
Purpose
The purpose of this study was to investigate the level of resilience in multiple myeloma patients and to identify the impact of symptom experience, cancer coping, and social support on resilience.
Methods: Data were collected from January 2022 to May 2022 using self-report structured questionnaires administered to 162 outpatients who were undergoing chemotherapy or follow-up care after multiple myeloma treatment. The measured variables included symptom experience, cancer coping, social support, and resilience. The collected data were analyzed using SPSS/WIN 25 for descriptive statistics, the independent t-test, one-way analysis of variance, the Scheffé test, Pearson correlation coefficients, and hierarchical regression analysis.
Results: The mean resilience score of the participants was 66 out of 100 points. The levels of resilience were significantly higher in patients who had a job, recognized the importance of religion, and had a good economic status. Significantly higher levels of resilience were also observed in patients with lower physical performance status, fewer symptom experiences, more positive cancer coping, and higher support from healthcare staff.
Conclusion: Monitoring the symptom experience and physical performance ability of patients with multiple myeloma is important for enhancing their resilience. Positive coping strategies need to be developed and additional support from nurses should be provided to strengthen the personal resilience of patients with multiple myeloma.
The purpose of this study was to investigate the level of resilience in multiple myeloma patients and to identify the impact of symptom experience, cancer coping, and social support on resilience.
Data were collected from January 2022 to May 2022 using self-report structured questionnaires administered to 162 outpatients who were undergoing chemotherapy or follow-up care after multiple myeloma treatment. The measured variables included symptom experience, cancer coping, social support, and resilience. The collected data were analyzed using SPSS/WIN 25 for descriptive statistics, the independent t-test, one-way analysis of variance, the Scheffé test, Pearson correlation coefficients, and hierarchical regression analysis.
The mean resilience score of the participants was 66 out of 100 points. The levels of resilience were significantly higher in patients who had a job, recognized the importance of religion, and had a good economic status. Significantly higher levels of resilience were also observed in patients with lower physical performance status, fewer symptom experiences, more positive cancer coping, and higher support from healthcare staff.
Monitoring the symptom experience and physical performance ability of patients with multiple myeloma is important for enhancing their resilience. Positive coping strategies need to be developed and additional support from nurses should be provided to strengthen the personal resilience of patients with multiple myeloma.
Multiple myeloma, the second most prevalent blood cancer in Korea, is characterized by the malignant transformation of plasma cells, which produce abnormal antibodies that can affect various parts of the body [1]. Over the past decade, the incidence of multiple myeloma has more than doubled. Despite this increase, advancements in treatment have led to a reduction in early mortality rates. Notably, the overall survival rate for patients over the age of 65 has improved from 31% to 56% [2], which has been accompanied by a shift toward perceiving the disease as a chronic condition requiring long-term management. Patients with multiple myeloma typically receive chemotherapy once or twice a week and may experience a range of side effects during their treatment. These side effects can include an increased risk of infection, anemia, and bleeding due to bone marrow suppression caused by chemotherapy, as well as nausea, vomiting, diarrhea, loss of appetite, and peripheral neuropathy [3]. Inadequate management of these symptoms can lead to heightened stress and anxiety among patients, which can negatively affect their ability to adapt to and recover from the disease [4].
Resilience, a concept that focuses on augmenting patients' strengths, signifies the ability to recover from adversities such as disease, crisis, and trauma [5]. Improving resilience positively impacts cancer patients' overall recovery process [6], as well as their psychological and social adjustment [7] and their sense of life goals [8]. However, not all cancer patients experience the same stresses and crises. Even though their prognosis may involve negative outcomes, these patients often demonstrate a strong will to live and a positive outlook on life. Numerous studies have explored the concept of resilience in cancer patients, but research specifically targeting patients with multiple myeloma in Korea is scarce. Previous studies on resilience in patients with blood cancer, which included a small subset of multiple myeloma patients, have offered some insights [9]. However, these studies have primarily concentrated on psychological aspects such as family support, anxiety, and depression, leaving a gap in our understanding of physical impacts on patients' resilience. Moreover, because these studies did not exclusively focus on multiple myeloma but also included patients with aplastic anemia and myelodysplastic syndrome, their findings cannot be easily generalized to the multiple myeloma population. The applicability of findings from the international literature on depression, resilience, and quality of life in multiple myeloma patients [10] to the Korean context is also limited. This is because these studies did not identify other variables related to resilience beyond depression and quality of life. Multiple myeloma remains an incurable disease, and the uncertainty surrounding disease progression in the early stages places a significant psychological burden on both patients and their families, with a high risk of recurrence even after treatment [11]. Men over the age of 65 are particularly susceptible to developing multiple myeloma. Compared to younger patients with other types of cancer, such as breast cancer, there is a lack of research on psycho-oncological interventions for this older demographic [12]. Therefore, it is necessary to conduct more proactive research on the life processes of cancer patients, considering their treatment is complex and necessitates long-term management. Investigating protective factors such as resilience in patients with multiple myeloma is also essential.
Patients with multiple myeloma experience a variety of symptoms, including peripheral neuropathy, fatigue, and constipation, throughout their treatment [4]. These symptoms persist even after treatment has concluded, significantly limiting patients' ability to engage in normal activities due to ongoing tests to monitor for cancer recurrence and the management of symptoms [13]. Beyond physical symptoms, psychosocial factors can also hinder recovery from the disease. Cancer coping, which refers to the strategies employed to manage the unpredictable course of cancer [14], is a critical variable that affects patients' psychological adjustment, functional level, disease progression, and survival rate [15]. Social support is another key factor that enables cancer patients to cope more effectively with their disease and cancer-related conditions during prolonged periods of illness, serving as a resource that helps patients maintain a positive outlook on life and confront life crises [16]. However, some studies have suggested that there is no relationship between factors such as symptom experience, cancer coping, and resilience [17, 18], underscoring the importance of ongoing research to clarify these connections. In cancer research, social support is typically categorized into two types: family support and healthcare staff support. While family support has been shown to have a significant relationship with resilience in some studies [18, 19], others have found no significant link between healthcare staff support and resilience [9]. Nonetheless, patients' quality of life is affected by the support provided by healthcare professionals [20], and many studies have highlighted the need for further research on external factors such as healthcare staff support [9, 21]. This study was conducted to identify the factors that influence resilience in patients with multiple myeloma, focusing on symptom experience, cancer coping, and social support as the primary variables. We also examined the effects of social support by distinguishing between family support and healthcare staff support. The results of this study are expected to provide foundational data for the development of effective intervention programs aimed at enhancing the resilience of multiple myeloma patients and their adjustment to life as cancer survivors.
The purpose of this cross-sectional descriptive survey was to determine the influence of symptom experience, cancer coping, and social support on resilience in patients with multiple myeloma.
This study was conducted among patients from the hematology department of a university hospital in Seoul, encompassing both inpatients and those attending the outpatient department. The participants included adults aged 19 and older who had been diagnosed with multiple myeloma. These individuals were currently undergoing chemotherapy or were in follow-up care post-cancer treatment. To be eligible for the study, participants needed to be capable of responding to the survey, communicating effectively, understanding the study's purpose, and providing consent to participate. Patients who were either unaware of their diagnosis or unable to communicate were excluded from the study.
The sample size was determined using the G*Power program (version 3.1.9.4), with a significance level set at.05, a power of .80, and a medium effect size of 0.15. Drawing on prior research [18, 22], we estimated that a minimum sample size of 135 would be necessary to accommodate 14 predictors. These predictors included gender, age, marital status, education level, religious, having a job, economic status, time since diagnosis, relapse, physical performance, symptom experience, cancer coping strategies, family support, and healthcare staff support. Considering a dropout rate of 30% based on a previous study [23], the questionnaire was distributed to 176 patients. After excluding incomplete questionnaires, a total of 162 questionnaires were finally used for data analysis.
The general characteristics included a total of 10 items: age, gender, marital status, educational level, religious, importance of religion, having a job, number of family members, primary caregiver, and perceived economic status. Disease-related characteristics comprised 5 items: treatment history (including types of chemotherapy and Hematopoietic Stem Cell Transplantation [HSCT] received to date), relapse, duration of illness, and physical performance. Physical performance ability was measured using the Eastern Cooperative Oncology Group Performance Status (ECOG PS). The ECOG PS is a tool for assessing overall mobility and physical condition, consisting of a single item [24]. It evaluates patients on a scale where grade 0 indicates "fully active, able to carry on all pre-disease performance without restriction," grade 1 signifies "symptomatic but ambulatory, able to carry out work of a light or sedentary nature," grade 2 corresponds to "ambulatory and capable of all self-care but unable to carry out any work activities; up and about more than 50% of waking hours," grade 3 represents "capable of only limited self-care, confined to bed or chair more than 50% of waking hours," and grade 4 denotes "completely disabled; cannot carry on any self-care; totally confined to bed or chair." Higher grades indicate more severe limitations in activity [25].
Symptom experience was measured using the Korean version of the M. D. Anderson Symptom Inventory (MDASI-K) [26, 27]. The MDASI-K is designed to measure a range of symptoms experienced by cancer patients and comprises 19 items. It is divided into two subsections: 13 items evaluate the severity of symptoms, while 6 items assess the extent to which symptoms interfere with daily life. Responses to each item are scored on a scale from 0 (none) to 10 (unimaginably severe). Scores of 5 or 6 denote moderate symptoms, whereas scores of 7 or above indicate severe symptoms. The total possible score spans from 0 to 190, with higher scores reflecting more severe symptomatology. At the time of its development, the tool demonstrated reliability with a Cronbach's α of .82 for symptom severity and .94 for interference with daily life [26]. In the current study, Cronbach's α was .90 for symptom severity and .92 for interference with daily life.
Cancer coping was measured using the Korean-Cancer Coping Questionnaire (K-CCQ) [15], which is a translated and modified version of the Cancer Coping Questionnaire (CCQ) [28]. The K-CCQ comprises 23 items, categorized into two subdomains: the total individual scale with 14 items, and the interpersonal scale with 9 items. These subdomains are designed to evaluate how individuals cope on a personal level and in their interactions with close ones. Responses are scored on a 5-point Likert scale, where 1 point corresponds to "not at all" and 4 points to "very often." The overall score can range from 23 to 92, with higher scores denoting more effective and positive coping strategies for cancer. In the study conducted by Kim et al. [15], the tool demonstrated a high level of reliability with a Cronbach's α of .90, which increased to .93 in the current study.
The social support scale developed by Tae [16] was utilized to evaluate social support, comprising 16 items that are categorized into two sub-areas: family support (8 items) and healthcare staff support (8 items). This instrument facilitates the independent measurement and scoring of each sub-area. In this study, the concepts of family support and healthcare staff support were analyzed distinctly. Consequently, the total score for each sub-area was employed in the analysis, rather than the aggregate score of the entire scale. Each item on the scale is rated using a Likert 5-point scale, which ranges from "not at all" (1 point) to "always" (5 points). The scoring range for both family support and healthcare staff support is from 8 to 40, with higher scores denoting greater levels of social support. At the time of its development, the reliability of the tool was reported as Cronbach's α of .82 for family support and .84 for healthcare staff support [16]. In the current study, the reliability was found to be .91 for family support and .87 for healthcare staff support.
Resilience was measured using the Korean version of the Connor Davidson Resilience Scale (K-CD-RISC) [29, 30]. The K-CD-RISC comprises 25 items that are categorized as follows: 7 items assess personal strength (tenacity), 8 items evaluate the capacity to withstand negative effects such as stress (persistence and durability), 4 items measure the ability to positively adapt to change, 2 items gauge optimism, 2 items pertain to emotional and cognitive control, and 2 items relate to self-efficacy. Each item is rated on a 5-point Likert scale, with options ranging from "not at all" (0 points) to "very much" (4 points). The total score can range from 0 to 100, with higher scores denoting greater resilience. When the tool was initially developed, Cronbach's α was reported as .89 [29]; in the present study, it was .73.
Data collection for this study took place from January to May 2022. Following approval from the Institutional Review Board (IRB) of the hospital where the study participants were receiving care, the researchers approached the nursing department to discuss the study's objectives and secured permission to gather data. Patients with multiple myeloma who met the inclusion criteria were identified during their routine visits to the outpatient clinic for monitoring or while admitted to the hospital for chemotherapy or follow-up care. The researchers explained the study's purpose to these patients, and only those who consented to participate were asked to complete the structured questionnaire. On average, the questionnaire required 20 to 30 minutes to complete. For participants who experienced difficulty completing the questionnaire independently, the researcher assisted by reading the questions aloud and recording the responses.
This study commenced after obtaining approval from the IRB of the researchers' institution (IRB No. KC21 QASI0951). Participants were fully informed about the research purpose, the procedure for completing the questionnaire, and the measures taken to protect their personal information, ensure confidentiality, and prevent the use of their data for any purposes other than the research. They were also advised that their participation was voluntary and that they could withdraw from the study at any time without consequence. Additionally, participants were provided with informational materials. To safeguard confidentiality, the researchers established a secure environment and administered an anonymous survey, identifying respondents solely by numbers. The data collected were to be retained for a period of three years, after which they would be permanently destroyed in a manner that precludes recovery. After data collection was completed, participants who completed the survey were given a small token of appreciation.
SPSS/WIN version 25.0 (IBM Corp., Armonk, NY, USA) was used to analyze the collected data. Descriptive statistics were calculated for the participants' general characteristics, disease-related characteristics, symptom experience, cancer coping, social support, and resilience. The independent t-test and one-way analysis of variance were used to examine the differences in resilience by general and disease-related characteristics, with the Scheffé test used for post-hoc analysis. Pearson correlation analysis was applied to investigate the relationships among symptom experience, cancer coping, social support, and resilience. Variables that demonstrated significant correlations in the univariate analysis were introduced as independent variables in the hierarchical regression analysis to identify the factors that influenced resilience.
The average age of the participants was 62.24±9.26 years, with 106 (65.4%) being under 65 years old. Eighty-three participants were women (51.2%), and 145 (89.5%) were married. Sixty-eight participants (42.0%) were high school graduates, while 64 (39.5%) held a college degree or higher. A total of 101 individuals (62.3%) identified as religious, with 78 (48.1%) considering religion to be important in their lives. Forty-three participants (26.5%) were currently employed. When asked about number of family member, excluding the participant, 51 (31.5%) reported having one family member, while 44 (27.2%) had two. The spouse was the most common primary caregiver (114 participants, 70.4%), with children serving as caregivers for 39 participants (24.1%). With respect to perceived economic status, the majority classified themselves as middle-class (99 participants, 61.1%), followed by those identifying as "low" (35 participants, 21.6%), and "high" (28 participants, 17.3%).
Regarding disease-related characteristics, 98 patients (60.5%) underwent chemotherapy and autologous transplant, 54 patients (33.3%) received only chemotherapy, and 10 patients (6.2%) were treated with chemotherapy and allogeneic transplant. A total of 90 patients (55.6%) had experienced a relapse. The time since diagnosis ranged from 1 to 3 years for 65 patients (40.1%) and was over 5 years for 54 patients (33.3%). The average ECOG PS was 2.26 with a standard deviation of ±1.01 (Table 1).
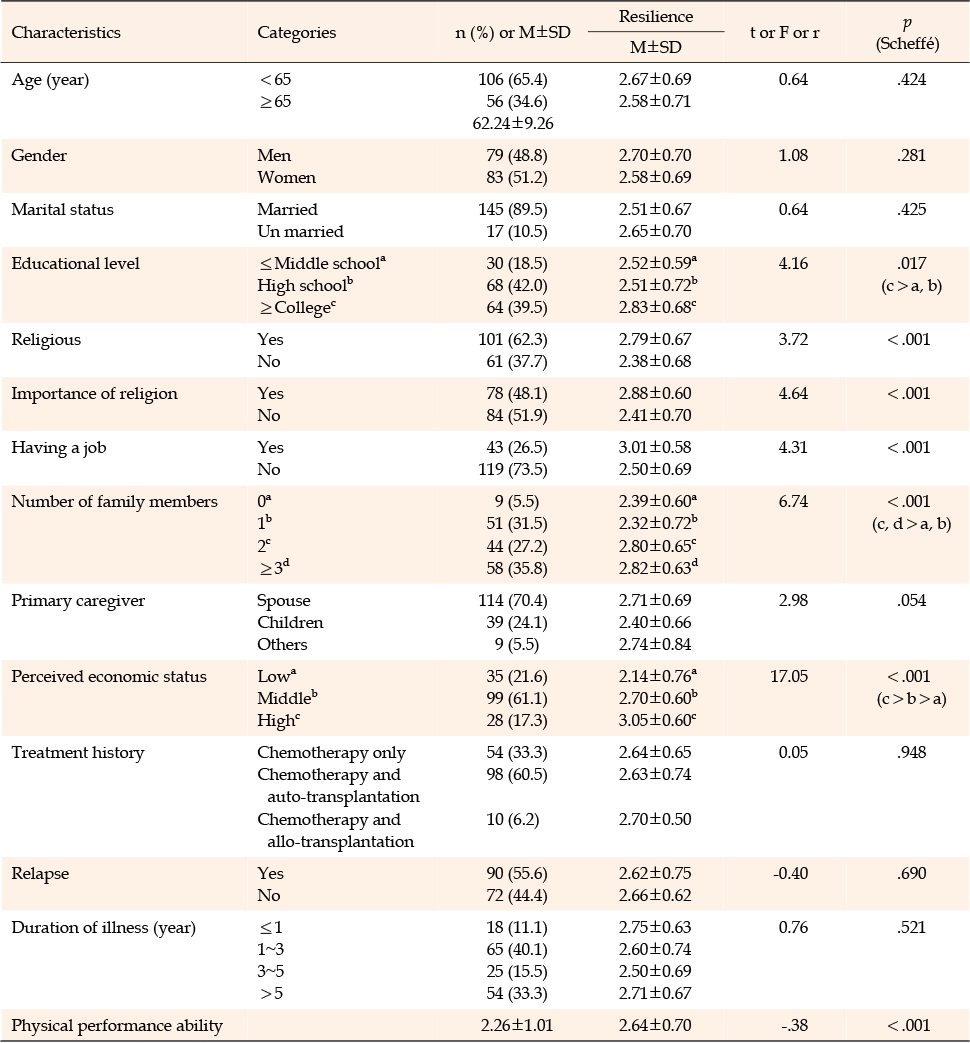
Table 1
Differences in Resilience according to General and Disease-related Characteristics (N=162)
The average score for symptom experience was 54.72±36.14, and that for cancer coping was 56.12±12.88. For social support, the average scores were 32.80±6.88 for family support and 30.56±7.04 for healthcare staff support. The average resilience score was 66.00±17.50 (Table 2).

Table 2
Levels of Symptom Experience, Cancer Coping, Social Support, and Resilience in Patients with Multiple Myeloma (N=162)
Statistically significant differences in resilience were observed across various general characteristics, including educational level, religious, the importance of religion, having a job, number of family members, and economic status. Specifically, participants with a college degree or higher exhibited greater resilience compared to those with only a middle or high school education (F=4.16, p=.017). Individuals who were religious (t=3.72, p<.001) and those who considered religion to be important (t=4.64, p<.001) also showed higher resilience. Regarding having a job, employed individuals were found to be more resilient than the unemployed (t=4.31, p<.001). Post-hoc analysis revealed that number of family member significantly predicted resilience (F=6.74, p<.001), with individuals from families with more than two members displaying greater resilience than those from smaller families with none or one family member. Perceived economic status also significantly affected resilience (F=17.05, p<.001), with post-hoc analysis showing a sequence of increasing resilience from those with low to medium to high economic status. Conversely, physical performance ability was negatively correlated with resilience (r=-.38, p<.001) (Table 1).
Resilience was found to be negatively correlated with symptom experience (r=-.26, p<.001), while it had a positive correlation with cancer coping (r=.50, p<.001). Resilience showed positive correlations with both family support (r=.43, p<.001) and healthcare staff support (r=.42, p<.001) (Table 3).
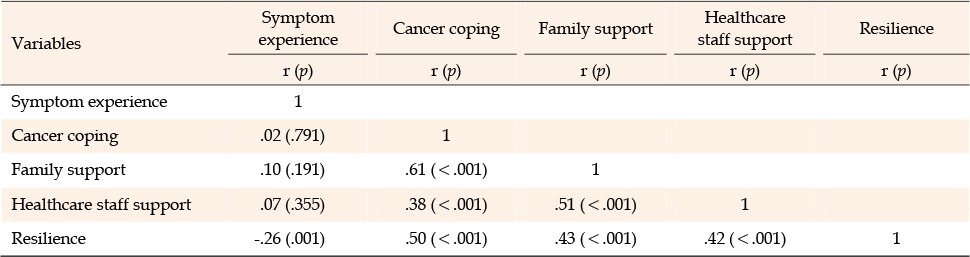
Table 3
Correlations among Symptom Experience, Cancer Coping, Social Support, and Resilience (N=162)
A three-step hierarchical regression analysis was conducted to identify factors that influence the resilience of participants (Table 4). The initial step incorporated variables that demonstrated statistically significant correlations with resilience in the univariate analysis, including religious, the importance of religion, educational level, having a job, number of family members, perceived economic status, and physical performance. In the second step, psychosocial factors such as symptom experience, cancer coping, and family support were added. This was done while controlling for the effects of general and disease-related characteristics to assess their direct impact on resilience. Finally, the third step introduced healthcare staff support as a variable that can be modified in clinical practice, to explore its direct effect on resilience.
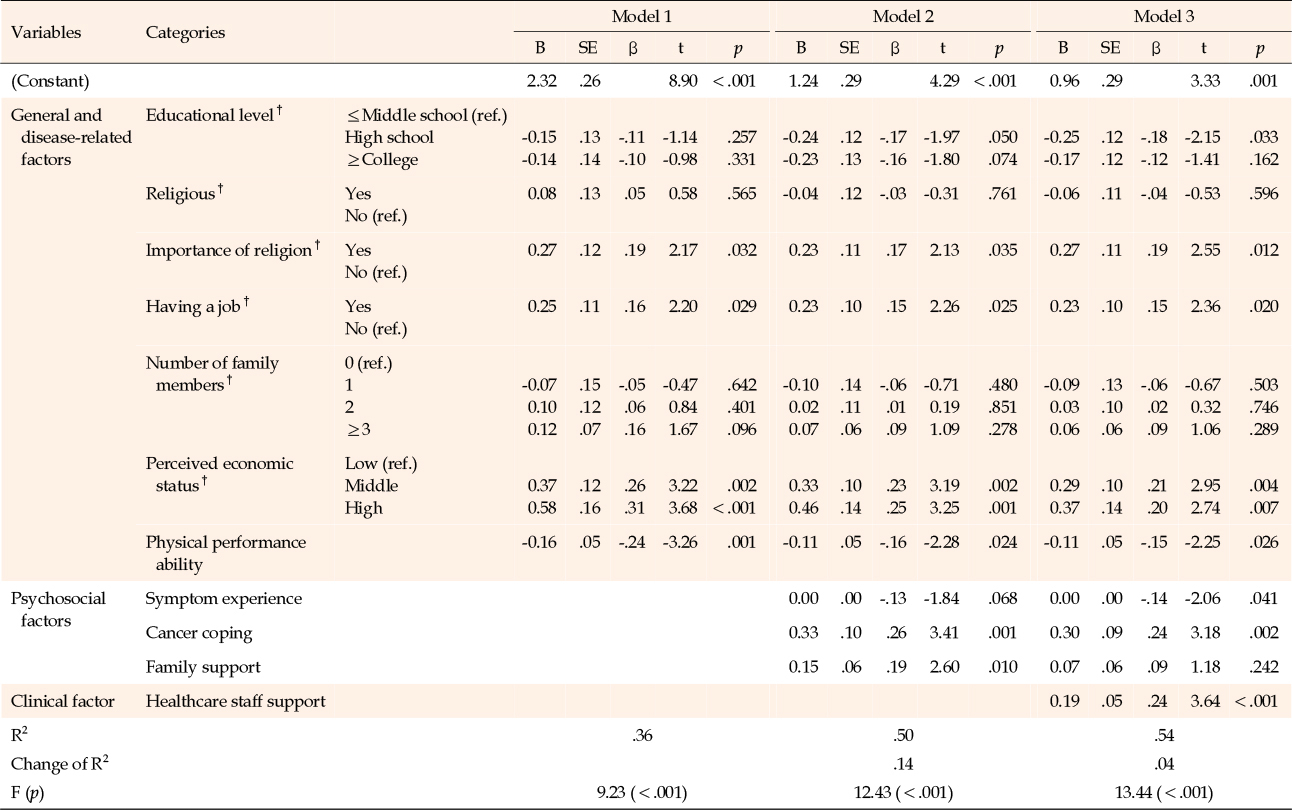
Table 4
Factors Influencing Resilience in Patients with Multiple Myeloma (N=162)
An assessment of the regression analysis's basic assumptions revealed that the correlation coefficients between the independent variables ranged from -0.06 to 0.51. This confirmed the independence of the variables, as none of the coefficients exceeded the threshold of 0.60. The tolerance values were between 0.42 and 0.74, all of which are above the minimum acceptable level of 0.1, and the Variance Inflation Factor (VIF) values ranged from 1.36 to 2.63. These VIF values are well below the critical value of 10, indicating that multicollinearity is not a concern. The assumptions regarding residuals were also satisfied. The normality of residuals was confirmed by the Kolmogorov-Smirnov test (z=0.875, p=.429), homoscedasticity was established by the Breusch-Pagan test (p=14.180, p=.512), and linearity was verified. The Durbin-Watson statistic of 1.98, with a Du value of 1.89, fell within the acceptable range of 1.89 to 2.11, suggesting the absence of autocorrelation.
In the hierarchical regression analysis, the factors significantly influencing resilience in Model 1 were the importance of religion (p=.032), having a job (p=.029), medium economic status (p=.002), high economic status (p<.001), and ECOG PS (p=.001), explaining 36.0% of the variance.
In Model 2, symptom experience, cancer coping, and family support were added as independent variables. The variances explained increased by 13.8% (p<.001), with cancer coping (β=.26, p=.001) and family support (β=.19, p=.010) significantly influencing resilience. This model accounted for 50.0% of the variance.
In Model 3, the addition of healthcare staff support increased the explained variance by 4.0% (p<.001), with symptom experience having a significant negative impact (β=-.14, p=.041), and both cancer coping (β=.24, p=.002) and healthcare staff support (β=.24, p<.001) having significant positive impacts. This model explained 54.0% of the resilience (Table 4).
This study aimed to assess resilience levels in patients with multiple myeloma and to determine the influence of symptom experience, cancer coping strategies, and social support on their resilience. We found that the average resilience score for patients with multiple myeloma was 66 out of 100. This score is lower than those reported in studies using the same measurement tool in patients with other hematologic malignancies, such as 71 points for other blood cancers [9] and 73 points for non-Hodgkin lymphoma [22]. It is also below the scores of elderly gastric cancer patients [18] (99 points) and colorectal cancer patients [19] (84 points). These findings indicate that the resilience of multiple myeloma patients is not only lower compared to other disease groups but also in comparison to other patient groups with similar hematologic conditions. The reduced resilience in multiple myeloma patients may be attributed to the frequent relapses and the demanding treatment regimens, which include chemotherapy and HSCT, as well as the associated symptoms and side effects [4]. Therefore, it is important to recognize their vulnerability in terms of resilience and develop nursing interventions to improve it.
Patients who reported experiencing symptoms in this study exhibited lower resilience levels compared to those without symptoms. This observation aligns with prior research involving elderly gastric cancer patients [18], yet it stands in contrast to findings from a study on lung cancer patients receiving chemotherapy [17]. Among multiple myeloma patients, fatigue was the most frequently reported complaint, followed by numbness, dry mouth, pain, and sleep disturbances. These symptoms may be associated with HSCT and innovative treatment approaches. Additionally, conditions such as neutropenia, peripheral neuropathy, fatigue, constipation, and embolism are likely related to these treatments [4]. Therefore, tailored management of side effects, considering the specific type and stage of treatment, is crucial for enhancing patient resilience.
Positive cancer coping was associated with a higher level of resilience. This finding aligns with studies on posttraumatic growth among breast cancer patients, where the approach to coping with cancer was a significant factor [14]. Coping is defined as the cognitive and behavioral efforts exerted to manage stressful situations that surpass an individual's capacity [28]. During recovery, cancer patients often employ positive coping strategies, such as planning, rather than resorting to defensive or avoidant tactics [31]. This suggests that the active and positive nature of coping can positively affect their resilience. To improve the resilience of patients with multiple myeloma, it is important to develop nursing interventions that encourage positive coping strategies.
Resilience in multiple myeloma patients was influenced by general characteristics. Specifically, those who were employed, valued religion, and perceived themselves to have a higher economic status tended to be more resilient. This aligns with previous research that has shown greater resilience among blood cancer patients who are employed and have a household income exceeding KRW 3 million [9]. These findings highlight the importance for nurses to consider employment and economic status as factors that can affect resilience, as well as the need to explore realistic social resources available to patients. Additionally, this study revealed that placing a stronger emphasis on the significance of religion correlates with higher resilience scores, regardless of the individual's religious affiliation. This indicates that the personal importance placed on religion may impact resilience, suggesting that further research is warranted to understand how spirituality contributes to resilience.
Physical performance influenced resilience in multiple myeloma patients in the current study. A positive correlation between higher levels of physical performance and resilience was observed, which is consistent with findings from previous research on colorectal cancer [32] and lymphoma patients [22]. Assessing physical performance is essential for selecting appropriate treatment methods in cancer care and should commence at the onset of therapy [33]. Patients with multiple myeloma may experience fluctuations in physical performance due to complications arising from treatment modalities such as chemotherapy. To improve physical performance, it is imperative for healthcare providers to regularly monitor patients' physical capabilities throughout their treatment and address any issues that may stem from reduced activity levels.
Higher levels of healthcare staff support were associated with increased resilience in multiple myeloma patients. In Model 3, the inclusion of healthcare staff support accounted for an additional 4.0% of the variance in resilience, confirming the direct effect of this support. This result is in line with previous research [19], which suggests that access to multidisciplinary resources and activities is essential for the optimal well-being of cancer patients during treatment. Consequently, medical professionals who care for multiple myeloma patients should actively participate in interventions that aim to enhance their psychosocial state and resilience. Although family support significantly boosted resilience in Model 2, its influence diminished when healthcare staff support was factored into Model 3. This observation contrasts with a study on breast cancer surgery patients, where family support emerged as the most influential factor in resilience [34]. Additionally, in a study encompassing colorectal cancer patients [19], the ultimate regression model disclosed that family support, among the social support variables, failed to attain statistical significance, consistent with our findings. Therefore, future studies should utilize various models to explore the relationship between social support-encompassing both healthcare staff and family support-and resilience. Previous studies on breast cancer patients [35] have shown that family support tends to decrease as the duration and frequency of treatment increase. However, the current study cannot corroborate this finding, as more than half of the participants had been diagnosed for over 3 years, and the study did not assess changes in resilience over the course of the disease. Therefore, additional research on the relationship between disease duration, family support, and resilience is recommended.
The limitations of this study are as follows: It was conducted with multiple myeloma patients from a single hospital and used convenience sampling, which may limit the representativeness of the study population. Additionally, the study did not consider the impact of different treatment drugs or the number of treatments received. Since the data on disease-related characteristics were collected through participants' subjective memories and self-reports, caution should be exercised when generalizing the findings. Despite these limitations, the study is significant as it has identified factors that influence the resilience of patients in Korea. From the perspective of nursing education, this study underscores the importance for clinical nurses to focus on patients' physical performance, symptom experience, cancer coping strategies, and the level of family support. It highlights the need to enhance these areas to improve patient outcomes. Moreover, the study contributes to a better understanding of resilience in multiple myeloma patients and emphasizes the critical role of healthcare staff support. This suggests a need for comprehensive nursing interventions that address both psychosocial and physical aspects, led by medical professionals. In terms of nursing research, the study is valuable as it identifies the level of resilience and its related factors, providing essential data for the development of intervention programs. For nursing practice, the study offers foundational data for creating multifaceted interventions aimed at helping multiple myeloma patients manage their disease, adapt to daily life, and maintain social engagement.
The study's findings underscore the importance of routinely evaluating the physical performance of patients with multiple myeloma, mitigating the physical symptoms resulting from chemotherapy side effects, and supporting their active engagement in managing stress. These interventions are crucial for facilitating their recovery process.
The study discovered that having a job, the importance of religion, economic status, physical performance, symptom experience, cancer coping, and healthcare staff support all influenced resilience in multiple myeloma patients. The findings of this study indicate that strategies to improve patients' resilience should include regular assessments of physical performance, as well as interventions and support for active coping in stressful situations. Future research should aim to identify more specific predictors of resilience in multiple myeloma patients, including various latent variables. Additionally, it is recommended to develop and test the effectiveness of programs designed to boost resilience. These programs should address the management of side effects tailored to the specific treatment drugs and stages of treatment, evaluate issues related to reduced activity levels, and provide psychological support while imparting knowledge for self-management and promoting behavioral changes.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - JHL & YHA.
Data collection - JHL.
Analysis and interpretation of the data - JHL & YHA.
Drafting and critical revision of the manuscript - JHL & YHA.
This article is a revision of the first author's master's thesis (dissertation) from The Catholic University of Korea.
This paper was researched with the support of the Hanmaum Scholarship from the Seoul Nurses Association in 2021.
 E-SUBMISSION
E-SUBMISSION