
Purpose
COVID-19 is both a national crisis and a cause of individual trauma. This trauma is experienced during the period of acute illness and for an unpredictable duration after recovery. This study explored experiences of COVID-19 patients in hospital isolation, providing a detailed account of their experiences to furnish basic data necessary for establishing strategies to address the psychosocial problems that may arise from the hospital isolation process and recovery period.
Methods: We conducted comprehensive interviews and qualitative content analysis.
We held in-depth interviews with five COVID-19 patients from May 16 to August 22, 2021, and also analyzed data from interviews with five patients conducted as part of another study on COVID-19 patients' perceptions. Thus, 10 participants' interviews were analyzed in this study.
Results: From the qualitative data, 34 codes, 9 subcategories, and 4 categories were identified. The categories included "Prioritization of epidemic prevention over treatment," "Victims who have been labeled as perpetrators," "Gratitude felt in difficult moments," and "Demand for respect from the system and society." After analyzing these categories, we derived the overarching theme of "It's okay, but it's not okay." Conclusion: During isolation treatment, it is crucial to uphold human rights as much as possible by prioritizing patient care, providing a comfortable environment, and offering clear guidance on their progress. Communication between patients and caregivers should be facilitated to provide psychological support.
Furthermore, national policies such as economic compensation and strategies for post-traumatic growth should be implemented to address grievances and facilitate recovery.
COVID-19 is both a national crisis and a cause of individual trauma. This trauma is experienced during the period of acute illness and for an unpredictable duration after recovery. This study explored experiences of COVID-19 patients in hospital isolation, providing a detailed account of their experiences to furnish basic data necessary for establishing strategies to address the psychosocial problems that may arise from the hospital isolation process and recovery period.
We conducted comprehensive interviews and qualitative content analysis. We held in-depth interviews with five COVID-19 patients from May 16 to August 22, 2021, and also analyzed data from interviews with five patients conducted as part of another study on COVID-19 patients' perceptions. Thus, 10 participants' interviews were analyzed in this study.
From the qualitative data, 34 codes, 9 subcategories, and 4 categories were identified. The categories included "Prioritization of epidemic prevention over treatment," "Victims who have been labeled as perpetrators," "Gratitude felt in difficult moments," and "Demand for respect from the system and society." After analyzing these categories, we derived the overarching theme of "It's okay, but it's not okay."
During isolation treatment, it is crucial to uphold human rights as much as possible by prioritizing patient care, providing a comfortable environment, and offering clear guidance on their progress. Communication between patients and caregivers should be facilitated to provide psychological support. Furthermore, national policies such as economic compensation and strategies for post-traumatic growth should be implemented to address grievances and facilitate recovery.
Coronavirus Disease 2019 (COVID-19) is classified as an "emerging infectious disease syndrome." This respiratory syndrome is characterized by symptoms such as fever, chills, muscle pain, dry cough, runny nose, sore throat, loss of appetite, and diarrhea. It is also categorized as a class 1 infectious disease [1]. As of February 17, 2022, there have been 530,555,425 reported cases and 6,294,067 deaths globally since the World Health Organization (WHO) declared the pandemic [2, 3]. In South Korea, the total number of infections has reached 18,119,415, resulting in 24,197 deaths [4].
In the initial stages of an epidemic, when evidence is limited, the primary goal is to quickly isolate all confirmed patients in medical facilities. This is achieved through the 3T strategy, which involves extensive testing and confirmation, epidemiological tracing, and isolation and treatment [5, 6]. The purpose of inpatient isolation treatment is to prevent the spread of infection from a patient with an infectious disease, a suspected infectious disease patient, or a carrier of a virulent disease pathogen to other patients or hospital staff [1]. As the number of confirmed cases increased, leading to shortages of hospital beds, medical personnel, and essential patient treatment equipment, a system was put in place. This system prioritized hospitalization for severe and critical patients, while asymptomatic and mild cases were monitored for symptoms in isolation facilities such as community treatment centers. In the early stages, due to a limited understanding of the disease's progression and characteristics, some individuals were isolated in community treatment centers for over a month. As more information about COVID-19 became available, the guidelines for epidemic prevention were continually revised [6].
Patients undergoing isolation and treatment spend the majority of their time alone. This often leads to feelings of shock and estrangement, self-blame or sadness from family and friends, and the experience of exclusion and discrimination when their infection becomes known to others [6, 7, 8]. These challenges continue even after discharge, manifesting as socioeconomic issues due to various lingering effects and the awareness of anxiety, depression, job loss, and social stigma [8]. Studies of patients infected with COVID-19 revealed that symptoms of post-traumatic stress disorder, such as fear of reinfection, social stigma, frustration, guilt, depression, anxiety, and sleep disturbance, can persist for months or even years [9, 10, 11]. To prevent these long-term physical and psychosocial problems in patients recovering from acute diseases, a strategy is needed to mitigate these unhealthy outcomes. Therefore, it is crucial to understand the specific aspects of patients' experiences, from the moment they are isolated due to COVID-19 to the start of their inpatient treatment.
A study examining the attitudes of South Korean COVID-19 patients towards hospital isolation found that some patients adopted a passive stance. Despite this, they were willing to accept and appreciate their circumstances, considering the potential for worse outcomes [11]. Other patients expressed feelings of injustice and exhibited maladaptive behavior due to social stigma, guilt, and fear. These responses suggest that these patients experienced significant confusion and negative emotions during their hospital isolation.
Research on the mental health of COVID-19 patients in China and Italy primarily focused on assessing levels of depression and anxiety [12, 13]. A retrospective chart review conducted in the UK reported symptoms such as sleep disorders, anxiety disorders, suicidal thoughts, mood disorders, decreased concentration, and headaches in patients [14]. These symptoms could be influenced by the impact of COVID-19 on the central nervous system, the severity of the infection, experiences in intensive care, the duration of hospitalization, and other personal characteristics.
Much of the existing literature focuses on developing strategies to overcome the trauma induced by COVID-19. Since this trauma originates from the point of infection, the experiences of patients during their hospital isolation could offer valuable insights. Previous studies have primarily concentrated on patients in the recovery phase following hospital isolation. Given the limitation that these studies do not fully capture the diverse experiences of patients during hospital isolation, it is crucial to investigate patients' experiences, specifically from the time of hospitalization and isolation to early recovery. Consequently, this study examined the experiences of hospital isolation and recovery in COVID-19 patients. Our findings could provide foundational data for devising intervention strategies to address various psychosocial issues that may emerge during hospital isolation and the subsequent recovery period.
We utilized a qualitative methodology, employing indepth interviews and qualitative content analysis, to investigate the experiences of isolation among COVID-19 patients.
This study utilized interview data from 10 participants. The data included comprehensive interviews with five participants, conducted by two authors well-versed in qualitative research, from May 16 to August 22, 2021. Additionally, the data incorporated raw interview transcripts from five other participants. These interviews, conducted with identical questions from November 14 to 29, 2020, were initially used to derive Q statements in a previous Q-methodology study. This study focused on varying perceptions of hospitalized isolation among COVID-19 patients [11]. The choice to employ a secondary analysis of primary qualitative datasets was driven by two objectives. First, it addressed a sensitive research area, and second, it facilitated access to a research population that is typically difficult to reach. Both of these factors can pose significant challenges to conducting research in areas considered sensitive or controversial [15].
The data collection period coincided with the early stages of the COVID-19 pandemic, a time when stringent social distancing measures were in place. This period also saw the prevalence of sporadic group infections, primarily through contact among acquaintances [5]. Given the social circumstances, access to participants was limited. Therefore, we incorporated and analyzed qualitative interview data from a previous study [11] into this study. The data in question were obtained from COVID-19 patients aged 19 and above who underwent hospitalization and isolation. Participants were selected through purposive and snowball sampling, involving the families, colleagues, religious groups, and hobby clubs of the authors. The 10 participants were hospitalized and isolated from August 2020 to June 2021 at two public medical centers, COVID-19-specific wards at a university hospital and a general hospital, and a community treatment center in G province and J province. From March 2020 to May 2022, COVID-19 beds in Korea were at community treatment centers for treating mild cases, infectious disease hospitals for moderate cases, and dedicated beds for severe patients, in response to the surge in COVID-19 cases and the availability of medical resources [5]. Additional characteristics of the participants are detailed in Table 1.
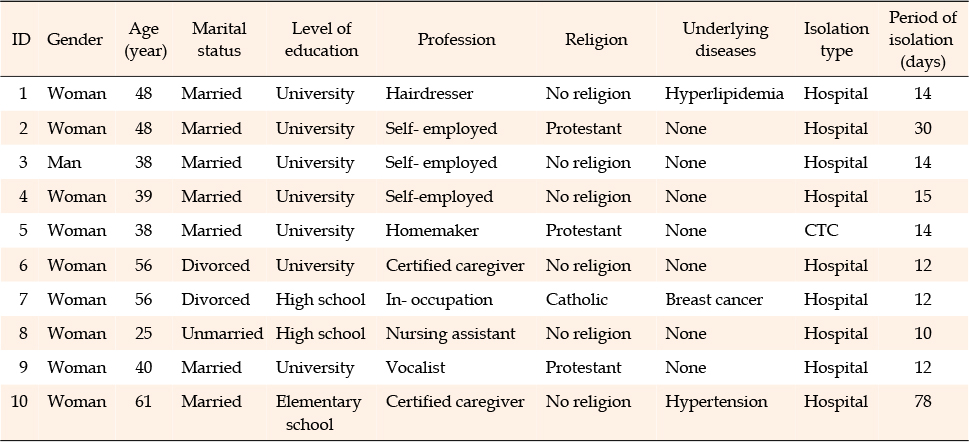
Table 1
Characteristics of the Participants (N=10)
The interviews took place between one and three months after the participants were discharged from the hospital. This timeframe was chosen based on previous studies, which were conducted anywhere from seven days [16] to one year [17] post-discharge. The schedule also took into account the Korean government's guidelines for enhanced isolation.
The main and follow-up interview questions for the five new participants in this study, as well as the questions used in previous studies [11], focused on the participants' experiences with COVID-19 hospital isolation. The questions included: "How did you perceive your experience of hospital isolation after contracting COVID-19?", "Can you describe your experiences in the isolation room?", "What physical changes did you notice after contracting COVID-19?", "What psychological changes did you experience as a result of isolation after contracting COVID-19?", "How would you evaluate your experience of COVID-19 infection and isolation?", and "In what ways did the COVID-19 infection and isolation impact your life?".
We conducted individual in-depth interviews using the method preferred by each participant. Three participants chose to have face-to-face interviews at their homes, while two opted for telephone interviews. In a previous study [11], we gathered data from five participants through face-to-face interviews either at their homes or in a cafe. Two participants from that study [11] were interviewed twice to supplement the initial interview, while the remaining eight participants were interviewed once. The interviews in this study lasted anywhere from 45 minutes to 1 hour and 40 minutes. The duration of the interview data used in the secondary analysis also ranged from 45 minutes to 1 hour and 40 minutes. All interviews were recorded using the audio-recording function on a mobile phone and were later transcribed by the authors who conducted the interviews. The transcriptions totaled 142 pages: 61 pages from the five participants in this study and 81 pages from the interview data of the five participants used for secondary analysis.
This study adhered to the ethical standards outlined in the Declaration of Helsinki and received ethical approval from the Institutional Review Board (IRB) of Gangneung-Wonju National University (No. GWNUIRB-2021-19-3). Participants were fully briefed on the study's subject matter and objectives, the methodology (including the necessity for in-depth interviews and audio recordings), the time commitment required, and their right to discontinue or withdraw their participation at any point without any negative consequences. They were reassured that only the authors would have access to the data, which would be disposed of upon the study's completion to protect their personal identities. Additionally, we obtained IRB approval for the secondary use of interview data from five participants from a previous study [11]. These individuals were informed that their interview data would be utilized in this study and their permission was sought. Informed consent for voluntary participation was obtained from all participants.
The data was examined using an inductive approach through qualitative content analysis, as outlined by Graneheim and Lundman [18]. This method of qualitative content analysis is focused on analyzing texts to understand their content and contextual meaning, with a particular emphasis on the language of communication [18].
The data analysis utilized the complete transcripts from the qualitative interviews conducted during the initial phase of the preceding Q-methodology study [11], as well as the transcript from the interview conducted in this study. The two authors who conducted the interviews independently reviewed the data, highlighting significant sentences and selecting meaning units that corresponded with the research questions. From the transcripts, a total of 411 meaningful statements were identified. These comprised 207 statements from the transcripts of this study and 204 statements from the transcripts used for secondary analysis.
The core of the selected meaning units was preserved while the contents were compressed, and then transformed into codes, a process known as meaning condensation. Similar codes were grouped together to create sub-categories, and these similar sub-categories were further grouped and abstracted into categories. Throughout this process, the authors consistently reviewed and revised the relevance of the codes, sub-categories, and categories to the data, as well as their alignment with the study's purpose, through ongoing discussions. Ultimately, a theme was identified by connecting the fundamental meanings of the categories.
In accordance with Lincoln and Guba's four criteria [19], the interview process incorporated open-ended questions, enabling participants to articulate their experiences freely. To ensure the credibility of data collection, interview recordings were meticulously transcribed. The authors extracted codes and categories from the data, paying close attention to the participants' words to ensure the credibility of the data analysis. Each author involved in the interviews analyzed the data, refining the naming and classification of codes, categories, and sub-categories through multiple discussions. We sought and incorporated feedback on our analysis from a nursing professor well-versed in qualitative research and a nurse from the COVID-19 treatment ward with qualitative research experience. This was followed by a member check conducted by two participants. We recruited participants of various ages from different institutions, collecting data until saturation was reached. To enhance the generalizability of our research findings, we presented the analysis results to two other COVID-19 survivors who were not part of the interview process. They were asked to compare the findings with their own experiences to verify the applicability. To ensure auditability, we provided detailed descriptions of the data collection and analysis procedures. For confirmability, authors not directly involved in COVID-19 treatments conducted the interviews and analyzed the data, striving to maintain an objective and non-judgmental attitude throughout the process.
The experiences of participants who were hospitalized and isolated due to COVID-19 infection were abstracted into 34 codes, 9 sub-categories, and 4 categories (Table 2). As a result of linking the meanings of these four categories, the overarching theme of "It's okay, but it's not okay" was derived. This theme indicates that the participants navigated the process of hospital isolation in a healthcare setting that prioritized disease control, without being adequately prepared to confront an emerging infectious disease. Despite the challenges, they gradually resumed their normal lives, buoyed by the comfort and support of those around them. However, they were impacted by being viewed as the culprits of the disease. Essentially, this theme suggests that while the physical illness has been overcome, the emotional scars inflicted by negative perceptions have not yet begun to mend.
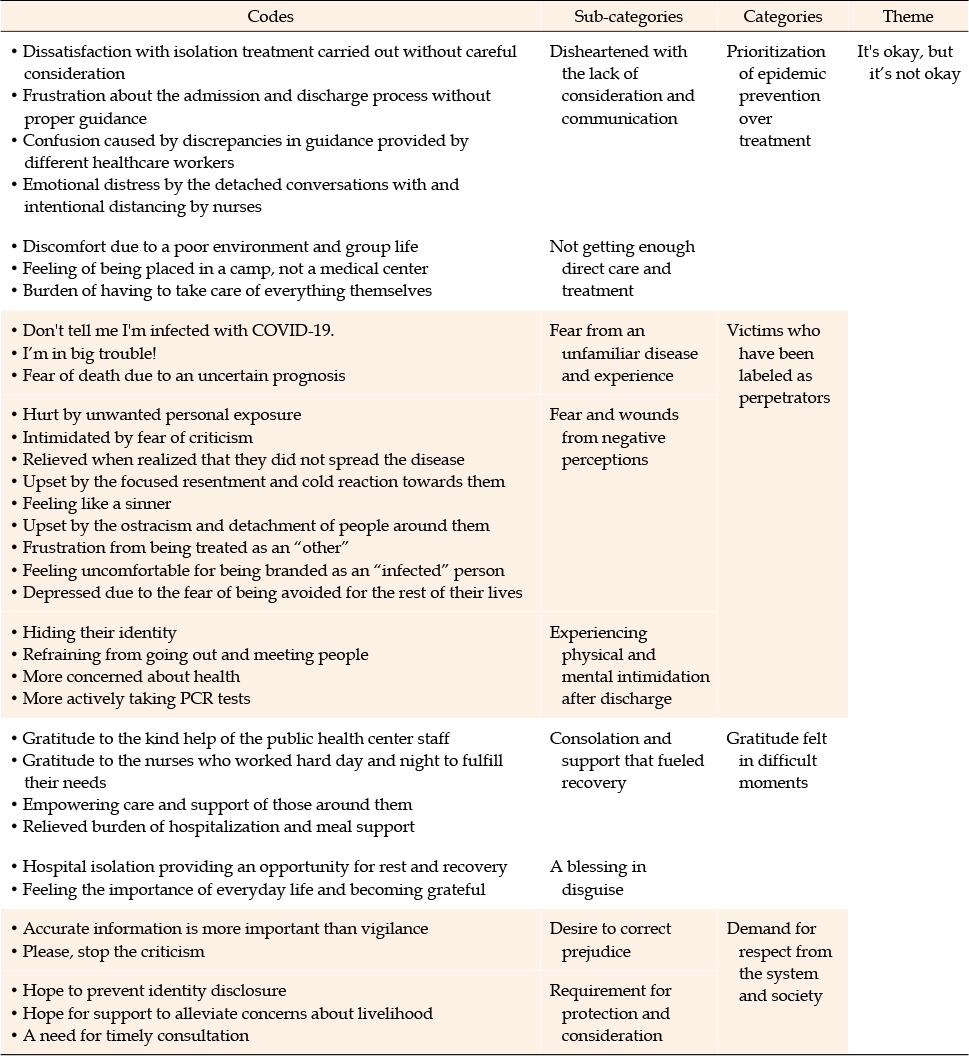
Table 2
Codes, Sub-categories, Categories, and Theme
The participants were placed in hospital isolation during the early stages of the pandemic, when information and understanding about COVID-19 were limited and neither vaccinations nor treatments were available. They perceived that the priority was given to preventing the spread of the disease to protect uninfected individuals, rather than treating those who were already infected.
Upon confirmation of their COVID-19 diagnosis, participants expressed disappointment due to the perceived lack of empathy, clear explanation, and effective communication from the staff and healthcare workers. They found the rapid and unfamiliar processes of isolation, hospitalization, and discharge to be disconcerting. The participants were particularly dissatisfied with the seemingly insensitive manner in which the isolation process was executed, which included staff entering their homes, indiscriminately spraying disinfectants, and treating them with a lack of consideration. However, they felt compelled to suppress their dissatisfaction, burdened by guilt for potentially inconveniencing others due to their infection.
There was one (isolation staff member) who was being very disrespectful. He handed my mother the clothing (protective clothing) and said, "Oh, that isn't it, see.." in a condescending way, which enraged me, but I couldn't say anything. (Participant 2)
The lack of clear instructions for hospital isolation from the public health center staff left the participants feeling inconvenienced. They were unable to bring necessary items with them to the hospital, and were further confused by the abrupt discharge notice, which lacked a sufficient explanation.
The public health center was too busy, and the staff did not provide proper guidance. I was confused and thought, "What is going on?" and "What should I do now?" It felt so weird. (Participant 1)
During their hospital isolation, participants expressed confusion due to inconsistent guidance provided by various healthcare workers. Although they understood that the nurses' maintenance of social distance and impersonal conversations were measures to control infection, they felt disheartened. They perceived themselves as being viewed as contemptible, even by the nurses.
The nurses would keep their distance as they were afraid of people infected with COVID-19, but… The conversation was very detached. It was a little sad that they kept too much of a distance. (Participant 6)
Participants requiring treatment and care felt overlooked. They were housed in inadequate facilities where there was a lack of sufficient showers and toilets, and medical equipment was shared among patients. Despite being COVID-19 patients themselves, some found it disconcerting to cohabitate with others who exhibited more severe symptoms.
There were only two toilets in the restroom, and there were too many people using them. We were all patients, but it felt uncomfortable to share them. (Participant 9)
The participants felt that their individual needs were not being met by healthcare workers, and that their care was reduced to mere phone inquiries about their well-being. This led them to believe that they were placed in these facilities primarily to prevent the spread of the epidemic, rather than to receive proper treatment and care. The rounds were not via videos or video chats, just phone calls.
It felt more like imprisonment in a camp than treatment for an illness, which was disheartening. (Participant 9)
Participants were required to monitor their own vital signs, a task typically performed by healthcare workers. They were also responsible for maintaining the cleanliness of their rooms and toilets. Those who were hospitalized alongside their families faced an even greater burden, as they were expected to care for their family members regardless of their own health status.
I was also a patient, but I took care of my mother like a nurse. (Participant 10)
The participants in this study were patients with an emerging infectious disease that presents more severe symptoms and side effects than the flu and carries a potential fatality risk. Despite being victims of this disease, they were instantly viewed as perpetrators upon testing positive, seen as causing inconvenience to others by spreading the infection. This negative perception persisted even after their discharge, leading to mental intimidation and physical weakness among the participants.
Some participants experienced only mild symptoms of COVID-19, while others had so few symptoms that they found it hard to believe they could be infected. However, upon being diagnosed with this unfamiliar infectious disease for which there was no established treatment, they were admitted to the hospital. They found themselves confined in a claustrophobic negative pressure cart, clad in a white protective suit unlike anything they had ever seen before. It was at this point that the seriousness of their situation truly hit home. The realization that they were suffering from a severe infectious disease, the gravity of which was constantly reported in the news along with daily statistics of critically ill patients and fatalities, filled them with fear for their lives.
I thought about it and went to sleep after taking some cold medicine. I kept thinking, "No, it can't be," but the symptoms persisted. (Participant 2)
Something that I had only seen in the news happened to me… Unspeakable emotions surged. (Participant 7)
In accordance with the national isolation policy, participants were specifically identified by a number assigned based on their infection order and location. In accordance with the government's guidelines for information disclosure and stringent social distancing measures, the movement paths of infected patients were made public. This led to unnecessary exposure of their personal information, resulting in some experiencing trauma due to witch hunts in local online communities.
I was also victimized by a Mom Cafe (an online community of mothers). --- I felt as if I had become a sort of celebrity. --- The name of our business was announced to the public, and was even broadcast on national television. (Participant 3)
The participants observed the harsh comments directed at individuals whose identities and daily movements had been disclosed after testing positive for the virus. This observation instilled a fear in them, making them worry about the potential backlash they might face. Consequently, they became more anxious about the test results of their close contacts than their own health. Their relief was palpable when these contacts tested negative.
I was afraid that people would blame it on me… There was so much criticism of patients with COVID-19… It's not like they wanted to get infected in the first place… (Participant 5)
If there was anyone who had been infected because of me, I would have been devastated. I was so grateful for that (no one was infected because of me). I am so grateful for that. (Participant 1)
However, when those who interacted with the participants contracted COVID-19, they were met with blame and resentment. Despite their attempts to minimize the harm to those around them, they were disheartened by the indifferent responses.
They commented angrily and hatefully, "Why did you wander around?" When this went on… I ended up saying, "I may be asymptomatic but I too am a patient… (Participant 7)
Some participants expressed feelings of guilt, believing they had committed a sin when the elderly individuals who contracted the disease from them passed away. They had yet to recover from this traumatic experience.
I still feel sorry. I still feel like a sinner and murderer. (Participant 10)
Although the participants were confirmed to be negative by the PCR test performed after their discharge from hospitals, they experienced ostracization and social detachment due to misinformation, which offended them.
I was upset when a school teacher asked my child, "Are the elderly patients (who tested positive) in their 70s your grandparents?" Well… Are all people infected with COVID-19 supposed to be our relatives? (Participant 5)
They were uncomfortable with the public knowledge of their infection details, such as their workplaces or restaurants they visited, even after being discharged. The looming possibility of social ostracization and the stigma attached to the term "infected" prevented them from overcoming their depression.
I'm OK, but not OK… I would live with the label, "infected with COVID-19," forever. Everyone knows. At work and all… (Participant 5)
The participants said that they were increasingly intimidated by the changes in their lives after being discharged. They concealed their identities due to the fear of social isolation stemming from negative societal perceptions. They also avoided social interactions due to the fear of reinfection and the potential inconvenience it could cause others. Furthermore, they became more cautious and meticulous in managing their health and controlling infections.
I whispered to my child, "Do not tell others that you have been infected with COVID-19." (Participant 5)
I took thorough measures to prevent the spread of the epidemic. The fear of doing harm to others really kept me alert. That thought was my primary worry. (Participant 9)
Participants whose circumstances compelled them to interact with many people as they returned to work or their business tried to dispel the concerns of those around them by proactively undergoing PCR tests at their own expense.
I took another PCR test at my own expense at the hospital after being discharged. --- I have classes to teach. So I ended up taking PCR tests five times… (Participant 3)
Although the isolation and hospitalization following COVID-19 infection were unfamiliar and challenging experiences that the participants would never wish to repeat, they managed to recover and survive thanks to the comfort and institutional support provided by those around them. They expressed gratitude for the opportunity to reflect and gain a newfound appreciation for the importance of everyday life.
The participants expressed their gratitude towards the staff at the public health center, who provided them with kind assistance throughout their isolation and hospitalization process. They appreciated the staff's attention to detail, as they catered to needs that could have easily been overlooked.
I felt grateful to the (public health center) staff --- There had been a lot of garbage around. They cleaned it up for me, and when we went out, they accompanied me to maintain my privacy from others… (Participant 2)
During their hospital isolation, the participants donned Level D protective clothing and acknowledged the challenges faced by the nurses who also wore this protective gear while caring for them. They expressed gratitude towards the nurses who attended to their minor requests and provided emotional support.
I kept thinking "The nurses are just wonderful, how could they manage to do that?" I am still very thankful for their service and dedication. (Participant 4)
The comfort and support of those around them helped the participants to recover. Thankfully, they were able to completely avoid the financial strain of hospitalization and meal costs through government subsidies.
I thought my students and their parents would react poorly, but the number of people who comforted me was more than I had expected; they wished for my recovery to take care of their children again, which was really empowering. (Participant 4)
I felt blessed that I was living in such a great country… It took care of everything… Good food, no medical expenses, and medication provided when I was feverish… (Participant 7)
Despite their physical and mental exhaustion during hospital isolation, the participants viewed it as a chance to rest, regain their health through healthy routines, and reflect on their hectic lives. Moreover, they expressed gratitude for the new perspective they gained after hospitalization, which underscored the significance of everyday life.
I think it was an opportunity for me to look back on my life, and now I enjoy my work. --- I realized the importance of everyday life. (Participant 8)
Based on their experiences, the participants worked diligently to rectify misinformation and eliminate prejudice related to COVID-19 in both institutional and societal contexts. Their aim was to foster an environment that would safeguard those infected and take into account their unique circumstances.
The participants had been viewing media reports designed to increase awareness about COVID-19. Consequently, when they contracted the virus, they experienced significant fear, which greatly affected their family members and those in their immediate surroundings. However, many participants noted that their symptoms differed from those depicted on television, leading them to desire more accurate information from government agencies.
Psychologically, the consequences of the inability to lead a social life were repeatedly emphasized by the media. I think it would also be helpful to report on people leading their daily lives safely... I wished that the KDCA provided more accurate information since there are people with different symptoms out there. (Participant 3)
The participants were keen to avoid any negative perceptions about them, given that they contracted the infection despite their caution. They understood that their situation was accidental and could happen to anyone.
Honestly, none of us thought, "I will spread it all around and get everyone infected."… I really hope that they would stop the criticism. (Participant 5)
The participants expressed a desire for the identities of COVID-19 patients to remain undisclosed to avoid any undue harm or distress.
Wouldn't it be better to keep people's information private to prevent them from being harmed or hurt? Government subsidies are important, but I want the government to think about this as well. (Participant 3)
The participants faced a threat to their livelihood due to a decrease in income, as they were unable to work while in isolation. Thankfully, they managed to temporarily cover their living expenses by receiving the national subsidy for COVID-19 patients. However, they expressed concern about their future and hoped that the government would provide sufficient institutional support to alleviate their livelihood worries.
My brothers and sisters helped me when I stopped earning money, but I couldn't work for about four to five months. (Participant 10)
The participants said that the psychological counseling service provided by the government was not helpful, as it had become a mere formality, and they hoped for timely interventions.
I needed counseling (by the counseling center) when I was really struggling… They called me long after my discharge when I was busy with my life. They told me to call the center whenever I needed help. I told them I would, and that I was feeling OK at the time. That was it. (Participant 5)
This study aimed to explore and understand the experiences of COVID-19 patients during hospital isolation and early recovery. The goal was to gather foundational data to develop an intervention strategy. This strategy would address the range of psychosocial issues that could emerge during hospital isolation and the subsequent recovery period.
Category 1 represented the participants' disillusionment over the prioritization of protecting the uninfected over treating those who are infected. The participants' confusion during their transfer to hospitals, coupled with the perceived harshness of healthcare workers, contributed to their negative emotions. In the initial stages of an infectious disease, isolation is often deemed the most effective solution. This approach has been adopted by South Korean health authorities in treating patients with COVID-19 [6]. While mandatory isolation is advantageous for public health preservation, it significantly curtails individual freedom [20]. Patients are prone to feelings of anger, confusion, and frustration when they are subjected to the stringent measures of healthcare workers, along with abrupt activity restrictions [21]. Therefore, in the process of implementing isolation measures to shield the public from new infectious diseases, it is crucial to also safeguard the rights of the infected. This can be achieved by providing ample explanation and securing consent, thereby minimizing any violation of their autonomy.
Poor communication within the health system significantly impacted the treatment experiences of COVID-19 patients [22]. The absence of clear guidance on hospital isolation, the deliberate distancing of healthcare workers post-hospitalization, and the feeling of being sequestered in a camp to prevent infection spread rather than for treatment, all contributed to patient confusion and disappointment. Isolation can induce negative psychological states such as anxiety, depression, and aggression, which in turn can negatively affect patients' coping abilities and self-esteem [10]. Consequently, it is crucial to establish a psychological first aid and support system that takes into account the experiences of COVID-19 patients. Additionally, it is important to foster awareness among isolated patients through a precise information delivery system.
Furthermore, the participants believed that residing in a group with other patients exhibiting more severe symptoms, in an inadequately equipped isolation environment, was not beneficial to their health. The adequacy of the isolation space was inversely proportional to the occurrence of mental health-related issues. This aligns with the findings of previous studies, which suggested that inadequate living spaces can negatively impact mental health [23]. The successful operation of isolation facilities hinged on several key factors: the deployment of adequate manpower and medical resources, the provision of therapeutic care, the availability of personal space for privacy, and the maintenance of external connections through various information technologies [24].
Category 2 related to the participants' feelings of physical and mental intimidation, as they unintentionally became agents of disease transmission, despite also being victims of the same infection. This negative perception lingered even after their hospital discharge. As potential infection sources, the participants were isolated from their families and the broader society. Concurrently, their personal information was revealed during the epidemiological investigation, making them susceptible to criticism from mainstream and social media [25]. Physical isolation fosters an "us versus others" dichotomy, with the isolated individuals instantly becoming the "others" and facing stigmatization [26].
The participants in this study felt guilty for unintentionally harming those around them and experienced resentment for being victims themselves. This aligns with the results of previous studies [11]. As their infection led to the closure of schools and workplaces, they developed a strong sense of guilt due to criticism from their families. They were forced to suppress their resentment and frustration [27]. As previous research has indicated, the presence of family members who are vulnerable to infectious diseases, such as the elderly, increases isolated patients' anxiety, requiring emergency psychological interventions [28].
Even after recovering from a novel infectious disease, patients often endure secondary harm in the form of social stigma, which stems from the heightened anxiety society exhibits towards those released from institutional isolation. As recovered patients, they face avoidance within their own homes, making it challenging to discuss their recovery with others [29]. These circumstances not only impede their physical recuperation but also obstruct the restoration of normalcy post-discharge, leading to symptoms such as depression and post-traumatic stress disorder [30]. The escalating concern about the spread and treatment of COVID-19 can muddle societal understanding, generating misinformation and triggering the infodemic phenomenon where unregulated information proliferates [27]. Consequently, it is crucial for public health systems to strive to mitigate the stigma associated with COVID-19 infection. They should advocate for the infected individuals and their families by disseminating accurate information to the public [24].
Category 3 focuses on the care and institutional support provided to patients, which aided their survival and recovery from the challenging periods of isolation and hospitalization they fear to relive. Participants bore psychological scars from the fear of new infectious diseases and negative societal perceptions. These findings align with prior studies that have documented challenges such as shock, isolation, guilt concerning family and friends, and exclusion and discrimination when the community learns of the infection [7, 8, 11]. Notably, over half of the participants in this study were self-employed or freelancers, and they faced criticism and resentment when their infection status was publicly disclosed in local online communities. Regular contact with family and friends was identified as a factor in overcoming a COVID-19 infection [31], aligning with research findings that suggest depression levels decrease as social interaction increases [32]. Moreover, social support was a significant predictor of disaster resilience and post-traumatic growth [32], indicating that social support also plays a crucial role in mitigating the negative effects of COVID-19 and fostering positive adaptation. Consequently, technical support such as remote video calls or the utilization of social resources for disadvantaged individuals should be considered as a strategy to enhance social support.
The participants, whose social interactions were confined solely to healthcare workers within the isolation facility, derived comfort from the warm attitudes of these professionals [31]. These findings underscore the importance of swiftly and effectively implementing empathetic psychological support systems for victims of emerging infectious diseases. Despite experiencing physical and mental exhaustion during their hospital isolation, the participants expressed gratitude for the chance to introspect and appreciate their lives. While the isolation induced negative emotions, the participants managed to avoid dwelling on these feelings by transforming them into opportunities for maturity and growth. A study on Severe Acute Respiratory Syndrome (SARS) revealed the potential for Post-Traumatic Growth (PTG) following an epidemic. Despite the prevalence of negative emotions during the SARS outbreak, some individuals viewed it as a chance to prioritize their family members, leading to "social growth." They achieved "personal growth" by resting, adopting healthier lifestyles, and learning to value everyday life [33]. PTG extends beyond merely returning to a previous state after enduring hardship; it involves a positive reassessment of life. It is crucial to evaluate the potential for PTG following a future COVID-19 pandemic and to identify coping strategies that could predict growth. This would help to mitigate the negative impacts of COVID-19 while fostering PTG.
Category 4 reflected the aspiration for a system capable of rectifying misinformation, eliminating prejudice, and safeguarding those infected. The participants expressed a desire for more precise information from government bodies and measures to prevent negative perceptions and personal exposure, given that anyone could be equally susceptible. The inadequate information supplied by the isolation authorities can induce stress and adversely impact mental health [28]. Consequently, it is vital to provide accurate information about isolation treatment, and relevant organizations must ensure patient anonymity during epidemiological investigations. During patient transportation by ambulance and the isolation process at the patient's residence, personal information often becomes exposed to neighbors. Therefore, patients should be treated with sensitivity throughout the hospitalization and isolation process [31].
The participants expressed a desire for institutional support and prompt psychological counseling interventions to help alleviate their concerns about their livelihoods. The absence of necessary resources and income can lead to ongoing anxiety and anger following isolation [34]. Therefore, institutional support serves as a crucial resource for mitigating additional stress and economic loss for those in isolation. One participant, who did not receive psychological support services during the challenging period of isolation and only received superficial guidance after discharge, highlighted the need for timely psychological support services. The National Center for Disaster and Trauma published specific guidelines for psychological support, including psychological first aid, in relation to COVID-19 in February 2020 [35]. Given that those in isolation often lack prior knowledge about psychological support services and clear guidance [11], it is necessary to provide proactive psychological support services to those experiencing confusion or mental distress due to a COVID-19 infection.
By linking the meanings of categories, this study ultimately derived the theme of "It's okay, but it's not okay." This theme implies that participants, who were inadequately prepared for an emerging infectious disease, experienced a hospital isolation process that seemed to prioritize disease control over their own recovery. Despite the challenges, they gradually resumed their daily routines with the help and support of those around them. However, the lingering trauma of being perceived as the source of infection was not easily overcome. Even after their isolation ended, participants felt the situation was unresolved due to persistent social stigma, which led to their ostracization. They also continued to worry about potentially infecting others [30]. Even after being medically cleared of COVID-19 and discharged, individuals may remain on high alert regarding health management and infection control, leaving a lasting, unhealed wound. Therefore, public health authorities should strive to prevent the exacerbation of mental health issues related to COVID-19 infection by offering ongoing psychosocial support services through local health systems, even after patients have been released from isolation.
There are some limitations of this study. First, the participants were selected through convenience sampling, without taking into account the severity of their conditions. Critically ill patients with altered consciousness were not included, which means potential differences in isolation treatment experiences based on patient severity were not considered. Second, the interviews were conducted one to three months post-discharge, so any recovery experiences beyond this period were not captured. Finally, the study was conducted during a time when strict isolation guidelines from health authorities were in place. Therefore, the isolation experiences may vary once these guidelines are relaxed.
After examining the experiences of COVID-19 inpatients during their hospital isolation and early recovery period, several conclusions were reached. In the dire circumstances of the COVID-19 pandemic, isolating infected individuals proved to be an effective strategy to prevent community transmission. However, when implementing isolation measures under the guise of public protection, it is crucial to prioritize minimizing infringements on autonomy and ensuring the human rights of the infected. Rather than focusing solely on their status as isolated individuals, they should be treated as patients requiring therapeutic care. It is necessary to ensure their well-being in hospital isolation by providing a comfortable physical environment, adequate staffing, and resources, as well as offering detailed guidance on institutional procedures and future progress. Healthcare workers should also address the loneliness these patients may experience by maintaining frequent communication.
This study revealed that participants, even after their isolation period had ended, felt overwhelmed by the physical and emotional toll of COVID-19 during the early stages of recovery. They found it challenging to return to their previous daily routines. Therefore, it is crucial to establish a psychological support system that takes into account the experiences of COVID-19 patients. It is also important to formulate a national policy that addresses the concerns of those in isolation, through measures such as emotional support and financial compensation. Additionally, more research is needed to identify coping strategies that could potentially predict growth, in order to minimize the negative impact of COVID-19 and promote PTG. This study is significant as it explores the psychological, social, and policy considerations necessary when implementing isolation treatment for infected patients during the early stages of emerging infectious diseases like COVID-19 in the future.
CONFLICTS OF INTEREST:Soo Jung Chang has been an editorial board member of the Korean Journal of Adult Nursing since 2019. She has not been involved in the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - CSJ and KGM.
Data collection - CSJ and SSH.
Analysis and interpretation of the data - CSJ, KGM, SSH and KJA.
Drafting and critical revision of the manuscript - CSJ, KGM, SSH and KJA.
 E-SUBMISSION
E-SUBMISSION