
Purpose
Cancer diagnosis is associated with psychological distress, which often leads to a significant reduction in adaptation and quality of life. This study aimed to identify the prevalence and related factors of psychological distress in newly diagnosed breast cancer patients.
Methods
The study included 138 women scheduled for surgery or neoadjuvant chemotherapy following a recent breast cancer diagnosis at a university hospital in Korea.
Psychological distress was assessed using the National Comprehensive Cancer Network Distress Thermometer and problem lists. Data collection occurred from November 1, 2021, to November 30, 2022. Descriptive statistics and logistic regression analysis were utilized for data analysis.
Results
The average age of the participants was 51.72 years. Among the 138 participants, 67.4% (n=93) reported moderate to severe levels of psychological distress. Multivariate logistic regression analysis identified financial burden (Odds Ratio [OR]=4.32), fears (OR=5.35), and nervousness (OR=5.50) as predictors of moderate to severe psychological distress.
Conclusion
Approximately two-thirds of newly diagnosed breast cancer patients experienced significant psychological distress.
Nervousness, fears, and financial burden were significant factors influencing this distress. Therefore, management of psychological distress should be implemented for patients experiencing financial burdens or emotional problems, such as nervousness and fear, from the time of diagnosis.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
Cancer diagnosis is associated with psychological distress, which often leads to a significant reduction in adaptation and quality of life. This study aimed to identify the prevalence and related factors of psychological distress in newly diagnosed breast cancer patients.
The study included 138 women scheduled for surgery or neoadjuvant chemotherapy following a recent breast cancer diagnosis at a university hospital in Korea. Psychological distress was assessed using the National Comprehensive Cancer Network Distress Thermometer and problem lists. Data collection occurred from November 1, 2021, to November 30, 2022. Descriptive statistics and logistic regression analysis were utilized for data analysis.
The average age of the participants was 51.72 years. Among the 138 participants, 67.4% (n=93) reported moderate to severe levels of psychological distress. Multivariate logistic regression analysis identified financial burden (Odds Ratio [OR]=4.32), fears (OR=5.35), and nervousness (OR=5.50) as predictors of moderate to severe psychological distress.
Approximately two-thirds of newly diagnosed breast cancer patients experienced significant psychological distress. Nervousness, fears, and financial burden were significant factors influencing this distress. Therefore, management of psychological distress should be implemented for patients experiencing financial burdens or emotional problems, such as nervousness and fear, from the time of diagnosis.
Breast cancer is the most common cancer among women worldwide [1]. In Korea, it is the second most prevalent cancer among women. The 5-year and 10-year relative survival rates are notably high, at 93.8% and 89.4% respectively, attributed to early diagnosis and advanced treatment options [1, 2]. With the rise in survival rates, patients are living longer as survivors, highlighting the need to focus on the health challenges they face [3, 4].
Cancer diagnosis induces significant psychological distress in patients [5]. Immediately following diagnosis, breast cancer patients often experience psychological problems such as anxiety, depression, worry, fear, and sadness. They may also experience physical symptoms like sleep disorders and fatigue, in addition to financial challenges [5, 6, 7]. In the initial stages post-diagnosis, breast cancer patients deal with psychological distress as they grapple with their diagnosis and confront an uncertain future with the disease [8]. Psychological distress is defined as an unpleasant emotional state that disrupts their ability to effectively respond to treatment across physical, psychological, social, and spiritual dimensions [9]. It includes a spectrum of negative emotions such as worry, anxiety, embarrassment, sadness, anger, guilt, and depression [5, 10].
The time of cancer diagnosis marks a critical juncture where patients must come to terms with their new reality and actively participate in their treatment plan [11]. Elevated levels of psychological distress can compromise decision-making abilities regarding treatment options and lead to increased unmet needs, complicating the adjustment to life as a cancer patient [12]. Specifically, high psychological distress at the time of breast cancer diagnosis adversely impacts the patients' quality of life by diminishing their satisfaction with cancer treatment and reducing their capacity to manage the sequelae or adverse effects of the treatment [13, 14, 15]. Consequently, a comprehensive examination of the factors that contribute to psychological distress in newly diagnosed breast cancer patients is essential. Identifying those at high risk and implementing interventions to reduce psychological distress are critical steps in improving patient outcomes [16].
Internationally, research efforts have consistently focused on determining the extent of psychological distress and related factors in newly diagnosed breast cancer patients, as well as developing and validating educational programs that address common psychological and social symptoms or difficulties [5, 17, 18, 19, 20, 21]. In South Korea, studies have been conducted to identify factors associated with psychological distress [22] and to validate distress management programs [3] for breast cancer patients who are currently undergoing treatment or have completed primary treatment. However, there have been few studies that specifically explore distress-related factors in newly diagnosed breast cancer patients [23]. Therefore, the purpose of this study is to explore the prevalence of psychological distress and related factors in patients with breast cancer at the time of diagnosis.
This cross-sectional study was conducted to determine the prevalence of psychological distress and its associated factors in patients newly diagnosed with breast cancer.
Participants were selected through convenience sampling from a pool of patients scheduled for surgery or neoadjuvant chemotherapy following a new breast cancer diagnosis at Ajou University Hospital between November 1, 2021, and November 30, 2022. The inclusion criteria mandated that participants understand the study's purpose and provide voluntary informed consent. The study targeted women aged 19 years or older, diagnosed with stage 1, 2, or 3 breast cancer, who had no previous history of cancer. The exclusion criteria encompassed health conditions likely to cause psychological distress, such as psychiatric illnesses or cognitive impairment.
We used G*Power 3.1.9.4 to calculate the required sample size for logistic regression analysis, assuming a significance level of α=.05, power=.80, and an Odds Ratio (OR) of 2.0 [22]. The minimum sample size required was 113 patients. To account for potential dropouts, we set the target sample size at 141 patients. After excluding three patients due to incomplete responses, data from the remaining 138 patients were included in the final analysis.
A structured questionnaire was used to measure participants’ sociodemographic characteristics (e.g., age, educational level, presence of spouse, occupation, and financial burden) and clinical characteristics (e.g., stage of cancer and presence of other diseases).
To assess the prevalence of psychological distress and its related factors, we employed the Distress Thermometer (DT) and Problem List (PL) version 3, developed by the National Comprehensive Cancer Network (NCCN) Management Panel in 2019. These tools are widely recognized for their effectiveness in initial psychological distress screening [9]. The DT uses an 11-point visual analogue scale, similar to a thermometer, to measure the level of psychological distress experienced by participants over the past week. The scale ranges from 0 points, indicating "no distress," to 10 points, indicating "extreme distress." Higher scores on this scale signify greater psychological distress. According to NCCN guidelines, a distress cut-off score of 4 points is recommended. Scores below 4 points are classified as mild psychological distress, while scores of 4 points or higher are classified as moderate to severe distress [9].
The NCCN also recommends using the PL to identify sources of psychological distress. The PL is composed of 39 items, distributed across five domains: practical problems (6 items), family problems (4 items), emotional problems (6 items), spiritual/religious problems (1 item), and physical problems (22 items). Participants indicate whether they have experienced each problem in the past week by marking each item with "yes" or "no."
Before initiating the study, we received approval from the Institutional Review Board at Ajou University Hospital (IRB No. AJOUIRB-SUR-2021-541). We obtained written informed consent from all participants, who were fully informed about the study's purpose, background, and participation procedures. An investigator thoroughly explained the methods of storing, managing, disposing of, and maintaining the confidentiality of personal information, ensuring participants were aware of their rights regarding data privacy. Participants were also informed that their involvement was entirely voluntary and that they could withdraw their consent at any time without facing any negative consequences.
Prior to commencing the study, we explained its objectives to the relevant department and secured their permission and cooperation. During the data collection phase, we enrolled patients from the study hospital who met the eligibility criteria and voluntarily provided written consent to participate. An investigator met with the participants in a private area of the breast cancer center, where they were given the study questionnaires along with an explanation sheet. The investigator thoroughly explained the study's objectives and background, outlined the participation process, provided an estimate of the time required to complete the questionnaires, and discussed the expected benefits and incentives. Additionally, the investigator emphasized the voluntary nature of participation, including the right to withdraw at any time. The methods for storing, managing, and disposing of the collected data were also explained. Participants were reassured that the authors had no conflicts of interest concerning the study's conduct and were provided with a contact number for any inquiries. Participants who gave their written consent then proceeded to fill out the structured self-report questionnaire, which took approximately 10 minutes to complete.
The data collected in this study were analyzed using IBM SPSS 25.0. The analysis methods are described as follows. Initially, we employed descriptive statistics to examine participants' sociodemographic and disease-related characteristics, the extent of psychological distress, problem lists, and the incidence within different psychological distress groups. Subsequently, we utilized the χ2 test, independent t-test, and Fisher exact test to analyze differences between psychological distress groups based on sociodemographic and disease-related characteristics. We then assessed differences between psychological distress groups according to participants' problem lists using the χ2 test, independent t-test, and Fisher exact test. Finally, we conducted binomial logistic regression analysis to identify factors influencing the psychological distress group.
Table 1 presents the sociodemographic and clinical characteristics of the participants. The average age was 51.72±9.41 years, with 70 participants (50.7%) having attained a high school education or less. A majority, 103 individuals (74.6%), reported having a spouse, and 109 (79.0%) were currently employed. Financially, 53 participants (38.4%) described their situation as 'burdensome' At diagnosis, the most prevalent cancer stage was stage 1, affecting 73 individuals (52.9%), followed by stage 2 with 54 individuals (39.1%), and stage 3 with 11 individuals (8.0%). Additionally, 87 participants (63.0%) indicated an absence of comorbidities (Table 1).
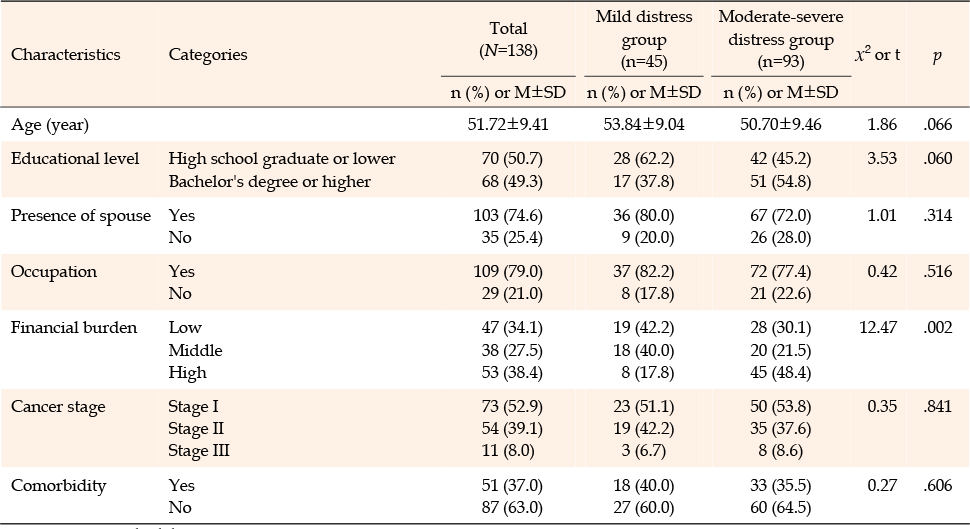
Table 1
Differences in Sociodemographic and Clinical Characteristics between the Two Groups (N=138)
The mean psychological distress score among the participants was 5.22±2.68. Those with a score below the DT cut-off score (<4 points) were categorized into the mild distress group, consisting of 45 individuals (32.6%). Conversely, participants scoring at or above the cut-off score (≥4 points) were placed in the moderate-severe distress group, which included 93 individuals (67.4%) (Table 2).
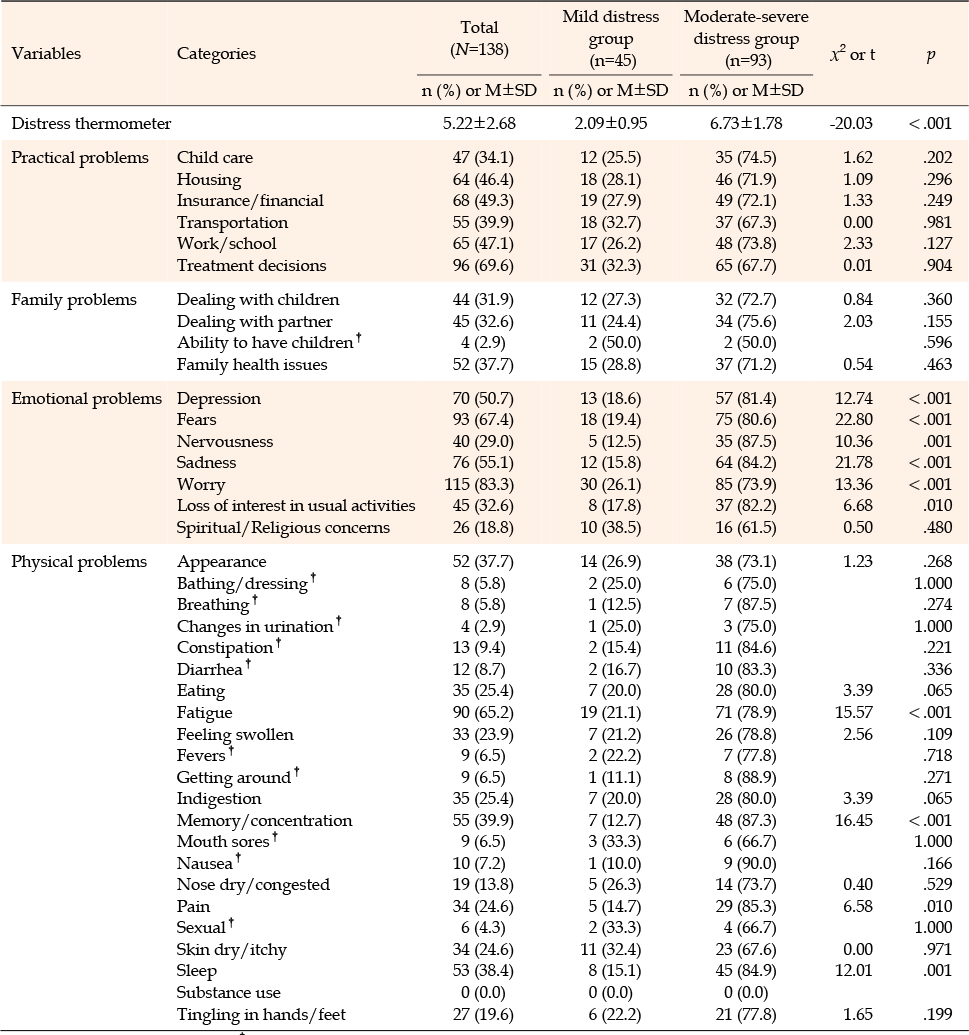
Table 2
Differences in Psychological Distress and Problem Lists between the Two Groups (N=138)
We analyzed participant-reported issues across five domains of the PL. In the practical problems domain, the most commonly reported issue was treatment decisions (96 cases, 69.6%), followed by insurance/financial problems (68 cases, 49.3%), and work/school issues (65 cases, 47.1%). In the family problems domain, the issues frequently reported were family health problems (52 cases, 37.7%), dealing with a partner (45 cases, 32.6%), and dealing with children (44 cases, 31.9%). In the emotional problems domain, the most common issues were worry (115 cases, 83.3%), fear (93 cases, 67.4%), sadness (76 cases, 55.1%), and depression (70 cases, 50.7%). Additionally, 26 individuals (18.8%) reported experiencing spiritual/religious problems. Among physical problems, fatigue was the most common issue (90 cases, 65.2%), followed by memory/concentration problems (55 cases, 39.9%), sleep problems (53 cases, 38.4%), and concerns about appearance (52 cases, 37.7%) (Table 2).
We analyzed differences in psychological distress according to participants' sociodemographic and clinical characteristics (Table 1). A higher percentage of participants in the moderate-severe distress group (48.4%) described their financial situation as 'burdensome' compared to those in the mild distress group (17.8%) (χ2=12.47, p=.002).
When examining differences in psychological distress among participants according to their PLs (Table 2), the moderate-severe distress group had higher ratios of patients reporting depression (χ2=12.74, p<.001), fear (χ2=22.80, p<.001), nervousness (χ2=10.36, p=.001), sadness (χ2=21.78, p<.001), worry (χ2=13.36, p<.001), and loss of interest in usual activities (χ2=6.68, p=.010) among emotional problems, and fatigue (χ2=15.57, p<.001), memory/concentration problems (χ2=16.45, p<.001), and sleep problems (χ2=12.01, p=.001) among physical problems than the mild distress group.
We conducted logistic regression analysis to explore the factors influencing participants' psychological distress, with the results detailed in Table 3. Initially, we confirmed that the model was well-fitted, as shown by a p-value of .923 in the Hosmer-Lemeshow test for goodness of fit for logistic regression models. Subsequently, we carried out binomial logistic regression analysis including financial burden and the PL items that demonstrated statistically significant differences at a .05 significance level in the univariate analysis (Table 3). The analysis identified financial burden, fears, and nervousness as significant factors contributing to psychological distress. Participants experiencing financial burden were 4.32 times more likely to fall into the moderate-severe distress category (OR=4.32, 95% CI=1.25, 14.97; p=.021) than those without such issues. Similarly, participants who reported issues with fears (OR=5.35, 95% CI=1.68, 17.0; p=.004) or nervousness (OR=5.50, 95% CI=1.48, 20.39; p=.011) were 5.35 and 5.5 times more likely, respectively, to be classified within the moderate-severe distress group.
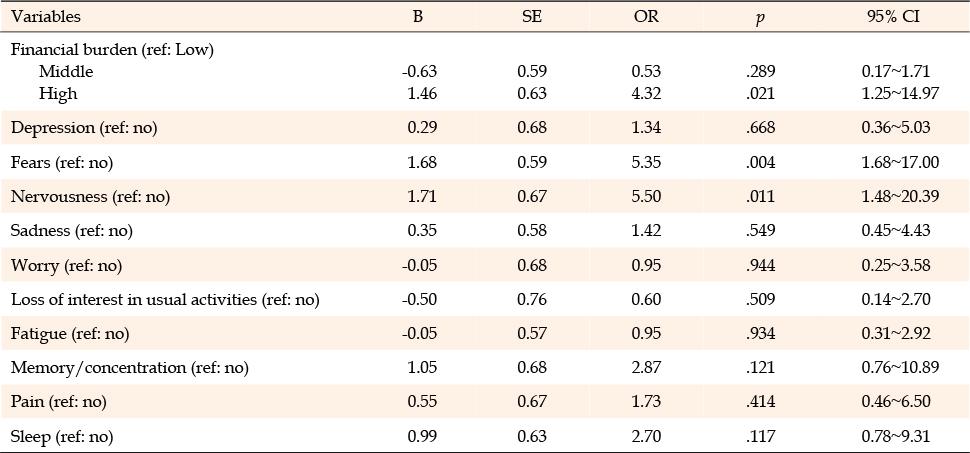
Table 3
Factors Influencing the Psychological Distress of Study Participants (N=138)
This cross-sectional study examined the prevalence of psychological distress and its associated factors in patients with breast cancer at the time of diagnosis. The average psychological distress score among participants was 5.22 points. According to the NCCN guidelines, which set a cut-off value at 4 points [9], 32.6% of participants fell into the mild distress category, while 67.4% were classified as experiencing moderate to severe distress. These findings align closely with those of Ciambella et al. [7], who reported that 66.5% of newly diagnosed breast cancer patients experienced moderate to severe stress using the same scale. However, this study's results show a higher prevalence of moderate to severe distress compared to the study of Zhao et al. [24], which found that 42.3% of patients undergoing treatment for breast cancer fell into this category, and that of Pang et al. [25], which reported that 50.8% of breast cancer survivors experienced moderate to severe distress.
Patients diagnosed with breast cancer often experience significant psychological distress due to life changes brought on by the diagnosis, anxiety about the treatment process, uncertainty about the future, and concerns regarding treatment side effects [5]. Those who suffer from severe psychological distress at the time of diagnosis tend to experience persistently high levels of distress even after survival [16]. Furthermore, psychological distress can adversely affect medical outcomes, including recovery from surgery and the experience of treatment side effects. This underscores the importance of developing practical approaches and strategies to identify psychological distress and manage high-risk patients from the outset [7, 14]. Therefore, it is essential to periodically assess the level of psychological distress from the time of cancer diagnosis and provide psychosocial support to mitigate it.
When we conducted logistic regression to identify factors influencing psychological distress in newly diagnosed breast cancer patients, we found that nervousness, fears, and financial burden were significant contributors. These factors differ from those affecting psychological distress in patients who have completed breast cancer treatment, which include age, fatigue, worry, anxiety, depression, and fear of cancer recurrence [22, 26, 27]. Following a breast cancer diagnosis, psychological distress is shaped by emotional factors such as nervousness and fear, along with financial concerns associated with accepting the diagnosis and preparing for treatment. In contrast, during or after treatment, psychological distress stems from the physical side effects of treatment, fear of cancer recurrence, and worries about resuming normal life [26, 27]. Therefore, psychological support and interventions need to be tailored to the specific needs of patients at each stage.
In this study, nervousness was identified as the strongest factor influencing psychological distress. Patients who responded "yes" to experiencing nervousness were 5.50 times more likely to be categorized within the moderate-severe distress group compared to those who answered "no." This finding aligns with research by Liu et al. [28], which also recognized nervousness as a significant factor affecting psychological distress among newly diagnosed breast cancer patients. Similarly, Ludwigson et al. [5], Mertz et al. [29], and Park et al. [16] reported that nervousness, along with worry, was the most prevalent emotional issue among patients at the time of their breast cancer diagnosis. The diagnosis of cancer is, in itself, an immensely stressful event for patients [12]. Upon diagnosis, patients are faced with the need to accept their condition and formulate treatment plans [28]. Nervousness can adversely impact a patient’s ability to manage their health or engage actively in their treatment. Therefore, it is crucial to assess and address nervousness in this group from the outset, possibly through psychological interventions designed to help patients adjust and cope, thereby mitigating negative emotional responses during treatment. Despite its significance, few studies have specifically examined nervousness in newly diagnosed breast cancer patients [28], highlighting a gap that warrants further investigation.
Next, participants who reported fears were 5.35 times more likely to fall into the moderate-severe psychological distress category compared to those who did not report such issues. Fears, along with worry and anxiety, were identified as the most significant contributors to psychological distress in a study by Ciambella et al. [7], which focused on newly diagnosed breast cancer patients. The diagnosis of cancer and subsequent treatment introduce significant changes in patients' lives [30]. Individuals newly diagnosed with cancer often harbor vague fears concerning their future treatment [31]. Fear, a distressing emotion, naturally arises following a cancer diagnosis [32]. It continues to affect psychological distress not only during treatment but also after the completion of primary treatment for breast cancer [26, 27], and it impacts patients’ adaptation to and compliance with treatment [32]. Therefore, it is crucial to assess the level of fear, information needs, and other related factors at the time of initial diagnosis and to develop management strategies that effectively support patients throughout their treatment.
Finally, participants who reported a financial burden were 4.32 times more likely to be categorized in the moderate-severe psychological distress group compared to those who reported no burden. These findings are consistent with research by Okeke et al. [17] and Liu et al. [28], which observed that breast cancer patients at diagnosis who were uninsured, unemployed, or facing financial issues experienced increased psychological distress. Patients who encounter financial difficulties prior to diagnosis or who feel burdened by the costs of treatment often suffer adverse outcomes, such as decreased compliance with treatment and delays or avoidance of necessary care [33, 34]. This financial burden continues to affect survivors, diminishing their quality of life even after treatment has ended [35]. Consequently, there is a pressing need to establish referral pathways that provide financial support to cancer patients facing economic hardships [34].
The significance of this study lies in its exploration of psychological distress and associated factors among newly diagnosed breast cancer patients, providing essential data for the development of distress management programs. However, the use of a convenience sample from a single university hospital limits the generalizability of the findings. Future research should investigate the factors related to psychological distress in newly diagnosed breast cancer patients across various regions. The NCCN psychological distress measurement scale, employed in this study, is globally recognized for its simplicity and rapid screening capabilities. However, the PL used for assessing distress factors relies on one-word answers, which constrains the precise identification of the actual problems experienced by patients [17, 22]. Subsequent research should utilize instruments that measure psychological distress with a focus on specific details, examining the relationships between psychological distress and factors such as nervousness, fears, and financial burden.
In this study, we aimed to investigate the prevalence and influencing factors of psychological distress in newly diagnosed breast cancer patients. We discovered that 67.4% of these patients experienced moderate to severe distress, primarily due to nervousness, fears, and financial burdens. Effective management of psychological distress in patients newly diagnosed with breast cancer necessitates the identification and evaluation of distress levels from the time of diagnosis. It is essential to develop psychological distress management programs that address both emotional aspects, such as nervousness and fears, and personal factors, including economic status.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Conceptualization - PJH, JYS, HMH, and JYJ.
Data curation - PJH, JYS, HMH, and JYJ.
Formal analysis - PJH and JYJ.
Investigation - PJH and JYJ.
Methodology - PJH.
Resources - PJH, JYS and HMH.
Supervision - PJH.
Validation - PJH.
Writing - original draft - PJH, JYS, HMH, and JYJ.
Writing - review & editing - PJH, JYS, HMH, and JYJ.
We wish to thank the participating patients and the staff at the Department of Breast Cancer Surgery at Ajou University Hospital. This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2021R1A2C1008444). This award was received by PJH. The authors have no relevant financial or non-financial interests to disclose. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
 E-SUBMISSION
E-SUBMISSION