Abstract
-
Purpose
This systematic review and meta-analysis examined the effects of shared decision-making (SDM)-based self-management interventions on health outcomes in patients with chronic obstructive pulmonary disease (COPD).
-
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, three databases were searched in July 2022, supplemented by gray literature and citation searching. Randomized controlled trials that integrated SDM components into COPD self-management programs were included. Two reviewers independently performed study selection, data extraction, and risk-of-bias assessment. Random-effects models were used to pool odds ratios (ORs) for dichotomous outcomes and standardized mean differences (SMDs) for continuous outcomes, with 95% confidence intervals (CIs). Outcomes included hospital readmission, health-related quality of life (HRQoL), functionality, physical symptoms, psychological symptoms (depression and anxiety), and self-efficacy.
-
Results
Seven studies (n=1,028) met the inclusion criteria. SDM-based interventions showed no statistically significant difference in hospital readmission (OR=1.59, 95% CI, 0.79 to 3.19; I²=49.1%) and no significant improvement in HRQoL (SMD=0.19, 95% CI, –0.14 to 0.51; I²=98.3%). Depression showed no significant effect (SMD=–0.01, 95% CI, –0.39 to 0.38; I²=98.1%). Self-efficacy improved slightly (SMD=0.12, 95% CI, 0.01 to 0.23; I²=89.4%), with substantial heterogeneity. Evidence for other secondary outcomes was inconsistent.
-
Conclusion
SDM-based self-management interventions did not demonstrate clear benefits for hospital readmission or HRQoL in patients with COPD. Given the heterogeneity across studies, these findings should be interpreted cautiously. Future trials should use standardized SDM frameworks, assess implementation fidelity, and apply consistent outcome measures to clarify the role of SDM in COPD management.
-
Key Words: Chronic obstructive pulmonary disease; Self-management; Decision making, shared; Systematic review; Meta-analysis
INTRODUCTION
Overall disease burden is commonly measured using disability-adjusted life years (DALYs) [
1]. The Global Burden of Disease Study reported 212.3 million cases of chronic obstructive pulmonary disease (COPD) worldwide in 2019, resulting in 3.3 million deaths and 74.4 million DALYs. This burden is expected to increase because of population aging, smoking, air pollution, and occupational exposure [
2]. Self-management strategies are essential for reducing the disease burden because they improve symptom control and health-related quality of life (HRQoL) while reducing healthcare utilization and associated costs [
3]. According to the Global Initiative for Chronic Obstructive Lung Disease 2024 report [
4], COPD self-management includes patient education, individualized action plans, and consistent communication with healthcare professionals to enhance patients’ motivation, confidence, and competence in managing their condition. These interventions have been shown to improve HRQoL and reduce respiratory disease-related hospital admissions [
5,
6], ultimately promoting better long-term outcomes [
7].
Shared decision-making (SDM) is defined as a collaborative process in which clinicians and patients share the best available evidence, explore treatment or management options, and select strategies that reflect the patient’s values and preferences [
8]. When applied to chronic disease management, SDM promotes patient engagement, supports problem-solving skills, and facilitates the establishment of realistic self-management goals [
9,
10]. SDM-based self-management emphasizes the joint development of action plans, progress review, and goal adjustment throughout the self-management period [
11]. In COPD, SDM-based self-management interventions may be incorporated into the development and revision of individualized self-management plans through collaboration between patients and healthcare professionals [
11].
Several frameworks have described the essential components of SDM. For example, the Agency for Healthcare Research and Quality (AHRQ) proposed the SHARE (seek your patient’s participation [S], help your patient explore and compare treatment options [H], assess your patient’s values and preferences [A], reach a decision with the patient [R], and evaluate the patient’s decision [E]) approach, described later, as a structured process for implementing SDM [
12]. Legare and Witteman [
13] similarly emphasized three core elements: patient-provider involvement, bidirectional information exchange, and deliberation regarding treatment preferences. However, SDM-based self-management interventions in previous studies have varied considerably in the extent to which these components were applied. Many interventions incorporated only selected SDM steps, and outcomes were often measured indirectly through satisfaction, preferences, or self-efficacy rather than clinical indicators [
14]. Previous COPD self-management studies have primarily focused on hospital readmission and HRQoL as major health outcomes [
15], whereas secondary outcomes have included functionality, physical and psychological symptoms, and self-efficacy, which may mediate improvements in HRQoL and reductions in readmission [
16,
17]. With increasing attention to SDM in healthcare research, its direct impact on COPD outcomes requires further clarification.
Although SDM has been associated with beneficial effects in chronic disease management [
18,
19], evidence regarding its specific influence in patients with COPD remains limited and inconsistent. In the broader SDM literature, beneficial effects have been reported more consistently for affective-cognitive outcomes, whereas effects on behavioral and health outcomes are more variable and may depend on how SDM is measured [
19]. Consistent with this pattern, a systematic review of SDM interventions for chronic respiratory diseases reported substantial heterogeneity in the included studies and outcome measures, which precluded meta-analysis and limited the generalizability of the findings to COPD-specific contexts [
9]. Existing systematic reviews of COPD self-management have primarily synthesized multicomponent self-management programs, making it difficult to isolate SDM as a core mechanism [
6]. Given the variation in SDM applications, uncertainty regarding its effectiveness, and growing emphasis on patient-centered care, synthesis of the existing evidence is needed to determine the role and potential benefits of SDM in COPD self-management.
Therefore, this study conducted a systematic review and meta-analysis of randomized controlled trials (RCTs) to evaluate the effects of SDM-based self-management interventions on hospital readmission and HRQoL and to examine secondary outcomes, including functionality, physical and psychological symptoms, and self-efficacy, in patients with COPD.
METHODS
1. Study Design
This study was a systematic review and meta-analysis of RCTs. The protocol was registered in the Prospective Register of Systematic Reviews (PROSPERO; CRD42022366542). This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [
20].
A systematic search was conducted in July 2022 using three core databases—MEDLINE, Ovid-EMBASE, and the Cochrane Central Register of Controlled Trials (CENTRAL)—to identify studies available through July 2022. An additional search for unpublished studies, including gray literature such as dissertations, was conducted using ProQuest Dissertations & Theses Global and Google Scholar. Citation searching was also performed. The core terms COPD, self-management, and SDM were selected based on the review question. Medical Subject Headings (MeSH) and free-text terms were identified and tested in MEDLINE and CENTRAL during preliminary scoping to refine each core concept. A search strategy was then developed for each core concept. The strategy was tailored to each database, and terms were combined using Boolean operators and database-specific syntax, including selected truncation and wildcard terms. No restrictions were placed on publication period or language. All identified records were published in English; therefore, no studies were excluded on the basis of language. The full search strategy for each database is presented in
Supplementary Data 1. To contextualize the findings, guidelines and narrative reviews published after the final search date were cited for background only and were not used for study identification, eligibility assessment, or quantitative synthesis.
The review included studies of adults aged ≥40 years who had been diagnosed with COPD according to diagnostic criteria, as well as studies that included patients with COPD in the total cohort (population). The age threshold of 40 years was applied because COPD is most commonly diagnosed in middle-aged and older adults, and this cutoff is widely used in COPD case-finding and epidemiological research [
2,
4].
The intervention was defined as an SDM-based self-management program that included at least two elements of the SHARE model proposed by AHRQ [
12]. The SHARE steps include seeking the patient’s participation, helping the patient explore and compare management options, assessing the patient’s values and preferences, reaching a shared decision, and evaluating and revising the decision as needed. Interventions that applied two or more of these steps before or during development of the self-management plan were classified as SDM-based self-management interventions. The self-management intervention was required to include at least two self-management components, such as education, exercise, medication management, physical activity, or lifestyle modification. The control group was required to receive either usual care or self-management interventions without SDM.
The primary outcomes were HRQoL and hospital readmission rates. Secondary outcomes included general functionality, physical and psychological symptoms, and self-efficacy. Outcome selection was informed by the SDM consequences framework proposed by Elwyn et al. [
21], which distinguishes between proximal, distal, and distant consequences of collaborative deliberation. Accordingly, self-efficacy was prespecified as an SDM-relevant determinant aligned with distal consequences, and hospital readmission was designated as a downstream healthcare utilization endpoint aligned with distant consequences. HRQoL was included as a patient-centered health outcome that may change through sustained implementation of the individualized self-management plan developed through SDM [
3,
6,
7,
15-
17]. General functionality and physical and psychological symptoms were also included as patient-centered outcomes commonly assessed in COPD self-management and SDM-related respiratory interventions [
6,
7,
9,
17].
Only RCTs were included in the analysis. Studies using secondary or tertiary data, abstracts or protocol-only articles, and studies conducted primarily in palliative or end-of-life care settings were excluded. Palliative care-based interventions were excluded because their primary aims and core components, such as symptom palliation and advance care planning, differ from those of SDM-based self-management interventions; including them could have introduced substantial clinical heterogeneity in intervention intent and expected outcomes [
22].
However, one study involving patients with both COPD and congestive heart failure was not excluded because its results were partially obtained from patients with COPD. Furthermore, both diseases share common symptoms, such as shortness of breath and wheezing, which can result in reduced physical activity despite having different causes [
23].
After the search, all identified studies were uploaded to EndNote X8 8.2 (Clarivate Analytics, Philadelphia, PA, USA), and duplicates were removed. Two trained reviewers (SYY and SYL) independently screened titles and abstracts to identify potentially eligible studies. The full texts of potentially eligible articles were then assessed independently by the same reviewers. Disagreements were resolved through discussion and consultation with a third reviewer (JYC) when necessary; however, no disagreements required third-party adjudication.
Data were extracted using a structured, predesigned Excel form. Extracted data included general study characteristics, participant characteristics, intervention characteristics, self-management contents, SDM processes, and outcomes. The SDM process was analyzed using the SHARE approach developed by AHRQ [
12]. The SDM components implemented in each study were coded according to the five AHRQ SHARE steps based on the AHRQ factsheet [
12]. Two trained reviewers (SYY and SYL) independently coded the presence of each SHARE step for each included study based on intervention descriptions and supplementary materials, when available. Discrepancies in SHARE-step coding were resolved through discussion, and if consensus could not be reached, a third reviewer (JYC) was consulted; however, no unresolved discrepancies occurred.
When data were missing, the corresponding authors were contacted by e-mail to request relevant unpublished information. Because one study did not report the standard deviation for HRQoL, an e-mail was sent to the author to request statistical values; however, the data could not be obtained. Two trained reviewers (SYY and SYL) randomly selected two studies and conducted a pilot extraction test. Subsequently, one reviewer extracted general study data, and two reviewers independently coded the SHARE steps and reached agreement.
5. Quality Assessment
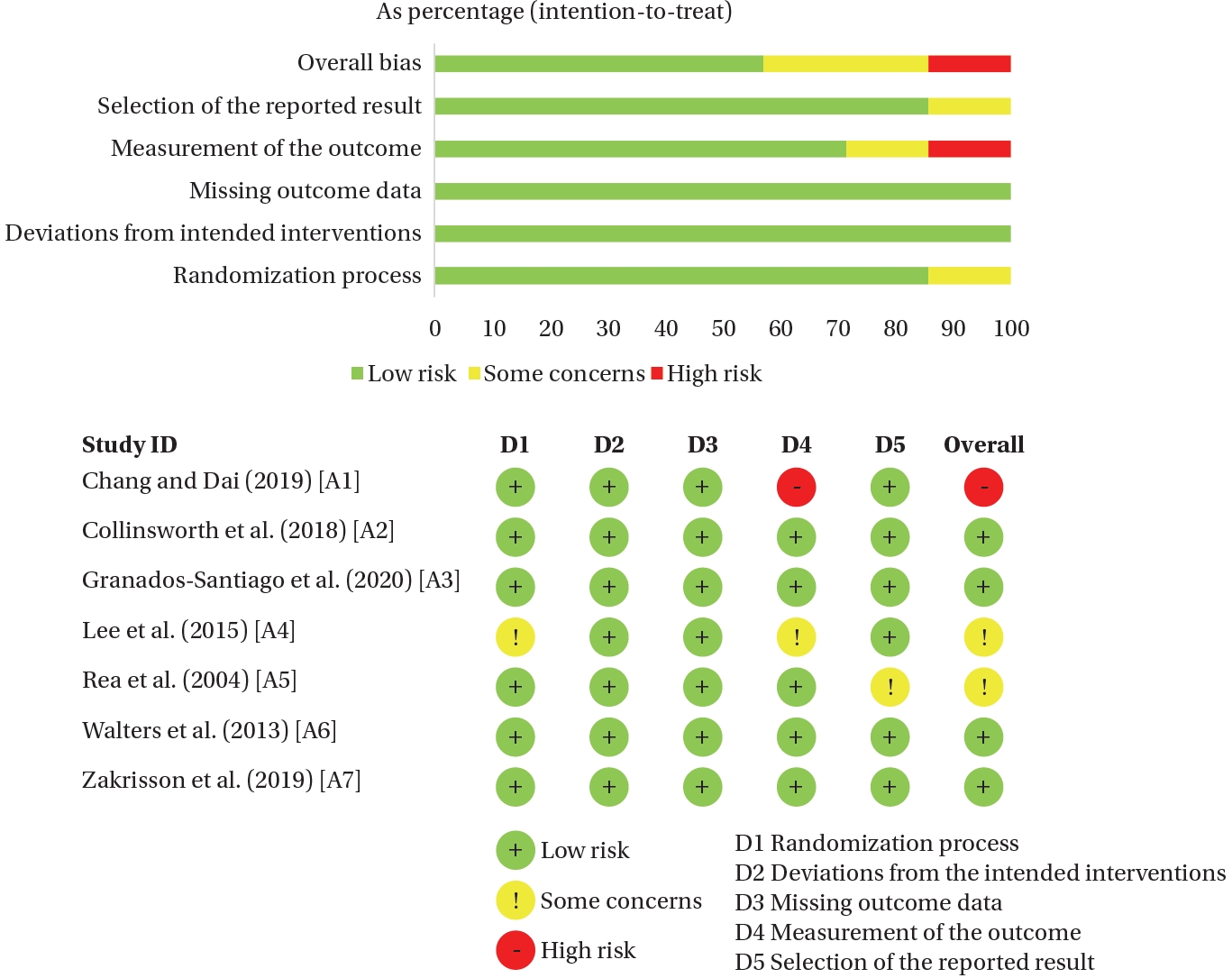
Literature quality was assessed using the Risk of Bias 2 tool (RoB 2) [
24]. The tool comprises five domains: bias arising from the randomization process, bias due to deviations from the intended interventions, bias due to missing outcome data, bias in outcome measurement, and bias in selection of the reported result. Two reviewers (SYY and SYL) independently assessed the RoB for each study. Consensus between the two reviewers was reached through discussion. A third reviewer (JYC) was consulted if consensus could not be achieved.
Effect size and heterogeneity analyses for hospital readmission, HRQoL, general functioning, physical symptoms, psychological symptoms, and self-efficacy were performed using Morris’s procedure [
25] for pretest-posttest control group designs, implemented in R with the “metafor” package [
26]. Meta-analysis was performed only when three or more studies were available for an outcome [
27]. When fewer than three studies were available, quantitative pooling was not conducted, and findings were summarized narratively; accordingly, general functioning, dyspnea, fatigue, and anxiety were not eligible for meta-analysis. A random-effects model was chosen to account for the inherent diversity of the studies because treatment effects were expected to differ across the selected studies beyond random sampling error.
Pooled effects are expressed as odds ratios (ORs) with 95% confidence intervals (CIs) for dichotomous outcomes. For continuous outcomes, standardized mean differences (SMDs) with 95% CIs were used when different instruments were applied [
27]. To align scale directions before computing SMDs, all continuous outcomes were oriented so that higher values consistently indicated improvement. For instruments in which higher scores reflected worse health status or symptoms, the sign of the effect estimate was reversed before standardization; standard deviations were not modified. When the posttest standard deviation was unavailable, it was replaced with the pretest standard deviation, and vice versa [
27]. When outcomes were reported at multiple follow-up time points within a study, data from the longest follow-up time point were extracted for meta-analysis. When a study included multiple outcomes for the same construct measured using different scales, a single weighted mean effect size was calculated for that study.
Heterogeneity among studies was assessed using forest plots, which allowed examination of overlap in CIs and variation in effect estimates. Heterogeneity among individual effect sizes was also assessed using Higgins’ I
2 [
28]. In this context, I² values of 25%, 50%, and ≥75% indicated low, moderate, and high heterogeneity, respectively. Given the small number of studies, the Hartung-Knapp adjustment with t-based inference was applied [
29]. No additional analyses, such as subgroup analyses, meta-regression, or sensitivity analyses, were conducted because the number of studies per outcome was insufficient. Given the small number of studies per outcome, a full GRADE (Grading of Recommendations Assessment, Development and Evaluation) Summary of Findings table was not produced; however, a brief outcome-level narrative assessment of certainty of evidence was conducted according to the GRADE domains [
27].
RESULTS
1. Study Identification and Selection
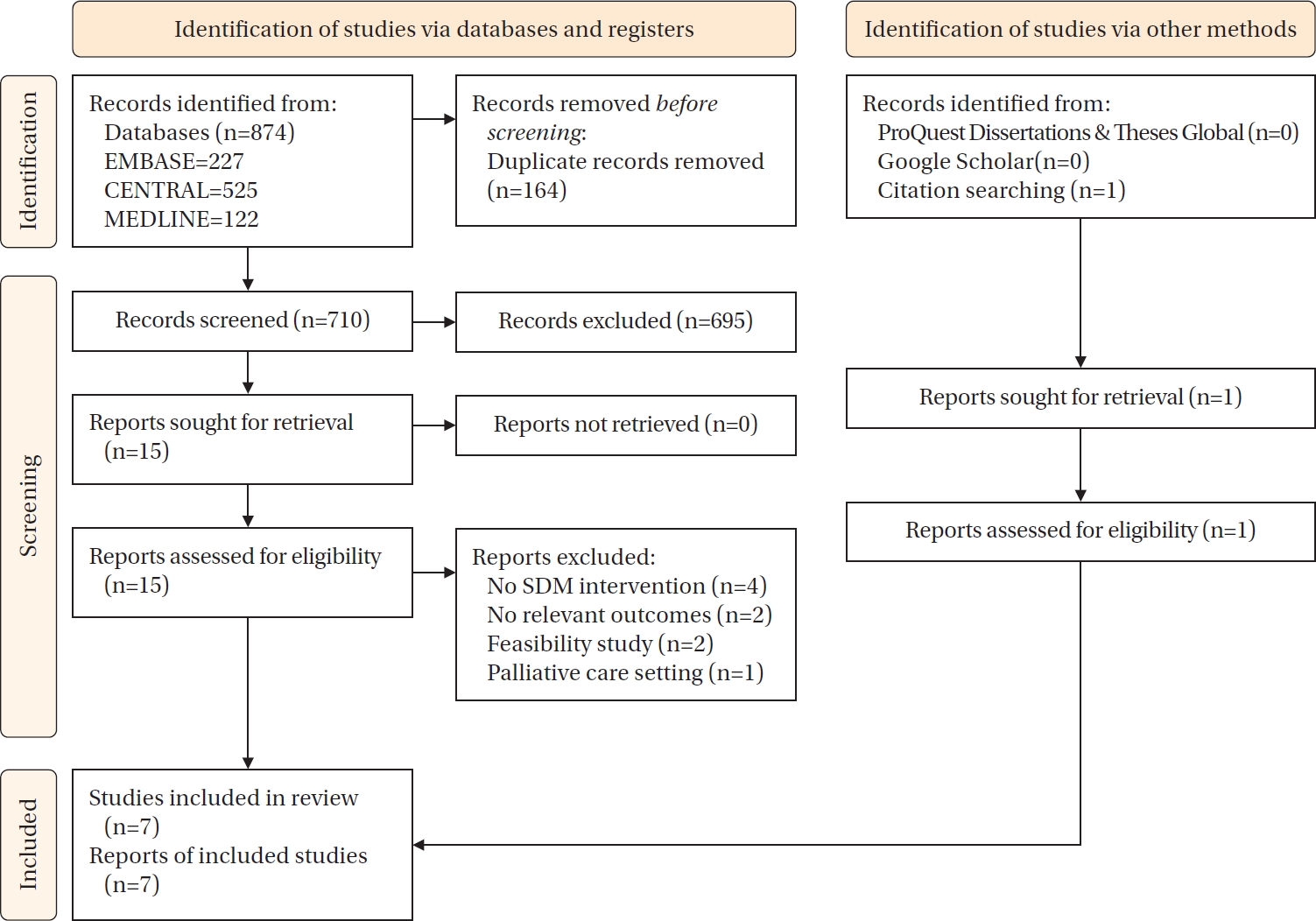
A total of 874 studies were identified through searches of the three databases, gray literature, and citation searching. After duplicates were removed and the titles and abstracts of 710 studies were reviewed, 695 studies were excluded based on the inclusion and exclusion criteria, leaving 15 studies for full-text review. After the full texts were reviewed, four studies were excluded because they did not apply SDM, two because they did not evaluate primary or secondary outcome variables, two because they focused on methodological feasibility, and one because it was conducted in a palliative care setting. Citation searching identified one additional study. Thus, seven studies were included in this systematic review and meta-analysis; the list is provided in
Supplementary Data 2.
Figure 1 shows the full study selection process using a PRISMA flow diagram.
Table 1 shows the characteristics of the selected studies [A1-7]. Regarding year of publication, four studies (57.1%) [A1-3,A7] were published between 2018 and 2022, two studies (28.6%) [A4,A6] were published between 2015 and 2013, respectively, and one study (14.3%) [A5] was published before 2013. The selected studies were conducted in Australia, New Zealand, South Korea, Spain, Sweden, Taiwan, and the United States.
The study settings were primary care institutions in three studies (42.8%) [A5-7], inpatient hospital settings in two studies (28.6%) [A2,A3], and outpatient hospital settings in two studies (28.6%) [A1,A4]. Six studies (85.7%) included only patients with COPD, and one study (14.3%) [A7] included patients with both COPD and congestive heart failure. The number of participants ranged from 42 to 308. The interventions included general COPD education and SDM support, as well as a flipped education program [A1], problem-solving counseling [A4], and health mentoring [A6]. The intervention period ranged from during hospitalization to 12 months. The self-management interventions included symptom management, medication adherence, diet, stress management, smoking cessation, lifestyle modification, exercise, and infection control.
3. Shared Decision-Making
Table 1 shows that none of the studies implemented all five SDM steps. Based on the SHARE approach, one study (14.3%) performed four steps [A3], and four studies (57.1%) performed three steps [A1,A2,A4,A7]. Step 1 involves encouraging patients to take an active role in decision-making, as implemented by Granados-Santiago et al. [A3], and creating a positive and supportive atmosphere to engage patients and their families in decision-making alongside the healthcare team, as demonstrated by Lee et al. [A4]. Step 2 focuses on presenting and explaining the options necessary for self-management strategies. Collinsworth et al. [A2] and Granados-Santiago et al. [A3] used these methods to support self-management strategies, whereas Chang and Dai [A1] and Rea et al. [A5] provided guidance and materials through booklets. Step 3 reflects patients’ preferences, interests, and priorities when determining self-management strategies, as implemented by Granados-Santiago et al. [A3]. Step 4 involved collaboratively setting COPD self-management action plans or goals and was applied in all studies [A1-7]. Finally, step 5 includes methods for checking patients’ self-management progress and, when necessary, revising self-management goals. This step was applied in six studies [A1,A2,A4-7].
4. Quality Assessment of the Selected Studies
Assessment using the Cochrane RoB 2 tool showed that four articles [A2,A3,A6,A7] had a low RoB. Two articles [A4,A5] had some concerns because of insufficient information on randomization and data collection or the absence of a prespecified analysis plan. One article [A1] had a high RoB because of lack of blinding and the potential for response bias from self-reported surveys (
Figure 2).
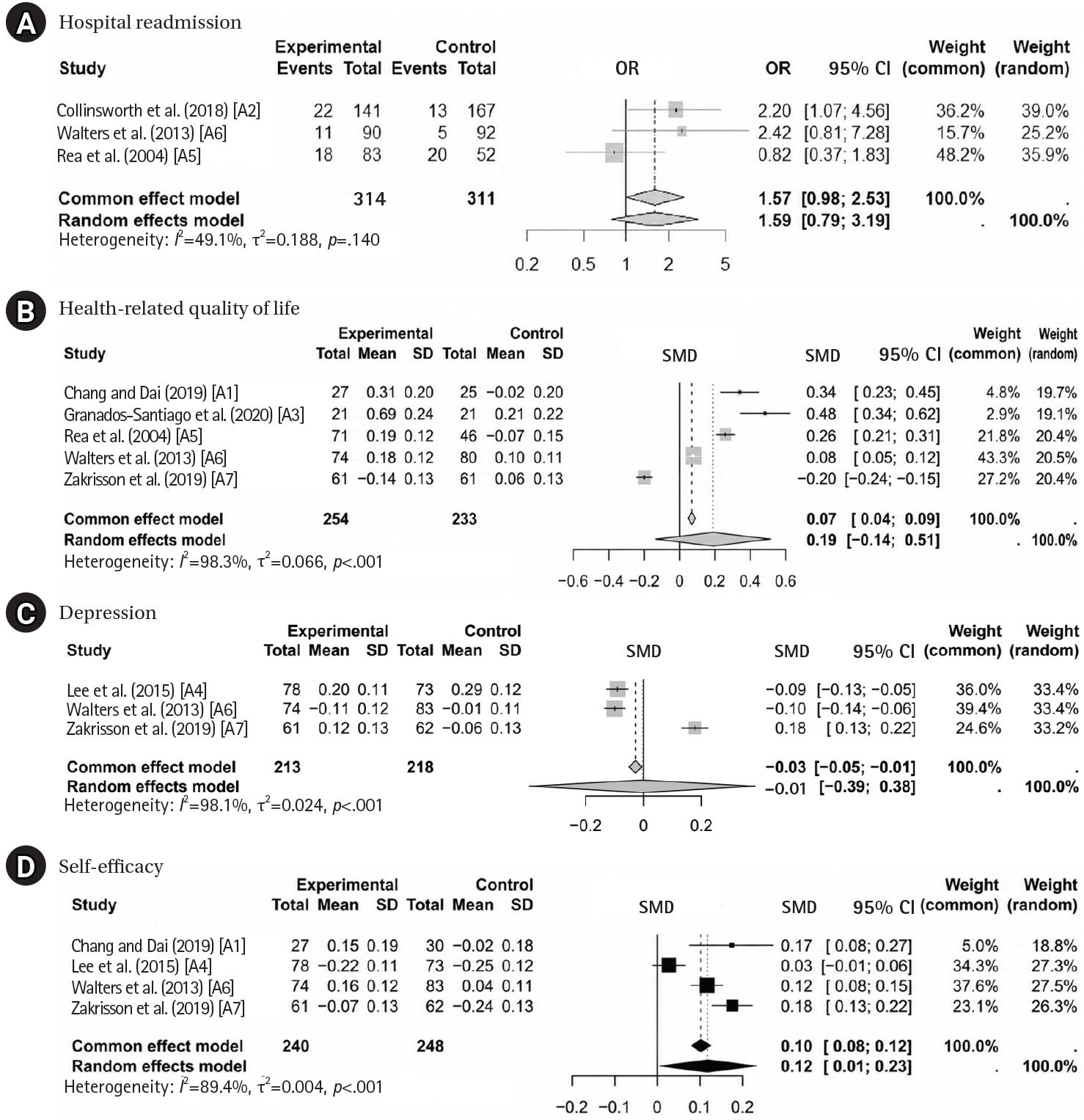
1) Primary outcomes
Three studies reported hospital readmissions (
Figure 3A). The pooled results (n=625) showed no statistically significant difference in hospital readmission between SDM-based interventions and controls (OR=1.59, 95% CI, 0.79 to 3.19;
p=.318), with moderate heterogeneity (I²=49.1%,
p=.140). Five studies (n=487) examined the effect of SDM on HRQoL using the COPD Assessment Test, EuroQol 5-Dimension, 36-Item Short Form Survey, and St. George’s Respiratory Questionnaire (
Figure 3B). The pooled results indicated no significant improvement in HRQoL (SMD=0.19, 95% CI, –0.14 to 0.51;
p=.184), with very high heterogeneity (I²=98.3%, Q=242.20, degrees of freedom [df]=4;
p<.001) (
Table 2).
2) Secondary outcomes
Depression was assessed in three studies using the Center for Epidemiologic Studies Depression Scale and Hospital Anxiety and Depression Scale (
Figure 3C). The pooled estimate showed no significant effect on depression (SMD=–0.01, 95% CI, –0.39 to 0.38;
p=.962), with considerable heterogeneity (I²=98.1%, Q=105.15, df=2;
p<.001) (
Table 2).
Self-efficacy was measured using the Coping Self-Efficacy Scale, Exercise Self-Efficacy Scale, Pulmonary Rehabilitation Adapted Index of Self-Efficacy, and Self-Efficacy to Manage Chronic Diseases. The pooled estimate showed a small but statistically significant positive effect of SDM-based interventions on self-efficacy (SMD=0.12, 95% CI, 0.01 to 0.23;
p=.043), with high heterogeneity (I²=89.4%, Q=28.31, df=3;
p<.001) (
Table 2,
Figure 3D).
General functioning showed mixed findings in two studies [A3,A7]. Regarding physical symptoms, dyspnea improved in one study [A3], whereas fatigue showed no significant between-group difference in another study [A7]. Anxiety outcomes were also inconsistent across the two studies that reported this outcome [A6,A7].
6. Certainty of Evidence (GRADE-Informed Narrative Assessment)
A GRADE-informed narrative assessment of certainty was conducted for each outcome. Because the number of included trials per outcome was small and reporting was limited, a formal Summary of Findings table was not produced; instead, certainty was rated narratively across key GRADE domains, including RoB, inconsistency, indirectness, and imprecision [
27], where assessment was feasible. Overall certainty ranged from moderate to very low.
For hospital readmission (3 studies; OR=1.59, 95% CI, 0.79 to 3.19; I²=49.1%), certainty was rated as moderate and was downgraded by one level for imprecision because of wide CIs spanning potential benefit and harm. For HRQoL (5 studies; SMD=0.19, 95% CI, –0.14 to 0.51; I²=98.3%), certainty was rated as very low and was downgraded for very serious inconsistency and imprecision. For depression (3 studies; SMD=–0.01, 95% CI, –0.39 to 0.38; I²=98.1%), certainty was rated as very low and was downgraded for very serious inconsistency and imprecision. For self-efficacy (4 studies; SMD=0.12, 95% CI, 0.01 to 0.23; I²=89.4%), certainty was rated as low and was downgraded for serious inconsistency and imprecision because of substantial heterogeneity and variability in effect estimates across trials.
DISCUSSION
This systematic review and meta-analysis evaluated the effects of SDM-based self-management programs on hospital readmission and HRQoL in patients with COPD. Seven studies with a combined sample size of 1,028 participants were included. The pooled estimates did not show statistically significant differences in hospital readmission or HRQoL; moreover, confidence in these findings was limited by substantial between-study heterogeneity and the small number of included trials. Among secondary outcomes, SDM-based self-management was associated with a small pooled improvement in self-efficacy, whereas no statistically significant difference was observed for depression. A GRADE-informed narrative appraisal suggested moderate to very low certainty across outcomes; thus, both the pooled improvement in self-efficacy and the nonsignificant findings for clinical outcomes should be interpreted as uncertain and subject to change as new evidence emerges.
Self-efficacy is a common proximal target of COPD self-management interventions. Prior reviews suggest that self-management programs may improve HRQoL and reduce respiratory-related hospital admissions, although effects vary across intervention components and follow-up periods [
6,
15]. In this review, SDM-integrated self-management was associated with a small improvement in self-efficacy but no statistically significant differences in hospital readmission or HRQoL. This pattern is consistent with the SDM literature, which indicates more consistent effects on affective-cognitive outcomes than on distal clinical endpoints [
19]. One plausible explanation is that SDM strengthens self-efficacy by increasing perceived involvement and autonomy and by supporting behavior change through collaborative goal setting, action planning, and follow-up feedback. These mechanisms are consistent with self-efficacy theory, which emphasizes mastery experiences and verbal persuasion as key sources of efficacy beliefs [
30,
31]. Future trials should test whether self-efficacy mediates downstream behavioral changes and clinical outcomes in SDM-based COPD self-management.
In the broader context of chronic respiratory disease, Barradell et al. [
9] identified eight SDM intervention studies and reported that outcomes were heterogeneous and inconsistently measured across trials, limiting confidence in downstream clinical effects. Although the included studies generally reported improvements in patient decision-making and health-related outcomes, the overall certainty of evidence was limited because of heterogeneity and RoB, and only a subset of interventions addressed patient-, clinician-, and consultation-level components in an integrated manner [
9]. Taken together, these findings suggest that downstream clinical effects may be difficult to detect without standardized SDM components and harmonized outcome assessments. This interpretation is consistent with the variability in SDM delivery observed across the included COPD studies, including differences in providers, delivery modes, and intervention duration.
Compared with prior COPD self-management meta-analyses, which primarily evaluated self-management irrespective of explicit SDM components and emphasized hospitalization rates and HRQoL as key outcomes [
6,
32], this review specifically examined self-management programs that incorporated SDM and assessed SDM implementation using the SHARE framework [
12]. The SHARE-based analysis showed that implementation across the included studies was partial and inconsistent; most interventions emphasized later SHARE steps, such as goal setting and follow-up, whereas systematic assessment of patient values or structured presentation of management options in earlier SHARE steps was seldom reported. This pattern likely reflects the challenge of fully applying all SHARE steps within structured intervention trials, in which detailed patient-provider interactions are not always captured. Accordingly, future trials should treat early SHARE steps, including structured presentation of management options and systematic elicitation of patient values and preferences, as required components and should verify fidelity to prespecified SDM components [
12,
33]. These findings suggest that the lack of clear effects of SDM on clinical outcomes may reflect insufficient integration of essential SDM components within the programs. Given that early SHARE steps were inconsistently implemented, proximal gains may partly reflect later-stage coaching elements, such as goal setting and follow-up, rather than full-spectrum SDM.
Potential sources of heterogeneity should therefore be considered. A key contributor was variability in how outcomes were measured across trials, as several constructs were assessed using different instruments with nonidentical content and responsiveness to change [
27]. For example, some studies used both disease-specific and generic instruments to assess patient-reported outcomes, including HRQoL, and some also included a measure of global life satisfaction. Because measurement nonequivalence can inflate between-study variability and limit interpretability, pooled estimates should be interpreted cautiously, with greater emphasis placed on the direction and consistency of effects across individual trials [
27]. In addition, differences in follow-up timing, populations, intervention intensity, and SDM implementation likely contributed to heterogeneity. Given the small number of studies per outcome, subgroup analyses and meta-regression were not feasible [
27]. Future trials should improve comparability by prespecifying primary instruments for key outcomes, harmonizing outcome definitions, and standardizing assessment time points.
In the final selection of seven studies, quality assessment revealed deficiencies in several areas. Nonblinded outcome assessments and unclear reporting of allocation concealment raised concerns about potential bias, particularly for self-reported outcomes such as self-efficacy and psychological symptoms. Moreover, some studies lacked information on protocol registration or institutional review board approval. Future trials should strengthen randomization procedures; clearly report sequence generation and allocation concealment in accordance with CONSORT guidance [
34]; blind outcome assessors whenever possible; and prioritize objective outcome sources, such as hospitalization records or administrative data, to minimize bias in outcome measurement, as emphasized in contemporary RoB guidance for randomized trials [
24]. Improving overall study quality through comprehensive documentation of study design and approval processes will contribute to more robust and reliable findings.
This study had several limitations. First, research on SDM in the context of self-management programs for patients with COPD remains in its early stages, resulting in a limited evidence base. Second, one study measured the same construct using multiple instruments. Although these measures were combined into a single weighted mean effect size where feasible, differences in instrument content and responsiveness may have limited comparability. Third, substantial heterogeneity across outcomes likely reflected differences in follow-up duration, intervention delivery, and the extent to which core SDM components were implemented. In addition, incomplete statistical reporting in one study restricted data synthesis. The literature search was conducted in July 2022; therefore, more recent studies may not have been captured. Because few studies were available per outcome, funnel plots and related tests were not performed, and small-study effects, including publication bias, could not be assessed [
27].
CONCLUSION
This systematic review and meta-analysis of seven RCTs assessed the effects of SDM-based self-management interventions on primary and secondary outcomes in patients with COPD. The pooled estimates showed no statistically significant differences in hospital readmission or HRQoL, whereas SDM-based self-management was associated with a small pooled improvement in self-efficacy. However, these findings should be interpreted cautiously given the substantial heterogeneity, small number of trials, and moderate to very low certainty of evidence. Future studies should strengthen the rigor of trial design and reporting, standardize outcome assessments, and ensure high-fidelity SDM delivery with consistent implementation and verification of the core SHARE steps.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and/or design acquisition - JYC; analysis - SYL and SYY; interpretation of the data - SYL and SYY; and drafting or critical revision of the manuscript for important intellectual content - JYC and SYY.
-
FUNDING
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (Grant Number NRF-2022R1A2C1010364).
-
ACKNOWLEDGEMENT
None.
-
DATA AVAILABILITY STATEMENT
The data can be obtained from the corresponding authors.
SUPPLEMENTARY MATERIAL
Figure 1.Flow diagram of the study selection process. SDM=shared decision-making.
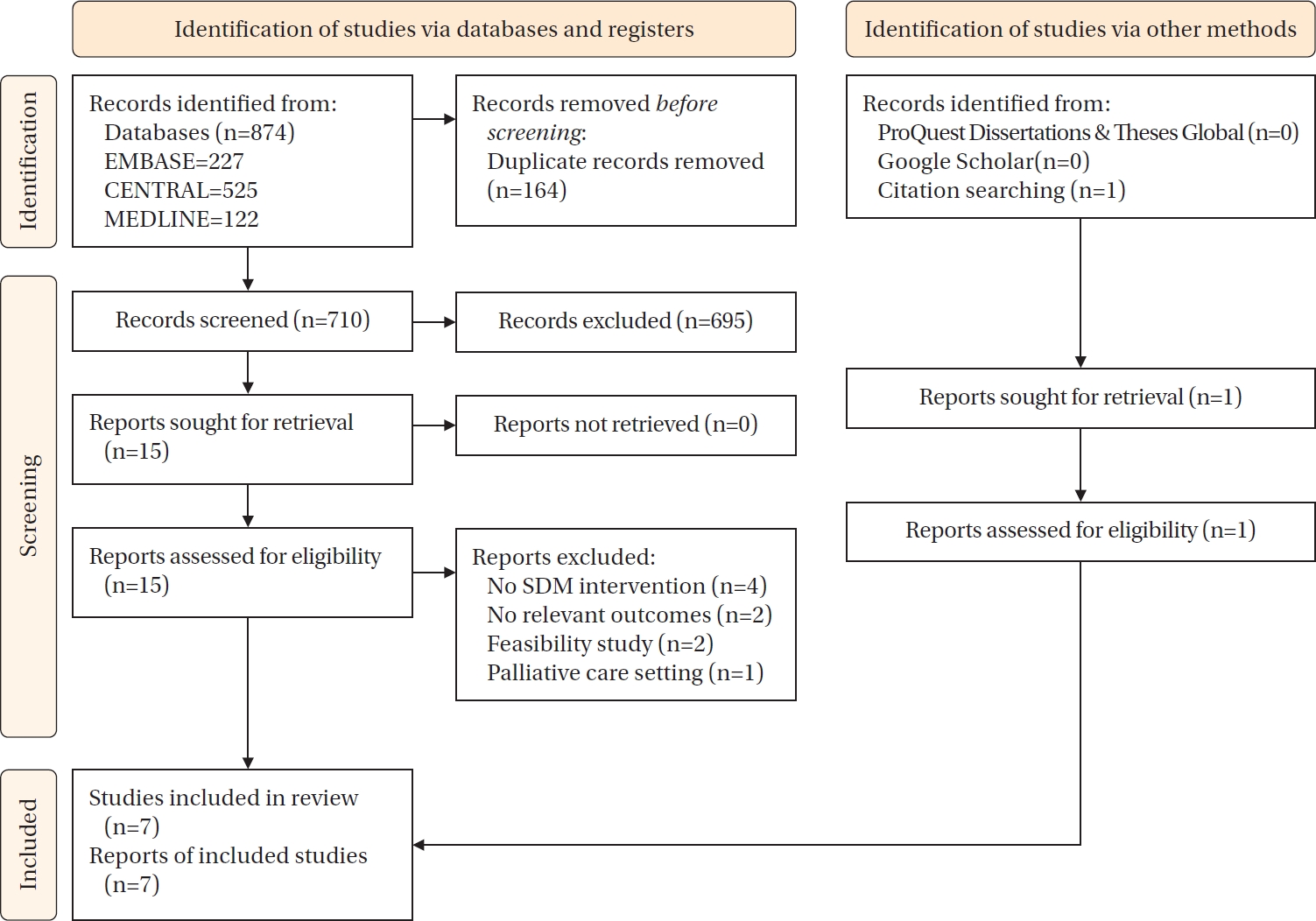
Figure 2.Assessment of the risk of bias in the included studies.
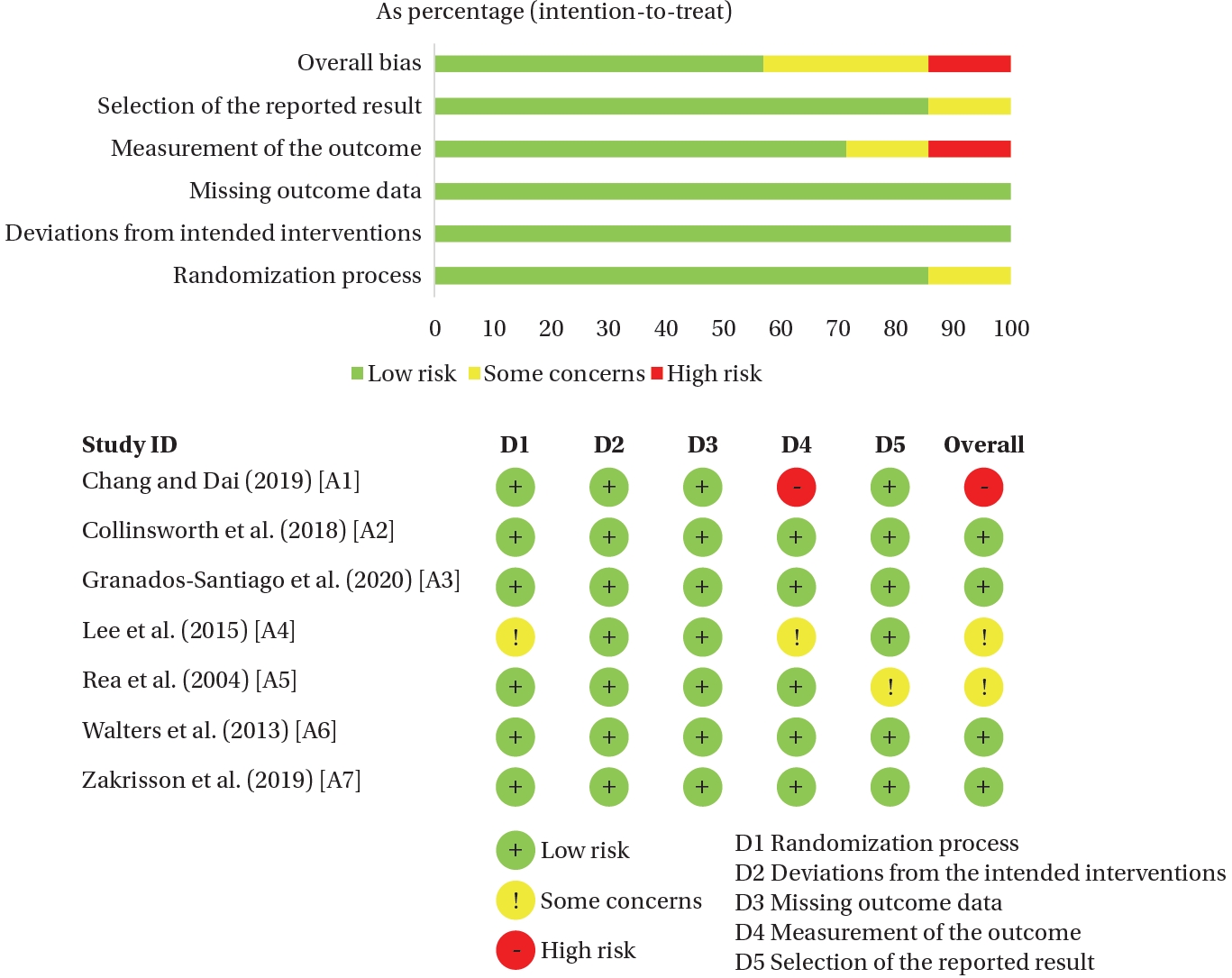
Figure 3.Forest plots of the effects of shared decision-making (SDM)-based self-management interventions. (A) For measuring hospital readmission, the number of readmitted participants in each group was used. (B) For measuring health-related quality of life, COPD Assessment Test was used in A1, EuroQol 5-Dimension was used in A3, the 36-Item Short Form Survey was used in A5, A6, and A7; Chronic Respiratory Disease Questionnaire was used in A5, and St. George’s Respiratory Questionnaire and Satisfaction with Life Scale were used in A6. (C) For measuring depression, the Center for Epidemiologic Studies Depression was used in A4 and A6, and the depression subscale of the Hospital Anxiety and Depression Scale was used in A6 and A7. (D) For measuring self-efficacy, the Pulmonary Rehabilitation Adapted Index of self-efficacy was used in A1, the Coping Self-Efficacy Scale was used in A4, the Self-Efficacy to Manage Chronic Disease in A6, and the Exercise Self-Efficacy Scale was used in A7. CI=confidence interval; OR=odds ratio; SD=standard deviation; SMD=standardized mean difference.
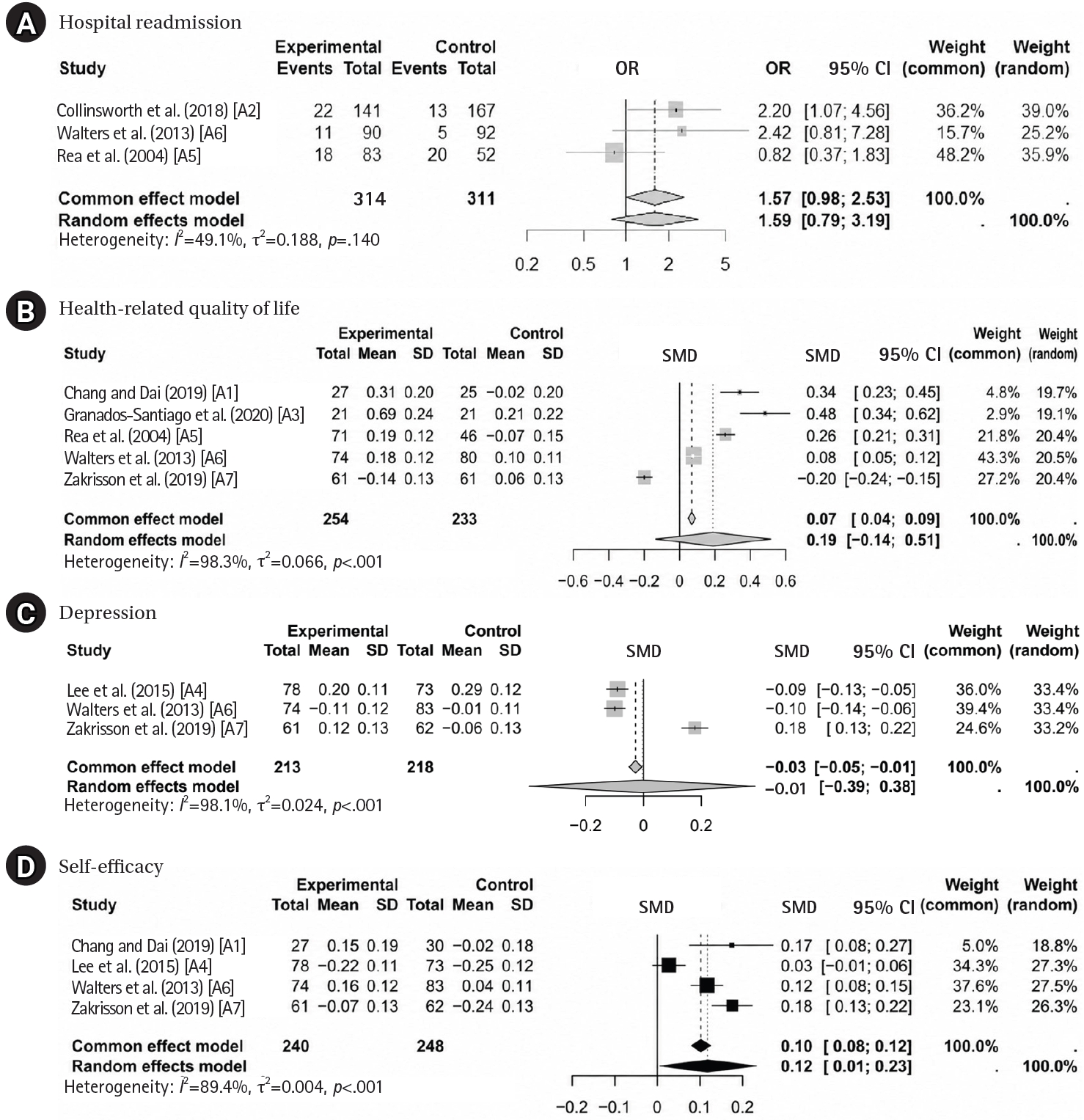
Table 1.Characteristics of the Included Studies (N=7)
|
No. |
Author (year) |
Country |
Setting |
Provider |
Participants |
Intervention |
Intervention period |
Control |
Self-management contents |
SDM process (SHARE) |
Outcomes (tools) |
|
A1 |
Chang and Dai (2019) |
Taiwan |
A medical center |
A nurse manager |
Patients with clinical COPD diagnosis established using the pulmonary function test (FEV1/FVC <0.7), aged >20 years (60, I=30 vs. C=30) |
Motivating, self-learning, reflecting, action-plan verbalizing, and action-taking (MSRAA) flipped self-management education program |
3 Months |
Conventional patient education |
- Pursed-lip breathing |
H |
- HRQoL (CAT) |
|
- Smoking cessation |
R |
- Self-efficacy (PRAISE) |
|
- Adopting environmental control measures |
E |
|
|
- Preventing respiratory tract infections |
|
|
|
- Taking medications regularly |
|
|
|
- Exercising regularly |
|
|
|
A2 |
Collinsworth et al. (2018) |
USA |
A community hospital |
Registered respiratory therapists |
COPD patients at least 24 hours after admission (308, I=141 vs. C=167) |
COPD education, SDM-based self-management planning, and follow-up telephone calls |
6 Months |
COPD education |
- Symptom management |
H |
- Hospital readmissions
|
|
- Medication management |
R |
- HRQoL (CAT) |
|
- Diet and nutrition |
E |
|
|
- Stress and coping |
|
|
|
- Smoking cessation |
|
|
|
- Physical activity |
|
|
|
A3 |
Granados-Santiago et al. (2020) |
Spain |
2 Hospitals |
NA |
Patients hospitalized due to AECOPD (42, I=21 vs. C=21) |
Individualized SDM and patient engagement programs added to standard treatment |
Hospitalization days |
Standard treatment |
-Pharmacological management |
S |
- HRQoL (EQ-5D) |
|
- Symptom control |
H |
- General functionality (FIM) |
|
- Healthy lifestyle promotion |
A |
- Physical symptoms (Borg scale) |
|
R |
|
|
A4 |
Lee et al. (2015) |
South Korea |
3 Outpatient clinics at 1 university hospital |
A registered nurse |
COPD patients aged 40–80 years in stable condition and expected to live ≥6 months (151, I=78 vs. C=73) |
Problem-solving counseling |
6 Months |
Usual care |
- Assessment of severity and managing exacerbation |
H |
- Psychological symptoms (CES-D) |
|
- Medication |
R |
- Self-efficacy (CSES) |
|
- Managing respiratory symptoms |
E |
|
|
- Oxygen therapy |
|
|
|
- Exercise |
|
|
|
- Nutrition |
|
|
|
- Stress management |
|
|
|
- Smoking cessation |
|
|
|
- Sleep |
|
|
|
- Infection |
|
|
|
- Immunization |
|
|
|
A5 |
Rea et al. (2004) |
New Zealand |
66 GP practices |
Participant’s GP and practice nurse |
Patients with moderate to severe COPD (135, I=83 vs. C=52) |
Care plans with predetermined goals, action plans, and education on COPD management |
12 Months |
Conventional care |
- Action plan |
R |
- Hospital admissions |
|
- Smoking cessation |
E |
- HRQoL (SF-36 and CRQ) |
|
- Medication and use of inhalers |
|
|
|
- Influenza vaccination |
|
|
|
- Participation in pulmonary rehabilitation |
|
|
|
A6 |
Walters et al. (2013) |
Australia |
31 General practices |
Community health nurses |
Patients aged >45 years with COPD, smoking history >10 pack-years, FEV1/FVC <0.7, and predicted FEV1 of 30%–80% after bronchodilatation (182, I=90 vs. C=92) |
Psychoeducation, self-management skills training, cognitive coping-skills training, communication-skills training, and promotion of self-efficacy |
12 Months |
Usual care plus monthly phone calls |
- Smoking cessation |
R |
- Hospital admission |
|
- Nutrition and alcohol |
E |
- HRQoL (SF-36, SGRQ, and SWLS) |
|
- Physical activity |
|
- Psychological symptoms (CES-D and HAD) |
|
- Psychosocial well-being |
|
- Self-efficacy (SEMCD) |
|
- Symptom management |
|
|
|
A7 |
Zakrisson et al. (2019) |
Sweden |
9 PHC centers |
A physiotherapist and a nurse |
Physician‐diagnosed congestive heart failure or spirometry‐verified diagnosis of COPD (FEV1/FVC <0.70 and predicted FEV1 <80% after bronchodilatation) as well as any symptoms (150, I=73 vs. C=77) |
Individualized action plans, goal-setting discussions, and support for patients to develop self-management skills and disease-related knowledge |
3 Months |
Usual care |
- Individualized action plans |
S |
- HRQoL (SF-36) |
|
- Supporting the patients to practice skills and gain knowledge |
R |
- General functionality (COPM) |
|
E |
- Physical symptoms (FIS-physical) |
|
|
- Psychological symptoms (HADS) |
|
|
- Self-efficacy (ESES) |
Table 2.Random-Effects Meta-Analysis of Shared Decision-Making between Pretest and Posttest
|
Variables |
k |
No. |
Q |
df |
p-value |
I2 (%) |
Effect size |
t |
p-value |
|
OR or SMD (95% CI) |
|
Primary outcomes |
|
|
|
|
|
|
|
|
|
|
Hospital readmission |
3 |
625 |
3.93 |
2 |
.140 |
49.1 |
1.59 (0.79 to 3.19) |
1.32 |
.318 |
|
HRQoL |
5 |
487 |
242.20 |
4 |
<.001 |
98.3 |
0.19 (−0.14 to 0.51) |
1.60 |
.184 |
|
Secondary outcomes |
|
|
|
|
|
|
|
|
|
|
Depression |
3 |
431 |
105.15 |
2 |
<.001 |
98.1 |
−0.01 (−0.39 to 0.38) |
−0.05 |
.962 |
|
Self-efficacy |
4 |
488 |
28.31 |
3 |
<.001 |
89.4 |
0.12 (0.01 to 0.23) |
3.37 |
.043 |
REFERENCES
- 1. World Health Organization (WHO). WHO methods and data sources for global burden of disease estimates 2000-2019 [Internet]. Geneva: World Health Organization; 2020 [cited 2023 December 3]. Available from: https://cdn.who.int/media/docs/default-source/gho-documents/global-health-estimates/ghe2019_daly-methods.pdf?sfvrsn=31b25009_7
- 2. Safiri S, Carson-Chahhoud K, Noori M, Nejadghaderi SA, Sullman MJ, Ahmadian Heris J, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990-2019: results from the global burden of disease study 2019. BMJ. 2022;378:e069679. https://doi.org/10.1136/bmj-2021-069679
- 3. Song X, Hallensleben C, Zhang W, Jiang Z, Shen H, Gobbens RJ, et al. Blended self-management interventions to reduce disease burden in patients with chronic obstructive pulmonary disease and asthma: systematic review and meta-analysis. J Med Internet Res. 2021;23(3):e24602. https://doi.org/10.2196/24602
- 4. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2024 report) [Internet]. Fontana, WI: Global Initiative for Chronic Obstructive Lung Disease; 2024 [cited 2024 May 25]. Available from: https://goldcopd.org/2024-gold-report/
- 5. Majothi S, Jolly K, Heneghan NR, Price MJ, Riley RD, Turner AM, et al. Supported self-management for patients with COPD who have recently been discharged from hospital: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10:853-67. https://doi.org/10.2147/COPD.S74162
- 6. Schrijver J, Lenferink A, Brusse-Keizer M, Zwerink M, van der Valk PD, van der Palen J, et al. Self-management interventions for people with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2022;1(1):CD002990. https://doi.org/10.1002/14651858.CD002990.pub4
- 7. Janjua S, Banchoff E, Threapleton CJ, Prigmore S, Fletcher J, Disler RT. Digital interventions for the management of chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2021;4(4):CD013246. https://doi.org/10.1002/14651858.CD013246.pub2
- 8. Elwyn G, Frosch D, Thomson R, Joseph-Williams N, Lloyd A, Kinnersley P, et al. Shared decision making: a model for clinical practice. J Gen Intern Med. 2012;27(10):1361-7. https://doi.org/10.1007/s11606-012-2077-6
- 9. Barradell AC, Gerlis C, Houchen-Wolloff L, Bekker HL, Robertson N, Singh SJ. Systematic review of shared decision-making interventions for people living with chronic respiratory diseases. BMJ Open. 2023;13(5):e069461. https://doi.org/10.1136/bmjopen-2022-069461
- 10. Lewis-Barned N. Shared decision making and support for self-management: a rationale for change. Future Hosp J. 2016;3(2):117-20. https://doi.org/10.7861/futurehosp.3-2-117
- 11. Bodenheimer T, Handley MA. Goal-setting for behavior change in primary care: an exploration and status report. Patient Educ Couns. 2009;76(2):174-80. https://doi.org/10.1016/j.pec.2009.06.001
- 12. Agency for Healthcare Research and Quality. The SHARE approach: a model for shared decision making - fact sheet [Internet]. Rockville, MD: Agency for Healthcare Research and Quality; 2020 [cited 2022 May 3]. Available from: https://www.ahrq.gov/health-literacy/professional-training/shareddecision/tools/factsheet.html
- 13. Legare F, Witteman HO. Shared decision making: examining key elements and barriers to adoption into routine clinical practice. Health Aff (Millwood). 2013;32(2):276-84. https://doi.org/10.1377/hlthaff.2012.1078
- 14. Lu Y, Elwyn G, Moulton BW, Volk RJ, Frosch DL, Spatz ES. Shared decision-making in the U.S.: evidence exists, but implementation science must now inform policy for real change to occur. Z Evid Fortbild Qual Gesundhwes. 2022;171:144-9. https://doi.org/10.1016/j.zefq.2022.04.031
- 15. Newham JJ, Presseau J, Heslop-Marshall K, Russell S, Ogunbayo OJ, Netts P, et al. Features of self-management interventions for people with COPD associated with improved health-related quality of life and reduced emergency department visits: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:1705-20. https://doi.org/10.2147/COPD.S133317
- 16. Benzo RP, Abascal-Bolado B, Dulohery MM. Self-management and quality of life in chronic obstructive pulmonary disease (COPD): the mediating effects of positive affect. Patient Educ Couns. 2016;99(4):617-23. https://doi.org/10.1016/j.pec.2015.10.031
- 17. Jolly K, Sidhu MS, Bates E, Majothi S, Sitch A, Bayliss S, et al. Systematic review of the effectiveness of community-based self-management interventions among primary care COPD patients. NPJ Prim Care Respir Med. 2018;28(1):44. https://doi.org/10.1038/s41533-018-0111-9
- 18. Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008;77(4):219-26. https://doi.org/10.1159/000126073
- 19. Shay LA, Lafata JE. Where is the evidence?: a systematic review of shared decision making and patient outcomes. Med Decis Making. 2015;35(1):114-31. https://doi.org/10.1177/0272989X14551638
- 20. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. https://doi.org/10.1136/bmj.n71
- 21. Elwyn G, Frosch DL, Kobrin S. Implementing shared decision-making: consider all the consequences. Implement Sci. 2016;11:114. https://doi.org/10.1186/s13012-016-0480-9
- 22. Janssen DJA, Bajwah S, Boon MH, Coleman C, Currow DC, Devillers A, et al. European Respiratory Society clinical practice guideline: palliative care for people with COPD or interstitial lung disease. Eur Respir J. 2023;62(2):2202014. https://doi.org/10.1183/13993003.02014-2022
- 23. Khalid K, Padda J, Komissarov A, Colaco LB, Padda S, Khan AS, et al. The coexistence of chronic obstructive pulmonary disease and heart failure. Cureus. 2021;13(8):e17387. https://doi.org/10.7759/cureus.17387
- 24. Sterne JA, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. https://doi.org/10.1136/bmj.l4898
- 25. Morris SB. Estimating effect sizes from pretest-posttest-control group designs. Organ Res Methods. 2008;11(2):364-86. https://doi.org/10.1177/1094428106291059
- 26. Viechtbauer W. Conducting meta-analyses in R with the metafor package. J Stat Softw. 2010;36(3):1-48. https://doi.org/10.18637/jss.v036.i03
- 27. Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. 2nd ed. Chichester: John Wiley & Sons; 2019.
- 28. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-60. https://doi.org/10.1136/bmj.327.7414.557
- 29. Hartung J, Knapp G. A refined method for the meta-analysis of controlled clinical trials with binary outcome. Stat Med. 2001;20(24):3875-89. https://doi.org/10.1002/sim.1009
- 30. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191-215. https://doi.org/10.1037//0033-295x.84.2.191
- 31. Bourbeau J, Nault D, Dang-Tan T. Self-management and behaviour modification in COPD. Patient Educ Couns. 2004;52(3):271-7. https://doi.org/10.1016/S0738-3991(03)00102-2
- 32. Zwerink M, Brusse-Keizer M, van der Valk PD, Zielhuis GA, Monninkhof EM, van der Palen J, et al. Self-management for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2014;2014(3):CD002990. https://doi.org/10.1002/14651858.CD002990.pub3
- 33. Borrelli B. The assessment, monitoring, and enhancement of treatment fidelity in public health clinical trials. J Public Health Dent. 2011;71(s1):S52-S63. https://doi.org/10.1111/j.1752-7325.2011.00233.x
- 34. Schulz KF, Altman DG, Moher D; CONSORT Group. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. https://doi.org/10.1136/bmj.c332


 E-SUBMISSION
E-SUBMISSION
