
Purpose
The aim of this study was to identify the coping profiles of patients with coronary artery disease and to examine their associations with cardiac health behavior.
Methods
In this cross-sectional study, data from 203 patients undergoing percutaneous coronary intervention for coronary artery disease were analyzed. Data collection occurred between September 2020 and June 2021, utilizing self-report questionnaires and electronic medical records at a cardiology outpatient clinic. Descriptive statistics, latent profile analysis, and logistic regression were employed for data analysis.
Results
The Type I coping profile was characterized by the greater use of most coping strategies, particularly problem-focused approaches, relative to the other profiles. The Type II coping profile exhibited below-average use of all coping strategies, except for substance use. The Type III coping profile displayed higher tendencies toward venting, self-blame, denial, behavioral disengagement, and substance use compared to the other profiles. Patients with the Type I coping profile displayed greater engagement in cardiac health behavior than those with Type II and Type III, as indicated by odds ratios of 2.57 (95% confidence interval=1.31~5.07) and 7.19 (95% confidence interval=2.10~24.56), respectively.
Conclusion
Participation in cardiac health behavior varies according to the coping profiles of patients with coronary artery disease. Healthcare providers should recognize and support appropriate coping strategies in these patients to promote healthy behaviors. A longitudinal study investigating how changes in coping profiles relate to cardiac health behavior could assist patients with coronary artery disease in maintaining such behaviors.
The aim of this study was to identify the coping profiles of patients with coronary artery disease and to examine their associations with cardiac health behavior.
In this cross-sectional study, data from 203 patients undergoing percutaneous coronary intervention for coronary artery disease were analyzed. Data collection occurred between September 2020 and June 2021, utilizing self-report questionnaires and electronic medical records at a cardiology outpatient clinic. Descriptive statistics, latent profile analysis, and logistic regression were employed for data analysis.
The Type I coping profile was characterized by the greater use of most coping strategies, particularly problem-focused approaches, relative to the other profiles. The Type II coping profile exhibited below-average use of all coping strategies, except for substance use. The Type III coping profile displayed higher tendencies toward venting, self-blame, denial, behavioral disengagement, and substance use compared to the other profiles. Patients with the Type I coping profile displayed greater engagement in cardiac health behavior than those with Type II and Type III, as indicated by odds ratios of 2.57 (95% confidence interval=1.31~5.07) and 7.19 (95% confidence interval=2.10~24.56), respectively.
Participation in cardiac health behavior varies according to the coping profiles of patients with coronary artery disease. Healthcare providers should recognize and support appropriate coping strategies in these patients to promote healthy behaviors. A longitudinal study investigating how changes in coping profiles relate to cardiac health behavior could assist patients with coronary artery disease in maintaining such behaviors.
Coronary Artery Disease (CAD) is the leading cause of mortality worldwide, accounting for 16.0% of all global deaths. In the two decades following the year 2000, its mortality rate sharply increased from about 2 million to 8.9 million deaths [1]. CAD represents 56.1% of all heart disease cases, and the number of patients with this condition has risen by 12.9% over the past 5 years [2]. Patients with CAD often undergo Percutaneous Coronary Intervention (PCI) to treat arterial occlusion. However, a meta-analysis of 19 recent randomized clinical trials revealed that within 5 years of stent placement, the incidence of major cardiovascular adverse events-including death and myocardial infarction-was 9.4%, with diabetes and smoking identified as significant risk factors [3]. In a Korean study, 52.3% of patients with CAD continued to smoke after PCI, and 33.1% reported consuming alcohol at least weekly following the procedure. Additionally, individuals with CAD generally engaged in low levels of aerobic physical activity [4]. These results indicate that many such patients maintain unhealthy lifestyle practices.
For patients with CAD, cardiac health behavior includes engaging in regular physical activity, abstaining from smoking, following a balanced diet, managing stress effectively, and taking personal responsibility for one's health to improve and maintain cardiac wellness [5]. In such patients, adherence to a healthy lifestyle significantly reduces the incidence of adverse cardiovascular outcomes, such as cardiac arrest, mortality, myocardial infarction, and revascularization [6]. The difficulty faced by patients with CAD in adhering to recommended cardiac health behaviors for the prevention of complications and recurrence highlights the challenges associated with modifying entrenched health-related behaviors [4]. Coping strategies have been identified as a means to facilitate cardiac health behavior in patients with CAD [7]. Consequently, understanding coping strategies is essential for promoting cardiac health behavior among these patients.
Coping is an adaptive process that aids in problem resolution by adjusting an individual's emotional response to their environment and modifying their perception of stressful situations [8]. Several studies have identified links between coping strategies and cardiac health behavior [7, 9, 10]. Active coping strategies are instrumental in promoting behaviors that support cardiac health, such as regular physical activity and smoking cessation, which are crucial for the secondary prevention of CAD [7]. In research conducted among African Americans, religious coping was shown to positively influence physical activity, diet, smoking habits, and scores on the American Heart Association's Life's Simple 7 [9]. In contrast, coping strategies such as denial, substance use, self-blame, and behavioral disengagement tend to hinder the management of chronic diseases like cancer and heart disease, potentially worsening these conditions and leading to depression, anxiety, distress, and a diminished quality of life [10]. Among patients with CAD, participation in cardiac rehabilitation increases when coping strategies such as task-oriented approaches and social support are employed [11]. Therefore, understanding the coping profiles of individuals who maintain positive cardiac health behavior can be instrumental in creating effective training programs on coping skills for patients with CAD.
Coping strategies appear to differ significantly between the general population and patients with CAD. The former predominantly utilize problem-focused and avoidance strategies, while the latter more commonly employ emotion-focused coping in addition to problem-focused approaches [12]. Ford et al. [13] introduced the concept of multiple conditioning, which refers to the simultaneous or sequential use of multiple coping strategies for a stressor, also termed a coping profile. This concept more accurately reflects how individuals manage stressors. Previous research on coping adaptability has employed three approaches: 1) examining individual coping strategies, 2) categorizing strategies into groups such as emotion- and problem-focused or approach-and-avoidance coping, and 3) exploring the combinations of strategies used by individuals [14]. However, most studies examining the coping profiles of patients with CAD are limited; they may only partially reflect the multidimensional interrelationships of coping, such as by analyzing a single coping strategy or focusing on the frequency of their use [12, 15].
Recently, Latent Profile Analysis (LPA) has been employed to examine combinations of coping strategies by presupposing the existence of latent classes and assigning individuals to these classes based on observed scoring patterns [14]. LPA identifies combinations of relationships within groups based on similar response patterns among individuals, thereby uncovering differences in characteristics that define distinct subgroups [16]. Although recent studies have investigated coping strategy combinations among individuals with cancer or in specific contexts, research on the association between coping patterns and cardiac health behavior in patients with CAD is notably lacking [14, 15]. Consequently, this study aimed to explore the coping profiles of patients with CAD using the Brief Coping Orientation to Problems Experienced (Brief-COPE) inventory [17], to examine the relationship between these profiles and cardiac health behavior, and to identify sociodemographic and disease-related characteristics associated with each profile.
This study analyzed secondary data derived from prior research [18]. The previous study examined 228 outpatients, aged 18 years or older, who had undergone PCI for CAD and visited the cardiology outpatient department at a university hospital in Metropolitan B, Korea. The research excluded individuals diagnosed with severe illnesses such as end-stage renal disease, cancer, or stroke in the previous year, as well as those with cognitive impairments. In the present study, questionnaires with more than 10% missing values for the Brief-COPE inventory (n=2) and participants over 75 years old (n=23) were omitted from the analysis. A prior study utilizing data from the Korea National Health and Nutrition Examination Survey, which categorized age groups into 65~75 years and ≥76 years, demonstrated that the prevalence and risk of CAD were significantly higher in the ≥76-year group [19]. To minimize the impact of advanced age on the present study, individuals aged 76 and older were excluded, resulting in a final sample of 203 patients between 18 and 75 years old. LPA is generally more suitable for larger sample sizes; however, the required sample size depends on a variety of factors [20]. Notably, the sample size does not appear to impact the power of the Akaike Information Criterion (AIC) or entropy [20], and the Bayesian Information Criterion (BIC) and Sample Size Adjustment BIC (SABIC) do not provide greater power with a larger sample [20]. Instead, statistical power is influenced by the quality and quantity of indicators [21]. The use of high-quality and/or numerous indicators (more than five) can compensate for a smaller sample size, such as the approximately 200 participants enrolled in this research. This compensation is accomplished by increasing statistical power, improving the accuracy of parameter estimation, and reducing bias [21]. Since the Brief-COPE instrument used in this study comprises 14 indicators, a sample size of 200 or greater was considered suitable. Therefore, a minimum sample size of 200 participants was established.
The sociodemographic measures assessed included sex, age, living status, education level, occupation, and monthly household income, as reported by participants through a self-report questionnaire. Disease-related characteristics were obtained from hospital medical records and included the time elapsed since the initial PCI, whether the patient underwent one or multiple PCI procedures, the left ventricular ejection fraction, and the number of comorbidities, as well as the presence of diabetes, dyslipidemia, and hypertension.
The Korean version of the Brief-COPE was used to determine the coping profiles of the participants [22]. The Brief-COPE is a 28-item instrument designed to evaluate how individuals cope with stressors [17]. It consists of 14 subscales: self-distraction, active coping, denial, substance use, use of emotional support, use of instrumental support, behavioral disengagement, venting, positive reframing, planning, humor, acceptance, religion, and self-blame. The Brief-COPE scales [17] classify coping strategies into three domains: problem-focused coping, which involves adaptive management of stressors; emotion-focused coping, which often entails maladaptive control of emotions in situations that are uncontrollable; and avoidant coping, which is maladaptive but can be effective in the short term. Each item on the scale is rated on a scale from 1 ("I have not been doing this at all") to 4 ("I have been doing this a lot"), with higher scores reflecting greater use of a given strategy. In previous research, the Cronbach's α for the Brief-COPE ranged from .50 to .90 according to Carver [17] and from .52 to .85 for the Korean version [22]. In the present study, the Cronbach's α values were as follows: .68 for active coping, .76 for use of instrumental support, .80 for planning, .61 for positive reframing, .40 for venting, .76 for use of emotional support, .77 for humor, .73 for acceptance, .54 for self-blame, .84 for religion, .70 for self-distraction, .57 for denial, .93 for substance use, and .62 for behavioral disengagement.
The Cardiac Health Behavior Scale for Korean adults was utilized to assess the cardiac health behavior of the participants [5]. The scale was developed through exploratory factor analysis, which identified a five-factor, 21-item model. This model was subsequently validated through confirmatory factor analysis [5]. The five domains of the scale are health responsibility (five items), exercise (four items), dietary behavior (six items), stress management (three items), and smoking cessation (three items). Responses to each item are scored using a 4-point Likert scale that ranges from 1 ("never") to 4 ("routinely"), with higher scores reflecting more favorable cardiac health behavior. In the research conducted by Song et al. [5], the Cronbach's α coefficients were reported as follows: .83 for the overall scale, .76 for both health responsibility and exercise, .70 for dietary behavior, .58 for stress management, and .70 for smoking cessation. In the present study, the Cronbach's α coefficients were .88 overall, .82 for health responsibility, .82 for exercise, .82 for dietary behavior, .80 for stress management, and .72 for smoking cessation.
The data collection process for this study has been detailed in previous research [18].
Ethical approval for this study was waived by the Pusan National University Institutional Review Board (PNU IRB/2021_167_HR) due to its use of existing data from the primary study. The primary research adhered to the principles of the Declaration of Helsinki and received approval from the Institutional Review Board of Pusan National University Hospital (H-2007-025-093). All participants in the primary study provided written informed consent, and the data used in this study were anonymized with serial numbers.
To evaluate the correlations among the 14 subscales of the Brief-COPE used in the LPA, Pearson correlation coefficients were calculated. LPA was conducted to categorize the latent coping profiles of participants. Each participant's latent profile was determined probabilistically, with individuals assigned to the most likely subgroup. AIC, BIC, and SABIC values were utilized to identify the optimal number of potential profiles. Given that BIC is a more reliable indicator than AIC and SABIC for determining a latent class model with a small sample size [20], it was the preferred information criterion in this study. The Lo-Mendell-Rubin Likelihood Ratio Test (LMR-LRT) and Bootstrap Likelihood Ratio Test (BLRT) were employed to validate models with varying numbers of profiles. Additionally, the quality of classification of the latent profile models was assessed using the entropy index. A model was considered to provide good classification if the entropy value exceeded 0.8 [20]. In this research, the number of latent profiles was chosen by considering the ratio and interpretability of each profile, in conjunction with the information index and entropy values [16].
The normality of the main variables was assessed using the Shapiro-Wilk test. For variables that were not normally distributed, nonparametric tests were employed. To examine the sociodemographic and disease-related characteristics of the participants according to their coping profiles, we used the Pearson χ2 and Kruskal-Wallis tests, applying the Bonferroni correction for post hoc analysis. Analysis of variance was then utilized to ascertain whether significant differences existed among coping profiles in terms of cardiac health behavior. Paired comparisons were also conducted between the identified coping profiles and cardiac health behavior, employing binomial logistic regression analysis to calculate odds ratios (ORs) and 95% confidence intervals (CIs). All tests of statistical significance were two-tailed, with a threshold of p<.05. Descriptive statistics were analyzed using SPSS 26.0 (IBM Corp., Armonk, NY, USA). For LPA, we used the tidyLPA package in R (R Foundation for Statistical Computing, Vienna, Austria).
Correlation analysis of the Brief-COPE scale revealed strong correlations between the following variables: use of emotional support and use of instrumental support (r=.74, p<.001), positive reframing and planning (r=.69, p<.001), self-distraction and active coping (r=.68, p<.001), positive reframing and acceptance (r=.60, p<.001), acceptance and use of emotional support (r=.63, p<.001), and positive reframing and use of instrumental support (r=.57, p<.001) (Table 1).
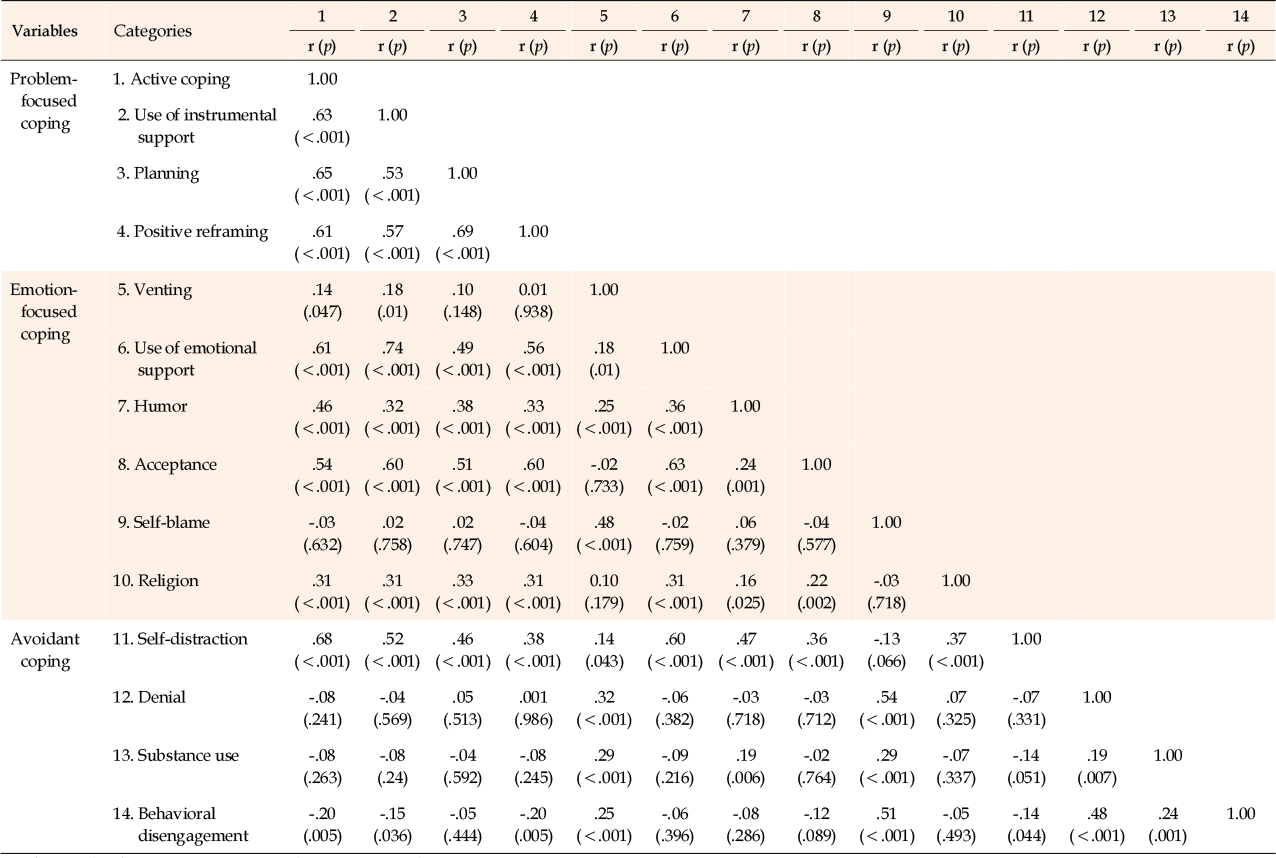
Table 1
Correlations within the Brief-COPE
Conversely, the analysis also identified several variables that did not exhibit significant correlations within the Brief-COPE scale. For instance, self-blame displayed no significant correlations with active coping, planning, positive reframing, use of instrumental support, humor, acceptance, denial, religion, self-distraction, substance use, and behavioral disengagement. Similarly, denial was not significantly correlated with active coping, use of instrumental support, planning, positive reframing, humor, acceptance, substance use, and behavioral disengagement (Table 1). Furthermore, substance use did not demonstrate significant correlations with active coping, use of instrumental support, planning, positive reframing, acceptance, and behavioral disengagement (Table 1).
To determine the optimal number of latent profiles based on coping strategies, the number of profiles was incrementally increased from two to six. This process involved examining model comparisons, information criteria, and classification quality (Figure 1). Both AIC and SABIC values decreased as more profiles were added. The LMR-LRT p-values for models ranging from two to six classes were all below .001. Similarly, BLRT yielded p-values indicating significance for models with two to six classes. The three-class model demonstrated the lowest Consistent AIC (CAIC) (9,942.85) and BIC (9,884.85) values, indicating superior fit. Furthermore, an entropy value of 0.92 in the three-class model indicated a high level of classification accuracy. Consequently, the three-class model was selected as the most appropriate for analyzing coping profiles (Figure 1).
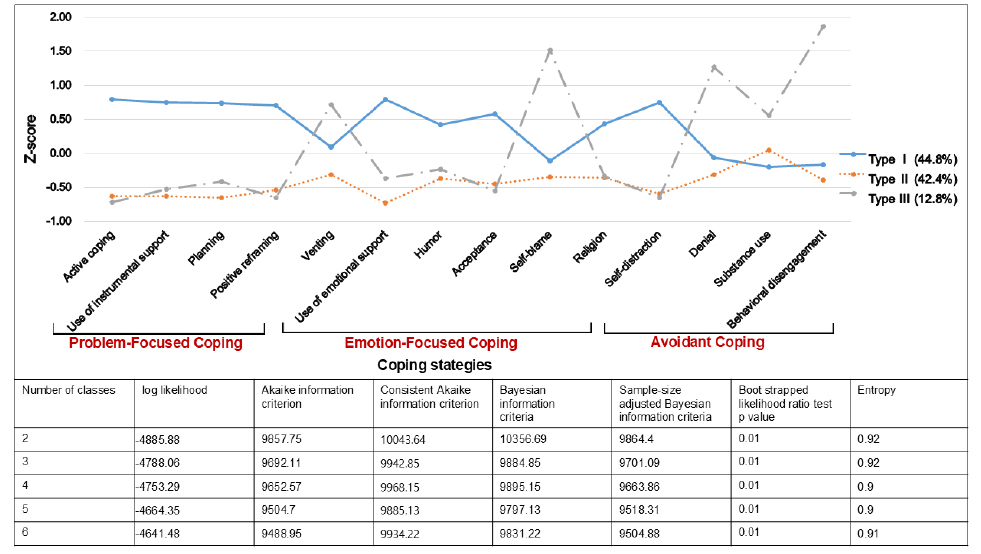
Figure 1
Coping profiles of participants.
The Type I coping profile was characterized by above-average scores for most coping strategies, with the most pronounced results for problem-focused coping methods. These included active coping, use of instrumental support, planning, and positive reframing. Among emotional coping strategies, these participants tended to employ emotional support, while among avoidance coping, they used self-distraction. In contrast, those with the Type II coping profile demonstrated poor use of coping strategies, with all coping strategies scoring below average except for substance use. Finally, the Type III coping profile exhibited a higher tendency toward venting, self-blame, denial, behavioral disengagement, and substance use than the other coping profiles. The scores for the remaining strategies were below zero, mirroring the Type II coping profile (Figure 1). The distribution of participants across coping profiles was 44.8% for Type I, 42.4% for Type II, and 12.8% for Type III.
Figure 1 illustrates significant differences in detailed coping strategy scores across the three coping profiles. The Type I coping profile exhibited significantly higher scores in active coping, use of emotional support, self-distraction, use of instrumental support, planning, positive reframing, acceptance, religion, and humor compared to the Type II and Type III coping profiles. The score for venting was significantly lower for the Type II coping profile than for Type I and Type III. Additionally, denial, self-blame, behavioral disengagement, and substance use scores were significantly higher for the Type III coping profile than for Type I and Type II.
Table 2 presents the sociodemographic and disease-related characteristics of the participants according to their coping profiles. Education level (χ2=10.32, p=.035) and monthly household income (χ2=13.16, p=.041) differed significantly among the three coping profiles.
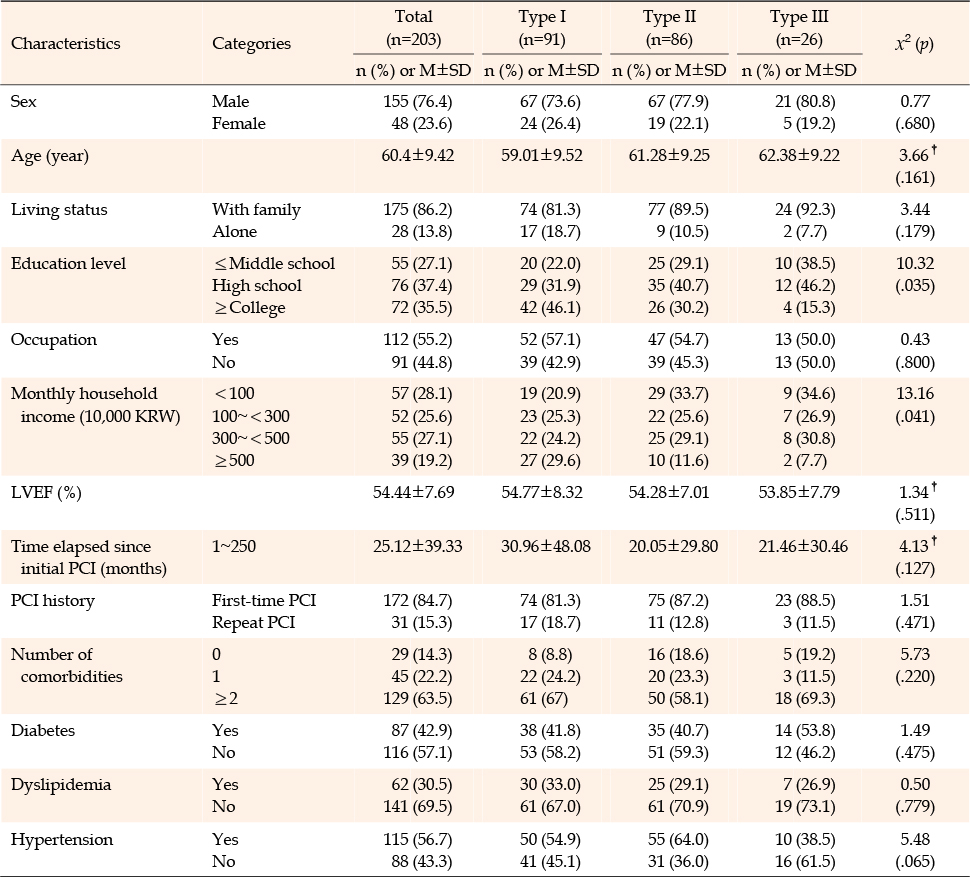
Table 2
Participant Characteristics and Association between Coping Profiles (N=203)
Table 3 details the differences in cardiac health behavior across coping profiles. The Type I coping profile attained the highest scores for cardiac health behavior, differing significantly from Type II and Type III (F=8.63, p<.001). Similarly, for health responsibility, the Type I coping profile scored significantly higher than Type II and Type III (F=8.83, p<.001). In the exercise category, the Type I coping profile again achieved the highest scores, differing significantly from Type II and Type III (F=3.97, p=.020). Likewise, regarding stress management, the Type I coping profile maintained the highest scores, with a significant difference from Type II and Type III (F=12.33, p<.001).
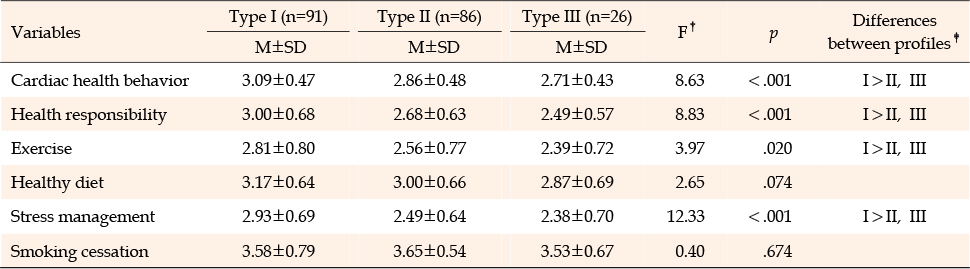
Table 3
Differences in Cardiac Health Behavior between Coping Profiles (N=203)
Figure 2 presents the results of pairwise comparisons of coping profiles, with binary logistic regression analysis employed to examine the associations between coping profiles and engagement in cardiac health behavior. Patients with the Type I coping profile were 2.57 times more likely to perform cardiac health behavior (OR=2.57, 95% CI=1.31~5.07) than those with the Type II coping profile and 7.19 times more likely (OR=7.19, 95% CI=2.1~24.56) than those with Type III coping profile. There was no statistically significant difference between patients with type II and Type III coping profiles regarding the degree of cardiac health behavior (OR=2.02, 95% CI=0.74~5.54).
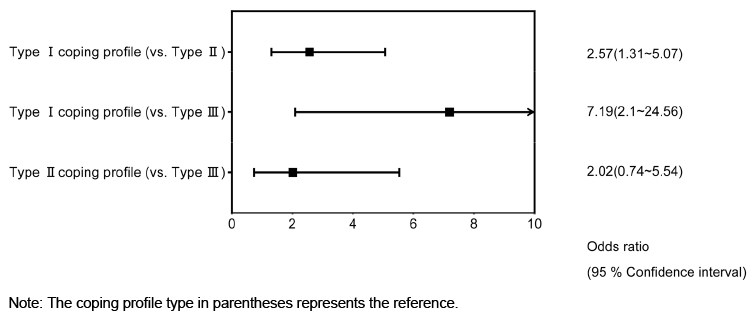
Figure 2
Comparison of odds ratios between coping profiles for cardiac health behavior.
This study aimed to identify the coping profiles of patients with CAD and to investigate whether levels of cardiac health behavior differ according to profile. We identified three distinct coping profiles among patients with CAD. Type I and Type II coping profiles were each observed in over 40% of the participants, suggesting that they may be representative of the coping strategies employed by these patients. Participants with Type I coping profile displayed greater engagement in cardiac health behavior than those with other profiles, as evidenced by ORs of 2.57 to 7.19. No significant differences were found in cardiac health behavior participation between patients with Type II and Type III coping profiles. Therefore, the Type I coping profile appears to be associated with a greater potential for effective coping, which is crucial for successful cardiac rehabilitation and health promotion.
As the number of profiles increased, continuous decreases were observed in AIC and SABIC values. Thus, greater model complexity led to reduced information loss and more effectively captured data variability [20]. p-values for LMR-LRT and BLRT across all models suggested that each additional class significantly improved data classification [20]. The LMR-LRT and BLRT tests assessed differences in model fit, with the p-values confirming that the inclusion of additional classes significantly increased the fit of the model. The three-class model demonstrated the lowest CAIC and BIC values, indicating that it was the most appropriate choice. Furthermore, the entropy value of 0.92 for the three-class model-the highest among the models tested-revealed outstanding classification accuracy and clear differentiation between classes [20]. Thus, the three-class model provided excellent fit and high classification accuracy, effectively distinguishing individuals with diverse coping strategies and supporting the development of tailored interventions.
Participants with Type I coping profiles employed both problem-focused and emotion-focused coping strategies more than patients with other coping profiles. Previous research indicated that 33.6% of individuals experiencing acute myocardial infarction utilized problem-focused coping, while 53.6% used emotion-focused strategies [12]. A prior study described a "problem-focused engagement" coping profile that involved planning and cognitive restructuring, which aligns with the active coping, planning, positive reframing, and acceptance strategies identified in this study [23]. Notably, participants with the Type I coping profile in this study were distinguished by their high use of humor as a coping strategy. Prior research has suggested that humor, an emotion-focused approach, serves as a stress buffer by reframing stressful events as more positive and less threatening experiences, thus reducing distress [24]. Additionally, distraction, which is considered an avoidance coping strategy, was commonly observed among participants with the Type I coping profile. Engaging in alternative activities to divert attention from problems has been suggested as an effective adaptation strategy for managing stress [25]. Thus, enhancing the coping strategies associated with the Type I coping profile could potentially improve stress adaptation, health-related quality of life, and survival rates, while reducing the recurrence of adverse events [23].
Conversely, participants with the Type II coping profile primarily relied on substances such as alcohol and tobacco to manage their stress. Correspondingly, they used other coping strategies less frequently, representing a passive approach to the disease. This response has been shown to negatively impact cardiac health behaviors, including participation in rehabilitation programs. A previous study indicated that approximately 21.5% of patients with CAD adopted coping strategies akin to Type II coping profiles and were less actively involved in cardiac rehabilitation [12]. Research conducted during the coronavirus disease 2019 isolation period showed that 26.9% of participants utilized few coping strategies overall and reported higher levels of depression, anxiety, and stress compared to those with a more engaged profile, who primarily used problem-focused coping strategies. This suggests that psychological interventions are needed for these individuals [14]. Moreover, the Type II coping profile, characterized by substance use rather than active management of disease-related challenges, has been shown to adversely affect the prognosis of CAD [6]. Interventions that can reduce such behavior are urgently needed.
Participants with the Type III coping profile were characterized by significantly higher self-blame, denial, and behavioral disengagement scores compared to those with the other profiles. Similarly, a previous study found that patients with CAD often resort to coping methods like self-blame and denial [11]. Behavioral disengagement coping strategies may involve blaming oneself for contracting the disease, denying its presence or severity, or reducing or abandoning efforts to address disease-related factors. Individuals with Type III coping profiles rarely engaged in problem-solving or emotion-focused coping, potentially leading to a decreased likelihood of seeking assistance from others and a lower propensity to confront problems directly. This behavior can delay critical health-related decisions, resulting in delayed hospital visits and suboptimal disease management; ultimately, poor health outcomes are the result [26]. Consequently, it is essential to implement educational interventions that encourage those with Type III coping profiles to shift from maladaptive strategies such as self-blame, denial, and behavioral disengagement to more beneficial coping strategies, including active coping, planning, and emotional coping, which can positively impact their health outcomes [6].
The three distinct coping profiles identified in this study exhibited differences in education level and monthly household income. Among participants with a Type I coping profile, 46.1% had a college degree or higher, while 29.6% reported a monthly household income of 5 million won or more (the highest income category), representing a greater proportion than the other coping profiles. In contrast, within the Type II and III coping profiles, 40.7% of participants in the Type II coping profile and 46.2% in the Type III coping profile had attained at least a middle school education, with over 30.0% reporting a monthly household income of less than 1 million won. Previous research has shown that individuals employing coping strategies such as acceptance, positive reframing, and planning-hallmarks of the Type I coping profile-tend to have higher monthly household incomes and education levels [27]. Conversely, chronically ill patients with low education levels and monthly household incomes often employ coping strategies like avoidance, self-blame, and denial [28]. This suggests a relationship between monthly household income, education level, and the use of specific coping strategies. Moreover, Korean patients who have undergone PCI exhibit greater engagement in cardiac health behaviors-including medication adherence, dietary regulation, exercise, lifestyle management, stress management, and emergency response-as their socioeconomic status increases [29]. These findings underscore the importance of identifying the coping profiles of individuals with CAD who exhibit lower socioeconomic status and education levels. It is essential to provide these patients with education on health behavior and coping strategies and to encourage the adoption of the Type I coping profile, focusing on their most frequently used coping strategies [27, 28, 29].
In this study, the cardiac health behavior scores for Korean patients with CAD were as follows: 3.09 for participants with the Type I coping profile, 2.86 for those with the Type II coping profile, and 2.71 for those with the Type III coping profile. These values were lower than the average score of 2.87 reported in a previous study of Koreans with this disease, who had an average age of 62.5 years [30]. Notably, participants with the Type II and III coping profiles demonstrated less appropriate cardiac health behavior than Type I patients. The present research indicated that among the five subcategories of cardiac health behavior, smoking cessation was prioritized highest across all coping profile types, consistent with findings from a previous study. Compared to Type II and Type III coping profiles, the Type I coping profile was associated with higher levels of health responsibility, exercise, and stress management within the five subcategories of cardiac health behavior. Patients with the Type I coping profile extensively employed both problem-focused and emotion-focused coping strategies. These approaches seem to increase health awareness in disease-related stress situations, causing the patient to recognize the need for health behaviors such as increased physical activity [11]. In contrast, participants with the Type II and Type III coping profiles were found to be more vulnerable to stress due to their limited use of effective coping strategies, as evidenced by their infrequent employment of such strategies and reliance on avoidant coping strategies, in contrast to the Type I coping profile [10].
In this study, Type I coping profile participants engaged in cardiac health behavior more intensely than those with a Type II coping profile, with an OR of 2.57. Prior research has shown that individuals who use problem-focused and emotion-focused coping strategies are more likely to engage in cardiac health behaviors, such as exercise and a healthy diet [5]. Accordingly, patients with Type II coping profile, who use general coping strategies less frequently, displayed poorer cardiac health behavior. The Type II coping profile was notably associated with substance use, such as smoking. We hypothesized that the higher incidence of smoking cessation attempts among Type II individuals, compared to Type I, was attributable to their higher smoking rates. Prior studies have indicated that reduced use of coping strategies is associated with lower participation in cardiac rehabilitation, which aligns with the present results [11]. Furthermore, the present research indicated that the Type III coping profile was associated with much lower engagement in cardiac health behavior than Type I, as evidenced by the OR for type I exceeding 7. The coping strategies characteristic of the Type III coping profile were generally the opposite of those seen in Type I coping profile. While patients with the Type I coping profile actively employed strategies to manage disease-related stress, those with the Type III coping profile tended to deny and avoid the situation, exemplifying a passive approach to cardiac health behavior [11]. Improving these fragile health behaviors is critical, since proactive health practices, such as regular exercise, healthy diet, and smoking cessation, can reduce the risk of future adverse cardiac events by up to 38% in patients with CAD [6]. The finding that 55.2% of study participants used negative coping strategies for cardiac health behavior underscores the urgent need for healthcare providers to assess and modify coping patterns among patients.
By identifying individual coping patterns in patients with CAD, healthcare providers could improve health behavior interventions. This approach enables the identification of vulnerable subgroups [31]. By recognizing patients with the Type II coping profile, characterized by substantial substance use, and those with the Type III coping profile, who tend to rely on self-blame, avoidance, and behavioral disengagement-particularly after PCI-providers can customize interventions to promote the adoption of Type I coping strategies. This support can help patients with CAD improve their health behaviors. Healthcare providers can support patients' coping skills through interactions that involve clearly communicating health information and fostering positive thinking [32]. Mindfulness and problem-solving interventions have also been recommended as effective methods for improving coping abilities [33, 34]. Mindfulness intervention involves a nonjudgmental awareness of thoughts, emotions, and bodily sensations by focusing intentionally on the present moment [34]. Problem-solving therapy aids individuals in achieving their health goals by defining health problems, considering personal priorities, and identifying resources, anticipated health outcomes, and challenges in implementing health goals [35]. Consequently, incorporating mindfulness and problem-solving therapy into cardiac rehabilitation training following acute treatment can be key to strengthening problem-focused and emotion-focused coping strategies in patients with CAD.
To our knowledge, this study is the first to use LPA to identify groups of individuals with similar score profiles for specific attributes, thereby determining the coping patterns of Korean adults who have undergone PCI following a CAD diagnosis. This study is valuable in its suggestion of a direction for training on coping skills that healthcare providers can offer to patients. Specifically, we identified three distinct coping profiles and explored the association of each profile with cardiac health behavior.
However, due to practical challenges, this research had some limitations. First, the study included a total of 203 participants, with more than 25 individuals in each group; however, one group contained only 26 individuals, which may limit the generalizability of the findings due to the small sample size [35]. Future studies should aim to include a larger sample size and utilize longitudinal data to increase the validity of the results. Second, we excluded two participants from this study because they provided incomplete responses on the Brief-COPE. Although model fit statistics can deteriorate when more than 10% of data are missing, the exclusion of only 1% of participants is unlikely to significantly affect the results [16]. Third, we identified high correlations among the subscales of the Brief-COPE instrument, which was used for the LPA. Morin and Marsh [35] have suggested that such correlations might indicate the presence of a global construct. The subscales of the Brief-COPE are all related to the broader construct of "coping strategies," potentially generating high intercorrelations. Nevertheless, each variable represented a distinct coping strategy. To address these issues, future research could consider estimating factor mixture models that include continuous factors or estimating latent categorical variables from residual covariances [35]. To avoid misclassification of latent classes due to correlations, we used multiple information indices and assessed classification quality to derive a statistically reliable latent profile model [20]. Notably, another study using the same tool identified coping profiles similar to those found in this study [14]. The coping profiles identified here were associated with varying levels of cardiac health behavior, validating the classification of coping profiles and demonstrating their heterogeneity by demonstrating distinct differences in their characteristics and outcomes. As an additional limitation, we were unable to subdivide and analyze the elapsed time after the onset of CAD. Since coping with stress can vary depending on the amount of stress and the duration of exposure to stressors, it is crucial to analyze the coping profile at each stress onset point to determine whether coping profiles and their patterns change over time. Finally, the results should be generalized with caution because the participants were selected from a single university hospital using a non-probability sampling method.
The present study identified three coping profiles among patients with CAD and examined their associations with cardiac health behavior. Patients who employed a range of coping strategies, particularly problem-focused coping methods, exhibited more behaviors conducive to cardiac health compared to patients with other coping profiles. Consequently, healthcare providers should recognize the coping patterns of patients with CAD and guide and encourage them to adopt coping strategies that promote cardiac health behavior. A longitudinal study is warranted to investigate changes in coping profiles over an extended period and to determine the relationships between specific coping trajectories and cardiac health behavior.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conceptualization - LYJ, LYS, JH, and CJC.
data curation - LYS, JH, and CJC.
data analysis - LYS, LYJ, and JS.
writing original draft, review & editing - LYS, LYJ, and JS.
All authors read and approved the final manuscript.
Source of funding: This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MIST) [No. 2018R1C1B6003419].
 E-SUBMISSION
E-SUBMISSION