PurposeThis study aims to explore the relationship between the discharge process and two-year prognosis in patients with Heart Failure (HF) who were hospitalized because of HF exacerbation. Methods Medical records were reviewed to identify patients admitted for HF exacerbation. Information regarding the following discharge processes was collected: follow-up visits, discharge educational contents, and the presence of family caregivers during patient education. HF-related events, including emergency department visits, readmissions, or death because of HF, were defined as a composite of events. A multivariate Cox proportional hazards regression model was used after adjusting for covariates to explore the association between the discharge process and HF-related events. Results A total of 201 patients were included in this study. In the two-year follow-up periods, 41 patients (20.4%) experienced at least one HF-related event. Follow-up visits were scheduled at an average of 8.11±2.92 days after discharge. Approximately 95.0% of the patients received discharge education with an average of 1.66±1.04 topics, and 69.7% of the families participated in this educational activity. In the multivariate Cox regression model, not having family members during education was associated with a longer time to HF-related events (hazard ratio: 2.09; 95% confidence interval: 1.001~4.346). However, follow-up visits and the amount of educational content received were not associated with time to HF-related events. Conclusion The presence of family caregivers during education appears to be a protective factor against adverse prognosis in patients with HF. Our results highlight the importance of family engagement during discharg
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
This study aims to explore the relationship between the discharge process and two-year prognosis in patients with Heart Failure (HF) who were hospitalized because of HF exacerbation.
Medical records were reviewed to identify patients admitted for HF exacerbation. Information regarding the following discharge processes was collected: follow-up visits, discharge educational contents, and the presence of family caregivers during patient education. HF-related events, including emergency department visits, readmissions, or death because of HF, were defined as a composite of events. A multivariate Cox proportional hazards regression model was used after adjusting for covariates to explore the association between the discharge process and HF-related events.
A total of 201 patients were included in this study. In the two-year follow-up periods, 41 patients (20.4%) experienced at least one HF-related event. Follow-up visits were scheduled at an average of 8.11±2.92 days after discharge. Approximately 95.0% of the patients received discharge education with an average of 1.66±1.04 topics, and 69.7% of the families participated in this educational activity. In the multivariate Cox regression model, not having family members during education was associated with a longer time to HF-related events (hazard ratio: 2.09; 95% confidence interval: 1.001~4.346). However, follow-up visits and the amount of educational content received were not associated with time to HF-related events.
The presence of family caregivers during education appears to be a protective factor against adverse prognosis in patients with HF. Our results highlight the importance of family engagement during discharge.
The number of patients with Heart Failure (HF) continues to increase worldwide, and this number is expected to increase owing to the aging population and advances in medical treatment [1, 2]. However, despite improvements in HF therapy, HF-related events, such as rates of readmission and Emergency Department (ED) visits, remain high [3], with short-term readmission rates ranging from 20% to 25%[4]. In addition, because of the cost of repeated hospitalizations, HF is considered a burden on health-care resources [1, 2, 5].
Researchers have investigated the factors related to poor prognosis (e.g., readmission) in patients with HF. A recent systematic review of models was conducted to predict the risk of readmission in patients with HF [6]. The predictors included in the predictive models for HF were grouped into three categories: clinical (e.g., laboratory values and vital signs), administrative (e.g., demographic variables), and psychosocial (e.g., psychiatric comorbidities and substance abuse). However, the predictive accuracy of these models ranges from poor to acceptable. In addition, it should be noted that the factors included in the predictive models were non-modifiable. This finding implies that additional modifiable factors should be considered to improve the predictive power of the prognosis of patients with HF who are discharged from the index hospital.
Transitional care includes interventions designed to prevent readmission among patients from one care setting to another [7]. Potentially modifiable factors, including those related to transitional care, are often related to the discharge process, such as education and follow-up visits. In addition, transitioning between inpatient and outpatient settings is critical for improving patient outcomes in cases such as HF-related events [3]. Therefore, this study aims to explore the relationship between factors related to the discharge process and HF-related prognosis among patients admitted to the hospital because of HF exacerbation in two years. In this study, prognosis is defined as the composite endpoint of death, rehospitalization, or ED visits because of HF (i.e., HF event-free survival).
This is a cross-sectional retrospective study that uses a medical record review method.
A chart review was conducted using data from discharged patients with HF (International Classification of Disease-10 codes 150.1~150.4, 150.9) in an academic medical center in Korea between January 2014 and March 2017. Eligible patients were admitted because of HF exacerbation and were discharged alive. We initially screened 818 records and excluded 516 because their primary reason for index hospitalization was not related to HF or because they died during index hospitalization. Of the 302 records retained, 101 were excluded because they did not include data on the variables of interest (e.g., living arrangement status and follow-up visits). Thus, 201 records were included in this study.
This study was exempted from approval, and the requirement to obtain informed consent was waived by the Institutional Review Board of 2017-05-025.
Electronic medical records were reviewed to extract the following information from index hospitalization: demographic, clinical, and discharge process information. To identify patient prognosis, patients’ electronic medical records were reviewed for a median of 444 days (interquartile range: 136~705 days) after index hospitalization. Three research nurses collected the data and were trained in a detailed data collection protocol for consistent data extraction. The principal investigator discussed ambiguity with the research nurses.
The discharge process factors included in this study were follow-up visits, patient education regarding HF self-care, and the presence of family caregivers during patient education sessions. A scientific statement from the American Heart Association (AHA) recommended systematic implementation of the principles of transitional care programs to prevent rehospitalizations for at-risk patients with HF [8]. The suggested components of transitional care include medication reconciliation, early post-discharge contact and communication between patients and clinicians, patient education related to self-care, interdisciplinary care coordination, and communicating patient health information to patients and their post-discharge health-care providers [8]. However, a systematic approach to transitional care (e.g., care coordination) has not been implemented in facilities in Korea, including the facility where this study was conducted. At the clinic, most patients are evaluated by the same clinicians during index hospitalization, and medication reconciliation is performed before discharge for all patients.
Of the suggested discharge information listed in the AHA scientific statement, only information about scheduling follow-up visits and patient education on self-care was available in medical records [8]. The number of days until the first scheduled clinic visit after discharge was calculated. The contents of self-care education were consistently available in patients’ medical records. The educational content of HF was categorized as pathophysiology, medication, low-sodium diet, symptom management, and exercise. Information about the presence of family caregivers during patient education was also included as a discharge process factor. The significant role of caregivers in the self-care of patients with HF is well-known [9, 10], and the American Association of Heart Failure Nurses’ position paper clearly states the importance of family involvement in educating patients [11]. Patients with medical records that indicated family involvement in patient education showed that family caregivers also received education.
The outcome of this study was defined as the composite endpoint of the time to the first HF-related event, including HF-related death, rehospitalization, or an ED visit because of HF exacerbation over two years after index hospitalization. This information was abstracted from the patients’ electronic medical records for up to two years after index hospitalization.
For demographic information, we collected data on age, sex, educational level, and living arrangements (living alone vs. living with others). For clinical information, we collected data on the left ventricular ejection fraction, etiology of HF, changes in weight between admission and discharge, number and names of discharge medications, and comorbid conditions. Finally, comorbidity burden was measured using the Charlson Comorbidity Index (CCI) [12], which is the sum of the weights for each condition. Comorbidity burden can be categorized as mild (1~2), moderate (3~4), or severe (≥5) [12].
To compare the patients’ demographic and clinical information, as well as information related to the discharge process between patients with and without HF-related events, an independent t-test, χ2 test, or Fisher’s exact test was conducted, as appropriate. Multivariable Cox proportional hazards regression was used after adjusting for age and changes in weight between admission and discharge to examine whether each discharge process factor predicted HF event-free survival: number of days to follow-up visits, the amount of educational content patients received regarding HF before discharge, and participation of family members during patient education sessions. All statistical analyses were performed using SPSS version 20.0 (IBM, Armonk, NY, USA). Statistical significance was set at p<.050.
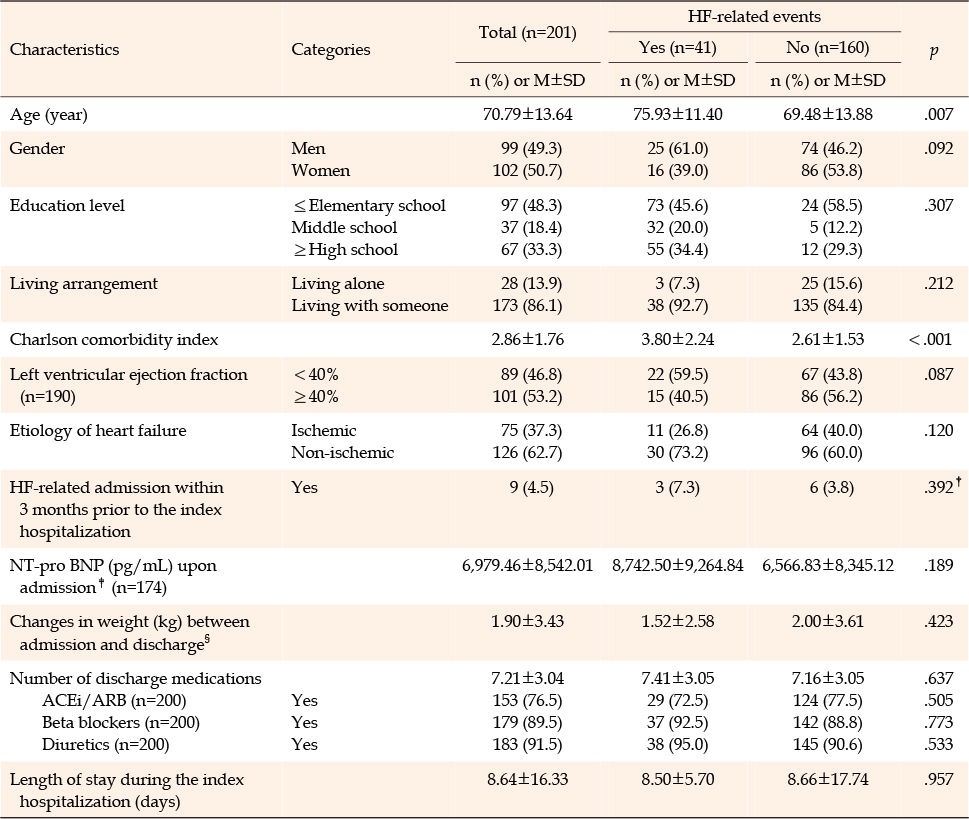
A total of 201 patients were included in the study, with similar proportions of women (50.7%) and men (49.3%) (Table 1). The mean age was 70.79±13.64 years. The majority had education below high school (66.7%), lived with others (86.1%), and had a non-ischemic HF etiology (62.7%). The proportion of patients with a reduced ejection fraction less than 40% was 46.8%. Patients stayed during index hospitalization for an average of 8.64±16.33 days. A comparison of the characteristics of patients with and without HF-related events indicated that patients with HF-related events were more likely to be older and have higher CCI scores than those without (p<.001).
Table 1 Sample Characteristics (N=201)
On average, follow-up visits were scheduled for approximately 8.11±2.92 days after discharge (Table 2). There were 59.2% of the patients who were scheduled for follow-up visits within one week of discharge. Education about HF before discharge was provided to 95.0% of the patients (n=191). HF educational content that was most frequently covered was related to medications (94.0%), followed by symptom management (41.8%), exercise (15.4%), a low-sodium diet (12.9%), and pathophysiology (1.5%). More than two-thirds of the patients (69.7%) were educated, along with their family members. There were no differences in the discharge process factors between patients with and without HF-related events, except that the patients with HF-related events received education about pathophysiology (Table 2).
Table 2 Factors Related to the Discharge Process
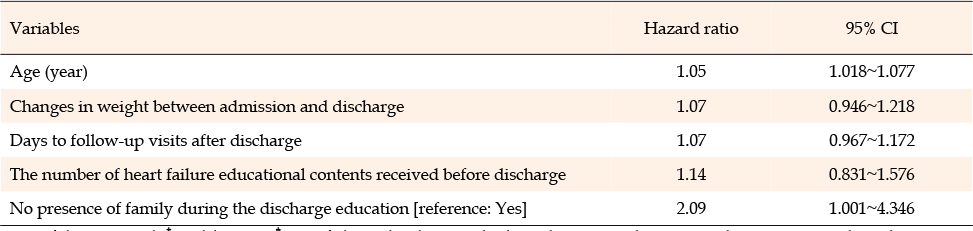
During the follow-up period (median, 444 days), one patient died because of HF-related reasons, and 40 patients had at least one of the following HF-related events: HF-related ED visits (n=3) or readmissions (n=37). In the multivariate Cox regression model (Table 3), after adjusting for covariates, patients without a family member present during educational sessions were 2.09 times more likely to have a shorter length of HF event-free survival (hazard ratio: 2.09; 95% confidence interval [CI]: 1.001~4.346). Among the covariates included in the model, age was associated with HF event-free survival; older patients were 1.05 times more likely to have a shorter time to HF event-free survival (hazard ratio: 1.05; 95% CI: 1.018~1.077).
Table 3 Multivariate Cox Regression Analysis† for Heart Failure-related Events‡ (N=201)
An additional multivariate Cox regression analysis was conducted to explore the relationship between the presence of family caregivers during educational sessions and time to HF event-free survival based on patients’ living arrangements. However, because only three patients who lived alone had HF-related events, additional analysis was conducted with patients who lived with someone. Patients who lived with someone but did not have a family member present during the discharge educational session were 2.19 times more likely to have a shorter HF event-free survival (hazard ratio: 2.19; 95% CI: 1.030~4.653).
This study examined whether discharge process factors are associated with HF event-free survival. We found that the participation of family members in patient educational sessions was related to longer HF event-free survival but was not related to either the number of days to follow-up visits or educational contents received before discharge. This result implies that when learning more about HF and HF management, it is helpful for family members to be educated as well so that they can help patients manage HF and potentially prevent adverse prognoses.
The immediate post-discharge period is called the “vulnerable phase” of hospitalization for HF [13]. A successful discharge process for this period as part of a transitional care program can help patients avoid preventable rehospitalization. In the United States, the Centers for Medicare and Medicaid Services have implemented several programs to decrease avoidable readmissions by improving the quality of care transition when patients are discharged from hospitals [14]. One of the most important quality measures in care transition is patient discharge education. According to a systematic review and meta-analysis by Fischer et al., the overall effect of providing HF discharge instructions on the time during repeated hospitalizations in patients with HF was not significant [15]. Similarly, in our study, the amount of educational content on HF before discharge was not associated with time to HF-related events.
Despite the significance of having family members present during educational sessions, the results of our study and that by Fischer et al. should be interpreted with caution. First, only three studies were included in Fischer et al.’s study to estimate the pooled effect of the discharge instructions. Second, the academic medical center where the data were collected for our study had no guidelines for nurses on how to educate patients and what content should be included. Nurses are in an ideal position to contribute to the outcomes of the discharge process, particularly discharge education [3]. However, given the lack of guidelines, the patients in our study only received verbal HF education from their nurses in an inconsistent manner.
Previous studies have suggested the importance of providing patient education so that patients have a comprehensive understanding of HF, symptoms, and self-care [16, 17]. However, in our study, education about a low-sodium diet, symptom management, and exercise was not provided to the majority of patients with HF. Thus, the lack of association between the number of discharge educational content received and HF-related prognosis might be explained in part by the limited educational content or quality of teaching strategies. To improve the quality of discharge education, system-level support, such as developing and standardizing educational content and training nurses on how to teach patients the necessary knowledge and skills to manage HF, is required. Because nurses play a key role in patient education, they can take the initiative to improve transitional care for patients with HF in Korea. In particular, they should adapt the recommendations developed in the United States [8] for transitional care of patients with HF in Korea.
Including families in discharge education and planning sessions is mandatory in some areas of the United States [18]. Specifically, investigators have described the important role of social support in HF management [9, 10] and have suggested that informal caregivers should be included in inpatient discharge education [11]. Our findings further support the claim that family members who participated in inpatient discharge education usually had better outcomes. However, simply living with others was not associated with event-free survival in the present study, which appeared to contradict the positive effect of family caregivers’ presence during discharge education on HF management, as living with someone was often considered a proxy for social support. A few studies have found a negative effect on patients’ self-care when informal caregivers are not knowledgeable about HF management [19]. For example, in one study, when patients with HF informed others, including their family members, about their worsening symptoms, some family members suggested that the patient should relax and gave other inappropriate advice about the patients’ symptom status, which resulted in a delay in seeking care [20]. In addition, caregivers’ preparedness to meet patients’ physical and emotional needs was associated with their contribution to self-care in HF [21]. Our findings further highlight the importance of family caregivers’ presence in discharge education, along with patients, to be helpful for the better management of HF. However, the point estimate of the presence of family caregivers during discharge education may not be reliable given that the 95% confidence interval is relatively wide owing to the small number of HF-related events in our study.
An early follow-up appointment within the first week of discharge is recommended by the AHA [8]. Most patients in our study were scheduled to visit their cardiologists within one week, and there were no differences in the number of days to follow-up visits between patients with and without HF-related events. This finding demonstrates an overall high adherence rate to follow-up visit scheduling after hospital discharge in patients with HF.
Furthermore, we found that patients with HF-related events were more likely to be older than those without HF-related events. Numerous studies have identified age as a risk factor for poor HF-related prognosis after discharge from index hospitalization [22, 23, 24]. Given the significant relationship between age and an adverse prognosis in patients with HF, it may be more important to promote the participation of family members of older patients in discharge education, as older patients may experience difficulty understanding the content.
This study has some limitations. Data were collected only by reviewing medical records. Because the information in medical records depends on clinician documentation, certain information may not be available, or records may be incomplete. For example, detailed information about family members who participated in discharge education, such as their relationship with the patient, family members’ level of HF knowledge, and whether family members lived with the patients, was unavailable. The number or length of educational sessions was also unavailable in the medical records. Because there are no formal discharge education guidelines for HF in the study hospital (based on a review of medical records) and most hospitals in Korea, it is unknown whether nurses tailored the depth of educational content and the number of education sessions depending on the patient’s situation (e.g., de novo HF vs. chronic HF). The functional status level at hospital discharge (e.g., New York Heart Association functional class), which can be an important predictor of HF-related events, was also unavailable because the information was not routinely recorded in medical records. In addition, we did not collect information on whether the patients had acute de novo HF or chronic HF exacerbations associated with readmission. Finally, this study was conducted at a single academic medical center, which might limit the generalizability of the findings.
This study aimed to explore the factors associated with the discharge process of event-free survival in patients with HF. The presence of family caregivers in educational sessions was found to be a protective factor against adverse prognosis in patients with HF. Our results highlight the importance of family engagement in managing HF. Therefore, clinicians should develop strategies to increase the participation of family members in the discharge process. However, no relationship was found between the educational content and patient prognosis. This result should be interpreted with caution because critical information related to education (e.g., depth of content and education modalities) was unavailable in the medical records. Therefore, further studies are required to examine the relationship between the discharge process and prognosis of patients with HF.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - LKS.
Data collection - LKS, MNE and PJH.
Analysis and interpretation of the data - LKS, LH, and MNE.
Drafting and critical revision of the manuscript - all authors.
This following funding supported this research: (1) the National Research Foundation of Korea grant funded by the Korean government (MEST; grant number: 2016R1A2B4008495); (2) BK21 Four Project (Center for Human-Caring Nurse Leaders for the Future) funded by the Ministry of Education (MOE, Sejong, Korea) and National Research Foundation of Korea (NRF).
Download a citation file in RIS format that can be imported by all major citation management software, including EndNote, ProCite, RefWorks, and Reference Manager.

 E-SUBMISSION
E-SUBMISSION