HRQoL in patients with atrial fibrillation. These results will be used as important fundamental data to develop nursing interventions in order to improve the HRQoL of patients with atrial fibrillation.
Atrial fibrillation is the most common arrhythmia characterized by irregular and rapid atrial contractions caused by electrical impulses in various parts of the atria [1]. According to the National Health Insurance Service's healthcare data, the number of people treated for atrial fibrillation (disease code I48) was 244,896 in 2020, an increase of 35.3% compared to 189,954 in 2016. Risk factors for atrial fibrillation include advanced age, male sex, coronary heart disease, diabetes, lung disease, hyperthyroidism, and electrolyte imbalances. It can commonly be triggered by mental stress, surgery, exercise, and alcoholism, even in normal individuals [2]. Patients with atrial fibrillation are often not recognized for the wide range of causative factors and symptoms associated with the disease. Consequently, they may miss the treatment or develop life-threatening complications such as stroke, hemorrhage, and uncontrolled arrhythmias, leading to readmissions that create social and economic burdens [1]. They have been reported to have a very poor quality of life, related to health, due to the nature of this condition, which not only causes physical and mental stress in itself but also impairs their daily and social life [3, 4]. Health-Related Quality of Life (HRQoL) is a subjective assessment of physical, mental, and social health [5]. The HRQoL of patients with atrial fibrillation has been found particularly poor compared to those with heart failure or other cardiac conditions [6], requiring active management.
For optimal treatment and management, patients with atrial fibrillation should have ongoing self-management, including monitoring signs and symptoms of atrial fibrillation, adhering to prescribed medications, monitoring for side effects, keeping appointments, and managing food and drug interactions when taking warfarin [7]. Self-management is an activity undertaken by an individual to maintain their life, health, and well-being. It involves the patient being an active participant, taking responsibility for managing their own health issues, learning the necessary knowledge and skills, and practicing healthy behaviors on their own [8]. The Korean Heart Rhythm Society reported that by presenting a clinical model of integrated practice guidelines for the treatment of atrial fibrillation [1] and performing self-management activities to maintain and improve a healthy lifestyle, subjects can manage symptoms, reduce fatal complications, maintain a sense of mental well-being, and reduce the likelihood of permanent atrial fibrillation, thereby, contributing to the increased quality of life [8, 9].
Self-efficacy, one of the key determinants of self-management, is the degree of confidence in one's ability to selectively mobilize the behavioral, cognitive, and emotional resources necessary to successfully perform a task and to execute and organize some kind of action [10]. Such resources include accomplishment experiences, vicarious experiences, verbal persuasion, and emotional arousal, all of which can be utilized as self-efficacy methods [10]. As the importance of self-efficacy in changing human behavior and sustaining the change has emerged [11], many studies in Korea have investigated the relationship between self-efficacy and HRQoL in patients with chronic diseases [11, 12]; however, it was difficult to find domestic studies on self-efficacy and HRQoL in patients with atrial fibrillation.
While atrial fibrillation may not be immediately recognized as a life-threatening condition by family, friends, or co-workers, patients' symptoms and concerns are often ignored [9], and even in clinical settings, it has been documented that patients have difficulty receiving the information and emotional support that they need for self-management [9, 13]. It has been shown that social support is a positive resource derived from the relationships surrounding an individual, which strengthens the individual's ability to overcome psychosocial difficulties or setbacks [14]. A study further provides evidence that higher levels of social support among chronically-ill patients facilitate the acquisition of disease-related materials and improve their ability to cope with the disease and, thus, their quality of life [12]. Patients with atrial fibrillation also suffer from a combination of physical and psychological difficulties due to disease-related characteristics [13]; however, thus far, domestic studies confirming the relationship between social support and the HRQoL in patients with atrial fibrillation are lacking [13, 15].
With the recent focus on positive psychology, grit has gained attention in the literature as a concept that is highly related to career, job, academic success, and happiness in life [16]. Grit refers to the passion and effort to achieve short- and long-term goals despite any setbacks or adversity and is considered an important trait with respect to measuring the quality of life [16]. People with high levels of grit are significantly more likely to achieve their personal goals than those with less grit [16]. They also have a more optimistic outlook, view small successes as victories, and have a positive life attitude rather than giving in to despair. In addition, people with higher levels of grit are more likely to successfully reenter life roles despite a diagnosis of atrial fibrillation. However, despite this attention to grit, previous studies have focused on students and educational areas [16], and domestic research on grit in clinical practice in Korea is scarce. To improve our understanding of grit and explore its potential application to HRQoL in patients with atrial fibrillation, it is, thus, important to examine the relationship between the two.
HRQoL in patients with atrial fibrillation has been studied to present various factors. General characteristics include age [2, 3, 4, 15], gender [4, 6, 17], occupation [2], and household income [3, 15], while disease-related characteristics have been reported to include symptom experience [2] and frequent hospitalizations [3, 9]. Psychological factors have been reported to include uncertainty [3, 18], depression [3, 15, 18], anxiety [3, 15, 18], and stress [9], whereas social factors include social support [13, 15]. However, these studies are limited to focusing on the symptom experience of the subjects or confirming the relevance or causality of some of the factors, making it difficult to apply them to develop nursing intervention strategies in order to improve the HRQoL of patients with atrial fibrillation. Against this backdrop, this study attempted to identify various factors influencing the HRQoL of patients with atrial fibrillation and provide fundamental data to develop nursing intervention programs to improve it.
This study aims to identify the extent of self-management behaviors, self-efficacy, grit, social support, and HRQoL in patients with atrial fibrillation and to determine the relationship between these variables and the impact of self-management behaviors, self-efficacy, grit, and social support on HRQoL.
This is a cross-sectional descriptive study to identify the impact of self-management behaviors, self-efficacy, grit, and social support of the patients with atrial fibrillation on their HRQoL.
The subjects of this study were patients aged 20 years or older who were diagnosed with atrial fibrillation and receiving outpatient treatment in the cardiology department of a university hospital in Metropolitan City B; they understood the purpose of the study and voluntarily agreed to participate in it. In particular, inclusion criteria were those who had been diagnosed with primary atrial fibrillation with normal ventricular function for more than three months [2] and those who could understand the questionnaire. Those diagnosed with mental illness (schizophrenia, dementia, etc.) or taking medications related to mental illness were excluded.
The G*Power 3.1.9.7 program was used to calculate the appropriate sample size for the multiple regression analysis. Based on a significance level of 0.05, a medium effect size of 0.15 [3, 14], a power of 0.80 [3], and 20 predictors (8 general characteristics, 8 disease-related characteristics, self-management behaviors, self-efficacy, social support, and grit), the required sample size was 157; considering a 10% dropout rate, 173 questionnaires were distributed. After excluding 15 non-responses, a total of 158 responses were used for statistical analysis.
This study was approved by the Institutional Review Board (IRB) of the investigator's institution (IRB No. 2203-006-112) and conducted in accordance with its procedures. An informed consent form was obtained from the nursing department, and permission was obtained from the attending physician prior to data collection. The participants were asked to sign a written consent form stating the purpose of the study, their voluntary participation, the confidentiality of their responses, and that their responses would not be used for any purpose other than the study. The questionnaires were kept in an envelope and not disclosed.
Based on previous studies [2], general characteristics consisted of eight questions including age, gender, cohabitation, education, occupation, monthly household income, alcohol consumption, and smoking status. Disease-related characteristics included eight questions based on previous studies [14] and comprised the duration of atrial fibrillation diagnosis, type of atrial fibrillation, number of hospitalizations for atrial fibrillation, number of comorbidity, type of comorbidity, stroke risk (CHA2DS2-VASc), type of anticoagulant/antiplatelet medication, subjective health status, and perceived stress. Stroke risk (CHA2DS2-VASc) was assigned 1 point each for congestive heart failure, hypertension, diabetes mellitus, vascular disease, and female sex, 2 points for previous stroke, and 2 points for those aged 75 years or older and 1 point for those aged 65 to 74 years, with a combined score of 0, 1, and 2 or more being low, intermediate, and high risk, respectively [1].
To measure self-management behaviors, the self-management behaviors tool developed by Jeon and Park [19] for cardiac patients taking anticoagulants, and modified and supplemented by Oh [20] for patients with atrial fibrillation, was used with permission from the respective authors. The tool comprises 4 subscales, each with 20 questions: 5 questions on medication, 7 questions on lifestyle, 3 questions on physical activity, and 5 questions on symptom monitoring. Each question is scored on a 5-point Likert scale ranging from 1 "not at all" to 5 "very much so," with a minimum of 20 and a maximum of 100, and higher scores indicate higher self-management behaviors. Cronbach's α was 0.84 in Jeon and Park's [19] study, 0.87 in Oh's [20] study, and 0.78 in this study, respectively.
Self-efficacy was measured with the Korean Adaptation of the General Self-Efficacy Scale (K-GSES), a Korean version of the General Self-Efficacy Scale (GSES) developed by Jerusalem and Schwarzer [21]. The K-GSES is available for use on Schwarzer's official website (http://userpage.fu-
Social support was measured using the Multidimensional Scale of Perceived Social Support developed by Zimet et al. [22] and adapted by Shin and Lee [23], with permission from the authors and adapters. The tool consists of 12 questions in 3 domains measuring family support, friend support, and support from significant others (healthcare providers). Each question is answered on a 5-point Likert scale ranging from 1 "not at all" to 5 "very much so," with a minimum of 12 and a maximum of 60, and higher scores indicate greater social support. At the time of development [22], the tool's reliability Cronbach's α was 0.85; it was 0.89 in a study by Shin and Lee [23], and in this study, it ranged from 0.88 to 0.91 for the subscales and 0.93 overall.
Grit was measured using the Short Grit Scale (Grit-S) developed by Duckworth et al. [16] and adapted by Kang et al. [24], validated by experts, with permission from the authors and adapters. This instrument consists of 4 items each for Consistency of Interest (CI) and Perseverance of Effort (PE). Of the subscales, CI measures the degree of difficulty in maintaining the interest needed to accomplish a goal (e.g., "I find it difficult to keep working hard at something that takes a long time"), reverse-coding each item. PE measures the degree to which a person sticks to their goals in the face of hurdles, failures, and hardships (e.g., "I finish what I start"). Each statement is rated on a 5-point Likert scale, ranging from 1 "not at all" to 5 "very much so," with minimum and maximum scores of 8 and 40, respectively, and higher scores indicate higher grit. At the time of development [16], the tool's reliability Cronbach's α was 0.78 for the CI, 0.84 for the PE, and 0.73 for the overall, respectively, while it ranged from 0.70 to 0.81 in the study by Kang et al. [24] and from 0.70 to 0.73 in our study.
For HRQoL, we used the Korean version of the Medical Outcomes Study Short Form-36 (SF-36) developed by Ware and Sherbourne [25] and tested for reliability and validity by Koh et al. [26]. This is a 36-item instrument consisting of domains of physical functioning, social functioning, physical role functioning, emotional role functioning, mental health, vitality, pain, general health status, and health status change. Of the total 36 questions, 35 questions are used for scoring, except for a single question that asks about the change in general health status over the past year. Each question scored in each domain is summed ranging from 0 to 100, with higher scores indicating higher HRQoL. It is calculated as a score from 0 to 100 points using the developer's formula, and it is also possible to calculate the score for each area. Higher scores indicate higher HRQoL. At the time of development [25], the tool's reliability Cronbach's α ranged from 0.84 to 0.95, and in this study, it ranged from 0.70 to 0.93.
The data for this study were collected from March 18 to July 1, 2022. A recruitment notice was posted in the outpatient department of cardiology at a university hospital in Metropolitan City B. Patients who voluntarily agreed to participate in the study and met the inclusion criteria were explained the purpose of the study. Subsequently, written consent was obtained, and a structured questionnaire was administered. If the subjects had difficulty completing the questionnaires themselves, the questionnaires were read to them and completed by the researcher, and the data on their disease-related characteristics were collected through questionnaires and medical records. The explanation of the research process and the completion of the questionnaire were conducted in a separate room, and the questionnaire took about 15 minutes to complete.
The data collected in this study were analyzed using the SPSS/WIN 22.0 statistical program. The general and disease-related characteristics of the subjects were calculated as real numbers, percentages, means, and standard deviations and were accordingly analyzed by independent t-test, one-way ANOVA, and post hoc test with Scheffé test to determine the differences in HRQoL. The subjects' self-management behaviors, self-efficacy, social support, grit, and HRQoL were calculated as means and standard deviations, and the relationship between the subjects' HRQoL and the variables was analyzed by Pearson's correlation coefficient. The variables that were significant at the level of significance <.05 in the univariate analysis were subjected to hierarchical multiple regression to determine the relative influence of general and disease-related characteristics and key variables on HRQoL [3].
The average age of the subjects was 61.01 years, and 105 (66.5%) were male. In addition, 129 (81.6%) of them lived with their families, and 62 (39.2%) had a high school education. Of all the subjects, 99 (62.7%) were employed, and 67 (42.4%) had a monthly household income of more than 4 million won. Furthermore, 108 (68.4%) did not drink alcohol, and 131 (82.9%) did not smoke (Table 1).
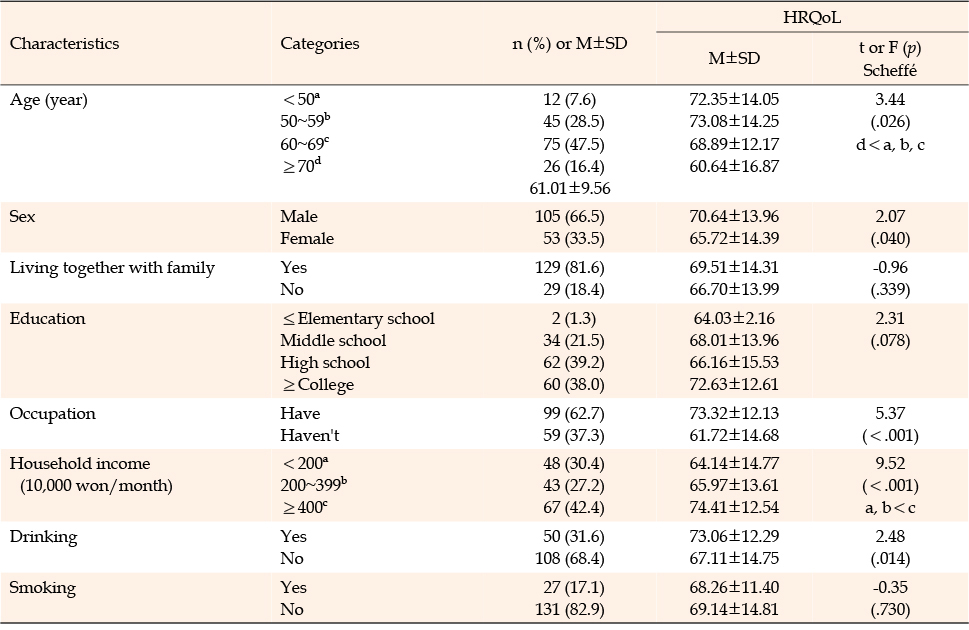
Table 1
Differences in Health-related Quality of Life according to General Characteristics (N=158)
There were significant differences in the HRQoL according to the general characteristics of the subjects: age (F= 3.44, p=.026), gender (t=2.07, p=.040), occupation (t=5.37, p<.001), monthly household income (F=9.52, p<.001), and alcohol consumption (t=2.48, p=.014). In other words, the HRQoL was higher if the subjects were male, had a job, and drank alcohol. As for the age, subjects under the age of 70 had higher HRQoL than other age groups, and those with a monthly household income of 4 million won or more had significantly higher HRQoL than those without (Table 1).
The duration of atrial fibrillation was more than 1 year to less than 5 years in 82 (51.9%) subjects. The type of atrial fibrillation was permanent in 96 (60.8%), persistent in 18 (11.4%), and paroxysmal in 44 (27.8%). Of all the subjects, 51 (32.3%) had been hospitalized for atrial fibrillation in the past, with an average of 0.54 hospitalizations, and 130 (82.3%) had comorbidities, including duplicate responses: 70 (54.3%) had hypertension, 43 (33.3%) had dyslipidemia, and 35 (27.1%) had diabetes. In addition, 80 (51.0%) had stroke risk, which was high. The most common anticoagulant used was vitamin K-independent oral anticoagulants with 106 (67.1%), followed by antiplatelet agents with 10 (6.3%) and vitamin K antagonists with 5 (3.2%). The mean subjective health status was 3.04±0.83 out of 5, with 83 (52.5%) fair, 36 (22.8%) good, and 28 (17.7%) poor, respectively. Perceived stress averaged 2.83±0.77 out of 5, with 85 (53.8%), 44 (27.8%), and 21 (13.3%) reporting moderate, low, and high, respectively (Table 2).
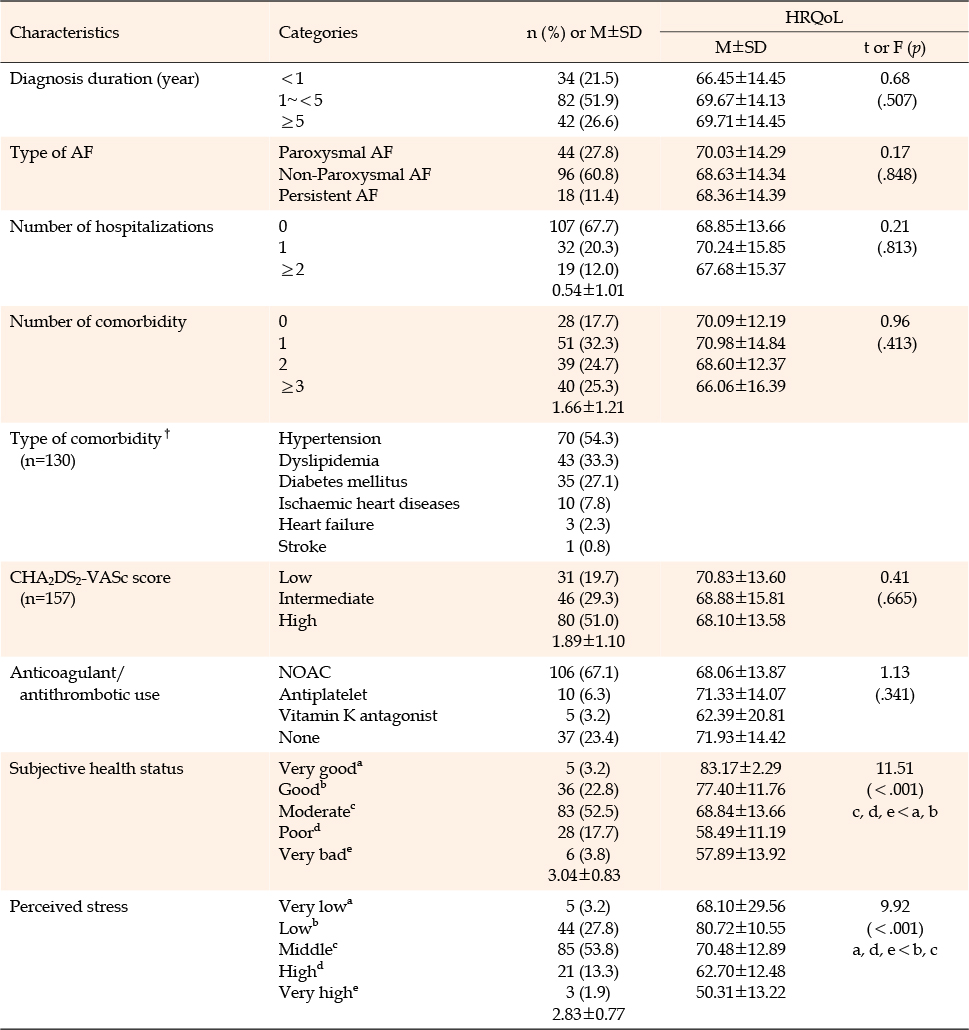
Table 2
Differences in Health-related Quality of Life according to Disease Characteristics (N=158)
The subjects' self-management behaviors averaged 76.91±8.96 out of 100, self-efficacy averaged 29.92±3.82 out of 40, social support averaged 48.63±8.52 out of 60, and grit averaged 27.31±3.77 out of 40. HRQoL averaged 68.99±14.25 out of 100 (Table 3).
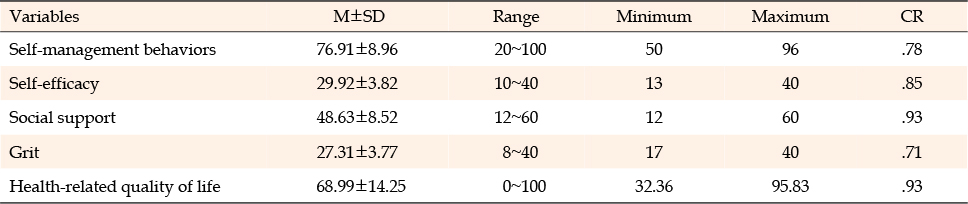
Table 3
Degree of Self-management Behaviors, Self-efficacy, Social Support, Grit, and Health-related Quality of Life (N=158)
Among the subjects' disease-related characteristics, subjective health status and perceived stress were significantly correlated with HRQoL; better subjective health status (r=.47, p<.001) and lower perceived stress (r=-.41, p<.001) were associated with higher HRQoL (Table 4).
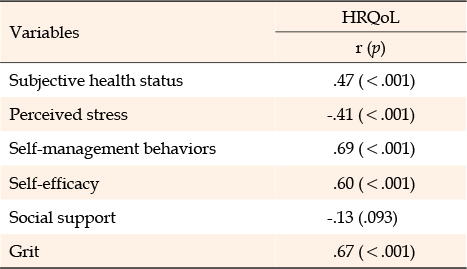
Table 4
Correlations among Subjective Health Status, Perceived Stress, Self-management Behaviors, Self-efficacy, Social Support, Grit, and HRQoL (N=158)
Subjects' self-management behaviors, self-efficacy, and grit were significantly correlated with HRQoL. In other words, higher self-management behaviors (r=.69, p<.001), higher self-efficacy (r=.60, p<.001), and higher grit (r=.67, p<.001) were associated with higher HRQoL. However, social support was not significantly correlated with HRQoL (r=-.13, p=.093) (Table 4).
Hierarchical multiple regression, an analysis method that controls the order of entry of a series of independent variables, was used to explore factors influencing the subjects' HRQoL. Prior to the analysis, we checked for multicollinearity. The tolerance values ranged from 0.47 to 0.90, all of which were above 0.1, and the Variation Inflation Factor (VIF) values ranged from 1.11 to 2.11, all of which were below 10, indicating no multicollinearity problems. In addition, the Durbin-Watson value was 2.09, which was close to 2, indicating no autocorrelation problem, and the residual analysis results showed that the model satisfied linearity, normality, and equidispersion.
Univariate analysis showed that age (β=-.18, p=.016), gender (β=.26, p=.001), occupation (β=.20, p=.010), and monthly household income (β=.20, p=.010) were significant factors when entered as dummies for age, gender, occupation, monthly household income, and alcohol consumption, which were significantly different from the HRQoL among general characteristics, with an explanatory power of 23.6% (F=9.37, p<.001). Step 2 was a model that added subjective health status and perceived stress, that is, two of the disease-related characteristics that were significantly correlated: subjective health status had a positive regression coefficient (β=.28, p<.001), whereas perceived stress had a negative regression coefficient (β=-.25, p<.001), with 18.6% additional explanatory power (F= 24.08, p<.001) while controlling for other factors. Finally, when self-management behaviors, self-efficacy, and grit, which were significantly correlated among the main variables, were entered as a third level while controlling for other factors, self-management behaviors (β=.27, p<.001), self-efficacy (β=.30, p<.001), and grit (β=.33, p<.001), all showed significant positive regression coefficients; the explanatory power of Model 3 was 32.4% (F=62.42, p<.001). The total explanatory power of these variables in the final model was 74.6% (Table 5).
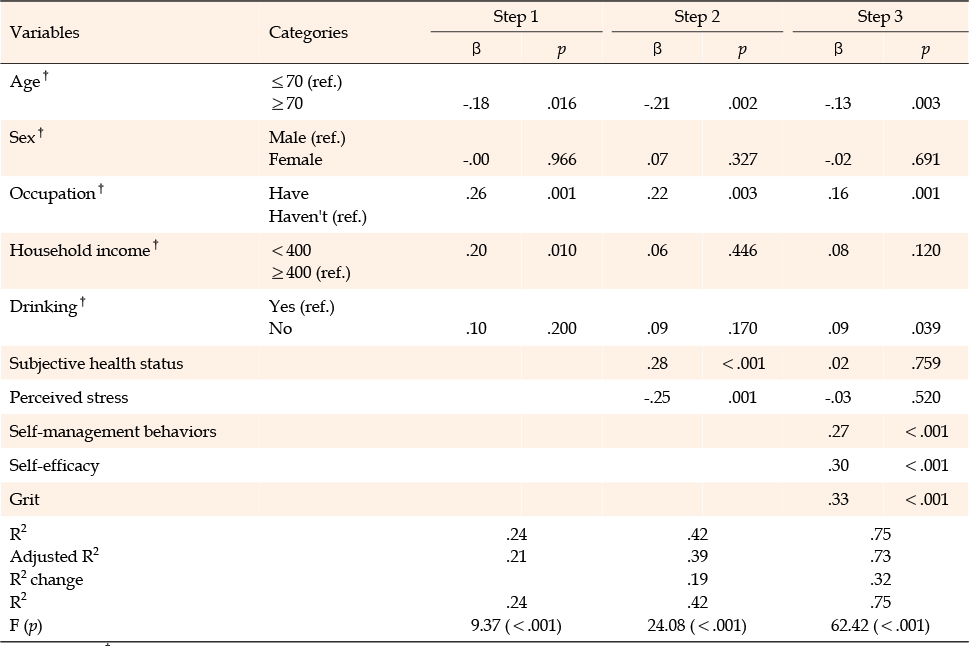
Table 5
Factors affecting to the HRQoL (N=158)
This study aimed to identify factors that affect the HRQoL of patients with atrial fibrillation and to provide a basis to develop nursing interventions to improve the HRQoL of such patients.
The mean score for subjective health status was 3.04 (out of 5), with 52.5%, 22.8%, and 17.7% in fair, good, and poor status, respectively. This is in line with the results of a study by Kim et al. [14] in which patients with atrial fibrillation were found to be in fair (44.0%), good (26.9%), and poor (20.8%) health, which can be considered slightly higher than average. The mean score for perceived stress was 2.83 (out of 5), with moderate (53.8%), low (27.8%), and high (13.3%). This is similar to the moderate (54.8%), low (22.7%), and high (22.6%) scores reported by Kim et al. [27] in their study of hypertensive patients. The mean score of self-management behaviors was 76.91, which is not substantially different from the score of 82.45 in a study by Kim et al. [14] using the same tool for patients with atrial fibrillation and that of 79.52 in an experimental group before an educational program to promote self-management in a study by Oh [20]. Self-efficacy was 29.92 (2.99 on a 4-point scale), which was comparable to the self-efficacy scores of patients with chronic liver disease at 28.99 [12] and that of hemodialysis patients at 2.77 [11]. Social support averaged 48.63, which was somewhat higher than the score of 43.28 for patients with chronic liver disease [12] and that of 43.60 for patients with atrial fibrillation [14]. These findings are likely due to differences in demographic characteristics rather than disease-specific characteristics of the study subjects; those with higher economic status and having a caregiver have reported higher levels of social support, which confirms our findings [28]. In other words, 81.6% of the subjects in this study were living with their families, and 42.4% had a monthly household income of more than 4 million won, indicating a relatively stable social and economic status. The mean grit score for patients with atrial fibrillation was 3.41, similar to that of patients with Parkinson's disease [29] and multiple sclerosis [30], at 3.65 and 3.8, respectively. This shows that not only patients with neurological dysfunction requiring rehabilitation but also patients with atrial fibrillation need lifelong management; thus, the high level of enthusiasm and persistence possessed by the subjects is a key factor for disease management. Therefore, the role and support of nurses seem to be important for increasing the grit level of patients with atrial fibrillation. The mean HRQoL was 68.99 out of 100, which was higher than the scores of 40.20 to 61.38 in studies that used the same instrument to determine the HRQoL of patients with atrial fibrillation [2, 3, 15]. This difference may be because the patients in the previous studies had lower household income [2, 3, 15], while the number of subjects with no job [2] and the number of hospitalization [3] were smaller than the subjects in our study.
The correlation analysis between the main variables of this study showed that HRQoL was significantly and positively correlated with self-management behaviors, self-efficacy, and grit. Among these variables, self-management behaviors showed the highest correlation, as self-management behaviors were identified as the most influential factor in the quality of life in elderly colorectal cancer patients [31], supporting the results of the present study. As the survival period of cancer patients has extended, self-management has become important for managing chronic diseases, including atrial fibrillation, which needs to be managed for life.
However, the results showed no significant correlation between social support and HRQoL. This is in agreement with a study [15] that reported that social support in patients with atrial fibrillation was not a factor in HRQoL. The HRQoL of patients with atrial fibrillation, who have less life-threatening conditions, seems to be influenced by internal factors such as symptom perception, ability to perform activities of daily living, subjective health status, and perceived stress rather than external factors such as social support. In addition, a study of middle-aged and elderly people in rural areas [32] reported that social support had no direct but significant indirect effect on HRQoL, mediated by self-efficacy. However, our results differed from a study that reported that patients with atrial fibrillation, who had sufficient social support, could cope better with their disease by obtaining a variety of information from themselves and others and had lower levels of depression, which positively affected their mental HRQoL [13]. Accordingly, further research is needed to clarify how social support affects HRQoL and through which pathways.
A hierarchical regression analysis to identify factors affecting HRQoL in patients with atrial fibrillation revealed that among general characteristics, age, occupation, and monthly household income were significant factors at Step 1. In the case of age, subjects in their 70s and older had lower HRQoL than other age groups. This is consistent with studies that have reported lower HRQoL in patients with atrial fibrillation aged 65 years or older or 70 years or older [2, 3, 15], suggesting that HRQoL is lower in older adults. By gender, men had higher HRQoL than women. This is in accordance with studies of patients with atrial fibrillation [6, 17], as well as studies of HRQoL in the Korean population as a whole [33], and is thought to be related to socioeconomic rather than disease characteristics. It was also reported that the quality of life of hemodialysis patients [11] was significantly different according to occupation and monthly household income, which supported the present study. Occupation and monthly household income are related to economic status, and the burden of healthcare costs for chronic patients can differ depending on economic status; thus, this study indicates that intervention strategies should be developed differently depending on economic status to improve the HRQoL of chronic patients.
In Step 2, among disease-related characteristics, subjective health status and perceived stress were found to have a significant impact on HRQoL. Subjective health status is how patients with atrial fibrillation perceive their health; thus, if they feel positive about their health, they may be more likely to take care of their health, and if they feel negative, they may be more motivated to take care of their health [27]. As such, nurses should fully understand the subjective health status of patients with atrial fibrillation in order to enhance their HRQoL, utilizing their optimism if it is positive and their motivation to manage their own health if it is negative. Additionally, patients with atrial fibrillation experience unpredictable and variable symptoms that make healthcare difficult, change their social lives, limit their ability to exercise and achieve their goals, and cause them to experience stress and emotional distress, leading to a decreased quality of life [9]. It is, therefore, necessary for nurses to educate patients on the recognition of symptoms and risk factors for complications of atrial fibrillation, encourage and listen to patients with atrial fibrillation to freely express their thoughts and feelings, and organize self-help groups or provide tailored individual interventions as needed.
In the final step, among the variables that were significantly associated with HRQoL, self-management behaviors, self-efficacy, and grit were identified as influential factors. This was consistent with the findings that higher levels of self-management were associated with a higher quality of life in patients with inflammatory bowel disease [28] and that self-efficacy significantly influenced the quality of life in patients with chronic liver disease [12]. Self-management behaviors and self-efficacy are known to have direct and indirect effects on patient outcomes. To ensure that patients with atrial fibrillation can lead normal lives despite experiencing symptoms throughout their lives, they must engage in self-management, take an active role in their disease management and be responsible for achieving an adequate level of well-being, and nurses must provide support to promote their self-management skills. In patients with atrial fibrillation, self-efficacy is the perceived confidence in one's ability to perform health-related behaviors, such as medication, diet, and exercise, and is an important factor in selecting and sustaining healthy behaviors. The self-efficacy of patients with atrial fibrillation should be improved through interventions that help them learn specific ways to manage their atrial fibrillation symptoms and strengthen their confidence, promoting self-management behaviors.
This study found that grit levels in patients with atrial fibrillation had the highest β value of 0.33, making it a very important factor for HRQoL. Grit is correlated with quality of life, particularly with the mental quality of life domain [29]. In a study of Parkinson's patients [29], subjects with higher levels of grit had higher emotional coping responses, exercised more, and were more confident than those with less grit. Even in patients with multiple sclerosis [30], subjects with high levels of grit reported higher HRQoL. In addition, they had higher psychological wellbeing due to their drive to face and overcome challenges [30]. Grit also affected their level of social functioning, with a stronger tendency to discover and learn about their disease through meaningful experiences and social connections [30]. As grit is a trait that can be learned, nurses should play a leadership role in improving HRQoL by continuously communicating and supporting patients with atrial fibrillation to promote this trait. This study is significant for finding out that grit has a positive impact on the HRQoL of patients with atrial fibrillation.
Consequently, this study distinguishes itself from previous studies by examining the relative magnitude of the impact of general and disease-related characteristics and psychosocial factors that may affect the HRQoL of patients with atrial fibrillation through hierarchical regression analysis. If we continue to explore strategies to identify and increase levels of grit and self-efficacy to improve HRQoL in patients with atrial fibrillation based on our findings, it will be possible to improve health outcomes for such patients. Despite the significance of this study, it is limited because of being conducted in a single geographic region and not accounting for differences in site diversity or regional characteristics.
This study identified self-management behaviors, selfefficacy, and grit as factors affecting the HRQoL in patients with atrial fibrillation. These results will be used as important fundamental data to develop nursing interventions in order to improve the HRQoL of patients with atrial fibrillation. Based on our findings, we make the following suggestions: First, this study was conducted only on patients with atrial fibrillation visiting a single university hospital; thus, there are limitations to generalizing the results, and the study must be conducted again with a larger number of patients. Second, to ensure consistency in the findings on social support and HRQoL, further research is needed to identify the pathways through which social support affects HRQoL. Finally, future researchers would benefit from developing specific and realistic nursing intervention strategies and verifying the effects to improve self-management behaviors, self-efficacy, and grit to promote the HRQoL among patients with atrial fibrillation.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - S-JY and L-HO.
Data collection - S-JY and L-HO.
Analysis and interpretation of the data - S-JY and L-HO.
Drafting and critical revision of the manuscript - S-JY and L-HO.
 E-SUBMISSION
E-SUBMISSION