
Purpose
The aim of this study was to systematically review the literature on the effects of mobile health applications in older adults with dementia or Mild Cognitive Impairment (MCI) and to quantify the effect size of these interventions through meta-analysis.
Methods
A systematic review and meta-analysis was conducted, with a total of seven databases searched on April 18, 2023. The risk of bias was evaluated using the Revised Cochrane Risk of Bias and the Risk of Bias in Non-randomized Studies of Interventions tools. Effect sizes were calculated using Hedges’ g within a random effects model, and subgroup analyses were also performed.
Results
A total of 10 studies were included in the systematic review, and six studies were included in the meta-analysis. Intervention groups exhibited a statistically significant improvement in cognitive function (Hedges’ g=0.33, 95% Confidence Interval [CI]=0.09~0.56, p=.007). Subgroup analyses revealed that older adults with MCI (Hedges’ g=0.41, 95% CI=0.12~0.69, p=.006) and interventions lasting more than 4 weeks (Hedges’ g=0.47, 95% CI=0.09~0.85, p=.016) demonstrated a significant cognitive improvement.
Conclusion
The results of this study indicate that mobile health applications may represent a suitable approach for improving cognitive function in older adults with MCI, emphasizing the need for at least a four-week intervention. These findings underscore the potential of mobile health interventions as a practical option for cognitive improvement in the early stages of cognitive decline.
The aim of this study was to systematically review the literature on the effects of mobile health applications in older adults with dementia or Mild Cognitive Impairment (MCI) and to quantify the effect size of these interventions through meta-analysis.
A systematic review and meta-analysis was conducted, with a total of seven databases searched on April 18, 2023. The risk of bias was evaluated using the Revised Cochrane Risk of Bias and the Risk of Bias in Non-randomized Studies of Interventions tools. Effect sizes were calculated using Hedges’ g within a random effects model, and subgroup analyses were also performed.
A total of 10 studies were included in the systematic review, and six studies were included in the meta-analysis. Intervention groups exhibited a statistically significant improvement in cognitive function (Hedges’ g=0.33, 95% Confidence Interval [CI]=0.09~0.56, p=.007). Subgroup analyses revealed that older adults with MCI (Hedges’ g=0.41, 95% CI=0.12~0.69, p=.006) and interventions lasting more than 4 weeks (Hedges’ g=0.47, 95% CI=0.09~0.85, p=.016) demonstrated a significant cognitive improvement.
The results of this study indicate that mobile health applications may represent a suitable approach for improving cognitive function in older adults with MCI, emphasizing the need for at least a four-week intervention. These findings underscore the potential of mobile health interventions as a practical option for cognitive improvement in the early stages of cognitive decline.
The World Health Organization has acknowledged the urgent need to address dementia, especially considering the lack of effective treatments and the anticipated tripling of the affected population to 150 million globally by 2050 [1]. Mild Cognitive Impairment (MCI) represents a transitional stage between normal cognitive function and dementia, characterized by preserved functional abilities [2]. The US Food and Drug Administration has approved aducanumab and lecanemab, drugs targeting Alzheimer’s disease by removing beta-amyloid from the brain. Although these drugs can slow cognitive decline in the early stages, they are not suitable for every patient [3]. With no effective pharmacological treatments for dementia currently available, efforts are now being focused on delaying the progression from MCI to dementia. The goal is to lessen both the prevalence and the economic impact of the disease [4].
Mobile health—the use of mobile wireless technologies for public health objectives—is a key component of eHealth, which involves the efficient and secure use of information and communication technologies within the healthcare sector. Mobile health applications serve a range of functions, such as providing telephone helplines, sending appointment reminders, facilitating mobile telehealth services, and enabling access to electronic patient records via mobile devices [5]. These applications offer convenience, portability, multimedia features, and absence of limitations based on time or location, making them highly accessible and convenient for health management [6].
Since 2013, research has increasingly focused on mobile health applications designed for older adults. These tools act as supplemental resources for self-care, enabling these individuals to better manage their health conditions [7]. However, evidence supporting the efficacy of mobile health applications remains limited. In particular, the level of evidence from previous studies, as detailed in systematic literature reviews, is generally low. Some studies report ambiguous or inconsistent results, and long-term research is notably absent [6, 8]. Systematic reviews examining mobile health applications for individuals with dementia have primarily highlighted patient-centric features, such as monitoring and reminders [9], along with user experience [10]. This underscores the need for further research to ascertain their therapeutic effectiveness. A separate scoping review examined cognitive training applications for older adults, including those with normal cognition [11], but its analysis was limited to cognitive functions. This limitation has hindered a broader assessment of the impacts of mobile health applications.
Systematic reviews and meta-analyses of high-quality studies can provide foundational data for older adults with dementia or MCI, who often have limited access to services and activities. Such data can substantially contribute to nursing research. This study was conducted to compile evidence on effective interventions and care strategies, potentially informing targeted nursing practices that seek to improve care quality and access for this vulnerable population. Furthermore, this analysis may suggest pathways for empirical advancements in the care of individuals with cognitive impairments.
The purpose of this study was twofold: first, to systematically review the literature on the effects of mobile health applications in older adults with dementia or MCI, and second, to determine the effect sizes of these interventions through meta-analysis. Our goal was to provide fundamental data to inform the development of mobile health applications specifically targeting older adults with dementia or MCI. By conducting systematic literature review and meta-analysis, we aimed to verify the effectiveness of mobile health applications, clarify research trends to reduce the redundancy of future studies, and offer refined and expanded guidance for future research.
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) 2020 statement [12].
The criteria for literature selection were established using the Participants, Intervention, Comparison, Outcome, and Study Design format, as recommended by the PRISMA group. The criteria are as follows [13]: 1) Population: older adults diagnosed with any type of dementia, including Alzheimer's disease and vascular dementia, as well as those with MCI, which represents a transitional stage between normal cognition and dementia. 2) Intervention: programs delivered via mobile health applications aimed at the prevention, management, and treatment of cognitive impairment. 3) Comparison: treatment as usual or conventional intervention. 4) Outcome: the overall impact of mobile health applications on various measures, such as cognition, depression, behavior, psychological symptoms, and quality of life. 5) Study Design: Randomized Controlled Trials (RCTs) and quasi-experimental pre-post designs with non-equivalent control groups.
Studies were excluded for the following reasons: 1) involved caregivers of individuals with dementia or MCI as participants; 2) directly compared mobile health applications; 3) qualitative studies; 4) grey literature (e.g., unpublished theses); 5) were unavailable in full text; or 6) were published in a language other than Korean or English.
We conducted a literature search on April 18, 2023. The databases for the search were selected based on the recommendations of the National Evidence-based Healthcare Collaboration Agency in Korea [14]. For international research, we accessed PubMed, CINAHL, and the Cochrane Library. For Korean research, we used the Research Information Sharing Service, Korean Studies Information Service System, DBpia, and the National Digital Science Library. The search terms for international databases were (MCI OR mild cognitive impairment OR dementia) AND (mobile applications OR mobile application OR smart phone OR tablet OR m-health OR mhealth OR mobile health). For the Korean databases, the search terms were (mild cognitive impairment OR dementia) AND (mobile applications OR smart phone OR tablet OR mobile health). In addition, a manual search was conducted using the references of the retrieved literature to identify additional relevant articles. For this literature search, no restrictions were imposed on the publication year.
The studies were organized and classified using reference management software (Endnote X20; Clarivate Analytics, Philadelphia, PA, USA) and Microsoft Excel 2020 (Microsoft Corp., Redmond, WA, USA). Duplicate studies were identified and removed using Endnote X20 and Microsoft Excel 2020. Titles and abstracts were initially screened to exclude studies that did not meet the inclusion criteria. Subsequently, the full texts of the remaining articles were thoroughly reviewed for final inclusion. Additionally, the reference lists of the selected studies were manually examined for additional relevant literature, culminating in the final literature selection for the systematic review. Data extraction included the following details: author(s), year of publication, research design, country, sample characteristics (including diagnosis, sample size, and mean age), intervention type and details (such as content, device used, duration of each session, total duration, and frequency), timing of measurements, comparison groups, outcome variables/measures, and statistical significance of the findings. The full process of study selection and data extraction was independently carried out by three researchers. Any disagreements were resolved through discussion and joint review of the original articles until a consensus was reached.
To assess the risk of bias in the selected articles, we employed the revised Cochrane risk of bias tool for randomized trials (RoB 2.0) for RCTs, along with the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) instrument for non-randomized studies [15]. Three researchers independently conducted the risk of bias assessment and resolved any discrepancies through discussion until a consensus was reached.
Statistical analyses for the meta-analysis were conducted using Comprehensive Meta-Analysis (CMA) version 3.0 (Biostat; Englewood, NJ, USA). A two-tailed p-value of less than .05 was considered to indicate statistical significance. Given the heterogeneity in intervention methods, measurement tools, timing, and duration among the studies, a constant treatment effect size could not be assumed. Consequently, for continuous data, a random effects model [16] was utilized to evaluate the Standardized Mean Difference (SMD) between the intervention and control groups. We opted to use the Hedges’ g, as it is an unbiased estimator of the population SMD and is generally preferred over the Cohen d or Glass Δ [17]. The interpretation of effect size was based on the 95% Confidence Interval (CI), with an effect deemed statistically significant if the 95% CI did not include zero. Effect sizes of 0.2, 0.5, and 0.8 are generally considered small, medium, and large, respectively [18]. Heterogeneity was assessed both visually, using a forest plot, and quantitatively, with the Higgins I2 statistic. An I2 value of 0% indicates no observed heterogeneity, values between 25% and 75% suggest moderate heterogeneity, and 75% or higher indicates substantial heterogeneity [14]. For analyses involving six or more studies with continuous variables, further analysis is recommended [19]. In line with this guidance, we conducted subgroup analyses based on diagnosis and the duration of intervention. Publication bias was evaluated using funnel plots. Due to the low heterogeneity observed among the included studies, no sensitivity analysis was performed.
This study was granted an exemption by the institutional review board of the affiliated university (No. ewha-202305-0041-01).
The decision process for the final selection of studies is depicted in a PRISMA 2020 flow diagram (Figure 1) [9]. From the initial 1,396 studies retrieved from seven databases, 327 duplicates were removed. Following the screening of titles and abstracts, 1,028 studies were excluded. Of the 41 articles that remained, 34 were eliminated after fulltext review. Furthermore, we performed a manual search of the reference lists in the retrieved articles, a method often used in systematic reviews [14]. This approach led to the identification of three additional articles, resulting in a total of 10 studies included in the review (Appendix 1).
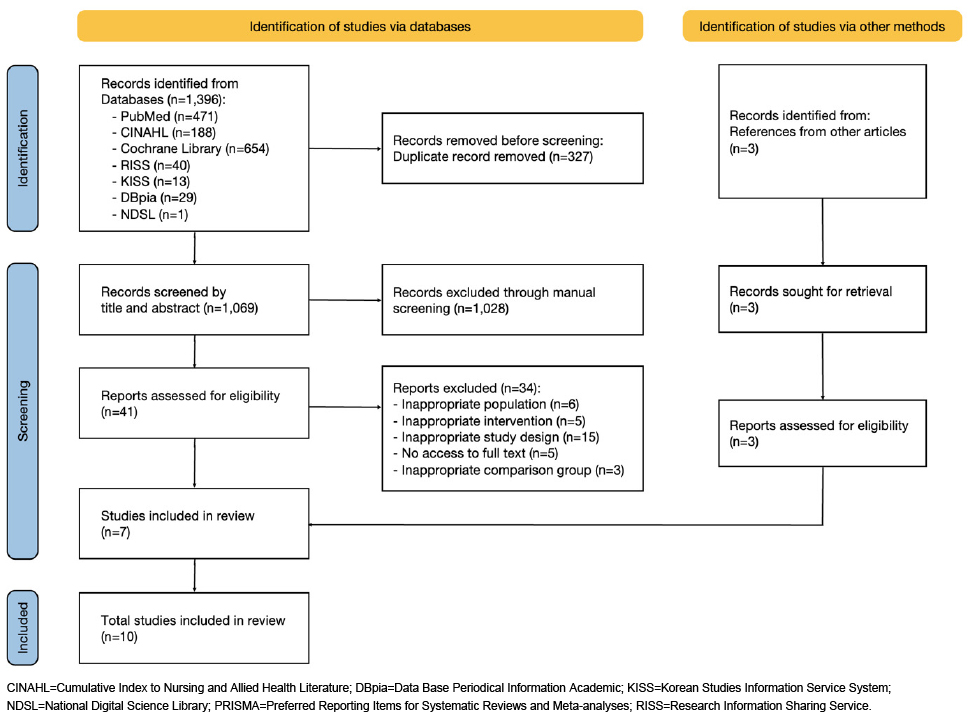
Figure 1
PRISMA flow diagram of study screening.
The general characteristics of the 10 articles analyzed in this study are summarized in Table 1. The articles were published between 2017 and 2022. The sample sizes were categorized as follows: seven studies had between 10 and 50 participants, two had between 50 and 90 participants, and one had 162 participants. Combined, the studies included 536 participants. After excluding one study that did not provide data on mean age [A5], the average age of the remaining 516 participants was 77.2 years. Regarding study design, nine articles were RCTs, and one article [A8] employed a pre-post design with a non-equivalent control group.
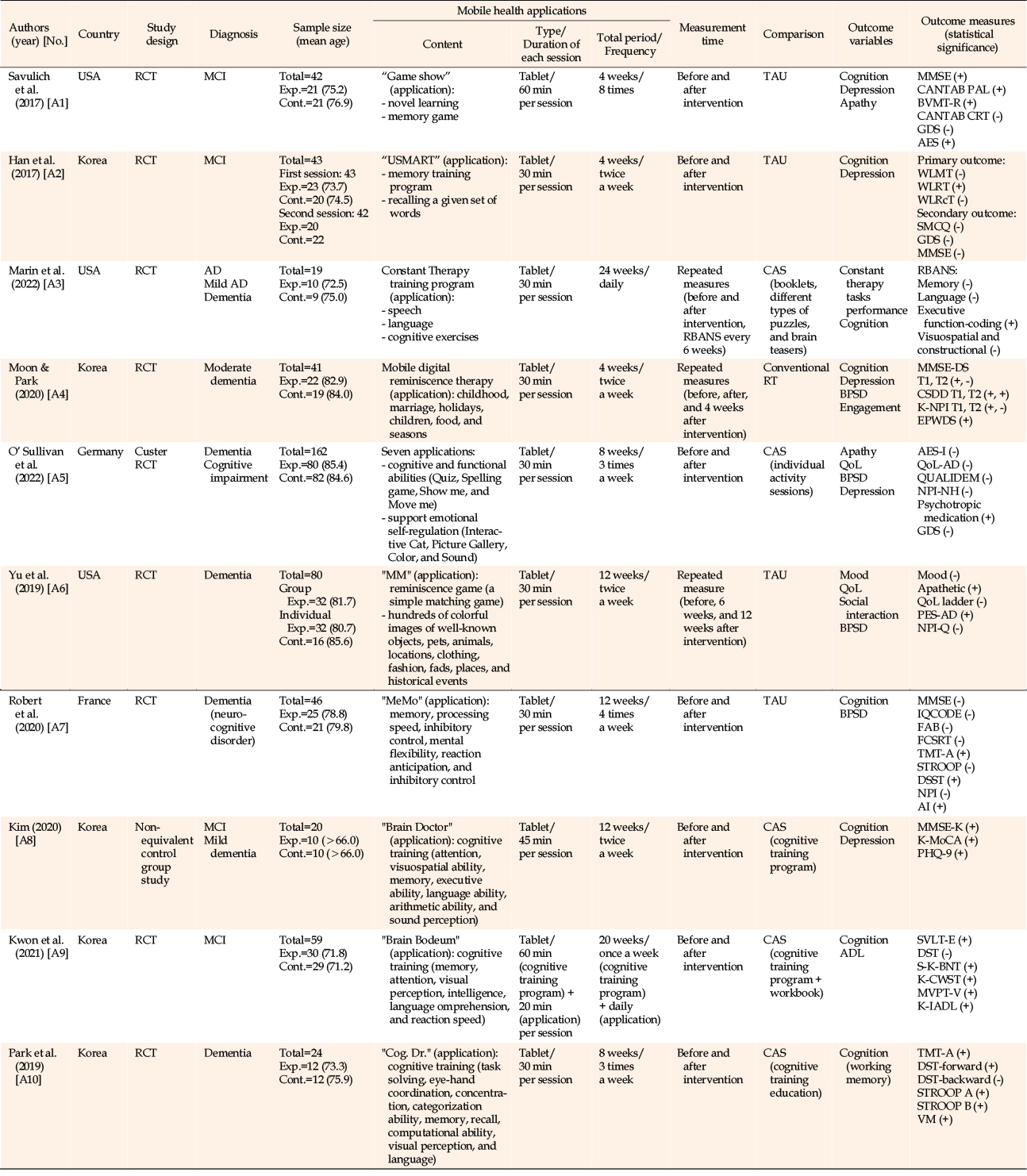
Table 1
Characteristics of Included Studies (N=10)
In all 10 studies, mobile health applications were used exclusively on tablets. The most common session duration was 30 minutes, which was reported in seven articles [A2-A7,A10]. The duration of the interventions was 4 to 8 weeks in five studies [A1,A2,A4,A5,A10], with twice-weekly sessions being the most common intervention frequency, occurring in four studies [A2,A4,A6,A8]. Measurements were most often conducted at pre- and post-intervention assessments, as found in seven studies [A1,A2,A5,A7-A10]. Regarding content, the interventions included cognitive training for memory enhancement in seven studies [A2,A3,A5,A7-A10], reminiscence therapy in two studies [A4,A6], and memory games in one study [A1]. These interventions incorporated elements such as language ability, attention and concentration, emotional self-regulation, visual-spatial skills, executive function, numerical ability, and sound recognition, as detailed in the literature.
The control groups received traditional interventions in six studies [A1,A4,A5,A8-A10] and standard care in four studies [A2,A3,A6,A7]. Traditional interventions encompassed cognitive training and education through booklets, workbooks, and paper materials, in addition to conventional reminiscence therapy. Regarding outcome variables, eight studies measured cognition [A1-A4,A7-A10], five studies evaluated depression [A1,A2, A4,A5,A8], and four studies examined behavioral and psychological symptoms of dementia [A4-A7]. Quality of life and apathy were each assessed in two studies: [A5,A6] and [A1,A5], respectively. Activities of daily living, mood, social interaction, engagement, and performance on Constant Therapy tasks were each evaluated in one study. Notably, some studies utilized multiple variables, leading to the presence of the same article in multiple categories in the analysis.
The risk of bias assessment results for the 10 included studies are presented in Figure 2. Among the nine RCTs assessed with the RoB 2.0 tool, three studies [A2,A4,A6] were evaluated as having a low risk of bias across all five domains. In another three studies [A1,A5,A9], one domain raised some concerns, while in two studies [A3,A7], two domains raised concerns, indicating potential bias. One study [A10] had issues in three domains, corresponding to a high risk of bias. The ROBINS-I tool was used to assess one non-randomized controlled study [A8], which demonstrated a moderate risk of bias overall.
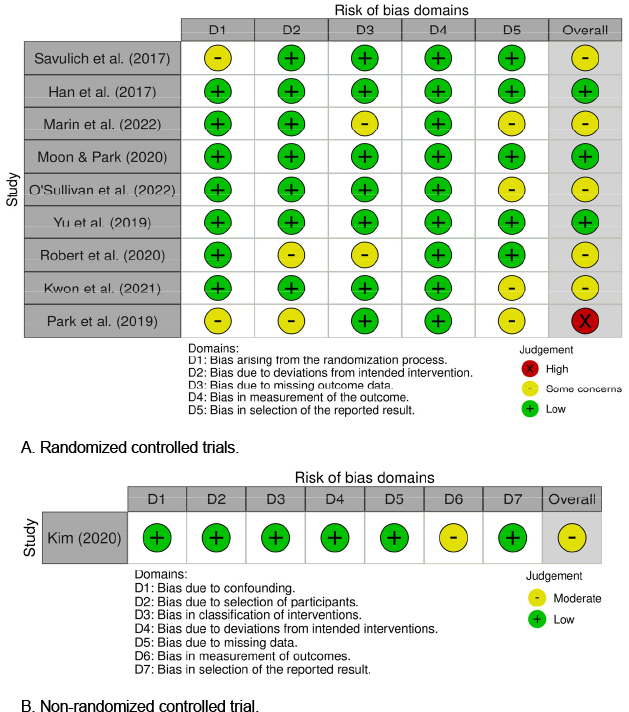
Figure 2
Quality appraisal.
A meta-analysis was conducted to evaluate the effect size of mobile health applications for older adults with dementia or MCI. Of the 10 total articles, this analysis included six studies that reported the mean, standard deviation, and sample size for the outcome variables. Although these studies differed in the outcome variables and measurement tools used, separate meta-analyses were performed for two variables present across multiple studies: cognitive function and depression. The findings are depicted in forest plots (Figure 3). To standardize the directionality of the effect size, the mean of the depression variable was multiplied by −1, as its direction was opposite to that of the cognitive function variable. Additionally, a funnel plot was used to evaluate publication bias. This plot indicated symmetry for the cognitive function variable but asymmetry for the depression variable. However, given the small number of studies analyzed (fewer than 10), determining the presence of publication bias was challenging (Appendix 2).
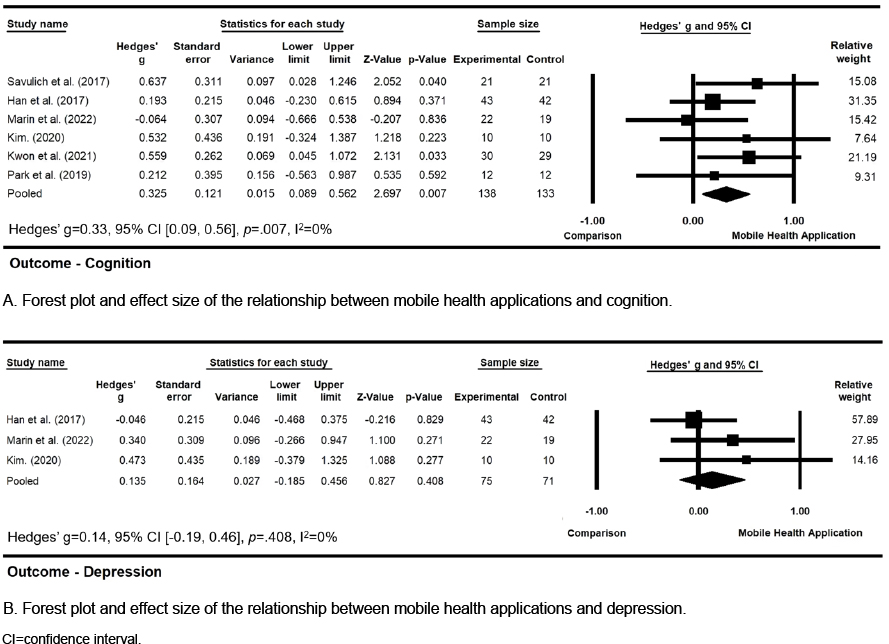
Figure 3
Forest plot and effect size.
A meta-analysis of six studies that investigated the impact of mobile health applications on cognitive function in the target population revealed a statistically significant, moderate effect size with low heterogeneity (Hedges’ g=0.33, 95% CI=0.09~0.56, p=.007, I2=0%). A separate meta-analysis of three studies evaluating the effects of these applications on depression within this population indicated a non-significant and small effect size, also with low heterogeneity (Hedges’ g=0.14, 95% CI=−0.19~0.46, p=.408, I2=0%).
Subgroup analyses of the impact of mobile health applications were performed based on diagnosis and the duration of intervention (Figure 4).
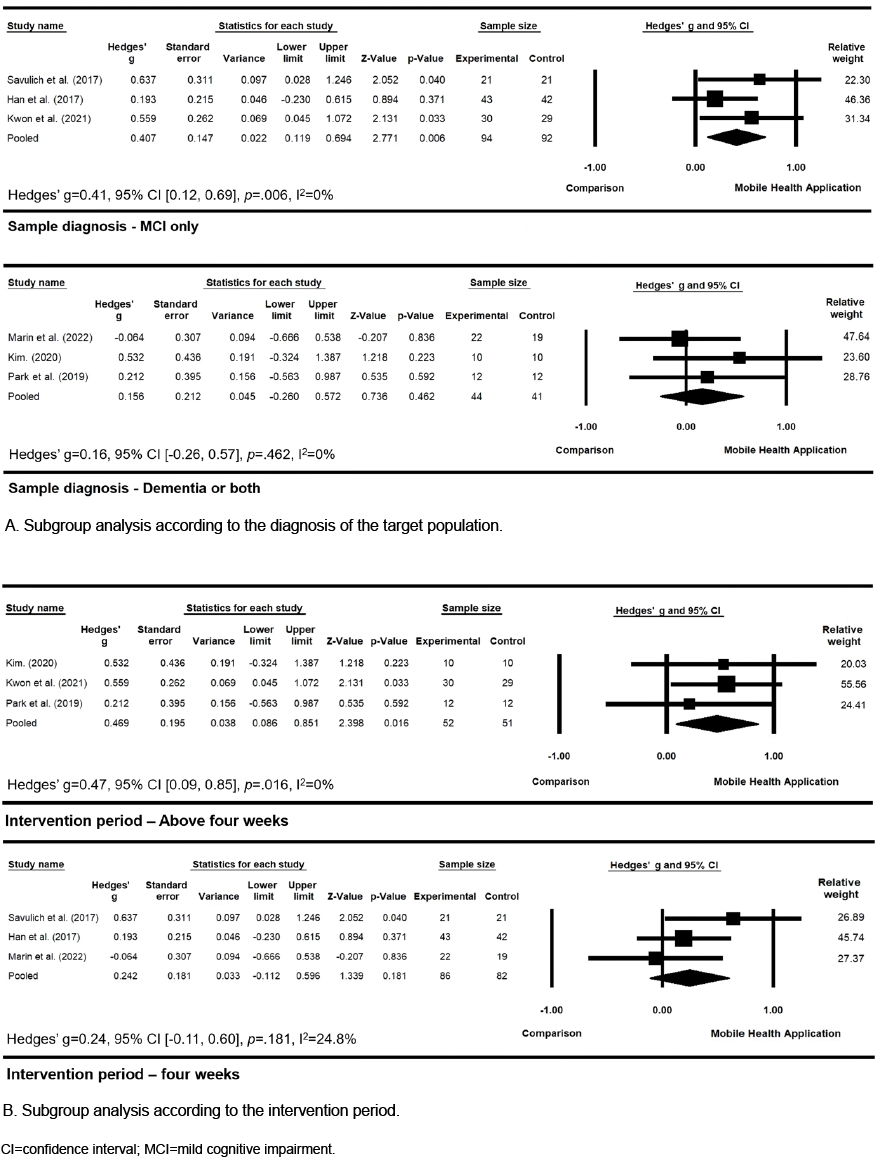
Figure 4
Forest plot of subgroup analysis.
A meta-analysis of three studies examining cognitive function in individuals with MCI revealed a significant, moderate effect size with low heterogeneity (Hedges’ g=0.41, 95% CI=0.12~0.69, p=.006, I2=0%). In contrast, a meta-analysis of studies that included older adults with both dementia and MCI (n=3) indicated a non-significant and small effect size, also with low heterogeneity (Hedges’ g=0.16, 95% CI=−0.26~0.57, p=.462, I2=0%).
A meta-analysis of three studies investigating the effects of using these applications for more than 4 weeks on cognitive function revealed a significant, moderate effect size with low heterogeneity (Hedges’ g=0.47, 95% CI=0.09~0.85, p=.016, I2=0%). In contrast, a meta-analysis of three studies examining the impact of applications used for 4 weeks showed a non-significant and small effect size regarding cognitive function, also with low heterogeneity (Hedges’ g=0.24, 95% CI=−0.11~0.60, p=.181, I2=24.8%).
This study examined the effects of mobile health applications in older adults with dementia or MCI through a systematic review and meta-analysis. A total of 10 studies were included in the review, with six of these incorporated into the meta-analysis.
The findings revealed that mobile health applications take various forms, including cognitive training, memory games, and reminiscence therapy. Compared to traditional interventions, mobile health applications were shown to be effective in improving a range of clinical outcomes. In South Korea, government-managed face-to-face dementia prevention education currently faces challenges, including space requirements, participant limitations, regional disparities, and resource shortages [20]. In contrast, mobile health applications offer versatile functions, including notifications and reminders, education, motivation, and prevention [6]. Once users learn to use these applications, they can independently participate in repeated interventions, making these programs accessible at home or within the community. Additionally, mobile health applications are cost-effective [21]. Therefore, the development and promotion of mobile health application interventions for older adults with cognitive decline could increase access and benefit local communities.
Among the 10 included studies, five involved participants aged 75 years or older. Excluding one study [A5] that did not report the mean age, the average age of the remaining 516 participants was 77.2 years. All 10 studies used tablets to provide the interventions. In the United States, smartphone ownership among older adults aged 65 and older rose from 13% in 2012 to 61% in 2021, while tablet ownership increased from less than 4% in 2012 to 44% in 2021 [22]. Previous research has indicated that tablets can be beneficial for cognition, enjoyment, knowledge acquisition, social connections, and communication among older adults with cognitive impairment [23]. Tablet applications have also been shown to improve the learning and functional abilities of older adults with dementia [24]. When introducing mobile health applications to the older adult population, challenges such as limited digital literacy and difficulties stemming from physical and sensory impairments may arise [25]. However, these challenges can be mitigated through ongoing education provided by caregivers, facilities, or healthcare professionals, as well as through training programs organized by local government authorities that teach older adults to use smart devices effectively.
The risk of bias assessment for this study indicated that, of the nine RCTs examined, four [A3,A5,A9,A10] exhibited potential selection bias. This can be attributed to the absence of information confirming that the analysis preceded the unblinding of the relevant intervention data. Consequently, future studies should include a detailed account of the timing of data unblinding. One study [A10] was found to have a high overall risk of bias, with issues across three domains: bias arising from the randomization process, bias due to deviations from the intended interventions, and concerns regarding selective outcome reporting. These problems may relate to the challenges of strictly enforcing blinding among participants and researchers in studies involving mobile health applications. Therefore, caution is advised when interpreting these findings. Nevertheless, for the measurement of outcomes, all nine RCTs were deemed to have a low risk of bias. This was facilitated by their use of independent evaluators who did not participate in the delivery of interventions, thereby improving the reliability of the outcome measurements. Additionally, the use of objective measurement tools, which are less susceptible to bias stemming from knowledge of the interventions during measurements.
In this study, mobile health applications were associated with reduced depression among older adults with dementia and MCI, although the effect size was small. This reduction was not statistically significant, contrasting with a previous study that reported a significant decrease in Geriatric Depression Scale (GDS) scores following ICT-based interventions [26]. However, the meta-analysis conducted in the prior study involved a single depression scale (the GDS), whereas three studies in the present analysis utilized different depression measurement scales.
The findings of the present meta-analysis indicated that overall, mobile health applications significantly improved cognitive function in older adults with dementia or MCI. However, the lack of prior systematic literature reviews focusing on the effects of mobile health applications in this population limited our ability to compare and validate these results. In a previous meta-analysis of ICT-based interventions for individuals with MCI [27], a significant improvement in cognitive function was noted, with an effect size slightly larger (SMD=0.45) than that of the present research (Hedges’ g=0.33). Additionally, in another meta-analysis study that examined computer-based interventions in the same population [28] found a significant improvement in cognitive function, with a larger effect size (SMD=0.82) compared to our findings. Similarly, a prior meta-analysis investigating the impact of computer-based cognitive training on individuals with MCI [29] also demonstrated a significant improvement in cognitive function. The effect size reported in that study (SMD=0.23) was slightly smaller than that found in this study.
In this study, the effect sizes of mobile health applications on cognitive function were examined based on the diagnosis of the participants (dementia or both, MCI only). The findings revealed that mobile health application use significantly improved cognitive function in participants with MCI. However, no significant effect was observed among the participants with dementia. This suggests that mobile health applications may be effective for individuals with mildly impaired cognitive function, but their impact on conditions such as dementia appears limited. A previous meta-analysis [8] that investigated the effects of digital therapeutics in the same population reported different outcomes for overall cognitive function, memory, and executive function in a subgroup analysis based on participant diagnosis. Consequently, further research is necessary to explore the differential effectiveness of mobile health applications in relation to patients’ diagnoses. Investigating the long-term efficacy of such interventions across a spectrum of cognitive conditions will not only help define their role in cognitive health management but also offer valuable insights for the development and use of individually tailored mobile health applications.
In this research, we also examined the effect size of mobile health applications on cognitive function based on the duration of intervention. Our findings indicated that using mobile health applications for more than 4 weeks led to significant improvements in cognitive function. Accordingly, to achieve meaningful cognitive benefits, an intervention period exceeding 4 weeks is recommended for mobile health application-based programs. However, these results appear to conflict with those of a previous meta-analysis [8], which investigated application-based interventions in a similar population. That study found that overall cognitive function improved significantly with interventions shorter than 8 weeks (SMD=0.39). In contrast, memory (SMD=0.55) and performance function (SMD=0.32) showed significant improvements only with interventions longer than 8 weeks. These discrepancies highlight the need to customize the length of the intervention to target specific cognitive outcomes. Further research is necessary to optimize mobile health strategies for cognitive improvement.
Several limitations of this study should be acknowledged. First, the study utilized an integrated approach that did not fully account for the differences in purpose, content, and duration of the various interventions delivered through mobile health applications. Second, despite efforts to obtain raw data from the original authors via email, we received no response. This led to a limited sample size for the meta-analysis, and as a result, only three studies were included in the subgroup analysis. Third, the analysis was restricted to published articles, which could potentially lead to an overestimation of the effect. Based on all three of these limitations, caution should be required when interpreting the results regarding the effects of mobile health applications. Fourth, among the studies included, only three were assessed as having a low risk of bias across all evaluated criteria, highlighting the need for future well-designed studies. Fifth, the study did not undergo a pre-registration process.
This study demonstrated the significant effects of mobile health applications on cognitive function in older adults with dementia or MCI. In subgroup analysis, the use of these applications significantly increased cognitive function among older adults with MCI. However, no significant effect on cognitive function was observed among older adults with dementia. Additionally, mobile health application-based interventions administered for longer than 4 weeks yielded significant improvements in cognitive function. Based on these results, we conclude that mobile health application usage may be effective for older adults with MCI, in contrast to those with progressive dementia. When planning interventions involving mobile health applications, it is advisable to consider a minimum intervention period of at least 4 weeks.
For future studies, it is crucial to accumulate additional research investigating the differential effects of mobile health application interventions based on a diagnosis of dementia or MCI. Additionally, repeated studies are needed to examine the effects of intervention duration. The findings of the present study could provide a foundation for developing and administering nursing interventions aimed at improving cognitive function in older adults with dementia or MCI.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - LM, PJ, and LS.
Analysis - LM, PJ, and LS.
Interpretation of the data - LM, PJ, and LS.
Drafting and/or critical revision of the manuscript for important intellectual content - LM, PJ, and LS.
A1. Savulich G, Piercy T, Fox C, Suckling J, Rowe JB, O'Brien JT, et al. Cognitive training using a novel memory game on an iPad in patients with amnestic mild cognitive impairment (aMCI). International Journal of Neuropsychopharmacology. 2017;20(8):624-33. https://doi.org/10.1093/ijnp/pyx040
A2. Han JW, Son KL, Byun HJ, Ko JW, Kim K, Hong JW, et al. Efficacy of the ubiquitous spaced retrieval-based memory advancement and rehabilitation training (USMART) program among patients with mild cognitive impairment: a randomized controlled crossover trial. Alzheimer's Research & Therapy. 2017;9(1):9:39. https://doi.org/10.1186/s13195-
A3. Marin A, DeCaro R, Schiloski K, Elshaar A, Dwyer B, Vives-Rodriguez A, et al. Home-based electronic cognitive therapy in patients with Alzheimer disease: feasibility randomized controlled trial. JMIR Formative Research. 2022;6(9):e34450. https://doi.org/10.2196/34450
A4. Moon S, Park K. The effect of digital reminiscence therapy on people with dementia: a pilot randomized controlled trial. BMC Geriatrics. 2020;20:166. https://doi.org/10.1186/s12877-
A5. O'Sullivan JL, Lech S, Gellert P, Grittner U, Voigt-Antons JN, Moller S, et al. A tablet-based intervention for activating nursing home residents with dementia: results from a cluster-randomized controlled trial. International Psychogeriatrics. 2022;34(2):129-41. https://doi.org/10.1017/S1041610221000818
A6. Yu F., Mathiason MA, Johnson K, Gaugler JE, Klassen D. Memory matters in dementia: efficacy of a mobile reminiscing therapy app. Alzheimer's & Dementia: Translational Research & Clinical Interventions. 2019;5(1):644-51. https://doi.org/10.1016/j.trci.2019.09.002
A7. Robert P, Manera V, Derreumaux A, Ferrandez YMM, Leone E, Fabre R, et al. Efficacy of a web app for cognitive training (MeMo) regarding cognitive and behavioral performance in people with neurocognitive disorders: randomized controlled trial. Journal of Medical Internet Research. 2020;22(3):e17167. https://doi.org/10.2196/17167
A8. Kim MH. The effect of a home visit cognitive training program using tablet-based recognition rehabilitation application (Brain Doctor) on local elderly people's cognitive function and depression. Journal of The Korean Society of Integrative Medicine. 2020;8(4):49-58. https://doi.org/10.15268/ksim.2020.8.4.049
A9. Kwon MH, Lee JS, Cha TH, Yoo DH, Kim H, Kim SK. Development and effectiveness verification of application-based cognitive training program for the elderly with dementia in community. The Journal of Korean Society of Occupational Therapy. 2021;29(1):27-39. https://doi.org/10.14519/kjot.2021.29.1.03
A10. Park HS, Moon JH, Jeong BL. The effect of Cog. Dr. on working memory in older adults with mild dementia. Journal of Korea Rehabilitation Welfare Engineering. 2019;13(2):109-17. https://doi.org/10.21288/resko.2019.13.2.109

 E-SUBMISSION
E-SUBMISSION