
Purpose
Cancer survivors face a high risk of developing secondary cancers; thus, they should consider their primary cancer experiences as signals to adopt secondary cancer-preventive behaviors. This study examined the mediating effect of perceived threat in the relationship between cue to action and such behaviors and identified the gender effect as a moderator in breast and colorectal cancer survivors.
Methods: A total of 505 cancer survivors (253 with breast cancer and 252 with colorectal cancer) participated in this study. These participants were involved in cancer-related physical activities at the outpatient oncology clinic of a tertiary teaching hospital in Korea. Participants completed structured, self-administered questionnaires, and a PROCESS macro was utilized to analyze the mediating effect of perceived threat.
Results: Cue to action positively affected perceived threat (B=0.38, p <.001). Additionally, both cue to action (B=0.20, p=.047) and perceived threat (B=1.28, p<.001) positively influenced secondary cancer-preventive behaviors. In the relationship between cue to action and these behaviors, perceived threat explained 30.0% of the variance. Gender was supported as a moderator in the relationship between cue to action and perceived threat. A bootstrap analysis confirmed the mediating effect of perceived threat.
Conclusion: Perceived threat can help cancer survivors understand the risk and seriousness of secondary cancer, thereby strengthening the relationship between cue to action and secondary cancer-preventive behaviors. Healthcare providers should provide accurate information as a cue to cancer survivors, enabling them to recognize the risk of secondary cancer.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
Cancer survivors face a high risk of developing secondary cancers; thus, they should consider their primary cancer experiences as signals to adopt secondary cancer-preventive behaviors. This study examined the mediating effect of perceived threat in the relationship between cue to action and such behaviors and identified the gender effect as a moderator in breast and colorectal cancer survivors.
A total of 505 cancer survivors (253 with breast cancer and 252 with colorectal cancer) participated in this study. These participants were involved in cancer-related physical activities at the outpatient oncology clinic of a tertiary teaching hospital in Korea. Participants completed structured, self-administered questionnaires, and a PROCESS macro was utilized to analyze the mediating effect of perceived threat.
Cue to action positively affected perceived threat (B=0.38, p<.001). Additionally, both cue to action (B=0.20, p=.047) and perceived threat (B=1.28, p<.001) positively influenced secondary cancer-preventive behaviors. In the relationship between cue to action and these behaviors, perceived threat explained 30.0% of the variance. Gender was supported as a moderator in the relationship between cue to action and perceived threat. A bootstrap analysis confirmed the mediating effect of perceived threat.
Perceived threat can help cancer survivors understand the risk and seriousness of secondary cancer, thereby strengthening the relationship between cue to action and secondary cancer-preventive behaviors. Healthcare providers should provide accurate information as a cue to cancer survivors, enabling them to recognize the risk of secondary cancer.
Cancer incidence and mortality are closely associated with lifestyle factors [1]. Breast and colorectal cancers serve as typical examples of this pattern [2, 3]. Recent studies have demonstrated that adopting a healthy lifestyle decreases the risk of cancer occurrence, recurrence, and mortality [1, 4]. Key lifestyle factors that contribute to cancer causation and mortality include smoking, alcohol consumption, obesity, diet, and physical inactivity. These factors are regarded as primary targets for prevention, emphasizing the importance of adhering to cancer-preventive lifestyle behaviors [1, 4]. In fact, studies have shown that making post-diagnosis lifestyle changes, such as increasing physical activity, can reduce the risk of breast and colorectal cancer recurrence and mortality by approximately 20% to 50% [5, 6].
Cancer survivors often acknowledge the importance of adopting healthy lifestyles following diagnosis and treatment. In-depth interviews with breast and colorectal cancer survivors, as well as their families, reveal that cancer survivors are more likely to adhere to healthy lifestyles based on persistent thinking compared to their family members [7]. Furthermore, a family history of cancer has been associated with increased adherence to healthy lifestyles [8]. Repeated exposure or a close relationship with someone who has cancer can serve as a catalyst for taking swift action toward healthier living.
Secondary cancer, which refers to a new cancer that develops after an initial cancer diagnosis, is distinct from recurrence and metastasis. A cohort study conducted from 1992 to 2008 involving 2,116,163 cancer patients in the United States found that 8.1% of cancer survivors developed secondary cancer [9]. Thus, the prevention and early detection of secondary cancer are crucial for cancer survivors. The Health Belief Model (HBM) suggests that individual perceptions of personal susceptibility and the severity of secondary cancer risk can aid in the prevention of secondary cancer.
The HBM is one of the most widely used frameworks in health behavior research [10]. It encompasses six key constructs: perceived susceptibility, perceived severity, benefits to action, barriers to action, self-efficacy, and cues to action. Together, perceived susceptibility and severity form a single construct, termed "perceived threat" [11, 12]. Despite its widespread application, the original HBM had certain limitations, including low predictive capability of its determinants, unspecified variable ordering, and undefined relationships among variables [13]. To better explain health behaviors with larger effect sizes, self-efficacy and cues to action have since been incorporated into the HBM.
Several empirical studies have demonstrated that perceived threat mediates the relationship between cues to action and healthy behaviors. One study investigating healthy behaviors in the context of the HBM revealed that a cue to action, when presented through a perceived threat, had both direct and indirect effects on tuberculosis screening intentions among Korean adults [10]. Perceived threat was also found to mediate the relationship between cues to action and weight management practices in college students [14]. Another HBM-based study reported a direct effect of cues to action and perceived threat on hypertension-preventive behaviors among adolescents [15]. Notably, that study also revealed an indirect effect of cues to action on hypertension-preventive behaviors through perceived threat, with these direct and indirect effects ranking as the first and second most influential factors in promoting healthy behaviors [15]. These findings lend support to the mediating role of perceived threat in the relationship between cues to action and behavioral intentions or healthy behaviors.
Considering breast and colorectal cancers as typical examples of lifestyle-related cancers, a gender difference is evident in the incidence of these two diseases, primarily because breast cancer predominantly occurs in women. This difference may lead to varying perceptions of cancer risk between men and women [16]. In a study examining perceived risk and worry associated with gender-specific breast and prostate cancer, men reported a higher perceived risk of developing cancers, while women reported more frequent cancer-related worry [16]. However, few investigations have been conducted into gender differences in cancer risk perception. Moreover, in studies examining the path from cue to action via perceived threat, the inclusion of Secondary Cancer-Preventive Behaviors (SCPBs) is often insufficient, despite the fact that cancer survivors are at high risk of developing secondary cancer. We conducted the present study to identify the mediating effect of perceived threat on the relationship between cue to action and SCPBs. Additionally, we sought to investigate gender differences as a moderating factor in the mediating effect of perceived threat.
This study was a cross-sectional and correlational design.
A convenience sample of patients undergoing oncology outpatient follow-up treatment in a tertiary teaching hospital was recruited between August 2019 and May 2020. This hospital, located in southwestern Korea, was equipped with 684 beds, 13 cancer clinics, and a hematopoietic stem-cell transplantation center. The inclusion criteria consisted of (1) stage 2 cancer survivors, who were in the extended survival period according to the Mullan cancer survival stages [17] and were receiving outpatient follow-up after acute treatment, including surgery, chemotherapy, and radiotherapy; (2) adult cancer survivors over 18 years old; and (3) cancer survivors with the ability to communicate both verbally and in writing.
Potentially eligible participants included 279 individuals with breast cancer and 273 with colorectal cancer. Among these participants were 505 cancer survivors, consisting of 253 with breast cancer and 252 with colorectal cancer. Based on the maximum likelihood method [18], our study required a sample size of at least 200 participants. Considering a 20% dropout rate, over 240 participants were chosen and completed the study questionnaire independently. Consequently, a total of 505 data were obtained without any missing values.
This study was approved by the institutional review board of G Hospital (IRB No. 1040198-190430-HR-032-02). Participants were given a $10.00 USD token of appreciation for their involvement.
Cue to action was assessed using a modified version of the original scale developed by Cho [19]. This scale comprises five items, encompassing both internal and external cues to action, and is rated on a five-point Likert scale. Higher scores signify a greater influence of the cue to action. In Cho's study, Cronbach's α was .79 [19], while in the current study, it was .70.
The concept of perceived threat is a combination of perceived susceptibility and perceived severity [10, 20]. To assess perceived threat, we adapted the HBM scale for breast cancer and breast self-examination, which was originally developed by Champion [20]. We used the Korean-validated version of the Champion HBM scale [21] and made a slight modification for this study by replacing "breast cancer" with "secondary cancer." This scale consists of 12 items, each rated on a 5-point Likert scale. Higher scores indicate higher levels of perceived threat. In Champion's [20] study, Cronbach's α was .87, while in the present study, it was .92.
To assess secondary cancer-preventive health behaviors, the researchers adapted the scale initially developed by Kim and Kim [22], which was based on the content of Korean cancer-prevention practice guidelines. In this study, items with a content validity index of .8 or higher were accepted after evaluation of the original 21 items by 10 experts, including five oncology nurses, two nursing professors, and three oncology physicians. Six items, such as smoking, cervical cancer vaccination, and sunlight exposure, were removed due to their low relevance to breast and colorectal cancer patients. The resulting scale comprises 15 items rated on a 5-point Likert scale, encompassing food intake (six items), stress management (two items), exercise and healthy weight (two items), alcohol consumption (one item), information seeking (one item), carcinogen exposure (one item), prevention of sexually transmitted diseases (one item), and cancer-screening examinations (one item). Higher scores indicate better cancer-prevention practices and health-promotion behaviors. Cronbach's α was .86 in Kim and Kim's study [22] and .81 in the present study.
Patients were identified in the waiting room of an outpatient clinic, where a trained assistant explained the purpose of the study, the content of the questionnaires, anonymity, and voluntary participation. After participants provided informed consent, they completed paper-and-pencil questionnaires, which took approximately 15 minutes. The assistant provided assistance to patients who required support, such as by reading the questionnaire aloud.
The data were analyzed using the PROCESS macro (version 3.3) developed by Hayes [23]. The independent t-test was employed to examine the differences in SCPBs. Pearson correlation coefficients were utilized to determine the relationships between cue to action, perceived threat, and SCPBs. The SPSS PROCESS macro was used to investigate the moderated mediating effect of perceived threat on the relationship between cue to action and SCPBs by gender (Figure 1). The statistical significance of the mediating effect was confirmed through bootstrap analysis [23].
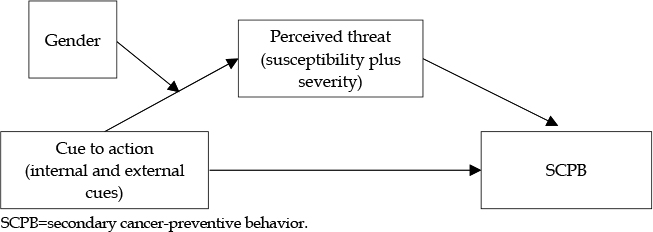
Figure 1
Theoretical framework applied for the adoption of secondary cancer-preventive behavior.
Table 1 displays the differences in general and disease characteristics between patients with breast and colorectal cancer. Significant differences were observed in gender (χ2=203.46, p<.001) and age (t=-9.74, p<.001). However, no significant differences were found in marital status, occupation, perceived economic status, private health insurance, disease duration, and perceived health status (p=.077~.700).
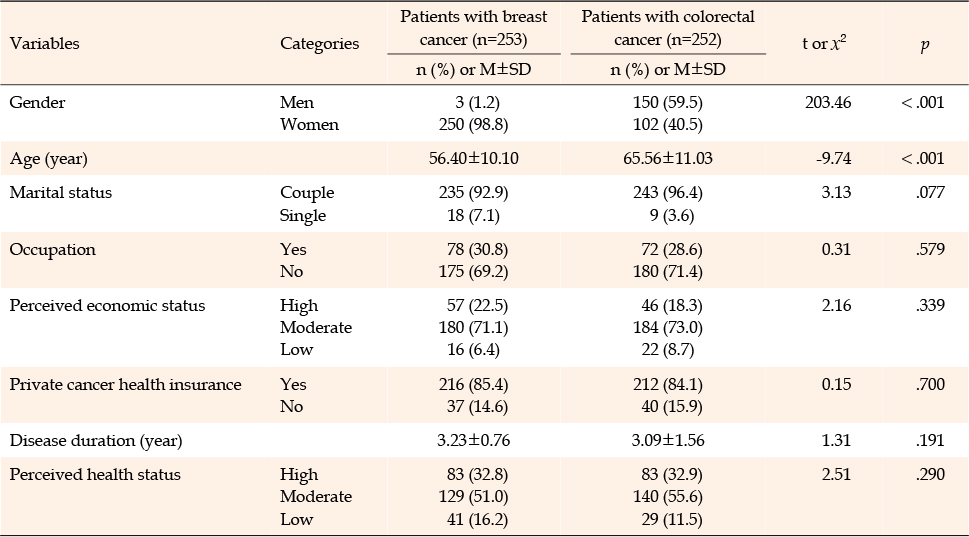
Table 1
General and Disease-related Characteristics of Patients with Breast and Colorectal Cancer (N=505)
Table 2 presents the differences in SCPBs based on the general and disease-related characteristics of the participants. A significant difference was observed in SCPBs concerning gender (t=-3.85, p<.001); however, no significant differences were observed in relation to cancer type, marital status, occupation, perceived economic status, private health insurance, disease duration, and perceived health status (p=.070~.931).
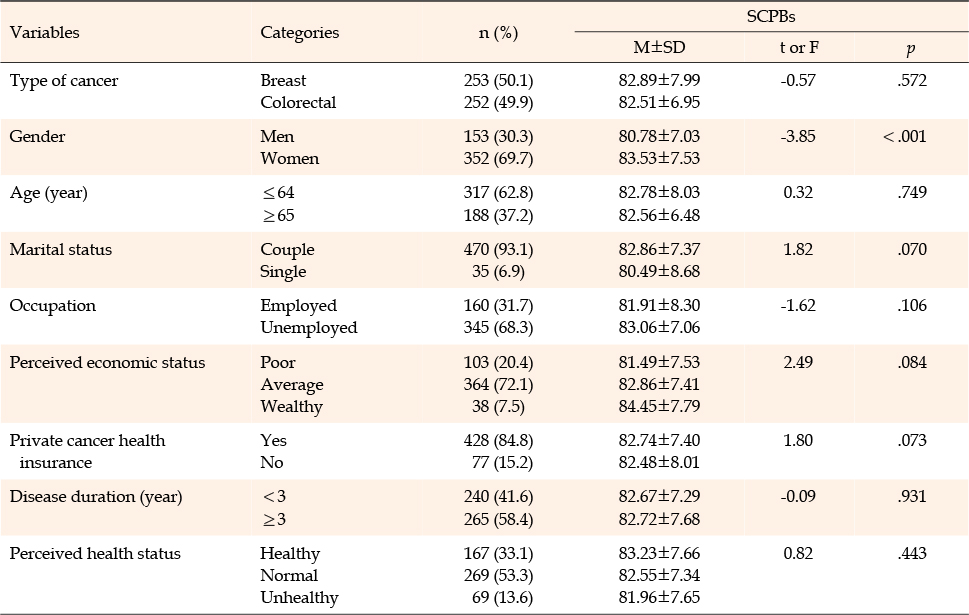
Table 2
SCPBs by General and Disease-related Characteristics (N=505)
The mean cue to action score was 15.42±3.20 of a potential 25 points, the mean perceived threat score was 27.67±3.38 out of 35 points, and the mean SCPB score was 82.70±7.49 out of 105 points.
Table 3 displays the correlations between the variables. Cue to action demonstrated a positive relationship with both perceived threat (r=.36, p<.001) and SCPBs (r=.13, p<.005). Additionally, perceived threat was positively associated with SCPBs (r=.55, p<.001).
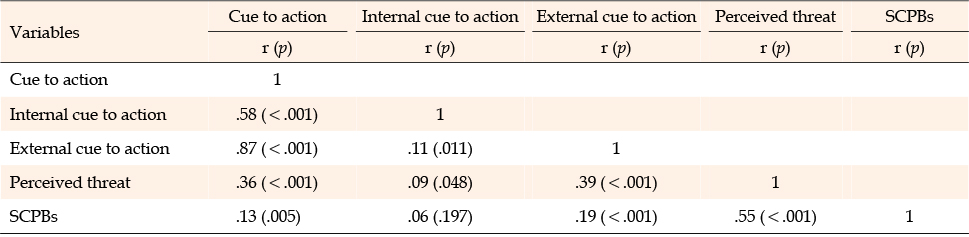
Table 3
Correlations of SCPBs with Cue to Action and Perceived Threat (N=505)
Table 4 shows the mediating effects of perceived threat in the association between cue to action and SCPBs. In the initial step, cue to action demonstrated a significant positive impact on perceived threat (B=0.38, p<.001). In the subsequent step, when both cue to action and perceived threat were considered as predictors and SCPBs as the dependent variable, cue to action (B=1.15, p=.047) and perceived threat (B=1.28, p<.001) exhibited significant positive effects on SCPBs. Perceived threat (R2=.30) accounted for 30% of the variance in the connection between cues to action and SCPBs. The bootstrap analysis verified the significant mediating influence of perceived threat (95% CI=0.37~0.62). In essence, perceived threat partially mediated the link between cue to action and SCPBs.
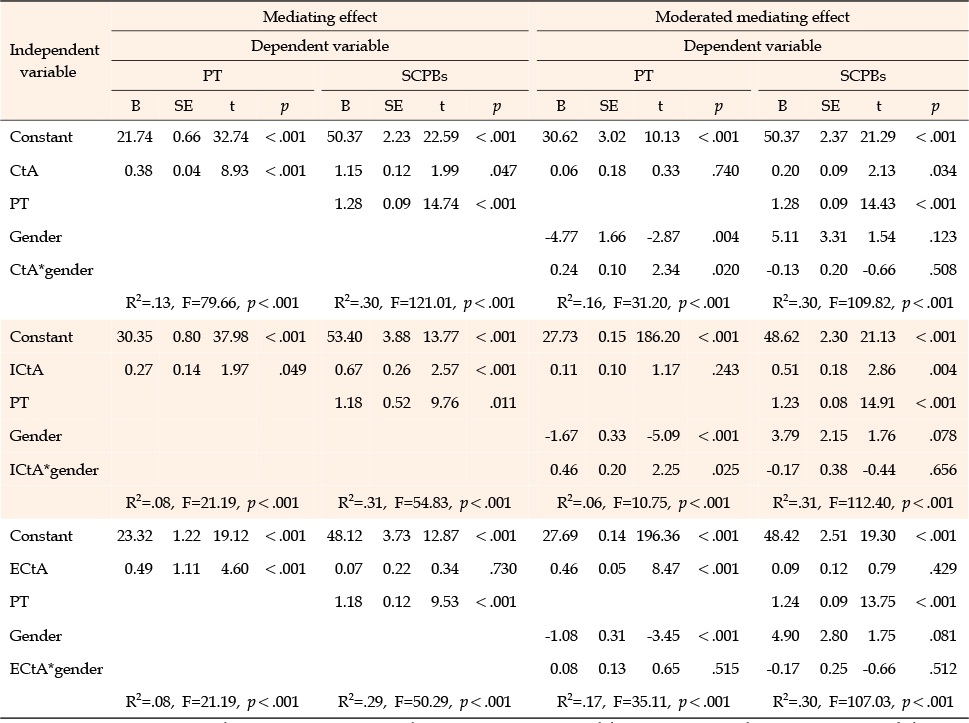
Table 4
Mediating Effects of Perceived Threat by Gender in the Relationship between Cue to Action and SCPBs (N=505)
An additional analysis revealed that perceived threat partially mediated the relationship between internal cues to action and SCPBs. In contrast, perceived threat fully mediated the relationship between external cues to action and SCPBs.
Table 4 demonstrates the moderated mediating effects of perceived threat on the relationship between cue to action and SCPBs, as influenced by gender. In the first step, a significant positive effect of cue to action on perceived threat was observed when considering gender (B=0.24, p=.020). In the second step, using cue to action and perceived threat as predictors and SCPBs as the dependent variable, both cue to action (B=0.20, p=.034) and perceived threat (B=1.28, p<.001) exhibited significant positive effects on SCPBs. Perceived threat (R2=.30) accounted for 30% of the variance in the relationship between cue to action and SCPBs. The bootstrap analysis verified the significant mediating effect of perceived threat (95% CI=0.35~0.60). In summary, the relationship between cue to action and SCPBs was mediated by perceived threat, which was moderated by gender.
An additional analysis revealed that the relationship between internal cues to action and SCPBs was mediated by perceived threat, which was moderated by gender. However, perceived threat moderated by gender did not have a mediating effect on the relationship between external cues to action and SCPBs.
In this study, we examined the relationships between cue to action, perceived threat, and SCPBs while exploring the mediating effect of perceived threat on the association between cue to action and SCPBs, with gender as a moderating factor. Previous HBM-based research has primarily been focused on perceived susceptibility, severity, benefits, and barriers, resulting in limited attention devoted to cue to action [14]. Our findings demonstrate that cue to action can contribute to the promotion of preventive behaviors and that the perceived threat, moderated by gender, can mediate the relationship between cue to action and SCPBs. This expands the capacity of the HBM to explain health behavior promotion.
The significant relationship between cue to action and perceived threat aligns with a previous study revealing that interpersonal cues to action influenced perceived threat in tuberculosis screening intention [10]. A cue to action is the stimulus required to initiate the decision-making process for acceptance of a recommended health action. Cues to action can be categorized into internal and external cues, with external cues further subdivided into interpersonal and media cues. In an HBM-based study examining Coronavirus Disease 2019 (COVID-19) preventive behaviors, the HBM accounted for 27% of the variance, and both internal and external cues to action were associated with COVID-19 preventive behaviors [24]. Additional analysis in this study identified cues impacting perceived threat and SCPBs, revealing that only internal cues to action directly affected both perceived threat and SCPBs. The HBM also accounts for 18.5% of the variability in moderate to vigorous physical activity among cancer survivors with relatives who have had cancer, as well as 8.3% of the variability in moderate to vigorous physical activity among survivors with relatives who have not had cancer. These earlier findings suggest that primary cancer experiences, such as the shock of a cancer diagnosis and the suffering caused by cancer treatment, may serve as internal cues. These experiences can also strengthen internal cues compared to external cues from the media or close friends and family. Therefore, cues to action, particularly internal ones, should be reinforced among individuals whose previous experiences enable them to perceive the threat. Oncology nurses should actively alleviate treatment-related symptoms in cancer patients undergoing aggressive treatments, such as nausea and vomiting, to enhance positive internal cues and facilitate appropriate perception of the threat of developing secondary cancer [25]. As previously mentioned, no prior studies are available on the relationship between cue to action and perceived threat, as cue to action has been treated as an additional variable in the HBM [26]. Further research is needed to explore the relationship between cue to action and perceived threat within the HBM and the impact of cue to action among individuals with previous cancer experiences, including survivorship.
Our findings demonstrated that gender moderated the effect of cue to action on perceived threat, meaning that perceived threat had a moderated mediation effect in the relationship between cue to action and SCPBs. In a previous study, when exposed to sentences that threatened gender identity, women with a stronger gender identification recalled fewer neutral words than men [27]. Men and women define "security" in slightly different ways, and women tend to identify more security threats than men [28]. These findings suggest that gender can moderate threat, and this moderated threat influences outcomes. However, in the present study, no moderated mediation effect of perceived threat was observed in the relationship between external cue to action and SCPBs by gender. Therefore, internal cue to action should account for gender differences, while external cue to action from media and interpersonal relationships can be applied to patients with breast or colorectal cancer regardless of gender.
Our findings demonstrate a positive relationship between cue to action and SCPBs, consistent with previous research. In healthy Korean individuals, cue to action was an important predictor of protective behavioral intention against Middle East Respiratory Syndrome [29]. Likewise, a recent study in the Philippines found a positive association between cue to action and COVID-19 preventive behaviors [30]. Additionally, our results indicate that perceived threat is correlated with SCPBs, and as a health belief, threat has influenced adherence in various patient populations [31]. A study involving Iranian college students discovered that perceived threat fully mediated the relationship between cue to action and weight-management behaviors, even though an earlier study did not support the direct effect of cue to action on such behaviors [14]. This finding implies that cancer survivors who have undergone aggressive treatment or witnessed secondary cancer in their peers may perceive a higher risk of developing secondary cancer, leading to increases in SCPBs to prevent its development. This observation underscores the critical role of perceived threat in shaping the behavior of cancer survivors. The mediation analysis in our study reveals that perceived threat mediates the relationship between cue to action and SCPBs among breast and colorectal cancer survivors. This mediating outcome suggests that cue to action exerts both direct and indirect influences on SCPBs.
In the HBM, the combination of perceived susceptibility and perceived severity is referred to as perceived threat [32]. Our findings indicate that perceived threat mediates the relationship between cue to action and SCPBs, suggesting that cue to action influences SCPBs both directly and indirectly by increasing perceived threat. This gives breast and colorectal cancer survivors a heightened awareness of their susceptibility to the severe risk of developing secondary cancer. This result is consistent with previous findings that perceived threat mediates the relationship between cue to action and hypertension-preventive behaviors among adolescents in Surakarta [15]. Similarly, a recent study revealed that the perceived threat of COVID-19, communicated through timely and accurate information, enabled Italians to take appropriate self-protective actions [33]. Therefore, recognizing and understanding threats through cues related to the risk of developing secondary cancer may have a significant impact, as engaging with the risk of developing secondary cancer enhances SCPBs.
While this study makes a meaningful contribution to SCPB research, it had some limitations. Firstly, it identifies the relationships between the three variables (cue to action, perceived threat, and SCPBs) based on the HBM; however, the causal connections between these can only be confirmed using the present cross-sectional data. Future longitudinal studies may reveal more accurate trajectories between these variables. Secondly, although this study employed slightly modified versions of the original instruments, the evaluation of their validity was not comprehensive. Lastly, the generalizability of these findings to male survivors is limited, as the current sample predominantly consisted of female survivors of breast cancer. Therefore, future studies should incorporate more diverse samples to expand the understanding of the findings presented in this study.
This study investigated the relationships between cue to action, perceived threat, and SCPBs, as well as the moderated mediating effect of perceived threat on SCBP by gender. In doing so, it contributes to the prevention of secondary cancers in at-risk populations based on the HBM. We found a positive correlation between cue to action and perceived threat with SCBP. This finding implies that oncology nurses should incorporate the concepts of cue to action and perceived threat, while taking into account gender differences as a mediator when planning and implementing interventions aimed at enhancing SCPBs among cancer survivors. The evidence that perceived threat mediates the relationship between cue to action and SCPBs supports the use of perceived threat to explain this association. Consequently, these findings may serve as a foundation for developing intervention programs to improve SCPBs among cancer survivors.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - BSY and CJY.
Data collection - BSY.
Analysis or interpretation of the data - CJY.
Drafting or critical revision of the manuscript for important intellectual content - BSY and CJY.
This article is a revision of the first author's doctoral thesis from Chonnam National University.
 E-SUBMISSION
E-SUBMISSION