
Purpose
Middle-aged women often experience weight gain, particularly as visceral fat, due to hormonal changes associated with menopause. Visceral fat, which accumulates in the abdomen, poses significant risks to cardiometabolic health. This cross-sectional study aimed to compare the cardiometabolic risks associated with Visceral Fat Obesity (VFO) and Subcutaneous Fat Obesity (SFO) in middle-aged Korean women and to identify factors that influence VFO.
Methods
Women aged 40 to 64 with overweight or obesity were recruited from March to April 2019. The study involved anthropometric measurements, fasting blood tests, and low-volume abdominal computed tomography. Additionally, participants provided self-reported sociodemographic, health-related, and lifestyle information, including Physical Activity (PA) and dietary intake.
Results
Of all participants, 70.8% were post-menopausal, and 55.1% had VFO. Those with VFO exhibited significantly higher mean values for waist circumference, total cholesterol, low-density lipoprotein cholesterol, triglycerides, fasting glucose, high sensitivity C-reactive protein, and the Framingham risk score compared to those with SFO. The factors influencing VFO were age (odds ratio (OR)=1.14; 95% confidence interval (CI), 1.032~1.247), body mass index (OR=1.47; 95% CI, 1.151 ~1.875), days of vigorous PA per week (OR=0.42; 95% CI, 0.244~0.735), and intake of animal calcium (OR=0.99; 95% CI, 0.988~0.997).
Conclusion
The findings indicate that middle-aged women with VFO face increased cardiometabolic risks. Since menopause is inevitable in women, targeting modifiable behaviors to reduce weight, particularly visceral fat, is crucial for lowering cardiometabolic risk.
Middle-aged women often experience weight gain, particularly as visceral fat, due to hormonal changes associated with menopause. Visceral fat, which accumulates in the abdomen, poses significant risks to cardiometabolic health. This cross-sectional study aimed to compare the cardiometabolic risks associated with Visceral Fat Obesity (VFO) and Subcutaneous Fat Obesity (SFO) in middle-aged Korean women and to identify factors that influence VFO.
Women aged 40 to 64 with overweight or obesity were recruited from March to April 2019. The study involved anthropometric measurements, fasting blood tests, and low-volume abdominal computed tomography. Additionally, participants provided self-reported sociodemographic, health-related, and lifestyle information, including Physical Activity (PA) and dietary intake.
Of all participants, 70.8% were post-menopausal, and 55.1% had VFO. Those with VFO exhibited significantly higher mean values for waist circumference, total cholesterol, low-density lipoprotein cholesterol, triglycerides, fasting glucose, high sensitivity C-reactive protein, and the Framingham risk score compared to those with SFO. The factors influencing VFO were age (odds ratio (OR)=1.14; 95% confidence interval (CI), 1.032~1.247), body mass index (OR=1.47; 95% CI, 1.151~1.875), days of vigorous PA per week (OR=0.42; 95% CI, 0.244~0.735), and intake of animal calcium (OR=0.99; 95% CI, 0.988~0.997).
The findings indicate that middle-aged women with VFO face increased cardiometabolic risks. Since menopause is inevitable in women, targeting modifiable behaviors to reduce weight, particularly visceral fat, is crucial for lowering cardiometabolic risk.
Obesity, which involves an excess of adipose tissue, is recognized as one of the most prevalent and preventable health issues [1]. While the rates of obesity and overweight among Korean adults are lower than in many developed countries, the westernization and urbanization of lifestyles in Asia have contributed to a rise in obesity-related diseases [2]. The Korean Ministry of Health and Welfare reported that in 2019, 33.8% of Korean adults were obese, with men at 41.8% and women at 25.0%. Furthermore, the prevalence of obesity in women increased with age [3]. A linear relationship between age and obesity has been observed among Korean women, with 25.8% in their 40s, 29.6% in their 50s, and 34.9% in their 60s, based on the Korean obesity guidelines which define obesity as a Body Mass Index (BMI) of 25 kg/m2 or higher [3, 4].
Obesity is widely recognized as a significant risk factor for Cardiovascular Disease (CVD) and metabolic disorders. However, not all forms of obesity are equally concerning. The specific type of obesity that poses a risk is determined by the distribution of body fat [5]. Central obesity, characterized by an excessive accumulation of visceral and subcutaneous fat in the abdomen, can lead to complications such as hypertension, abnormal serum lipid levels, heart disease, stroke, and elevated insulin levels [1]. Visceral fat is also linked to insulin resistance, hyperinsulinemia, Type 2 Diabetes Mellitus (T2DM), dyslipidemia, increased inflammatory levels, and blood clot formation. Moreover, it serves as an independent marker for increased risk of cardiovascular and metabolic morbidity and mortality [6].
Cardiometabolic risk involves assessing the combined risk factors associated with CVD and metabolic disorders [7]. Metabolic Syndrome (MS) is characterized by a cluster of conditions including abdominal obesity, elevated Blood Pressure (BP), reduced High-Density Lipoprotein-Cholesterol (HDL-C), and increased levels of triglycerides and blood glucose. Individuals with MS are five times more likely to develop T2DM and three times more likely to develop CVD than those without MS [8]. The identification of CVD in conjunction with MS has led to the concept of cardiometabolic syndrome [7]. Notably, in 2022, CVD was the second leading cause of death among Koreans, with the mortality rate for women being higher than for men, at 140.6 and 128.7 per 100,000, respectively [9].
Visceral adipose tissue is known to increase until the ages of 65~70, after which it decreases in both men and women [10]. In women, the onset of menopause typically leads to a gradual increase in body fat during their 40s, while decreases in estrogen and progesterone levels can accelerate the accumulation of visceral fat [11]. Although the distribution of body fat is influenced by various factors, previous studies primarily examined the effects of age [12] and Physical Activity (PA) [13] on the Visceral Fat Area (VFA). The objectives of this study were to 1) investigate the cardiometabolic risks associated with different types of obesity by comparing Visceral Fat Obesity (VFO) and Subcutaneous Fat Obesity (SFO) in terms of VFA, and 2) identify specific factors influencing VFO in middle-aged Korean women who are overweight or obese.
This study employed a cross-sectional design. The sample size was calculated for logistic regression using the G*Power 3.1.9.4 program. A minimum of 89 participants was required, with a significance level set at .05, an odds ratio of 1.933 [14], a power (1-β) of .80, and an incidence rate of 50.0% for VFO. Convenience sampling was utilized to recruit participants. Korean women aged 40 to 64 years were recruited from two community centers and one sports center in Seoul, where their height and weight were measured. Women with a BMI of 23 kg/m2 or higher were classified as overweight or obese [4] and were recruited between March and April 2019. The exclusion criteria included women who were pregnant or had severe illnesses that disrupted daily functioning.
This investigation adhered to the principles set forth in the Declaration of Helsinki. Data collection commenced following approval from the Korea University Institutional Review Board (KUIRB-2019-0030-02). Written informed consent was obtained from each participant.
Self-reported questionnaires were used to collect sociodemographic data, health-related information, and lifestyle characteristics. The sociodemographic data included age, marital status, highest level of education completed, occupation, monthly household income, and religion. Health-related information encompassed age at menopause, comorbidities, medications, and family history of CVD. Lifestyle characteristics covered PA and eating habits. Participants completed a short version of the International Physical Activity Questionnaire (IPAQ) [15] in Korean, which was analyzed according to the guidelines of the IPAQ Research Committee [16]. For participants who exercised regularly, additional questions were asked about the types of exercise, weekly frequency, and duration.
For assessing eating habits, researchers utilized a three-day food diary along with 24-hour recall and intake frequency questionnaires. Sodium intake habits were evaluated using questionnaires previously employed in the "My Heart My Mind" study [17], adhering to the nutritional guidelines set by the National Hypertension Center in Korea. The questionnaire identified foods high in sodium based on weekly intake frequency. In this study, Cronbach's α for this scale was .60. Fat intake was measured using a Korean version of the Food Habits Questionnaire [18]. A score of 2.5 or higher, derived from dividing the total score by the number of questions, was interpreted as high fat intake, accounting for 29.0% or more of total caloric intake from fat. Cronbach's α for this tool was .73 in a previous study [19] and .65 in the current study. Permission to use these measurements was obtained from the original developer and translator via email.
The survey inquired about the regularity of meal times, frequency of eating out, late-night meals, and supper times. Additionally, participants were asked to keep a 3-day food diary based on a 24-hour recall method. The intake of nutrients, including calories, carbohydrates, fats (animal/plant), proteins (animal/plant), dietary fiber, calcium (animal/plant), sodium, potassium, iron, and cholesterol, was assessed using the CAN-pro 4.0, a computer-aided nutritional analysis program developed by the Korean Nutrition Society.
Obesity-related characteristics were assessed by measuring BMI, which involved recording height and body weight (DS-102, Dongshan Genix). Additionally, body fat percentage and muscle mass were evaluated using bioelectric impedance analysis (IOI 353, Jawon Medical). Abdominal body fat measurements, such as VFA, Subcutaneous Fat Area (SFA), and the VFA/SFA ratio, were obtained through low-volume abdominal computed tomography (LVACT). VFO was defined as having a VFA of 100 cm2 or greater on LVACT [20].
Cardiometabolic risk was assessed using five components of MS: Waist Circumference (WC), BP, triglycerides, HDL-C, and Fasting Blood Glucose (FBG) [21]. Additional factors included Total Cholesterol (TC), Low-Density Lipoprotein Cholesterol (LDL-C), High-Sensitivity C-Reactive Protein (hs-CRP), and a 10-year CVD risk estimate calculated by the Framingham Risk Score (FRS). Waist circumference was measured with a flexible tape. BP readings were obtained using an automatic machine (EASY X 800R/L, Jawon Medical). A minimum fasting period of 10 hours was required before blood tests at Korea University Hospital. The CVD risk associated with hs-CRP was stratified into three categories: <1.0 mg/L for low risk, 1.0~3.0 mg/L for moderate risk, and >3.0 mg/L for high risk [22]. The 10-year CVD risk estimate was used to predict the likelihood of coronary artery diseases over the next decade. Factors such as age, smoking status, FBG, systolic BP, TC, and HDL-C were used to calculate these risk scores. The Framingham risk score was divided into three risk categories: low (<10.0%), moderate (10.0~20.0%), and high (>20.0%) [23].
Statistical analyses were conducted using SPSS v.24 (IBM Corp., Armonk, USA). For variables with normal and non-normal distributions, the independent t-test or Mann-Whitney U-test was utilized for between-group comparisons. Categorical variables were analyzed using the χ2 test or Fisher exact test. Multiple logistic regression models were employed to explore the factors influencing the incidence of VFO. A significance level of 5% (p<.05) and 95% confidence intervals (CIs) were applied.
The mean age of all participants (n=89) was 51.99±6.83 years, with 63 women (70.8%) being post-menopausal. Over half (55.1%) were identified as having VFO, defined by a VFA of 100 cm2 or more, as measured by LVACT. The sociodemographic and health-related information of participants, categorized by obesity type, is detailed in Table 1. The average age of participants with VFO was 52.76±6.99, compared to 51.05±6.60 for those with SFO; however, this difference was not statistically significant. On average, each woman had 1.25±1.33 comorbidities, with 66.3% reporting one or more diseases beyond obesity. Dyslipidemia (21.3%) and hypertension (16.9%) were the most prevalent comorbidities. Notably, the incidence of dyslipidemia was more than double in women with VFO compared to those with SFO (χ2=3.39, p=.066). Of the 19 women diagnosed with dyslipidemia, only nine (47.3%) adhered to their prescribed medication regimen. Among the 15 women with hypertension, 12 (80.0%) were taking antihypertensive medications. In the VFO group, four women reported having T2DM, whereas none in the SFO group did. Differences in sociodemographic and health-related information between the groups were not statistically significant.
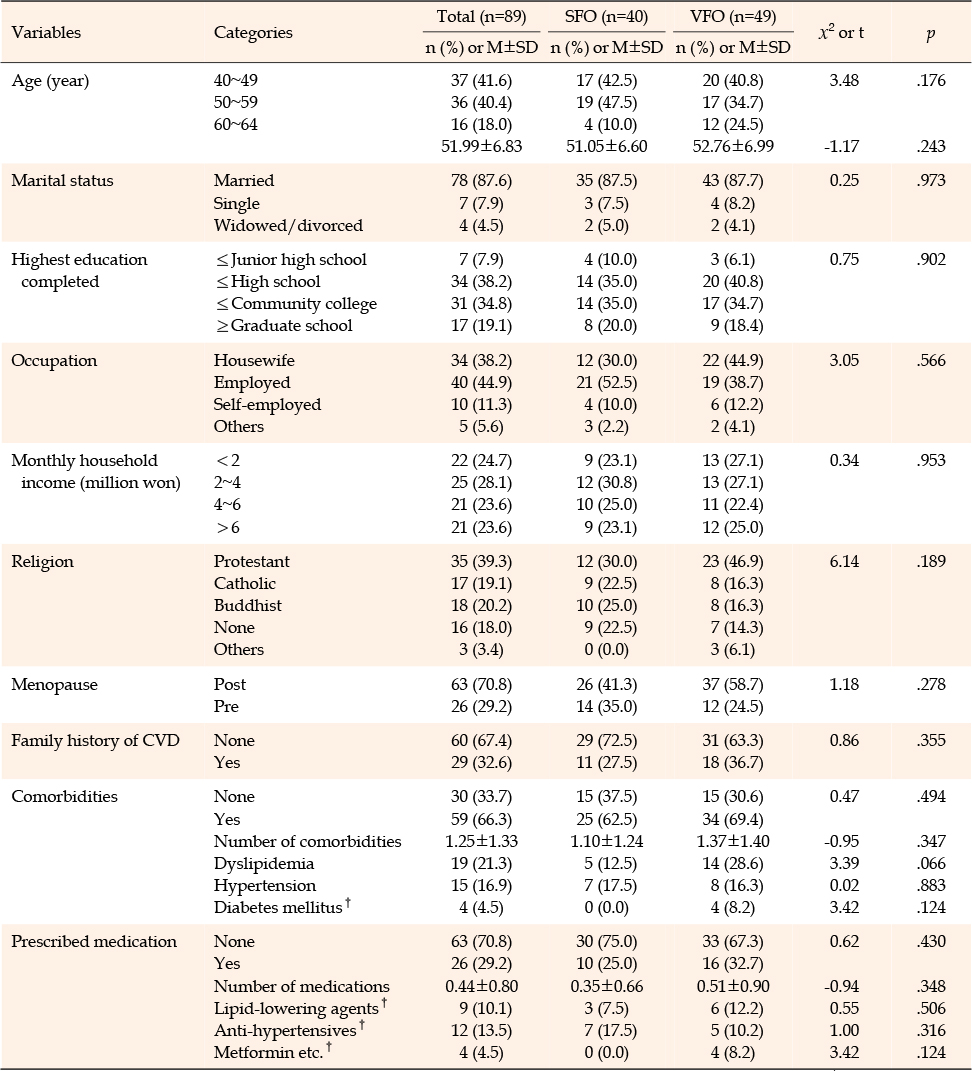
Table 1
Sociodemographic and Health-related Characteristics of Participants
When their PA was analyzed by obesity type (Table 2), a significant difference in the regularity of PA between groups was observed (χ2=4.47, p=.035). Only 10.2% (n=5) of the VFO group engaged in regular exercise, compared to 27.5% (n=11) in the SFO group. The average number of days per week spent on vigorous PA was significantly higher in the SFO group compared to the VFO group (t=2.34, p=.023).
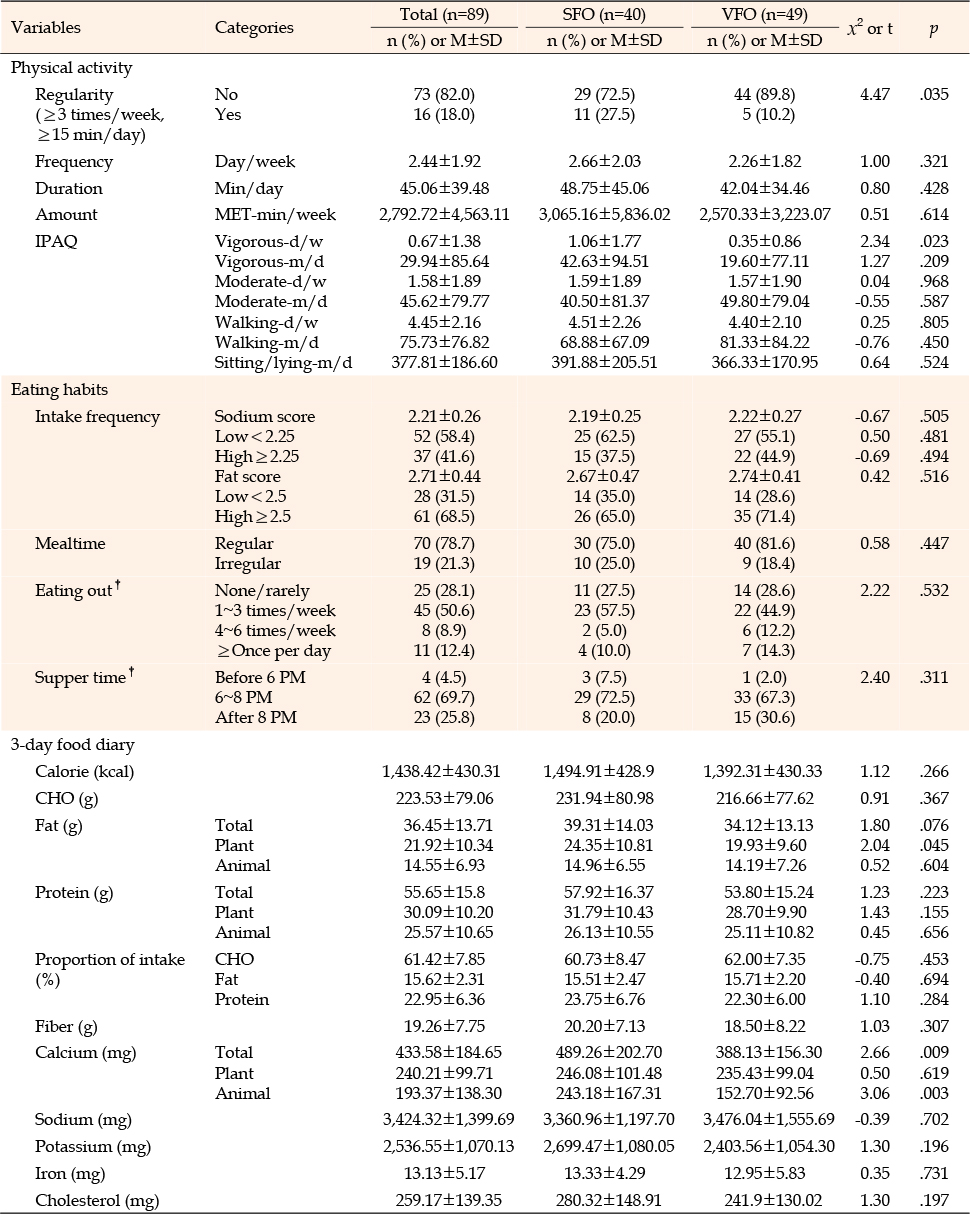
Table 2
Comparison of Lifestyle Characteristics Based on Obesity Type
Concerning diet, 78.7% (n=70) of the participants ate regularly, and their intake of protein, fat, and carbohydrates was deemed adequate according to their 3-day dietary recall (Table 2). The majority of women in both groups consumed high levels of fat; 71.4% (n=35) in the VFO group and 65.0% (n=26) in the SFO group. The average frequency score for fat intake was high in both groups. Fat intake in the VFO group (2.74±0.41) was slightly higher than in the SFO group (2.67±0.47), though the difference was not statistically significant. According to the analysis of daily nutrient intake from the 3-day food diary, the mean intake of plant fat in the VFO group was significantly lower than that in the SFO group (t=2.04, p=.045). Similarly, the intake of animal calcium in the VFO group was significantly lower than in the SFO group (t=3.06, p=.003). Although the differences were not significant, a higher proportion of participants in the VFO group reported eating out more than four times per week or once daily, and having late dinners after 8 PM, compared to those in the SFO group (26.5% vs 15.0%; 30.6% vs 20.0%).
Obesity indicators are detailed in Table 3. The mean BMI values and body fat percentages for both groups classified them as obese; however, the VFO group exhibited significantly higher BMI values than the SFO group (t=-2.98, p=.004). Specifically, 57.3% (n=51) of the participants were obese, 32.6% (n=29) were overweight, and 10.1% (n=9) were severely obese. The difference in the distribution of obesity levels between the groups was significant (χ2=7.83, p=.018), indicating a higher prevalence and severity of obesity in the VFO group. Additionally, the VFO group had significantly higher mean body fat rates (t=-3.03, p=.003), higher mean VFA (t=-11.04, p<.001), and a higher mean ratio of visceral to subcutaneous fat (t=-7.10, p<.001) than the SFO group. No significant differences were observed in muscle mass or SFA between the two groups.
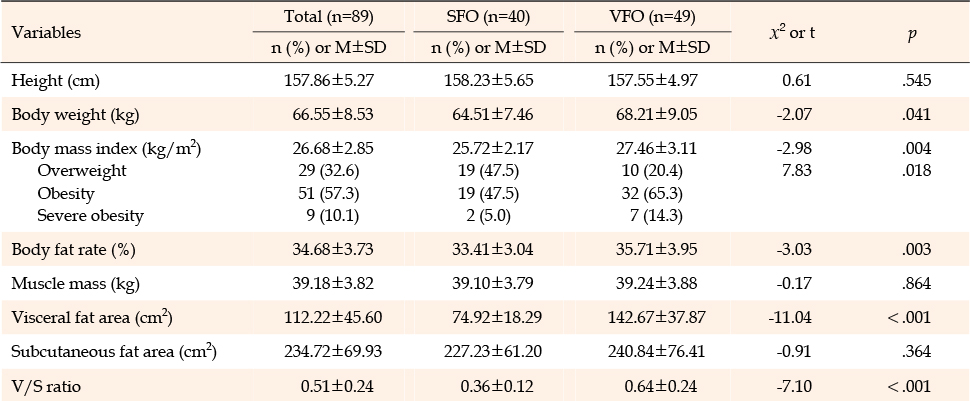
Table 3
Comparison of Obesity Indicators Based on Obesity Type
MS factors, LDL-C, TC, hs-CRP, and FRS are summarized in Table 4. The mean values of WC for the VFO and SFO groups indicated abdominal obesity (92.89±6.25 cm and 88.87±6.42 cm, respectively). The mean values of WC (t=-2.98, p=.004), triglycerides (t=-5.15, p<.001), and FBG (t=-2.27, p=.010) in the VFO group were found to be abnormal and significantly higher than in the SFO groups. There were no significant differences in the mean values of BP and HDL-C between two groups, and both values were within normal ranges. In the VFO group, the mean values of TC (t=-2.27, p=.026) and LDL-C were abnormal and significantly higher than those of the SFO group (t=-2.38, p=.020). The median value of hs-CRP in the VFO group, was 1.10 indicating moderate risk for CVD, and this value was significantly higher than that in the SFO group (0.38; z=-3.71, p<.001). In the VFO group, there were 20 (40.8%) individuals at moderate risk and six (12.2%) at high risk for CVD, whereas in the SFO group, there were only seven (17.5%) at moderate risk and two (5.0%) at high risk. The frequency of hs-CRP-related CVD risk was almost three times higher in the VFO group, making this difference significant (χ2=8.47, p=.011). The estimated 10-year CVD risk for the VFO group was 7.09±4.37%, significantly higher than that of the SFO group, which was 4.99±2.74% (t=-2.76, p=.007).
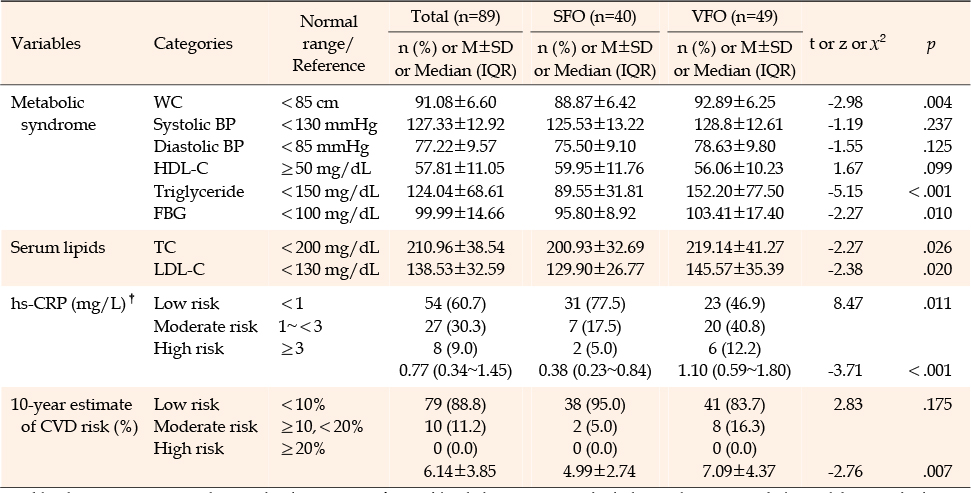
Table 4
Comparison of Cardiometabolic Risk Based on Obesity Type
Multiple logistic regression models were employed to explore the factors influencing the incidence of VFO. Variables that were statistically significant in the univariate analyses were included as covariates if they had a p-value less than 0.25. Four variables remained significant: BMI, animal calcium intake, number of days engaging in vigorous PA per week, and age (Table 5). The fit of the regression model was confirmed to be adequate (χ2=36.82, p<.001), and Nagelkerke's R2 was 45.3%. Overall, this model was able to accurately classify 78.7% of VFO cases.

Table 5
Factors Influencing Visceral Fat in Middle-aged Women with Overweight or Obesity
The four variables were significantly associated with the presence of VFO. Specifically, while controlling for other variables, the odds of having VFO increased by 1.47 times with each 1 kg/m2 increase in BMI (95% CI=1.151~1.875) compared to SFO. Additionally, the odds of having VFO decreased by 57.6% with each additional day of vigorous PA participation per week (OR=0.42; 95% CI=0.244~0.735). Furthermore, the odds of having VFO increased by 1.14 times with each additional year of age (95% CI=1.032~1.247). Lastly, the odds of having VFO decreased by 1% with each 1-mg increase in animal calcium intake (OR=0.99; 95% CI=0.988~0.997).
This study demonstrated an association between VFO and cardiometabolic risk in middle-aged women with excessive weight. Additionally, factors such as age, BMI, frequency of vigorous PA per week, and intake of animal-derived calcium were found to influence VFO in this demographic. These findings are consistent with previous research that identified aging as a risk factor for the accumulation of visceral fat [6, 12]. This relationship may be linked to hormonal changes that occur during menopause in middle-aged women. Estrogen significantly influences fat distribution, leading to a tendency for men to accumulate fat in the abdominal region and for women in the thighs. The perimenopausal period is characterized by a significant decrease in estrogen levels, which is accompanied by a redistribution of fat from subcutaneous to visceral areas [24]. Previous research has shown that VFA increased significantly by 8.2% and 5.8% annually, both two years before and after the final menstrual period, indicating that the prevalence of visceral adiposity increases with age [11].
Previous studies have demonstrated a positive association between BMI and visceral fat [25]. Although BMI does not distinguish between muscle and fat mass, nor does it consider the distribution of fat, it continues to be a practical tool for assessing obesity in clinical settings. Nevertheless, its limitations should be acknowledged, especially in situations where regional fat distribution is crucial for cardiometabolic health.
The frequency of vigorous PA has been shown to positively impact the reduction of VFO. This aligns with findings from a previous meta-analysis, which indicated that aerobic exercise of a certain intensity effectively reduces VFA [13]. High-intensity physical activity promotes the release of adiponectin, and studies have established a strong correlation between adiponectin levels and changes in visceral adipose tissue [26]. Research suggests that high-intensity exercise is more effective than moderate or low-intensity exercise in reducing visceral adipose tissue and improving insulin sensitivity, with intensity being more crucial than duration [27]. However, the relationship between exercise intensity and VFA requires further experimental research using more objective and accurate measurements, as the findings of this study were based on self-reported data, which are vulnerable to subjectivity.
The present study found that an increase in animal calcium intake was associated with a decreased risk of VFO. The exact mechanisms by which calcium intake affects visceral fat accumulation are not fully understood. However, potential pathways may include the suppression of calcitriol levels, which reduces fat deposition [28], and enhancements in insulin sensitivity [29]. A previous study [30] demonstrated that elevated visceral fat is associated with lower calcium intake. While prior interventional studies have explored the combined effects of calcium and vitamin D3 intake on visceral fat [31], there remains a scarcity of human intervention studies focusing solely on the effects of calcium. Additionally, this study revealed that calcium intake, particularly from animal sources, was significantly lower in the VFO group compared to the SFO group. Given the link between bone mass reduction and menopause, the importance of calcium intake is particularly critical for middle-aged Korean women, whose consumption often falls below the recommended levels for their age [32].
Dyslipidemia was the most common comorbidity observed in this study, occurring twice as frequently in the VFO group compared to the SFO group. Additionally, T2DM was exclusively found in the VFO group. Abnormal mean values of triglycerides, TC, LDL-C, and FBG in the VFO group further supported the link between visceral fat and both dyslipidemia and T2DM. Interestingly, the mean BP values for both groups were within the normal range, despite a 16.9% prevalence of hypertension. This can be partly attributed to the high adherence rate (80.0%) to antihypertensive medication. In contrast, only 47.3% of those diagnosed with dyslipidemia adhered to their prescribed lipid-lowering medication regimen. This underscores the critical importance of medication adherence, which cannot be overstated.
Although regular exercise was not considered a factor influencing VFO, a significant difference was observed between the two groups. Women with SFO engaged in regular and more vigorous exercise compared to those with VFO. However, regardless of the type of obesity, middle-aged women with weight issues generally exhibited low PA levels. This aligns with a national report indicating that the adherence rate to aerobic PA among Korean women aged 40 to 59 is lower than that of Korean men in the same age group and their younger female counterparts [3]. Given that muscle mass and SFA were similar in the two groups, an effective exercise program for women with excessive weight or obesity should include strategies to increase muscle mass and reduce fat tissue in a manner that is feasible for them to maintain.
Regardless of the type of obesity, 41.6% of all participants were found to have a high sodium diet, consuming almost 1.5 times more than the recommended amount of 2300 mg [32]. Although sodium intake was not identified as a factor influencing VFO in this study, previous research has reported a significant correlation between urinary sodium output and VFA, as confirmed by abdominal CT [33]. Therefore, reducing sodium intake is advisable not only for women with hypertension but also for those with VFO. According to the analysis of a 3-day food diary, the daily proportions of protein, fat, and carbohydrate intake appeared to be adequate overall. However, the frequency of fat intake was high, as evidenced by more than two-thirds of the participants, regardless of obesity type. Given that significantly higher values of TC, LDL-C, and triglycerides in the VFO group were associated with animal fat intake, and considering the significantly lower intake of plant fats in the VFO group than in the SFO group, an increased intake of plant fats over animal fats is recommended for middle-aged women with VFO.
Women with VFO exhibited higher body weight, BMI, body fat percentage, VFA, and V/S ratio compared to those with SFO. Additionally, the VFO group displayed metabolic syndrome characterized by three abnormal factors: WC, triglycerides, and FBG. The mean values of BMI, WC, and VFA in each group were indicative of obesity and abdominal obesity, aligning with previous studies that demonstrated a correlational relationship between BMI, WC, and VFA [34]. Furthermore, the VFO group had significantly higher abnormal values of TC and LDL-C, suggesting a higher incidence of dyslipidemia in women with VFO. This aligns with earlier research highlighting the negative impact of VFO on cardiometabolic risk in women [5]. Additionally, the average hs-CRP level in the VFO group indicated a moderate risk, with the number of women at moderate or high risk being more than double that in the SFO group. This finding further supports the link between VFA and inflammation, which may increase the risk of CVD [6]. Moreover, the 10-year CVD risk estimate for the VFO group was significantly higher than that for the SFO group, corroborating the findings of Neeland et al. [35]. In summary, middle-aged women with VFO are at an increased risk for cardiometabolic disorders; therefore, it is crucial to manage their VFO comprehensively before the onset of menopause.
By incorporating the relevant factors identified from this study, lifestyle intervention programs can be designed to improve cardiometabolic health by reducing visceral fat. In particular, as vigorous PA has been shown to reduce visceral obesity, it is anticipated that targeted exercise programs emphasizing high-intensity activities can be developed. However, the reliability of these study results is compromised by the use of self-reported questionnaires to assess physical activity and dietary behaviors, which introduces the potential for recall bias and responder bias. Future research should employ objective measures, such as wearable devices, to obtain more accurate assessments of health behaviors. Additionally, as all participants were recruited from Seoul, Korea, the generalizability of the findings to women in other regions may be limited. Including participants from a variety of regions would improve the broader applicability of the findings. While this study concentrated on exercise and dietary habits, the omission of other lifestyle factors such as smoking and alcohol consumption is a limitation. This suggests a need for future studies to more comprehensively explore their impact on visceral fat and cardiometabolic risk.
This study demonstrated a positive association between VFO and cardiometabolic risk, identifying key factors influencing VFO in middle-aged women who are overweight. Significant differences were observed in body weight, BMI, WC, cholesterol profile, hs-CRP, and the 10-year estimate for CVD risk between the SFO group and the VFO group. Since abdominal fat gradually increases with age and with the onset of menopause, managing visceral fat is crucial for the health of middle-aged women. Although aging and menopause are inevitable, modifiable health behaviors such as healthy eating and regular PA should be closely monitored to reduce the accumulation of visceral fat. In conclusion, there is an urgent need for weight management programs that focus on reducing visceral fat accumulation in abdominal obesity among middle-aged women.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Conception and design of study - NS and JC.
Acquisition of data - SK.
Analysis and/or interpretation of data - SK and NS.
Drafting the manuscript - SK and NS.
Revising the manuscript critically for important intellectual content - NS and JC.
Approval of the version of the manuscript to be published (the names of all authors must be listed) - SK, NS, and JC.
This work was supported by the Korean Society of Adult Nursing and Korea University Institute of Nursing Research in 2018. The funding source had no involvement in study design, collection, analysis and interpretation of data, writing of the report or decision to submit the article for publication.
This article is a revision of the first author's master's thesis from Korea University.
 E-SUBMISSION
E-SUBMISSION