
Purpose
This study was conducted to develop a conceptual framework for understanding non-adherence to self-management among patients with Chronic Obstructive Pulmonary Disease (COPD). This was accomplished through a literature review, in-depth interviews with patients, and a survey of healthcare professionals featuring semi-structured open-ended questions.
Methods
First, a systematic literature review was conducted across five databases. Next, 25 patients with COPD participated in detailed interviews that included seven semi-structured questions. Subsequently, 15 healthcare professionals completed a survey about factor categories and specific factors associated with non-adherence to COPD self-management. Categories and factors identified at least once across these three methods were documented. Finally, two researchers conducted preliminary mapping of the relationships between factor categories and individual factors, which was assessed for face validity by a third researcher. All processes were conducted from March 28, 2022, and January 30, 2023.
Results
The research revealed eight factor categories and 53 individual factors associated with non-adherence to COPD self-management. The categories encompassed personal, socioeconomic, disease-related, functional, treatment- related, health system-related, and environmental characteristics. The literature review, patient interviews, and survey of healthcare professionals yielded 35, 19, and 44 factors, respectively. Twelve factors were identified using all three sources. All processes were conducted from March 28, 2022, and January 30, 2023.
Conclusion
In this study, quantitative and qualitative methods were employed to develop a conceptual framework for non-adherence to COPD self-management. The findings indicate that effective self-management of this condition requires not only patient effort but also adaptations to complex treatment regimens, societal perceptions, and workplace environments.
This study was conducted to develop a conceptual framework for understanding non-adherence to self-management among patients with Chronic Obstructive Pulmonary Disease (COPD). This was accomplished through a literature review, in-depth interviews with patients, and a survey of healthcare professionals featuring semi-structured open-ended questions.
First, a systematic literature review was conducted across five databases. Next, 25 patients with COPD participated in detailed interviews that included seven semi-structured questions. Subsequently, 15 healthcare professionals completed a survey about factor categories and specific factors associated with non-adherence to COPD self-management. Categories and factors identified at least once across these three methods were documented. Finally, two researchers conducted preliminary mapping of the relationships between factor categories and individual factors, which was assessed for face validity by a third researcher. All processes were conducted from March 28, 2022, and January 30, 2023.
The research revealed eight factor categories and 53 individual factors associated with non-adherence to COPD self-management. The categories encompassed personal, socioeconomic, disease-related, functional, treatment-related, health system-related, and environmental characteristics. The literature review, patient interviews, and survey of healthcare professionals yielded 35, 19, and 44 factors, respectively. Twelve factors were identified using all three sources. All processes were conducted from March 28, 2022, and January 30, 2023.
In this study, quantitative and qualitative methods were employed to develop a conceptual framework for non-adherence to COPD self-management. The findings indicate that effective self-management of this condition requires not only patient effort but also adaptations to complex treatment regimens, societal perceptions, and workplace environments.
Chronic Obstructive Pulmonary Disease (COPD) is the most common chronic illness worldwide, with a 12% prevalence and a 5% mortality rate [1]. In Korea, the diagnosis rates of other chronic diseases such as hypertension (71.4%) and diabetes (65.2%) far exceed the diagnosis rate of COPD, which stands at 2.5% [2]. Furthermore, smoking represents a primary cause of COPD, with one study finding that 60.6% of smokers exhibited symptoms of the disease. However, approximately half of these individuals reported not seeking routine medical care, and only 0.4% spontaneously recognized COPD as a respiratory disease [3]. Another study found that even among patients diagnosed with COPD, more than half did not adhere to self-management [4]. Furthermore, only 13.9% of patients were found to use their inhalers correctly while the proper use of treatments such as inhalers is associated with lower hospitalization and mortality rates [5].
The goal of COPD self-management is to empower patients to recognize the value of this practice and actively participate in managing the condition [6]. This involves patients supporting their health through exercise and dietary adjustments, understanding the severity of their symptoms, and communicating these symptoms to healthcare professionals for appropriate treatment [7]. A systematic literature review demonstrated that various COPD self-management interventions enhance patient knowledge, medication adherence, physical activity, and success in smoking cessation [8]. Additionally, a Cochrane systematic review revealed that such interventions can improve quality of life and reduce the risk of respiratory-related hospitalization [9]. Despite these beneficial outcomes, many patients with COPD struggle with adhering to self-management protocols due to insufficient awareness of the disease. They often discontinue their medication once symptoms subside, which can adversely impact not only their physical health, but also their social and psychological well-being [10]. Consequently, strategies to address non-adherence and improve quality of life are necessary [11].
Given that self-management of COPD is a cost-effective strategy for disease treatment, numerous studies have been conducted on the factors influencing adherence and non-adherence [7, 12]. Factors associated with adherence include high education level, low number of comorbidities, strong health beliefs, high satisfaction with inhalers, participation in self-management with professionals, and education on exacerbation and symptom management [13, 14]. Conversely, factors linked to non-adherence include a lack of knowledge and understanding of COPD, frustration with the condition, poor emergency response, and insufficient education by professionals [7, 15]. However, these factors have been infrequently identified, contributing to an absence of comprehensive research investigating the full range of non-adherence factors or the development of a conceptual framework for non-adherence to COPD self-management.
To develop COPD self-management programs having continuous effects, it should preced to identify the crucial causes of non-adherence among patients [15]. However, the complexities of non-adherence behaviors are not fully understood due to ambiguous definitions, inadequate diagnosis, a failure to consider various contributing factors, and a lack of integrated research findings [12]. Consequently, insufficient research has been aimed at developing a conceptual framework by categorizing the factors related to non-adherence in COPD self-management [14, 16].
A conceptual framework is a systematic combination of concepts based on researchers’ reasoning or provisional conclusions, intended to enhance the understanding of phenomena [15]. Expert panel investigations, such as Delphi surveys, are utilized to establish priorities and develop conceptual frameworks in areas that have been insufficiently researched and thus require comprehensive review [17]. This approach facilitates the organization of concepts into hierarchical domains or subdomains. Therefore, it is crucial to develop a framework that comprehensively synthesizes and categorizes factors associated with non-adherence to COPD self-management by identifying both non-adherence and adherence factors and assigning attributes to these concepts [18]. This study classified the factors associated with non-adherence to COPD self-management by incorporating literature reviews, patient perspectives, and expert panel insights, thereby providing a solid theoretical foundation for understanding non-adherence factors.
Accordingly, the purpose of this study was to develop a conceptual framework associated with non-adherence among patients with COPD. This was accomplished using three approaches: a literature review, in-depth interviews with patients, and surveys of healthcare professionals featuring semi-structured open-ended questions.
This investigation was an exploratory study conducted to develop a conceptual framework for understanding factors associated with non-adherence in patients with COPD.
The literature search and article selection were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines [19].
The research question for the literature search was, “What are the factors associated with non-adherence to self-management in patients with COPD?” The study population consisted of adults over 40 years old with COPD, and the intervention was defined as a self-management program, with the inclusion of an analysis of risk factors for non-compliance. The inclusion criteria are self-management programs for patients with COPD had to incorporate a minimum of two of the following interventions: pharmacotherapy, exercise, symptom management, smoking cessation, and dietary modifications, among others.
The literature search was conducted from March 28 to April 10, 2022. International searches were conducted using Excerpta Medica Database (EMBASE) and Ovid MEDLINE. Keywords such as “patient compliance,” “non-compliance,” “acceptance,” “adherence,” “non-adherence,” “self-management,” “factors,” and “predictors” were combined using the Boolean operator OR, while “pulmonary disease, chronic obstructive” was combined using AND. The literature type was restricted to academic articles, and the search was limited to articles published in English. For the Korean literature, searches were performed in the National Assembly Library, Research Information Sharing Service (RISS), and DBpia databases using the keywords “chronic obstructive pulmonary disease,” “adherence,” and “non-adherence.” To focus on recent research investigating factors influencing non-adherence to COPD self-management, the publication years were limited to the period from March 2012 to Feburary 2022, a 10-year span.
The retrieved articles were organized using EndNote X8 8.2 (Clarivate Analytics, Philadelphia, PA, USA). After the exclusion of 189 duplicates from five domestic and international databases, 1,693 articles were identified. Two reviewers (YSY and REJ) independently screened the titles and abstracts based on the inclusion and exclusion criteria. These criteria excluded studies of asthma or overlap syndrome (407 articles), those unrelated to self-management or non-adherence (316 articles), qualitative studies (193 articles), review studies (412 articles), and protocol studies (118 articles), resulting in 247 articles for preliminary selection. The two reviewers then read the full texts of the initially selected articles, assessing their content for inclusion in the final analysis. Consequently, 202 articles were further removed due to having mismatched participant criteria, covering unrelated research topics, or being review articles, ultimately leaving 45 articles (Figure 1). Any discrepancies that arose during the literature selection process were resolved by consensus.
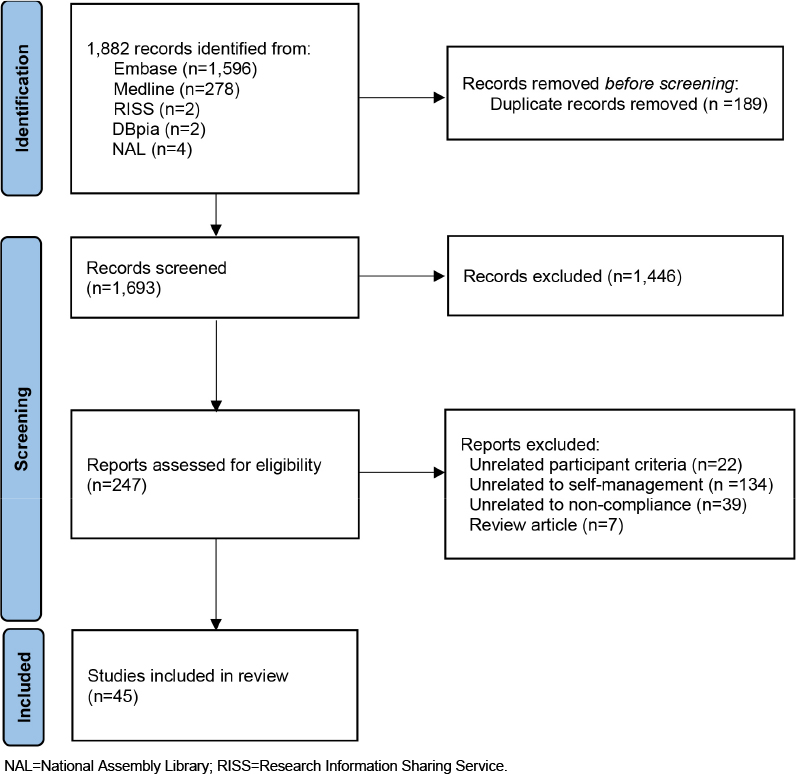
Figure 1
Selection flow for literature.
After article selection, the two researchers independently identified factors associated with non-adherence to self-management in COPD. Any discrepancies were addressed by reviewing the literature again and reaching a consensus, thus ensuring that the findings were grounded in robust evidence.
Between July 26, 2022, and January 12, 2023, 30-minute, in-depth, one-on-one interviews were conducted with patients from the Pulmonology Department at C University Hospital in G city who consented to participate in the study. Selection was focused on patients with COPD who were over 40 years old and who met specific diagnostic criteria [20]. A researcher (REJ) with qualitative research experience conducted the interviews in a quiet consultation room, asking semi-structured questions and making additional inquiries as needed. Data were collected from a total of 28 participants using seven semi-structured questions. The interviewing process was concluded once it reached saturation, as evidenced by the repetitive nature of the responses.
From October 1 to October 20, 2022, a panel of 15 experts was established, comprising five nurses, five nursing college professors, two pulmonology professors, and three resident physicians. These individuals were selected for their expertise in the field and their minimum of 1 year’s experience in caring for patients with COPD. The optimal number of experts for the panel was determined to be between 10 and 18, hence the selection of 15 members [21]. The average age of the participants was 41.53±11.51 years.
Using semi-structured open-ended questions, the experts were asked to describe categories of factors and specific factors associated with non-adherence to self-management in patients with COPD.
From October 1 to October 20, 2022, the investigators sent the expert panel an e-mail to obtain panel survey. After obtaining consent, a researcher distributed questionnaires and subsequently collected the completed surveys along with the consent forms.
During the analysis of the semi-structured survey, the factor categories and factors identified by the expert panel were extracted, with no incorporation of researcher opinions. Following this, similar terms—such as those related to forgetting medication intake, forgetfulness in general, social gatherings, and social activities—were consolidated under a single representative term selected for each group.
The researchers identified factor categories and factors associated with non-adherence to self-management in COPD. These were extracted using at least one of the three methods employed: the literature review, in-depth patient interviews, and semi-structured questions posed to the expert panel. Although the levels of evidence varied, these research findings, elicited patient preferences, and expert responses formed the foundation of evidences [22]. This approach led to the identification of factors cited in at least one of the three methods as contributing to non-adherence in COPD.
Based on the expert panel’s assessment of the relationships between COPD non-adherence factor categories and factors derived from the semi-structured questions, as well as prior research on the impact of non-adherence in chronic disease self-management [23, 24], two researchers (REJ and CSH) independently established links between factor categories and factors. For five factors with initial disagreement, repeated examination was conducted to reach a full consensus.
The preliminary draft of the linkage between factor categories and factors was reviewed by one researcher (CJY) for face validity. Following this review, the conceptual framework was revised and finalized.
To ensure the ethical integrity of this study, the researchers secured approval from the institutional review board of C university Hospital (IRB No. CNUH-2022-232). Prior to administering the questionnaire, participants were fully informed of the purpose and methods of the study. Those who agreed to participate gave their written consent. Participants were assured that the information collected from the questionnaire would be used exclusively for research purposes and that their personal information would be kept confidential. They were also informed that this information would be securely disposed of after a specified period following the analysis. Additionally, each participant received a small token of appreciation for their involvement.
Eight factor categories and 53 specific factors contributing to non-adherence in COPD self-management were identified. The distribution of these factors was as follows: 35 were derived from the literature review, 19 from the in-depth patient interviews [25], and 44 from the survey of the expert panel. The eight factor categories identified were personal, socioeconomic, disease-related, psychological, functional, treatment-related, healthcare system-related, and environmental characteristics. Twelve factors were identified using all three methods: age, sex, occupation, smoking status, social support, comorbidity, emotional state, self-efficacy, forgetfulness, physical activity, complexity of treatment, and number of medications (Table 1).
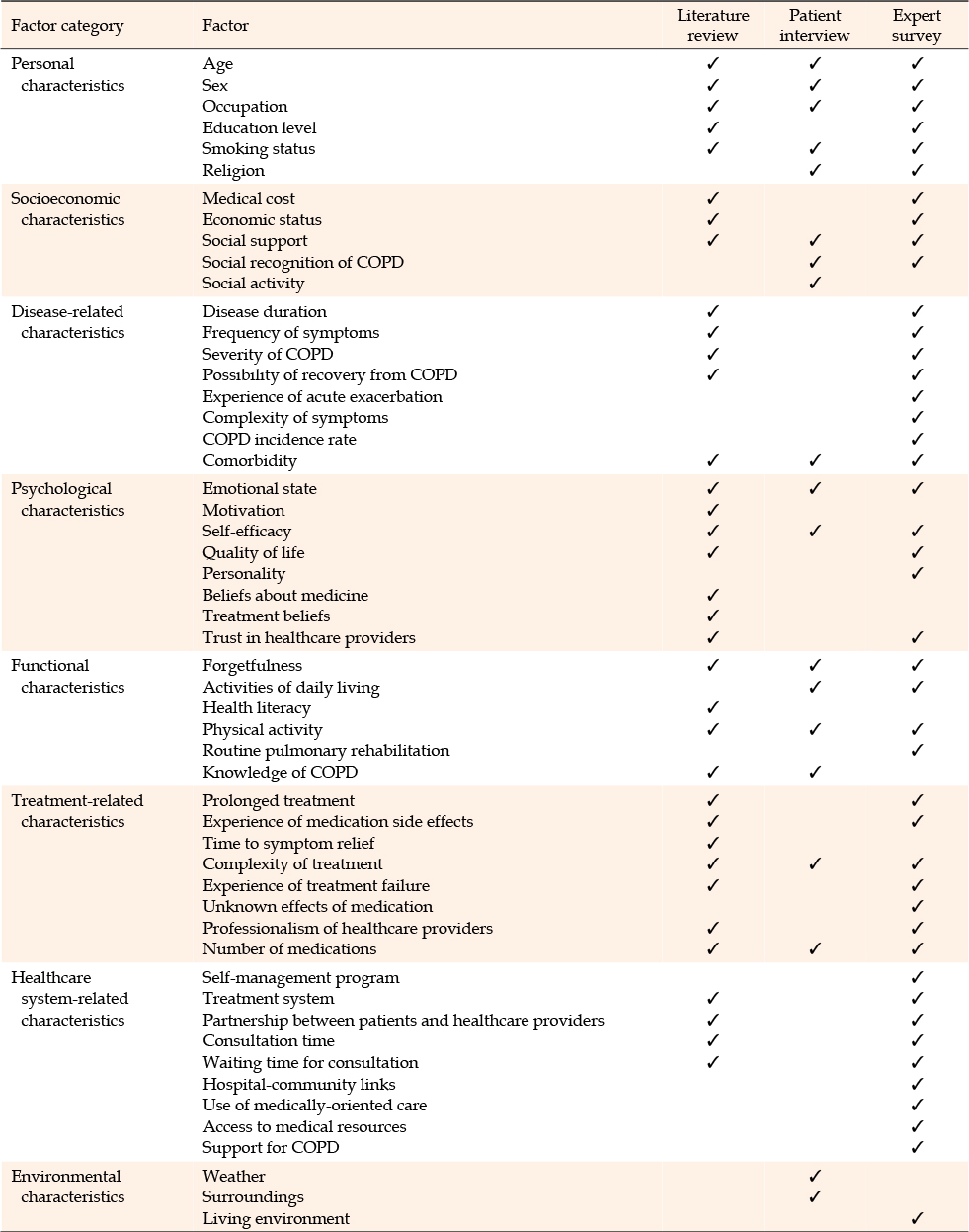
Table 1
Factor Categories and Factors Associated with Non-Adherence to COPD Self-Management
A preliminary draft was then developed. This draft identified six factors categorized under personal characteristics, five under socioeconomic characteristics, eight under disease-related characteristics, eight under psychological characteristics, six under functional characteristics, eight under treatment-related characteristics, nine under healthcare system-related characteristics, and three under environmental characteristics (Table 1).
The initial draft categorized “self-management programs” under healthcare system-related characteristics. However, based on the assessment of face validity and the findings of the literature review [26, 27], these programs were reclassified as treatment-related characteristics. With this change, the conceptual framework for non-adherence to COPD self-management was finalized (Figure 2).
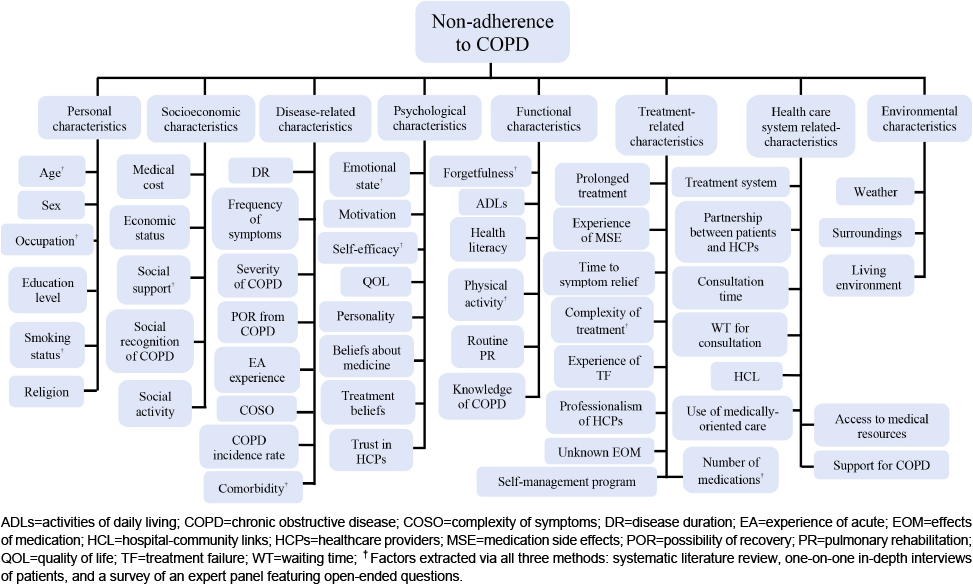
Figure 2
Schema for factor categories and factors associated with non-adherence to COPD self-management.
Based on the established linkages, the factors associated with non-adherence to COPD self-management were divided into eight categories: personal (n=6), socioeconomic (n=5), disease-related (n=8), psychological (n=8), functional (n=6), treatment-related (n=9), healthcare system-related (n=8), and environmental characteristics (n=3). The treatment-related category had the highest number of associated factors, with nine linked items. Among the factors identified using all three methods, personal characteristics appeared most frequently, with four of its six total factors identified. For socioeconomic characteristics, this value was one out of five; for disease-related characteristics, it was one out of eight; for psychological characteristics, two out of eight; for functional characteristics, two out of six; and for treatment-related characteristics, two out of nine. None of the factors categorized as healthcare system-related characteristics (eight in total) or environmental characteristics (three in total) were identified by all three methods. Consequently, personal characteristics had the highest rate of linkage with non-adherence.
This study entailed the development of a conceptual framework for understanding non-adherence to self-management among patients with COPD. The framework was constructed by extracting, categorizing, and linking relevant factor categories from a literature review, in-depth patient interviews, and expert surveys featuring semi-structured questions. Its objective was to address gaps in previous research [3, 12] by including factors identified through at least one of the three aforementioned methods as categories and specific factors related to non-adherence. The development and refinement of the conceptual framework were informed by systematic reviews of approximately 100 existing frameworks related to medication adherence [28], as well as frameworks cited in two pieces of literature and recent evidence [29]. Although the number of non-adherence factors identified through patient interviews was limited, the inclusion of factors unique to patients with COPD supports the thoroughness of the framework. Furthermore, the value of this study lies not only in its comprehensive and systematic identification of non-adherence factors but also in the hierarchical structuring of these factors. This approach enhances the understanding of the complex phenomenon of non-adherence to self-management in COPD, which extends beyond issues of medication adherence. The diversity of areas from which non-adherence factors were extracted suggests that this conceptual framework could have broad applications in the development of models for predicting non-adherence and in designing interventions to reduce non-adherence rates.
The study revealed eight categories and 53 factors associated with non-adherence in the self-management of patients with COPD. These categories encompassed personal, socioeconomic, disease-related, psychological, functional, treatment-related, healthcare system-related, and environmental characteristics. While the expert semi-structured interviews yielded factors across all categories, the literature review did not reveal any environmental characteristics, and the in-depth patient interviews uncovered no healthcare system-related factors. Moreover, disease-related and treatment-related characteristics were infrequently identified, with the exceptions being comorbidities, the complexity of treatment, and the number of medications. The absence of environmental characteristics in the literature review suggests that researchers investigating non-adherence factors in COPD self-management have predominantly focused on micro perspectives, such as individual, socioeconomic, psychological, disease, and treatment-related aspects. This trend aligns with studies on non-adherence in the self-management of other chronic diseases, such as hypertension and diabetes [30, 31]. However, relative to other chronic diseases, COPD is more closely associated with environmental factors that influence its onset and progression [32]. Patients with COPD experience significantly more frequent and severe episodes of breathlessness due to weather and their surrounding environment compared to patients with chronic heart failure [33]. This breathlessness often necessitates a restful environment or the use of short acting metered-dose inhalers, thereby exploring the inclusion of environmental characteristics as a category of factors in non-adherence to COPD self-management. Outdoor activities, which are impacted by levels of particulate matter and fine particulate matter [34], further contribute to the inescapable impact of environmental characteristics. Consequently, this study is distinguished from previous research as the first to recognize environmental characteristics as a category of factors contributing to non-adherence.
In-depth one-on-one interviews of patients with COPD revealed no factors related to characteristics of the healthcare system and very few factors related to disease- or treatment-related characteristics. This suggests that patients tend to attribute their non-adherence to self-management to personal characteristics or their immediate environment, indicating a lack of awareness that the healthcare system, disease, or treatment characteristics could influence their non-adherence. Similar findings have emerged from qualitative research involving in-depth interviews with 30 patients with COPD, in which facilitators of medication adherence were identified in the patient’s personal or immediate surroundings, including the use of diaries or visual/temporal cues for medication intake, along with family support. No facilitators related to the healthcare system or disease and treatment were identified from the interviews [35]. This indicates that these patients view themselves as passive recipients of care, not recognizing their active role in treatment. The recent paradigm shift in healthcare, which now recognizes patients as active participants in their treatment rather than solely as service recipients, represents a promising step forward [36]. Specifically, the proactive engagement of patients in COPD management marks a meaningful advancement [36]. However, prior research on the level of activation in self-management among patients with COPD indicated that 23% demonstrated low activation, with only 15% considered “activated” in managing the condition [37]. To encourage those with COPD to actively participate in their treatment, it is crucial that they recognize the potential for improved disease management through enhancements to the hospital system, alleviation of COPD symptoms, and stable treatment. Numerous studies have underscored the importance of disease and treatment characteristics in determining adherence or non-adherence to self-management [6]. Since recognizing factors of non-adherence can lead to increased adherence rates, it is crucial to extend these findings beyond research or academic publications and to inform COPD patients, raising their awareness of how disease- and treatment-related characteristics can influence their self-management behaviors.
Across all three methods used in this study—the literature review, patient interviews, and questions posed to the expert panel—12 common factors associated with non-adherence to COPD self-management were identified. Although these factors were not determined through quantitative analysis, which makes it challenging to establish them as the primary causes of non-adherence, their consistent emergence across all methods indicates their importance. Most of the factors are related to personal, psychological, and functional characteristics, underscoring the necessity of addressing these areas in management strategies. Notably, four of the six factors pertaining to personal characteristics—excluding education level and religion—were highlighted by all three methods, indicating the key role of personal characteristics in non-adherence to COPD self-management. Since most personal characteristics (with the exception of smoking status) cannot be easily changed, patients who have COPD in conjunction with disadvantageous unmodifiable factors such as age, sex, and occupation may face a relatively high risk of non-adherence. Therefore, it is essential to focus on addressing modifiable factors like smoking status, social support, self-efficacy, and physical activity, as well as devising strategies to target these elements.
The primary limitation of this study was the difficulty of fully eliminating the influence of the researchers’ subjective perspectives when linking factor categories and factors. This risk inherently persists despite the employment of a thorough, systematic approach to identify and categorize the factors impacting non-adherence to COPD self-management. Additionally, the group of COPD experts consulted was confined to a single region, limiting the diversity of viewpoints.
This study involved the development of a conceptual framework based on eight identified factor categories and 53 specific factors that influence non-adherence to self-management among patients with COPD. By categorizing these factors, the study establishes a foundation for future research focused on interventions designed to improve COPD self-management.
Therefore, future research should employ this conceptual framework for quantitative analyses through pairwise comparisons of the factor categories and specific factors.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Conceptualization and/or Methodology - CJY.
Data curation and/or Analysis - REJ, YSY & CSH.
Funding acquisition - CJY.
Investigation - CJY.
Project administration and/or Supervision - CJY Resources and/or Software - REJ, YSY & CSH.
Validation - YSY & CSH.
Visualization - REJ, YSY & CSH.
Writing-original draft and/or Review & editing - CJY, REJ, YSY & CSH.
This work was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Education (NRF-2022R1A2C1010364).
 E-SUBMISSION
E-SUBMISSION