
Purpose
This systematic review and meta-analysis aimed to investigate the effects of aromatherapy interventions on stroke symptoms in stroke patients.
Methods
This study adhered to the Preferred Reporting Items of Systematic Reviews and Meta-Analysis guidelines. Relevant studies published between 2004 and 2022 were searched in the PubMed, CINAHL, Cochrane Library, EMBASE, ERIC, and RISS databases. The review included randomized and non-randomized studies of stroke patients who received aromatherapy interventions targeting stroke symptoms. The extracted literature was evaluated via the ROB 2 and ROBINS-1 quality appraisal checklists and visualized using a risk-of-bias visualization tool.
Results
The review included five randomized controlled trials and five quasi-experimental studies. The results showed that aromatherapy, administered through massage, inhalation, acupressure, mouth care, and olfactory stimulation, was effective in alleviating pain, constipation, oral health, motor power, muscle strength, balance, fatigue, and sleep quality. Aromatherapy also demonstrated beneficial effects in reducing depression, stress, delirium, blood pressure, pulse rate, respiration rate, serum cortisol, and antioxidants, while enhancing happiness, body temperature, and quality of life. A meta-analysis of mean differences in post-test results revealed that three studies reported a significant effect on pain, with an effect size of 1.85 (95% CI, 0.18~3.51).
Conclusion
Aromatherapy had positive effects on physical, physiological, psychological, cognitive, and integrative health outcomes. We recommend the use of aromatherapy in stroke patients to improve pain relief and health outcomes.
This systematic review and meta-analysis aimed to investigate the effects of aromatherapy interventions on stroke symptoms in stroke patients.
This study adhered to the Preferred Reporting Items of Systematic Reviews and Meta-Analysis guidelines. Relevant studies published between 2004 and 2022 were searched in the PubMed, CINAHL, Cochrane Library, EMBASE, ERIC, and RISS databases. The review included randomized and non-randomized studies of stroke patients who received aromatherapy interventions targeting stroke symptoms. The extracted literature was evaluated via the ROB 2 and ROBINS-1 quality appraisal checklists and visualized using a risk-of-bias visualization tool.
The review included five randomized controlled trials and five quasi-experimental studies. The results showed that aromatherapy, administered through massage, inhalation, acupressure, mouth care, and olfactory stimulation, was effective in alleviating pain, constipation, oral health, motor power, muscle strength, balance, fatigue, and sleep quality. Aromatherapy also demonstrated beneficial effects in reducing depression, stress, delirium, blood pressure, pulse rate, respiration rate, serum cortisol, and antioxidants, while enhancing happiness, body temperature, and quality of life. A meta-analysis of mean differences in post-test results revealed that three studies reported a significant effect on pain, with an effect size of 1.85 (95% CI, 0.18~3.51).
Aromatherapy had positive effects on physical, physiological, psychological, cognitive, and integrative health outcomes. We recommend the use of aromatherapy in stroke patients to improve pain relief and health outcomes.
A stroke is a neurological disorder characterized by impaired brain function, which is caused by the rupture or blockage of blood vessels that supply blood to a part of the brain due to a vascular issue [1]. Stroke ranks as the second leading cause of death and the third leading cause of disability worldwide [2]. The incidence and prevalence of stroke are substantially increasing in most countries, largely due to population growth and aging [2]. Similarly, the number of stroke patients in Korea has been steadily rising each year, from 94,813 in 2015 to 113,455 in 2018, and most recently, 120,305 in 2021 [3]. The prevalence of stroke in Korea is also on an upward trend. Depending on the severity of the disability or damage, long-term care and treatment may be necessary, leading to substantial social opportunity costs [4].
Stroke symptoms can vary based on the size and location of the infarct. These may include paralysis or hemiplegia, disturbances in consciousness, paresthesia or loss of sensation, visual disturbances, cognitive impairment, aphasia, dysphagia, and emotional anxiety. The prognosis for patients can also differ, depending on the location and size of the stroke. The extent of the damage can result in either complete or incomplete recovery [1]. For stroke patients requiring long-term rehabilitation and care due to sequelae from sudden neurological damage following the onset of a stroke, active nursing interventions in physical, psychological, and cognitive aspects are essential [5].
Stroke recurrence, the possibility of death, and functional recovery, are significant concerns for patients and their families, given that clinical presentations and responses to treatment can vary widely among patients [1]. Implementing nursing interventions for stroke patients is a crucial aspect of rehabilitation, aimed at enhancing patient comfort and minimizing stress. Aromatherapy, with its antioxidant properties, has been reported to offer neuroprotective effects, thereby reducing neurological symptoms and providing emotional benefits such as stress relief [6].
Aromatherapy is a fast-growing complementary therapy worldwide [7]. The therapeutic use of essential oils, extracted from plants through steam distillation or pressing, has been practiced for centuries. These oils can be inhaled or absorbed through the skin [8]. Essential oils have been utilized extensively in both the East and West for thousands of years for physical and mental healing. They were introduced as a natural treatment, known as aromatherapy, by French cosmetic chemist Rend-Maurice Gatefosse in the 1930s [9]. The medicinal properties of essential oils include bactericidal or antiseptic effects, expectorant qualities, cellular regeneration, activation of capillary circulation, anti-inflammatory effects, pain reduction, bloating alleviation, spasmolytic and neuroleptic properties, and nerve-strengthening capabilities [9]. Aromatherapy, as a complementary and alternative therapy, can be integrated with medical treatment by nurses or other health professionals [10]. However, skin absorption of the compounds used in aromatherapy may cause irritation, and skin testing is recommended for those with sensitive skin or allergies [11]. In addition, dropouts due to nausea and vomiting occurred in previous studies [12], implying that essential oils may cause adverse reactions such as nausea, dizziness, and headache. Therefore, it is necessary to select an appropriate intervention in an individualized manner according to the patient's condition and symptoms.
Previous research on aromatherapy in stroke patients has demonstrated that the use of aromatic solutions in oral care for older adults with stroke can decrease oral bacteria and enhance oral health [13]. Additionally, aromatic massage has been found to lessen upper extremity pain in stroke patients [14], as well as alleviate pain, depression, and sleep disturbances [15]. It has also proven effective in relieving constipation [16]. Essential oils have been shown to possess anti-inflammatory and antioxidant properties, along with psychological effects that can mitigate both physical and emotional conditions, such as delirium [17], fatigue, and euphoria [18].
Although several experimental studies have used aromatherapy in stroke patients [13, 14, 15, 16, 17, 18], there is a lack of overall analyses and meta-analyses of therapeutic interventions. This systematic review explored various aspects of aromatherapy interventions for stroke patients, and the results are expected to serve as a valuable resource for the planning and execution of viable nursing interventions in clinical practice. The objective of this study was to carry out a systematic review of experimental studies that investigated the impact of aromatherapy interventions on stroke patients, to identify the content and characteristics of diverse interventions, and to assess their effects on stroke patients. This study will lay the groundwork for the effective implementation of optimal aromatherapy nursing interventions for stroke patients. The specific objectives were to identify aromatherapy intervention methods applied to stroke patients and to evaluate their effects.
This study systematically reviewed experimental aromatherapy interventions, assessing their effectiveness in treating stroke patients through a meta-analysis. The review process adhered to the reporting guidelines for systematic reviews as outlined in PRISMA (Preferred Reporting Items of Systematic Reviews and Meta-Analyses) [19], NECA (National Evidence-based Collaborating Agency)’s Health Technology Assessment Methodology [20], and the Cochrane Handbook for Systematic Reviews of Interventions version 6.3 [21].
The search strategy involved querying international search databases with the following terms: “stroke [MeSH] AND (aroma* OR aromatherapy [MeSH])” in PubMed, “hemiplegia AND (aroma* OR aromatherapy [MeSH]),” “hemiplegic AND (aroma* OR aromatherapy [MeSH])” in CINAHL, and “stroke AND (aroma OR aromatherapy)” in the Cochrane Library. Additional search terms included “hemiplegia AND (aroma OR aromatherapy),” “hemiplegic AND (aroma OR aromatherapy),” “‘aroma therapy hemiplegia’ OR ((‘aroma’/exp OR aroma) AND (‘therapy’/exp OR therapy) AND (‘hemiplegia’/exp OR hemiplegia))” in EMBASE, and “ (‘stroke’/exp OR stroke)” in ERIC. A professor of bibliometrics was consulted in formulating our search strategy. To minimize the possibility of skewed findings, a manual search was also conducted (Appendix 1).
The literature was selected through advanced searching using the Participant, Intervention, Comparison, Outcome, Setting, Time-Study Design (PICOST-SD) framework. Case reports were independently extracted and evaluated by two researchers. The parameters of the PICOST-SD framework were as follows: 1) participants: stroke patients; 2) intervention: aromatherapy; 3) comparison: non-aromatherapy; 4) outcome: health outcomes; 5) setting: clinical or non-clinical settings; 6) time: post-stroke phase; and 7) study design: randomized and non-randomized studies. The final data were jointly reviewed by the researchers, and concordance was confirmed through a meeting. In the event of discrepancies, the results from the meeting between the investigators were used. The selection of databases was guided by the areas recommended by the COre, Standard, Ideal (COSI) of the National Library of Medicine (NLM) [22]. The inclusion criteria were as follows: 1) studies involving aromatherapy interventions, 2) quasi-experimental studies and randomized experimental studies, 3) studies focusing on stroke patients, 4) journal articles written in either Korean or English, and 5) articles published up until May 2023. The exclusion criteria included: 1) dissertations and works in progress, 2) gray literature, such as research reports and conference proceedings, 3) monographs, 4) protocol studies and articles without results, 5) studies with a one-group design, and 6) studies involving animals.
Two researchers independently conducted a literature review, extracted data, and analyzed the results. The search took place from June 5 to June 15, 2023, using electronic sources. MeSH and Emtree were used as search terms, along with natural language and synonyms. The literature search was carried out using six search engines: PubMed, CINAHL, Cochrane Library, EMBASE, ERIC, and RISS. A total of 506 articles were found (372/86/12/10/0/26 respectively), spanning the time period from 1961 to 2023. An additional four articles were located through a manual search of reference lists and Google Scholar, bringing the total to 510 articles. We then removed 52 duplicates based on the author, study title, and year of publication, leaving 458 articles. After reading all the titles and abstracts, we excluded 416 articles that did not involve stroke patients or aromatherapy interventions, and one study report could not be retrieved, which left us with 41 articles. Upon reading the full texts of these 41 articles, we eliminated 19 investigational studies, 10 studies with study designs incompatible with the scope of the present study, one study involving rats, and one study not related to aromatherapy. This process resulted in the final selection of 10 articles from 2004 to 2022 (Figure 1) (Appendix 2).
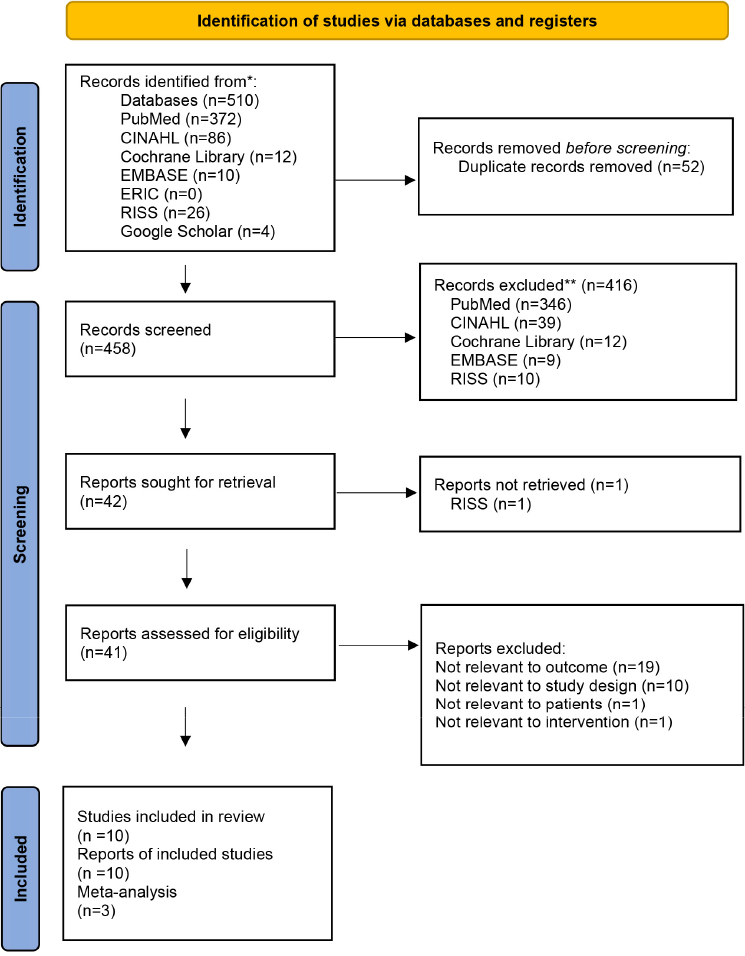
Figure 1
PRISMA 2020 diagram.
The final quality assessment of the chosen articles was conducted using Cochrane's Risk-Of-Bias 2 (ROB-2) [14], which includes six domains for randomized trials, and the Risk-Of-Bias In Non-randomized Studies of Interventions (ROBINS-I) [23] tool, published in 2016, for non-randomized trials. The agreement between the two researchers on the final assessment results was evaluated using the Kappa coefficient, and only areas with a strong agreement of .80 or higher were retained [19]. Inter-rater consistency was measured, with Cohen’s κ coefficients of .80~1.00. Any disagreements were addressed through discussion among the researchers, and the articles were reviewed again to finalize the quality assessment. As a result of the quality assessment, the final 10 articles were selected. The results for the selected articles were displayed as traffic light charts and bar charts using Risk-of-bias VISualization (robvis), a tool for visualizing quality assessment [24] (Appendix 3).
The final 10 selected papers underwent a qualitative analysis, with each paper's analysis documented as a case report. These case reports encompassed general characteristics such as the first author, year, country, intervention setting, study design, participant characteristics, and the number of final analyses in both control and experimental groups. The intervention methods were also detailed, including the name, form, duration, and frequency of the intervention, as well as the control intervention. The reports also covered intervention measures, such as dependent variables and measurement tools. Intervention outcomes were documented, including physical, physiological, psychological, and cognitive outcomes, as well as quality of life. The quality of the literature, effect size, and any publication bias were also assessed.
A total of 10 articles were identified, with publication dates spanning from 2004 (A1) to 2022 (A10). The distribution of these articles was skewed towards domestic studies, with eight originating from South Korea (A1-A7,A9), one from Iran (A8), and one from Turkey (A10). One study (A8) included patients in the acute phase (within 12 hours of onset of stroke), and the others involved at least one month of follow-up. The interventions took place in various settings, including hospitals and rehabilitation centers. The studies employed different designs, with five having randomized experimental designs (A3,A7-A10) and the other five having quasi-experimental designs (A1,A2,A4-A6). The number of participants in these studies varied, ranging from a minimum of 14 (A7) to a maximum of 91 (A10) stroke patients (Table 1).
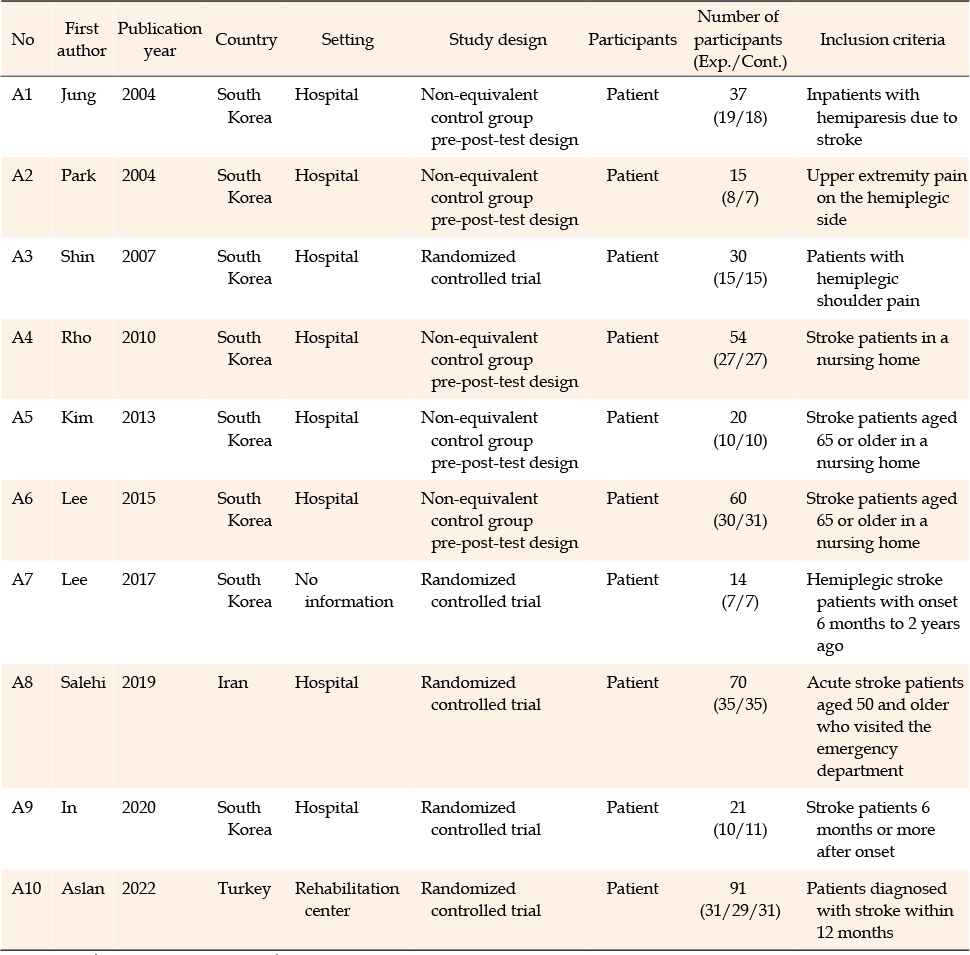
Table 1
Characteristics of Selected Studies
The interventions encompassed seven studies (A1-A5,A7,A10) that utilized aromatic oils, absorbed into the skin via massage and acupressure. Three studies (A8-A10) employed nasal inhalation, and one study (A6) used mucosal absorption through oral gargling. Four studies (A4,A8-A10) exclusively used lavender oil, while six studies (A1-A3,A5-A7) incorporated a blend of two or more oils. The oils used in these blends included lavender, juniper berry, rosemary, pepper, bergamot, clary sage, peppermint, sweet marjoram, sweet orange, black pepper, and patchouli. The duration of the interventions varied, ranging from 1 day (A4) to 4 weeks (A10), with a minimum of 2 interventions (A4) and a maximum of 28 (A3). The control groups consisted of two placebo oils (A2,A8), two saline solutions (A6,A9), two massage (A4) or acupressure (A3) treatments, two standard physical therapy (A7) or nursing care (A10) procedures, and two no-treatment groups (A1,A5) that did not use aroma oils (Table 2).
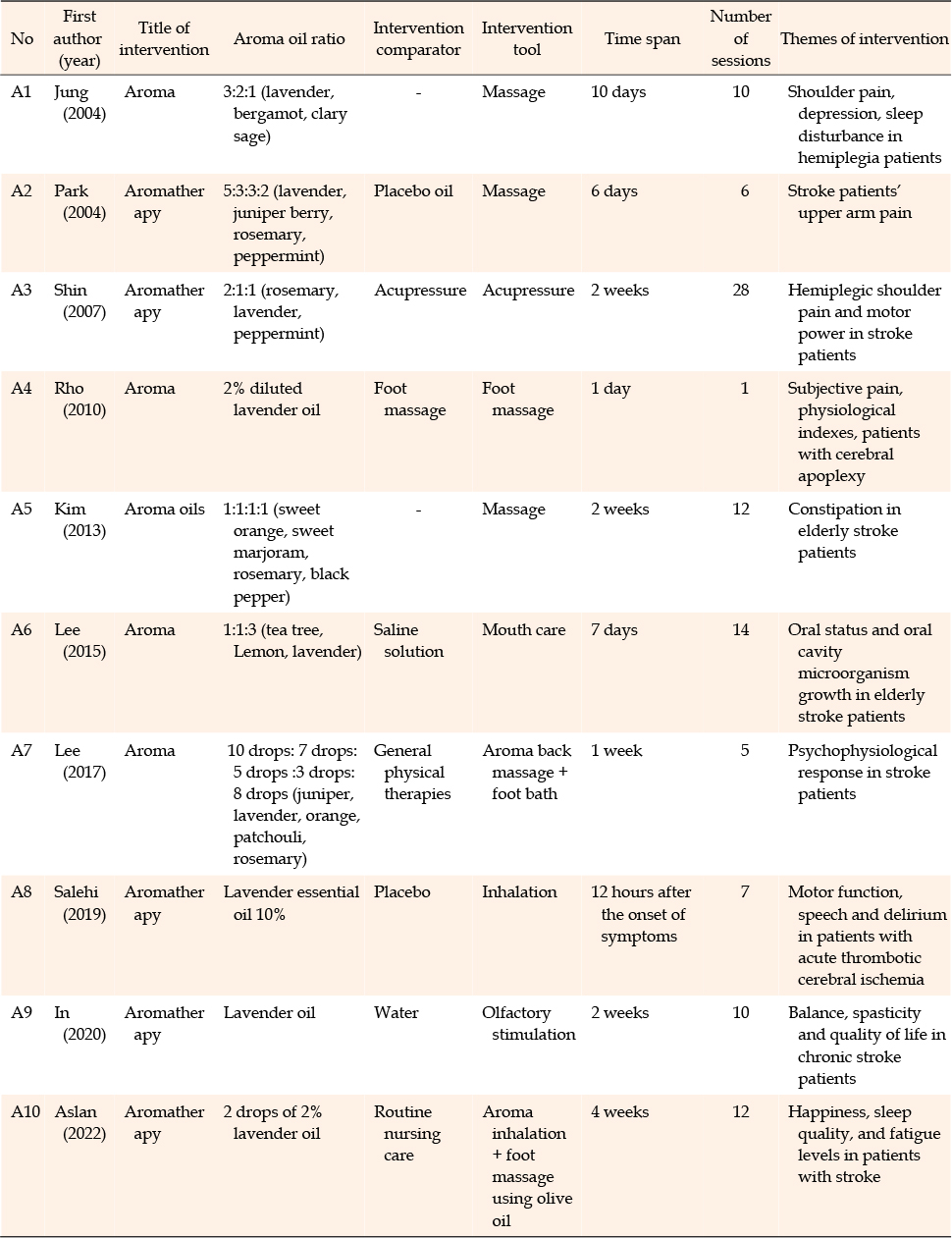
Table 2
Intervention Characteristics of Selected Studies
The studies designed to test the effectiveness of aromatherapy utilized several dependent variables. These included pain (A1-A4), constipation (A5), oral status (A6), motor power (A3), muscle strength (A8), spasticity and balance (A9), fatigue (A10), and various physiological variables. The physiological variables encompassed blood pressure, pulse, respiration (A4), body temperature (A7), blood cortisol levels (A4), oral microorganism growth (A6), blood antioxidants, and malondialdehyde (A8). Psychological outcomes were also measured, including stress, mood (A7), sleep satisfaction (A1,A7,A10), and happiness (A10). Cognitive outcomes were assessed as well, with a focus on speech and delirium (A8). Lastly, quality of life was evaluated (A9). In the 10 articles reviewed, pain was the most frequently assessed outcome, appearing in four articles (A1-A4). The measurement tools used for this variable were primarily the Visual Analogue Scale (VAS) (A1,A3,A4) (Table 3).
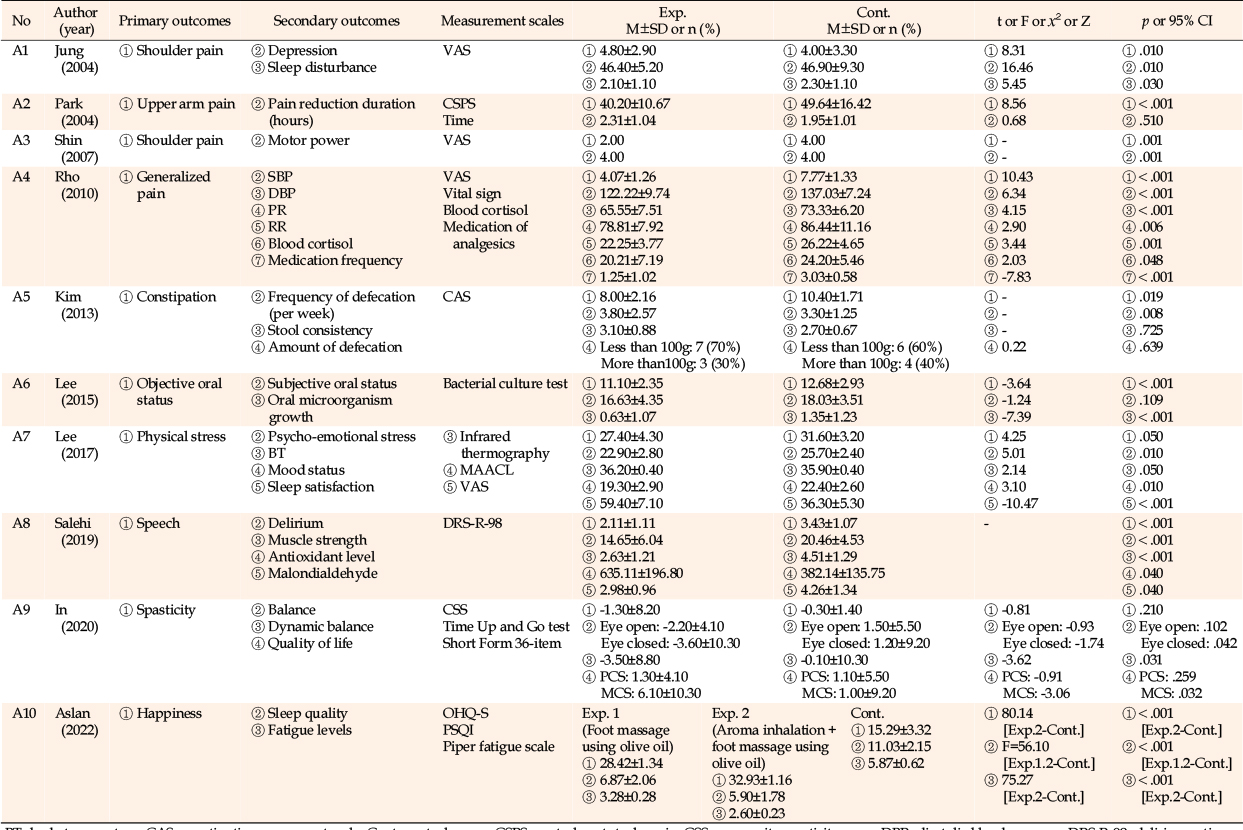
Table 3
Outcomes of Selected Studies
The aromatherapy interventions demonstrated a somewhat positive impact on the physical conditions of stroke patients. Notably, there were statistically significant differences (p<.001 to .01) in pain scores among the experimental groups that received either massage (A1,A2,A4) or acupressure (A3) with aroma oils (A1-A4). These scores were measured using the VAS (A1,A3,A4) and Central Stroke Pain Scale (CSPS) (A2) tools. Following an abdominal massage with aroma oil, there was a significant reduction in the constipation urge score to 8.00±2.16 (p=.019), and an increase in the frequency of defecation per week (p=.008) (A5). However, there were no significant differences in stool consistency (p=.725) and amount (p=.639) between the experimental and control groups (A5). In the case of oral care with an aroma solution (A6), the objective oral condition status significantly decreased to 11.10±2.35 (t=-3.64, p<.001). However, the subjective oral status score decreased to 16.63±4.35, which was not a significant difference (t=-1.24, p=.109). Significant post-intervention differences were observed in motor power (A3) and muscle strength (A8) variables in the study that used aromatic acupressure (A3) and aromatic inhalation (A8) (p=.001, p<.001). However, spasticity (A9) in another study that used aromatic inhalation (A9) did not significantly change from pre-intervention to post-intervention (Z=-0.81, p=.210). A significant difference was found in static balance, as measured by the Composite Spasticity Score (CSS) with eyes closed (Z=-1.74, p=.042), and dynamic balance, as measured by the Timed Up and Go (TUG) test with eyes closed (Z=-3.62, p=.031) (A9). Finally, fatigue measured after the aroma inhalation and foot massage using olive oil intervention was 2.60±0.23, which was statistically significant (p<.001) (A10) (Table 3).
Aroma oil foot massage was found to significantly reduce systolic blood pressure (p<.001), diastolic blood pressure (p<.001), pulse rate (p=.006), respiration rate (p=.001), and blood cortisol levels (p=.048) (A4). Conversely, aroma solution oral care (A6) led to a notable increase in the oral microorganism growth (p<.001). Additionally, inhaling aroma oil resulted in a significant increase in blood antioxidants (p=.040) and malondialdehyde (p=.040) (A8) (Table 3).
Statistically significant differences were observed in depression (p=.010) (A1), physical stress (t=4.25, p=.050) (A7), psycho-emotional stress (t=5.01, p=.010) (A5), mood status (t=3.10, p=.010) (A7), sleep disturbance (t=5.45, p=.030) (A1), and sleep satisfaction (t=-10.47, p<.001) (A7) as a result of the aroma massage intervention. The experimental group, which received aroma inhalation and foot massage, demonstrated significantly higher levels of happiness, as measured by the Oxford Happiness Questionnaire-Short form (OHQ-S) (χ2=80.14, p<.001), and sleep quality, as measured by the Pittsburgh Sleep Quality Index (PSQI) (F=56.10, p<.001), compared to the control group following the intervention (A10) (Table 3).
The aroma inhalation intervention resulted in a statistically significant reduction in both delirium (p<.001) and speech (p<.001), as measured by the Delirium Rating Scale-Revised-98 (DRS-R-98), when compared to the control group (A8) (Table 3).
The quality of life was assessed post-aroma inhalation intervention using the Short Form 36-item measurement tool (A9). No significant difference was observed between the two groups in the Physical Component Summary (PCS) (Z=-0.91, p=.259). However, the Mental Component Summary (MCS) was statistically significantly higher in comparison to the control group (Z=-3.06, p=.032) (Table 3).
Five Randomized Controlled Trials (RCTs) (A3,A7-A10) were evaluated using the ROB 2 tool, while five non-randomized studies (A1,A2,A4-A6) were evaluated using the ROBINS-I tool. The results were visualized using traffic light charts and bar charts in robvis, a tool for quality assessment visualization. The comprehensive assessment of the five RCTs using ROB 2 revealed a moderate risk of bias in the randomization order in two studies (A7,A9), a moderate risk of bias due to deviation from the intended intervention in one study (A7), a moderate risk of bias due to missing intervention outcome data in one study (A8), and a moderate risk of bias due to the selection of reported outcomes in one study (A7). The overall quality assessment of the five non-randomized studies using ROBINS-I resulted in two studies showing “very high” (A1,A5), one with “high” (A4), and two with “moderate” (A2,A6) ratings. Bias due to confounding was rated as “very high” for two studies (A1,A5), “high” for two (A4,A6), and “severe” for one (A2). Selection bias in the studies was rated as “no information” in one study (A5) and “low” in four studies (A1,A2,A4,A6). The bias for deviation from the intended intervention was rated as “very high” in two studies (A1,A5) and “severe” in one study (A4). The bias in the intervention outcome measures was rated as “severe” for three studies (A1,A4,A5) and “low” for two studies (A2,A6), and the bias in the selection of reported study outcomes was rated as “severe” for five studies (A1,A2,A4-A6) (Appendix 3).
Out of the 10 selected articles, four (A1-A4) identified pain as the most common outcome variable. Except for one article (A3) where the standard deviation was not provided, three articles (A1,A2,A4) with comparable pre- and post-intervention outcome values examined the effect size of aromatherapy on pain in stroke patients, involving a total of 112 patients. The Comprehensive Meta-Analysis V4 program was used to perform a statistical analysis of effect size and homogeneity. The heterogeneity analysis for the meta-analysis using a random-effect model revealed the following results: I2=92.0%, Q=25.06, p<.001. The overall effect size of the study was 1.85, with a 95% confidence interval ranging from 0.18 to 3.51. Based on Cohen's interpretation criteria, according to which a mean effect size of 0.2 or less indicates a small effect, 0.5 signifies a moderate effect, and 0.8 or more represents a large effect [25], the effect size of this study confirmed that the aromatherapy intervention significantly reduced pain in stroke patients (Figure 2).
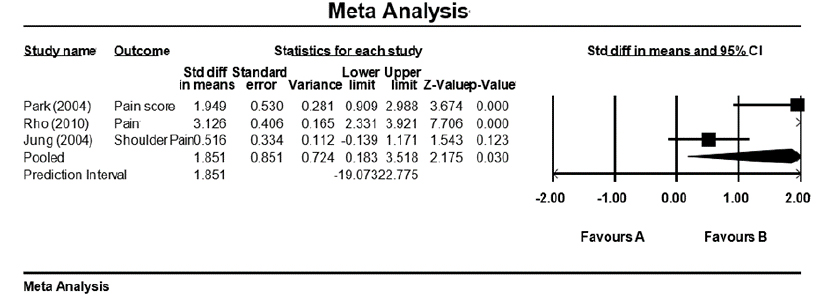
Figure 2
Forest plot of pain outcome.
Publication bias was assessed using a funnel plot. Despite the small sample size of the studies, which were distributed in the lower central region of the plot, the graph maintained a relatively symmetrical shape around the center line. This symmetry led us to conclude that no publication bias was present (Figure 3)
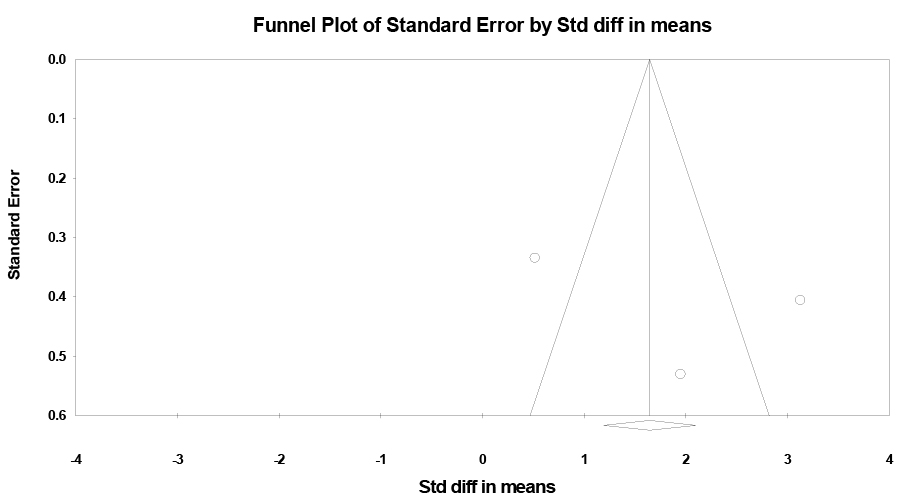
Figure 3
Funnel plot of standard error by standardized difference in means.
This systematic review and meta-analysis investigated the effectiveness of aromatherapy interventions in stroke patients, focusing on the impact on integrated health outcomes such as physical, physiological, psychological, cognitive, and quality of life aspects. The outcome variables employed in aromatherapy interventions for stroke patients encompassed a wide range, including pain, depression, sleep disturbance, motor and balance skills, constipation, oral health, psychological responses and mood, language, delirium, spasticity, quality of life, happiness, sleep quality, and fatigue. The majority of these variables showed positive effects. Physical health outcomes included pain and fatigue relief, an increased number of bowel movements per week, improved objective oral health, enhanced muscle strength and power, and improved static and dynamic balance. Physiological markers also showed positive effects, with improvements noted in blood pressure, pulse, respiration, blood cortisol, and blood antioxidant levels. In terms of psychological health, there was a reduction in depression and stress levels, a decrease in sleep disturbances, an increase in sleep quality and satisfaction, and a rise in happiness levels. Cognitive health improvements were also observed, with a decrease in delirium, an increase in language skills, and an enhancement in the quality of life as an integrated health outcome.
In terms of physical health, pain was the most frequently measured variable, in four studies (A1-A4), followed by sleep-related outcomes in three studies (A1,A7,A10). This study's meta-analysis of three studies (A1,A2,A4) confirmed the high efficacy of aromatherapy for pain relief. Among the interventions provided to stroke patients for pain relief, massage was the most common, featured in three studies (A1,A2,A4), with acupressure appearing in one study (A3). This suggests that skin-to-skin interventions are effective. The impact of aromatherapy on pain has been explored in other conditions as well, with aromatherapy shown to reduce pain in patients with knee osteoarthritis [26]. A study on foot massage using aromatic oils in older adults also found a statistically significant reduction in chronic pain in the experimental group compared to the control group [27]. Another study on patients with low back pain reported that aromatic oils were effective in reducing pain in patients who received acupressure [28]. This supports the notion that massage or acupressure with aromatic oils could be an alternative treatment for pain relief. Therefore, massage or acupressure with aromatic oils may have a positive effect on pain reduction in stroke patients and could be considered as a nursing intervention.
The most frequently utilized aromatic oil in pain management studies was lavender. In one study, it was used independently (A4), while in three other studies, it was part of a blend of three to four aromatic oils, including lavender (A1-A3). The aromatic oils used in these blends were lavender, juniper berry, rosemary, peppermint, bergamot, and clary sage. Lavender, an essential oil, is known for its analgesic, anti-inflammatory, antifungal, fungicidal, and antispasmodic properties. It is also recognized for its ability to soothe the nervous system, lower blood pressure, and alleviate anxiety and pain [7]. Past research has demonstrated that lavender essential oil can decrease the intensity of lower back pain [28], and its application has proven effective in reducing pain in mothers post-cesarean section [29]. Furthermore, a study involving patients undergoing breast biopsy found no difference in pain intensity or analgesia rates, but did report significantly higher satisfaction with pain management compared to the control group [30]. These findings endorse the use of lavender oil to alleviate pain and enhance satisfaction with pain management. Therefore, it can be suggested as a supplementary therapeutic intervention to mitigate pain in stroke patients. In a prior study, two-thirds of patients reported experiencing pain six months after a stroke diagnosis, with about half of these patients reporting the onset of new pain [31]. This persistent, uncontrolled pain, which can disrupt daily activities and rehabilitation, has the potential to not only delay recovery but also impact quality of life. Therefore, pain management in stroke patients is a crucial aspect of patient care and necessitates proactive clinical intervention.
Sleep, the second most commonly assessed variable, was evaluated through sleep disturbance, sleep satisfaction, and sleep quality. Although it was challenging to conduct a meta-analysis due to the varying measurement variables, three studies confirmed that aromatherapy reduced sleep disturbance, enhanced sleep satisfaction, and improved sleep quality. Given the high effectiveness of these individual outcomes, we can recommend aromatherapy for addressing sleep issues in stroke patients. The oils utilized in the interventions were solely lavender in the first study (A10), and a blend of three to five essential oils, including lavender, in the second study (A1,A7). All three studies used massage with aromatic oils as the intervention method, suggesting that massage with lavender may be a suitable aromatherapy approach for sleep problems in stroke patients. Prior research has indicated that inhalation therapy with aromatic oils improved sleep quality in patients with ischemic heart disease compared to a control group [32]. A meta-analysis reviewing the impact of aromatherapy on sleep quality in adults and older adults found that it enhanced sleep quality and alleviated stress, pain, anxiety, depression, and fatigue [33], corroborating the findings of this study. Many patients report sleep disturbances following hospitalization due to illness or environmental changes [34]. Stroke patients, in particular, report sleep issues such as sleep-related breathing disorders, wakefulness disturbances, and insomnia due to various environmental factors that arise post-hospitalization [35]. Sleep disorders in stroke patients can impact neurological, cognitive, and mental functions. Poor sleep quality and daytime fatigue can result in a poor prognosis during a period of intensive rehabilitation [35]. Therefore, it is crucial to pay attention to and actively address sleep disorders in stroke patients. While aromatherapy is effective in managing sleep disorders and can be actively recommended in clinical practice, further research is needed to establish the evidence before it can be implemented as a nursing intervention.
The most frequently used experimental interventions were dermal absorption via massage or acupressure (A1-A5,A7), followed by nasal inhalation (A8-A10), and absorption through the oral mucosa (A6). The duration of these interventions varied from as short as one day (A4) to as long as four weeks (A10). The number of experimental interventions also varied, ranging from one (A4) to 28 (A3), although most studies involved short-term applications of two weeks or less (A1-A9). Due to the varying intervention periods in the literature, this study was unable to meta-analyze the effect size by intervention period. Therefore, it is recommended that future studies be conducted to verify the effectiveness of the intervention period or to confirm the persistence of the effect through long-term follow-up studies. The strength of this study lies in its provision of comprehensive evidence supporting the use of aromatherapy as a nursing intervention for stroke patients, particularly in relation to pain and sleep. Furthermore, it is noteworthy that this study systematically reviewed and characterized the intervention methods and outcome variables of aromatherapy, thereby providing valuable data for planning nursing interventions to assist stroke patients and for selecting effective methods.
This study has several limitations. First, the 10 articles that were ultimately analyzed were published during a relatively long interval, between 2004 and 2022, highlighting the need for more early-stage interventions and research. Second, the inclusion of only two international studies and the predominance of domestic studies made it challenging to ascertain the status of aromatherapy interventions globally. Therefore, it is crucial to broaden the evidence base of aromatherapy to include more international studies. Third, the experimental sites were primarily hospitals, which are clinical settings for patients with stroke hemiparesis. This necessitates the validation of the intervention in other settings such as homes, rehabilitation hospitals, and nursing homes. Fourth, the study design comprised five randomized experimental studies and five quasi-experimental studies. More randomized experimental studies are needed to bolster the evidence regarding the effectiveness of aromatherapy. The quality assessment of the articles revealed that some had a high risk of bias, which calls for caution when generalizing the results of this study. Lastly, the meta-analysis in this study was limited to only three studies that allowed a comparison of pre-intervention and post-intervention outcome values for a common pain variable. As a result, other outcome variables were not meta-analyzed.
This study was undertaken to collect data supporting the use of aromatherapy as a suitable intervention for stroke patients. A meta-analysis was performed to identify the effect size on pain relief. The meta-analysis results indicated that aromatherapy effectively reduced pain, with an effect size of 1.85 for pain in stroke patients. The studies reviewed revealed positive impacts on physical, physiological, psychological, cognitive, and integrative health outcomes. Consequently, we advocate for the use of aromatherapy to alleviate pain and enhance health outcomes in stroke patients. We eagerly anticipate high-quality randomized controlled trials to support the clinical use of aromatherapy as a nursing intervention to improve stroke patients' health. In this study, the outcome variables were diverse and inconsistent across the literature, complicating a comprehensive confirmation of effects on identical variables. Therefore, it is essential to validate the effects of aromatherapy on pain in stroke patients in a replicated study, standardizing the type of essential oil, intervention method, duration, and number of sessions. This study is a meta-analysis of the effect size of aromatherapy on pain in stroke patients, anticipated to elevate the evidence level for aromatherapy interventions, offer guidance in clinical practice, and be actively employed as a nursing intervention for symptom relief.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - LAR and KHK.
Data collection - LAR and KHK.
Analysis and interpretation of the data - LAR and KHK.
Drafting and critical revision of the manuscript - LAR and KHK.
Funding acquisition - KHK.
This work was supported by the National Research Foundation of Korea (NRF) Grant funded by the Korea government (MIST) (No. RS-2023-00239284).

A1. Jung HM, Jeon YS. Effects of the aroma massage on shoulder pain, depression, sleep disturbance in hemiparesis patients. The Korean Journal of Rehabilitation Nursing. 2004;7(2):231-7.
A2. Park JE, Kim MA. A pilot study on the effect of aroma massage on stroke patients' upper arm pain. Clinical Nursing Research. 2004;10:184-95.
A3. Shin BC, Lee MS. Effects of aromatherapy acupressure on hemiplegic shoulder pain and motor power in stroke patients: a pilot study. The Journal of Alternative and Complementary Medicine. 2007;13(2):247-51. https://doi.org/10.1089/acm.2006.6189
A4. Rho HK, Kim KH, Choi MH, Kim JS. E. Effects of aroma foot relaxation massage on subjective pain and physiological indexes of patients with cerebral apoplexy. Journal of the Korean Data Analysis Society. 2010;12(6B):3087-101.
A5. Kim YG, Bae HS. The effect of abdominal massage with aroma oils on constipation in elderly stroke patients. Asian Journal of Beauty and Cosmetology. 2013;11(5):883-90.
A6. Lee EH, Park HJ. Effects of special mouth care with an aroma solution on oral status and oral cavity microorganism growth in elderly stroke patients. Journal Korean Academy Nursing. 2015;45(1):46-53. https://doi.org/10.4040/jkan.2015.45.1.46
A7. Lee JH, Seo EK, Shim JS. The effects of aroma massage and foot bath on psychophysiological response in stroke patients. Journal of Physical Therapy Science. 2017;29(8):1292-6. https://doi.org/10.1589/jpts.29.1292
A8. Salehi SS, Lorigooini Z, Jivad N, Ghadimi K. Effect of aromatherapy with lavender 10% essential oil on motor function, speech and delirium in patients with acute thrombotic cerebral ischemia. Caspian Journal of Neurological Sciences. 2019; 5(2):49-55. https://doi.org/10.32598/CJNS.5.17.49
A9. In TS, Kin HK. Effect of olfactory stimulation on balance, spasticity and quality of life in chronic stroke patients. Journal of the Korea Entertainment Industry Association (JKEIA). 2020;14(3):403-10. https://doi.org/10.21184/jkeia.2020.4.14.3.403
A10. Aslan KSU, Altin S. Aromatherapy and foot massage on happiness, sleep quality, and fatigue levels in patients with stroke: a randomized controlled trial. European Journal of Integrative Medicine. 2022;54:102164. https://doi.org/10.1016/j.eujim.2022.102164


 E-SUBMISSION
E-SUBMISSION