
Purpose
This study aimed to verify the potential use of postoperative pulmonary complications prediction models in patients with lung resection.
Methods
In this retrospective study, 1,160 patients were selected among the admitted patients who underwent lung resection surgery. The predictive validity of the Assess Respiratory Risk in Surgical Patients in Catalonia Tool (ARISCAT) and the Pulmonary Complications Risk Score (PCRS)-lung resection model were assessed based on the sensitivity, specificity, positive and negative predictive values, and Area Under the receiver operating characteristic Curve (AUC).
Results
Of the patients, 420 (36.2%) developed postoperative pulmonary complications after lung resection surgery within 30 days. The sensitivity, specificity, positive predictive values, and negative predictive values were 52.2%, 70.6%, 49.0%, and 74.0%, respectively, for the ARISCAT (cut-off point of 47), and 53.8%, 78.5%, 15.3%, and 95.9%, respectively, for the PCRS-lung resection model (cut-off point of 147). The AUCs were 0.65 (ARISCAT) and 0.70 (PCRS-lung resection model).
Conclusion
The findings indicate that the predictive validity values of the ARISCAT was sufficient, and the PCRS-lung resection model was good. However, the clinical usefulness of the models should be verified in future studies.
This study aimed to verify the potential use of postoperative pulmonary complications prediction models in patients with lung resection.
In this retrospective study, 1,160 patients were selected among the admitted patients who underwent lung resection surgery. The predictive validity of the Assess Respiratory Risk in Surgical Patients in Catalonia Tool (ARISCAT) and the Pulmonary Complications Risk Score (PCRS)-lung resection model were assessed based on the sensitivity, specificity, positive and negative predictive values, and Area Under the receiver operating characteristic Curve (AUC).
Of the patients, 420 (36.2%) developed postoperative pulmonary complications after lung resection surgery within 30 days. The sensitivity, specificity, positive predictive values, and negative predictive values were 52.2%, 70.6%, 49.0%, and 74.0%, respectively, for the ARISCAT (cut-off point of 47), and 53.8%, 78.5%, 15.3%, and 95.9%, respectively, for the PCRS-lung resection model (cut-off point of 147). The AUCs were 0.65 (ARISCAT) and 0.70 (PCRS-lung resection model).
The findings indicate that the predictive validity values of the ARISCAT was sufficient, and the PCRS-lung resection model was good. However, the clinical usefulness of the models should be verified in future studies.
Lung resection is a surgical procedure performed to treat a disease of the lungs such as malignant tumors, infection, and trauma, and is mainly applied as a surgical method for lung cancer [1]. As the incidence of lung cancer in Korea gradually increases every year from 21,358 in 2010 to 28,949 in 2020, the number of lung resections performed also rises [2, 3]. After lung resection, pulmonary function deteriorates due to the aftermath of anesthesia, loss of lung parenchyma due to surgery, pain, chest movement restriction, and inefficient bronchial secretion discharge [4, 5]. Poor respiratory function increases the risk of postoperative pulmonary complications [6, 7].
According to the European Perioperative Clinical Outcome (EPCO), Postoperative Pulmonary Complications (PPCs) refers to respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, and aspiration pneumonia [8]. However, previous studies and clinical practice have used various definitions [9, 10, 11]. The incidence of PPCs in patients undergoing thoracic surgery varies from 3% to 49% [12, 13], and that of pulmonary complications after lung resection was particularly high at 21.3% [14]. In Korea, the incidence of pulmonary complications in patients undergoing general surgery was 6.8% [15], and the incidence of pulmonary complications after lung resection was 14.1% [9].
PPCs contribute to negative outcomes such as increased postoperative morbidity and mortality and increased medical costs due to prolonged hospital stay [16]. Patients who develop PPCs suffer from deteriorating functional status, and one in seven patients are reported to have died in a hospital [17, 18]. Therefore, early identification of the risks of developing PPCs facilitates timely treatment and preventive interventions [18], reducing morbidity, mortality, and medical costs of the patients [19].
Currently, the Assess Respiratory Risk in Surgical Patients in Catalonia Tool (ARISCAT) is the most known tool for predicting PPCs [17], which is developed for patients who receive general anesthesia, spinal anesthesia, or local anesthesia for surgery. ARISCAT includes comprehensive PPCs such as respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, and aspiration pneumonia. ARISCAT is derived using variables that can be evaluated easily and objectively in clinical practice and are often used to validate other tools [12, 20, 21, 22]. The American College of Surgeons reported six types of surgery with a high incidence of PPCs (lung resection, laparotomy for abdominal aortic aneurysm, pancreatectomy, hepatectomy, esophagectomy, and laparotomy for aortic iliac artery repair) and developed six types of Pulmonary Complications Risk Scores (PCRS) [10] using National Surgical Quality Improvement Program (NSQIP), a large-scale surgical outcome database. One of these is the PCRS-lung resection model.
In a study that verified the validity of a predictive model for PPCs, Mazo et al. [23] confirmed the generalization of ARISCAT through a large-scale European cohort study but suggested that the model should be evaluated in other geographical environments. Azharuddin and Yunyongying [24] showed the application of ARISCAT to the US population without additional validation. Therefore, to use the predictive model for PPCs, it is necessary to verify its validity according to the geographical environment and population characteristics. However, although models for predicting PPCs are being continuously developed, external validation of predictive models other than ARISCAT [25] is insufficient, and the validity of the PCRS-lung resection model has rarely been reported.
In Korea, a few studies have verified the validity of predictive models for PPCs, except for one study [12] that compared predictive models for PPCs using ARISCAT and nutritional and inflammatory indices. Therefore, it is necessary to investigate the validity of a risk prediction model for PPCs in patients undergoing lung resection with a high incidence of PPCs.
To prevent the negative physical and economic effects of PPCs, which frequently occur in patients undergoing lung resection, it is essential to use a reliable predictive model through validation [26]. Therefore, this study aims to identify a predictive model for PPCs that can be suitably applied to domestic patients by evaluating and comparing the predictive validity of the PCRS-lung resection model and ARISCAT.
Identifying a predictive model for PPCs suitable for patients undergoing lung resection is crucial in nursing because it can contribute to developing evidence-based practice for cooperation and communication with medical staff, in addition to serving as basic data for practice and education, which nurses can use to establish a systematic patient assessment and nursing plan in clinical practice. In patients who have undergone lung resection, the primary goal of nursing is to prevent postoperative pulmonary complications. Therefore, screening of high-risk patients by applying objectively verified tools and early detection and prevention of PPCs through intensive monitoring and observation of risk factors will help improve the quality of nursing.
The purpose of this study is to determine the incidence of PPCs in patients who have undergone lung resection, and to identify a predictive model for PPCs with high predictive validity for these patients by evaluating the sensitivity, specificity, positive predictive value, negative predictive value, and Area Under the receiver operating characteristic Curve (AUC) of ARISCAT and PCRS-lung resection model.
This retrospective survey study used medical records to examine the incidence of PPCs in lung resection patients, and to suggest a predictive model for PPCs with high predictive validity for patients undergoing lung resection by comparing and analyzing the sensitivity, specificity, positive predictive value, negative predictive value, and AUC of ARISCAT and PCRS-lung resection model.
The study subjects were inpatients who underwent lung resection from May 1, 2018, to April 30, 2021, at a university hospital located in B city. The selection criteria for patients were those aged 18 years or older who had undergone wedge resection, segmentectomy, lobectomy, or pneumonectomy, excluding patients undergoing surgery other than lung resection during hospitalization, patients diagnosed with pneumonia before surgery, and patients experiencing PPCs 30 days after surgery. The number of inpatients who underwent lung resection during the study period was 1,216. The study excluded 21 patients under the age of 18, 29 patients who underwent surgery in addition to lung resection during hospitalization, one patient diagnosed with pneumonia before surgery, and five patients who experienced PPCs 30 days after surgery. There were no other missing data; therefore, 1,160 patients were included in the target population. According to the literature [27], the minimum sample size required for external validation of a predictive model is 100 events. Accordingly, considering that the incidence rate of PPCs in Korea was from 8.6% to 14.1% [9, 12], at least 710 and at most 1,163 patients were needed to collect data from 100 patients with PPCs. As the number of lung resections performed in this hospital for one year is about 400 times, 3-year data were collected and investigated.
Prior to conducting this study, approval (PNU IRB/2021_70_HR) was obtained from the Bioethics Committee of P University in B City, and medical record inquiry was approved through the hospital's office. For the data collected, a serial number was assigned to each subject's patient registration number to avoid identification of personal information. To prevent the leakage of research content, it was coded and stored in an encrypted security device so that only researchers could access it. Research data would be retained for 3 years before deletion.
This study investigated the demographic and clinical characteristics of the study subjects. Age and gender were examined for demographic characteristics, and preoperative, surgical, and postoperative characteristics were investigated for clinical characteristics. Preoperative characteristics include smoking status (last cigarette within one year, smoking cessation over one year, never smoked), underlying disease, diagnosis, preoperative functional status (independent, partially independent, dependent), preoperative blood test results (oxygen saturation, hemoglobin, albumin, and hematocrit), and the American Society of Anesthesiologist's (ASA) physical status classification. Regarding surgery, range of lung resection, surgical incision, emergency procedure (Yes or No), and duration of surgery were included, and for postoperative characteristics, Intensive Care Unit (ICU) stay, length of stay, postoperative hospital stay, and type of discharge were included. These data were confirmed using the electronic medical record. The ASA physical status classification [28] is used to assess the fitness of patients before surgery. ASA 1, 2, 3, 4, 5, and 6 refer to a normal healthy patient, a patient with mild systemic disease, a patient with severe systemic disease, a patient with severe systemic disease that is a constant threat to life, a moribund patient who is not expected to survive without operation, and a declared brain-dead patient whose organs are being removed for donor purposes, respectively. Each characteristic was based on the predictive factors of ARISCAT [17] and PCRS-lung resection model [10], and factors representing the subjects' postoperative status.
ARISCAT [17], developed in Spain, was approved by the author as a tool to assess the risk of PPCs in surgical patients. The PPCs included in this tool were respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, and aspiration pneumonia, and detailed diagnostic criteria [17] were presented. Accordingly, in this study, the absence of PPCs was determined by finding the content from the medical records corresponding to these criteria. Respiratory infection was defined as a condition when one or more of the following criteria was met: a case when antibiotics were being administered for suspected respiratory infection, the onset of or changes in sputum, the onset of or changes in lung opacity, fever, or white blood cell count >12,000/µL. Respiratory failure was defined as a condition when one of the following criteria was met: arterial partial oxygen pressure (PaO2) <60 mmHg, the ratio of arterial blood oxygen partial pressure (PaO2) to inspired oxygen concentration (FiO2) <300, or oximetry <90% requiring oxygen therapy. Pleural effusion, atelectasis, and pneumothorax were confirmed by chest radiographs or medical records. Bronchospasm was a case where bronchodilators were used for newly discovered expiratory wheezing, and aspiration pneumonia was a case where acute lung damage was observed due to aspiration of refluxed gastric contents. This study confirmed these criteria and investigated it using medical records.
In ARISCAT, the risk of pulmonary complications is assessed using seven items: age, preoperative oxygen saturation, respiratory infection within a month, preoperative hemoglobin concentration, surgical incision site, surgical time, and emergency surgery. The medical records of the subjects were used to evaluate the above items. Regarding the test results, this study checked the date and time closest to the preoperative period. In terms of determining whether there were respiratory infections, the records of respiratory infections in the outpatient or hospitalization records were checked and any symptom of respiratory infections such as cough and sputum and their duration were confirmed.
Scores for each item were as follows: 0 for those under 50 years of age, 3 for those aged 51~80 years, and 16 for those over 80 years of age. Preoperative oxygen saturation ≥96% received 0 points, followed by 8 points for saturation of 91~95%, and 24 points for saturation ≤90%. No point was given if there was no respiratory infection within the past month, and 17 points were given if there was infection. No point was given for hemoglobin concentration of more than 10 g/dL, and 11 points for that less than 10 g/dL. Regarding the surgical incision site, 0 points were given for the peripheral area, 15 points for the upper abdomen, and 24 points for the intrathoracic cavity. In addition, 0 points were given for operation time of less than 2 hours, 16 points for that of 2~3 hours, and 23 points for that more than 3 hours. Regarding the emergency procedure, 0 points were given for elective surgery and 8 points for emergency surgery. The combined scores ranged from 0~123 points and was classified into three levels: less than 26 points as low risk, 26~44 points as intermediate risk, and 45 points or more as high risk.
The PCRS-lung resection model [10] developed in the United States was designed to predict PPCs using the national database, and its use was approved by the author. In this model, PPCs were defined as re-intubation, postoperative pneumonia, and prolonged mechanical ventilation that occurred within 30 days after surgery. Unplanned reintubation was defined as a case when a patient was re-intubated and ventilator-assisted due to the onset of respiratory or heart failure manifested by severe respiratory distress, hypoxia, hypercapnia, or respiratory acidosis within 30 days of surgery. Postoperative pneumonia was defined as a case when a crackling sound or dullness was observed in the chest during physical examination, with the onset of purulent sputum or changes in the characteristics of sputum, a positive blood culture, or when bacteria were isolated from bronchial aspiration or biopsy specimens. Postoperative pneumonia was defined as a case when the onset or gradual infiltration, consolidation, cavitation, or pleural effusion were observed on chest radiographs, with the onset of purulent sputum or changes in sputum's characteristics, a positive blood culture, isolation of bacteria from specimens obtained by bronchial aspiration and biopsy, virus isolation and antigen detection from respiratory specimens, a 4-fold increase in immunoglobulin M or immunoglobulin G, or histopathological evidence of pneumonia. Prolongation of mechanical ventilation was defined as a case when the length of assisted breathing through a ventilator during hospitalization after surgery exceeded 48 hours.
In the PCRS-lung resection model, the risk of pulmonary complications was evaluated using 12 items: age, gender, preoperative serum albumin concentration, ASA classification, congestive heart failure within 1 month, history of chronic obstructive pulmonary disease, smoking history in the past year, preoperative dyspnea at rest and moderate dyspnea, preoperative functional status, preoperative hematocrit, total operative time, and preoperative sepsis. The onset of congestive heart failure and preoperative sepsis during the past month were checked using hospitalization records, records before anesthesia, and nursing records. Regarding the onset of dyspnea at rest or moderate dyspnea, cases where the thoracic surgeon recorded'shortness of breath at rest' in the hospitalization or outpatient record were investigated.
Each item was given the following scores: 10 points for patients aged 60~69 years old, 29 points for those aged 70~79 years, 58 points for those aged 80 years or older; 0 points for women and 26 points for men; 0 points for serum albumin levels ≥3.5 g/dL and 62 points for those less than 3.5 g/dL; 0 points for ASA classification of 1~2 and 54 points for 3~5; 0 points for the absence of congestive heart failure 1 month before surgery and 80 points for the onset congestive heart failure; 0 points for having no history of Chronic Obstructive Pulmonary Disease (COPD), 67 points for having a history of COPD; 0 points for no history of smoking within 1 year and 42 points for having a history of smoking; 0 points for the absence of dyspnea at rest and moderate dyspnea and 24 points for the onset; 0 points for independent functional status and 95 points for fully or partially dependent functional status; 0 points for hematocrit values ≥37% in men, 38 points for those less than 37%, 0 points for those ≥35% in women, and 38 points for those less than 38%; 36 points for 90~139 minutes of operation time and 56 points for 140~202 minutes; and 0 points for no sepsis and 122 points for the onset. The combined score ranged from 10 to 762 points, and the expected incidence of PPCs according to the range of scores was 1.5~2.4% for less than 111 points, 4.4~4.9% for 111~172 points, 8.8~9.1% for 173~231 points, and 17.2~17.8% for a score of more than 231 points.
In this study, data was collected after obtaining approval for the use of electronic medical records at P University Hospital in B City. Subsequently, its Medical Information Team provided a list of data corresponding to the surgical codes of wedge resection (O1401, O1403 - O1405), segmentectomy (O1410), lobe and lung segmentectomy (O1423), lobectomy (O1421, O1422, O1424), pneumonectomy (O1431-O1432). Data was gathered for about two months from August 1, 2021. All data were directly collected by one researcher using these medical records. To evaluate preoperative characteristics, surgical characteristics, postoperative characteristics, the onset of PPCs, and each item (risk factor) of the instrument, outpatient, hospitalization, pre-op, nursing, and clinical observation records, diagnostic test and imaging test results, progress records, and consultation records were collected by searching the integrated electronic medical records.
The data obtained was analyzed using the IBM SPSS Statistics for Windows, Version 25.0 program (IBM Corp., Armonk; NY) as follows.
• The demographic and clinical characteristics of the subjects were calculated as frequency, percentage, mean and standard deviation, minimum value, and maximum value.
• The sensitivity, specificity, positive predictive value, and negative predictive value of each tool were presented, and the case with the highest Youden index was determined as the cut-off score. Sensitivity was calculated as the ratio of subjects predicted to be at risk of PPCs to the score of the prediction model among patients with PPCs. Specificity was calculated as the ratio of subjects predicted to be in a non-risk group for PPCs to the score of the prediction tool among patients without PPCs. The positive predictive value was calculated as the ratio of subjects who developed PPCs to the total number of patients predicted to be in a risk group for PPCs. The negative predictive value was calculated as the ratio of subjects who did not develop PPCs to the total number of patients predicted to be in a non-risk group for PPCs. The Youden index refers to the value obtained by subtracting 1 from the sum of the ratios of sensitivity and specificity ( [sensitivity + specificity] - 1).
• To compare the overall predictive validity, the ROC curve of each model was drawn and the AUC was calculated, with a 95% Confidence Interval (CI).
Table 1 lists the demographic and clinical characteristics of the subjects. The average age was 62.95±13.43 years, and men accounted for 60.7%. Regarding the clinical characteristics, 58.1% of the subjects had no smoking history before surgery, and 24.1% had a smoking history within the past one year. Approximately 82.2% of the subjects had underlying health conditions, including hypertension (36.8%) and diabetes (20.9%). The diagnosis of 76.4% of the subjects was lung cancer, of which 40.9% of the subjects were in stage 1. Functionally independent status was the most common at 98.7%. An ASA classification of 2 was the most frequent at 73.5%. Regarding surgery, lobectomy accounted for 59.3%, followed by wedge resection at 59.0%, and thoracoscopic surgery was the most common at 99.6%. Most of the surgeries were elective, and emergency surgeries accounted for only 0.5%; the average total operation time of the subjects was 147.64±74.09 minutes.
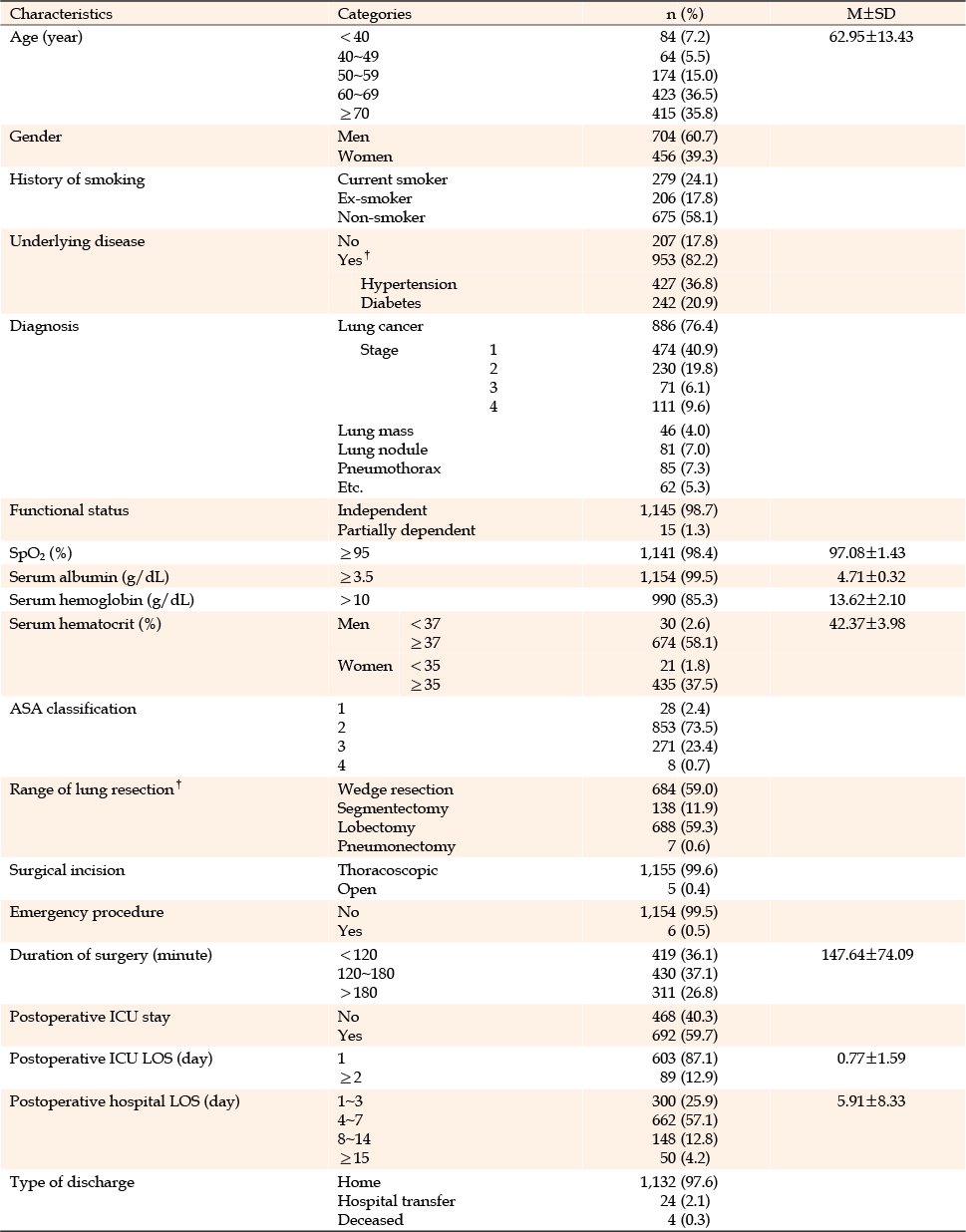
Table 1
Demographic and Clinical Characteristics of the Subjects (N=1,160)
In terms of the postoperative characteristics of the subjects, 59.7% of the subjects stayed in the ICU, and the average length of stay in the ICU was 0.77±1.59 days, of which 87.1% of the subjects stayed for one day. The average length of stay for post-surgery hospitalization was 5.91±8.33 days, with 4.2% of the subjects staying for more than 15 days after surgery and 0.8% of them staying for more than 30 days. In most cases, the length of stay was prolonged due to the use of a ventilator or application of high-flow oxygen therapy due to pneumonia and respiratory failure after surgery. Regarding the discharge type, 97.6% of the subjects were discharged home, but 2.1% were transferred to skilled nursing facilities for rehabilitation due to continuous pain or postoperative helplessness; 0.3% of the subjects died due to exacerbation of pneumonia and respiratory failure (Table 2).
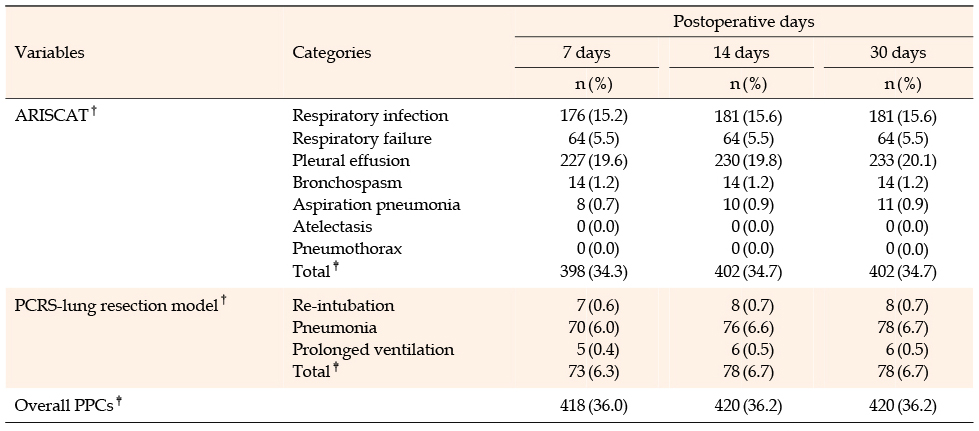
Table 2
Incidence of Postoperative Pulmonary Complications
The frequency of PPCs among 1,160 subjects was divided into the 7th, 14th, and 30th days after surgery according to the criterion of each tool. In ARISCAT, respiratory infection occurred in 15.6% of the subjects, pleural effusion in 20.1%, and aspiration pneumonia in 0.9%. In the PCRS-lung resection model, reintubation and prolonged mechanical ventilation occurred in 0.7% and 0.5% of the subjects, respectively, pneumonia in 6.7%, and the sum of PPCs was 6.7% within 30 days of surgery. The total incidence rate of the subjects who met the criteria for each tool was 36.0% on the 7th day and 36.2% on the 14th and 30th days, excluding duplicates (Table 2).
The sensitivity, specificity, positive predictive value, and negative predictive value according to the ARISCAT score were as follows (Table 3). In this study, the sensitivity, specificity, positive predictive value, and negative predictive value (26 points for the intermediate-risk group and 45 points for the high-risk group) suggested by the original author of ARISCAT were 98.8%, 10.3%, 36.9%, and 94.0%, respectively, at 26 points and 53.5%, 69.8%, 48.4%, and 73.9%, respectively, at 45 points. The sensitivity, specificity, positive predictive value, and negative predictive value at the cut-off scores based on quartiles were 98.8%, 10.3%, 36.9%, and 94.0%, respectively, at 27 points in the first quartile (Q1). They were 74.6%, 43.8%, 41.3%, 76.5%, respectively, at 43 points in the second quartile (Q2), and 51.7%, 71.5%, 49.1%, and 73.6%, respectively, at 50 points in the third quartile (Q3). The predictive validity at 27 points (Q1) of ARISCAT was the same as the predictive validity at 26 points, the cut-off score for the medium-risk group according to the original tool. In this study, the cut-off score at which the Youden index had the maximum value in ARISCAT was 47 points, which was higher than the boundary (45 points) of the high-risk group presented in the original tool. The sensitivity, specificity, positive predictive value, and negative predictive value at 47 points were 53.2%, 70.6%, 49.0%, and 74.0%, respectively.
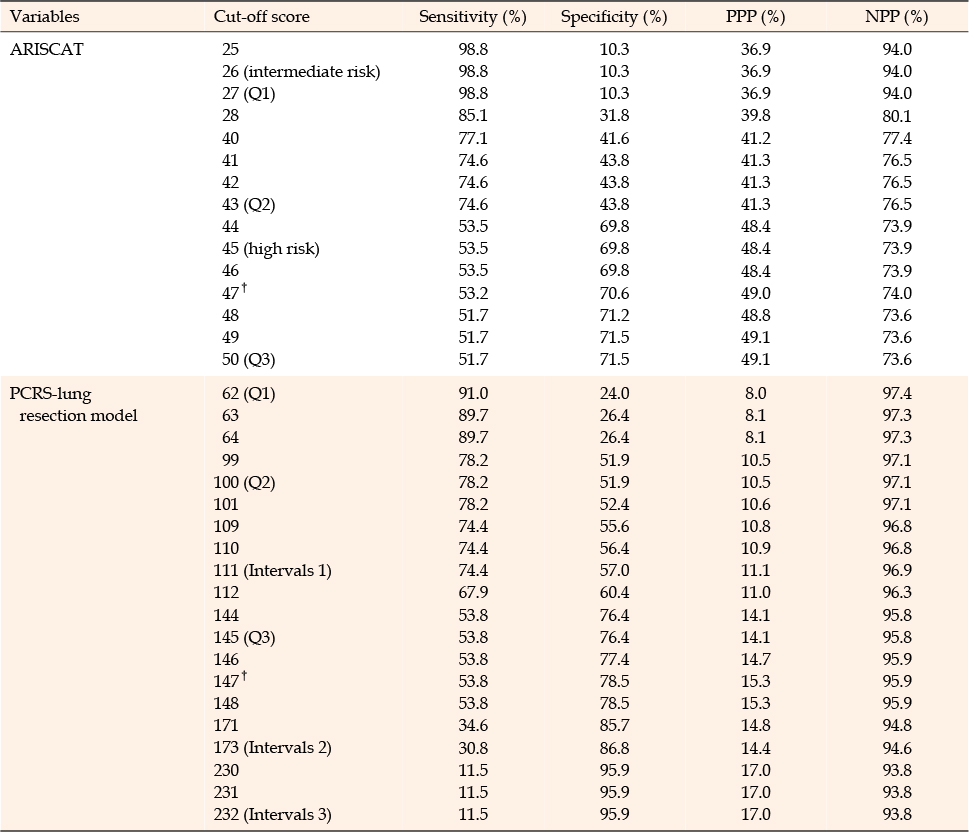
Table 3
Tests of Scales at Various Cut-off Scores
To evaluate the validity of the tools, a ROC curve was drawn, and AUC was calculated and compared for each tool. The larger the AUC, the higher is the validity of the diagnostic test. An AUC of less than 0.5 is not useful, 0.5 to less than 0.6 is bad, 0.6 to less than 0.7 is sufficient, 0.7 to less than 0.8 is good, 0.8 to less than 0.9 is very good, and 0.9 or more to 1.0 is excellent [29]. In this study, the ROC curve of ARISCAT is depicted in Figure 1. The AUC of ARISCAT was 0.65 (95% CI 0.61 to 0.68), indicating that it was sufficient.
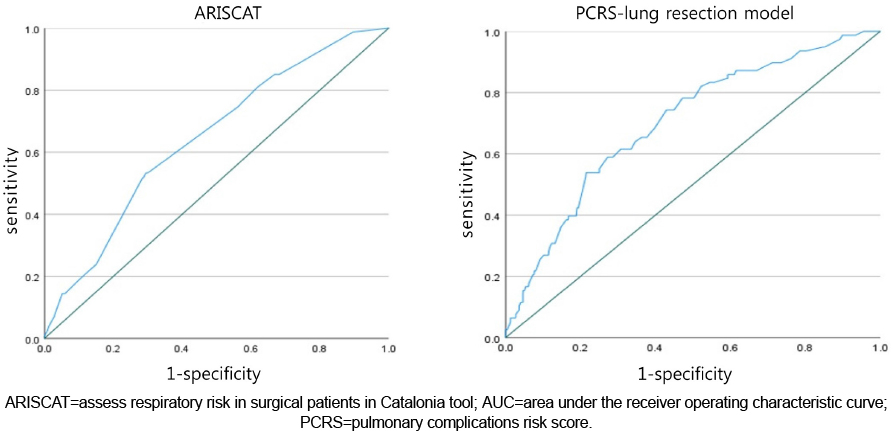
Figure 1
Receiver operating characteristic curves of ARISCAT (AUC=0.65) and PCRS-lung resection model (AUC=0.70).
The sensitivity, specificity, positive predictive value, and negative predictive value according to the score of the PCRS-lung resection model are listed in Table 3. In this study, the sensitivity, specificity, positive predictive value, and negative predictive value at the scores proposed by the original authors of the model were 74.4%, 57.0%, 11.1%, and 96.9%, respectively, at 111 points, 30.8%, 86.8%, 14.4%, and 94.6%, respectively, at 173 points and 11.5%, 95.9%, 17.0%, and 93.8%, respectively, at 232 points. The sensitivity, specificity, positive predictive value, and negative predictive value in the score based on quartiles were 91.0%, 24.0%, 8.0%, and 97.4%, respectively, at 62 points in Q1, 78.2%, 51.9%, 10.5%, and 97.1%, respectively, at 100 points in Q2, and 53.8%, 76.4%, 14.1%, and 95.8%, respectively, at 145 points in Q3. In the PCRS-pulmonary resection model, the cut-off score at which the Youden index had the maximum value was 147 points, which was lower than the score for the group with the highest risk of occurrence (>231 points) suggested by the original author. The sensitivity, specificity, positive predictive value, and negative predictive value at that time were 53.8%, 78.5%, 15.3%, and 95.9%, respectively.
In this study, the ROC curve of the PCRS-lung resection model is depicted in Figure 1. The AUC of the model was 0.70 (95% CI 0.64~0.76), which indicates that the tool is good.
This study found that the incidence of PPCs in inpatients who underwent lung resection was 34.7% in ARISCAT and 6.7% in PCRS-lung resection model, and the AUC of each model was 0.65 in ARISCAT and 0.70 in PCRS-lung resection model.
Among the various ranges of PPCs suggested in previous studies [9, 10, 11], this study investigated the incidence according to each predictive tool to explore pulmonary complications that should be carefully observed in lung resection. In this study, the PPC rate of the PCRS-lung resection model was similar to the one shown in the developmental study [10], which was 7.6%. However, the difference between the ARISCAT and PCRS-lung resection model in the incidence of PPCs is considered to be due to the different definitions or ranges of PPCs defined in each tool. ARISCAT consists of seven items (respiratory infection, respiratory failure, pleural effusion, atelectasis, pneumothorax, bronchospasm, and aspiration pneumonia), whereas the PCRS-lung resection model consists of three items (reintubation, pneumonia, and prolonged mechanical ventilation). In particular, among the ARISCAT items, the incidence of pleural effusion was the highest, which generally causes an imbalance in pleural fluid turnover within 24~48 hours after lung resection [30]. It is considered a postoperative phenomenon and not a complication [31]. It was difficult to compare the incidence of PPCs as few previous studies matched the scope defined as PPCs. Therefore, a standard should be first established for the definition and scope of PPCs.
This study investigated PPCs that occurred within 30 days after lung resection based on previous studies [10, 14], which suggested that the duration of PPCs varied from 7 to 30 days after surgery. However, there was very little change in the incidence of PPCs at 7, 14, and 30 days after surgery. This reflects the fact that the length of stay of lung resection patients is short, less than a week on average, and most PPCs occur within a week.
The gender distribution of the subjects in this study was 60.7% men and 39.3% women, with more men with an average age of 62.95 years. This is similar to the distribution of subjects in previous studies [4, 9, 15] on PPCs of patients with lung cancer who underwent lung resection in Korea, with 58.6~62.6% men, 37.4~41.4% women, and an average age of 62~67 years. Lung cancer was the most common diagnosis in 76.4% of the subjects, probably because lung resection is mainly applied as the primary treatment method for early lung cancer [32]. The most common method of surgical incision was thoracoscopic surgery. The rate of thoracoscopic surgery was high among subjects because the use of minimally invasive surgery reduced the incidence of PPCs and contributed to the rapid recovery of patients compared to thoracotomy [33]; thus, the number of thoracoscopic surgeries is increasing in clinical practice. In a previous study [9] that analyzed data from 2012 to 2014, the frequency of use was similar, with thoracotomy at 44.9% and thoracoscopy at 55.1%. However, in a previous study [4] that analyzed data from 2015 to 2018, the rate of subjects who underwent thoracoscopic surgery was high at 95.3%; the results of this study are interpreted in a similar context.
In this study, sensitivity was considered first in the evaluation of risk prediction tools for PPC. Sensitivity and specificity are ideally high in the evaluation of diagnostic tools, but this is practically impossible. Therefore, this study inferred that considering sensitivity [34], which refers to a test's ability to designate an individual with a disease as positive, is more in line with the purpose of screening in terms of prevention. PPCs lead to serious negative consequences such as prolonged hospital stay and increased mortality [16, 17]; therefore, preventive aspects are important. Thus, sensitivity was considered a priority. In this study, the cut-off score at which the Youden index of ARISCAT reached the maximum value was 47 points, which was similar to the cut-off score of 45 points for the high-risk group for PPCs suggested by the author of the original study. However, to predict the probability of occurrence in the high risk group more accurately, the sensitivity and negative predictive value may be increased by adjusting the cut-off score of the high-risk group to 43 points, the Q2 score in this study. The cut-off score at which the Youden index of the PCRS-lung resection model had the maximum value was 147 points, which corresponded to the second lowest risk group (111-172 points) among the 4-stage risk group classifications suggested by the author of the original study. Therefore, when applying the PCRS-lung resection model to domestic patients, the cut-off score of the high-risk group should be decreased to 147~148 points to increase sensitivity and negative predictive value.
Through this study, the sensitivity, specificity, positive predictive value, and negative predictive value were examined in quartiles of each prediction tool score and the cut-off score at which the Youden index had the maximum value. However, it was difficult to interpret this due to the lack of comparable previous studies. The cut-off score of the high-risk group in the predictive tool in this study differs from that of the original tool because ARISCAT was developed for the Spanish population, and the PCRS-lung resection model was developed for the US population. There may also be differences in the geographic environment of Korea. To generalize the application of the predictive tool, it is necessary to confirm geographical mobility and stability [17, 35]. Therefore, repeated analyses are needed to confirm the optimal cut-off score for domestic lung resection patients in follow-up studies.
As a result of checking the AUC of each model in this study, the PCRS-lung resection model was similar to 0.74 indicated in the previous study [10], but the ARISCAT was 0.65, which was lower than 0.80~0.81 in the previous study [21, 23]. This might be due to a difference in the subjects, as the previous study included both patients who underwent abdominal surgery and general surgery; thus, it can be assumed that ARISCAT lacks specificity to apply to patients with a single lung resection. Meanwhile, in a previous study [12] targeting patients who underwent lung resection for lung cancer, the AUC of ARISCAT was 0.54, which was lower than that of this study. This may be related to the inclusion of persistent air leaks, chylochophora, hemorrhage, and empyema, which are outside the category of PPCs suggested by ARISCAT in previous studies.
Predictive validity was examined by applying ARISCAT and the PCRS-lung resection model, which assessed the risk of PPCs. To comprehensively assess PPCs in lung resection patients, the PCRS-lung resection model can be considered as a more appropriate tool because it is surgery specific.
The limitation of this study was that the definition of PPCs, which is used in various clinical settings, was investigated by applying the categories and detailed criteria presented in each prediction tool. Thus, follow-up studies are needed to clarify the definition of PPCs. In addition, this study was a retrospective investigation using medical records for inpatients who underwent lung resection at a university hospital, with limitations in generalizing, interpreting, and applying the study results. In the future, a prospective study that investigates patients who have undergone lung resection at multiple hospitals is needed.
However, this study is significant in that it explored predictive validity by applying the ARISCAT and PCRS-lung resection models, which have not yet been actively studied in Korea, to domestic patients who have undergone lung resection. In addition, since the definition of PPCs has not been presented, there have been difficulties in diagnosing them in practice. This study presented the incidence of PPCs in patients with lung resection and suggested an appropriate predictive tool by applying the criteria defined by the two tools. In addition, objective predictive tools are currently being used to select high-risk groups for falls and pressure ulcers in clinical practice. As such, the PCRS-lung resection model can be used to evaluate the risk of PPCs in patients, share information among medical staff, and provide preventive care. To this end, research on the development of protocols for the provision of interventions should be conducted according to the additional verification and classification of predictive tools so that they can be used in nursing practice.
This study investigated the incidence of PPCs in inpatients who underwent lung resection at a university hospital, and analyzed the predictive validity of each tool by applying ARISCAT and the PCRS-lung resection model. This was a retrospective study to explore the applicability of a predictive tool for PPCs to domestic patients who underwent lung resection.
This study demonstrated that among 1,160 inpatients who underwent lung resection, PPCs occurred in 34.7% of patients in ARISCAT and 6.7% in the PCRS-lung resection model. ARISCAT showed sufficient accuracy, and the PCRS-lung resection model showed good accuracy. Therefore, the PCRS-lung resection model can be used as a valid predictive tool for PPCs in domestic patients.
The PCRS-lung resection model presented in this study will provide nursing care to prevent PPCs by selecting a high-risk group for PPCs in inpatients who have undergone lung resection. Therefore, it should be used in clinical nursing practice. In addition, future studies should analyze the predictive validity of tools for PPCs based on multiple hospitals and identify the optimal cut-off score for domestic lung resection patients. Finally, the incidence of PPCs in surgeries other than lung resection should be investigated and predictive validity compared using tools specific to each operation.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - JS and HS-K.
Data collection - JS.
Analysis of the data - JS.
Interpretation of the data - JS and HS-K.
Drafting of the manuscript - JS and HS-K.
Critical revision of the manuscript - JS and HS-K.
This manuscript is a modified form of the first author's master's thesis from Pusan National University.
 E-SUBMISSION
E-SUBMISSION