
Purpose
The purpose of this study was to investigate the impacts of digital literacy, attitudes towards internet health information, and e-health literacy on health promotion behavior among adults.
Methods
A cross-sectional survey design was used. Data were collected from 260 adults aged 19 and older from two provinces. Data were collected from September 1 to 22, 2020. The data were analyzed using descriptive statistics, the independent t-test, one-way analysis of variance, Pearson correlation coefficients, and hierarchical multiple regression analysis.
Results
Hierarchic multiple regression analysis was conducted to evaluate the impact of the analyzed variables on participants' health promotion progress older age, better self-perceived health status, frequency of exercise (≥3/week), frequency of exercise (1~2/week), higher digital literacy scores, and no smoking history were associated with a higher degree of health promotion behavior, with an explanatory power of 37.0%.
Conclusion
Based on these results, in order to improve health promotion behavior in adults, it is necessary to pay more attention to younger people, those who do not exercise regularly, and smokers. In particular, as digital literacy was found to be a factor influencing health promotion behavior in adults, it is necessary to consider strategies that are tailored towards improving digital literacy in adults from all age groups and to conduct systematic education on digital devices.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
The purpose of this study was to investigate the impacts of digital literacy, attitudes towards internet health information, and e-health literacy on health promotion behavior among adults.
A cross-sectional survey design was used. Data were collected from 260 adults aged 19 and older from two provinces. Data were collected from September 1 to 22, 2020. The data were analyzed using descriptive statistics, the independent t-test, one-way analysis of variance, Pearson correlation coefficients, and hierarchical multiple regression analysis.
Hierarchic multiple regression analysis was conducted to evaluate the impact of the analyzed variables on participants' health promotion progress older age, better self-perceived health status, frequency of exercise (≥3/week), frequency of exercise (1~2/week), higher digital literacy scores, and no smoking history were associated with a higher degree of health promotion behavior, with an explanatory power of 37.0%.
Based on these results, in order to improve health promotion behavior in adults, it is necessary to pay more attention to younger people, those who do not exercise regularly, and smokers. In particular, as digital literacy was found to be a factor influencing health promotion behavior in adults, it is necessary to consider strategies that are tailored towards improving digital literacy in adults from all age groups and to conduct systematic education on digital devices.
As the health paradigm has shifted from a disease-centered to a prevention-centered approach, the focus of healthcare policies has also transitioned from treatment to prevention, reflecting an increasing interest in managing chronic diseases as society ages [1]. The prevalence of adult diseases, such as diabetes and hypertension, continues to rise among both young adults and the elderly, with the majority of diseases now trending towards chronic conditions across all age groups [2]. One-third of Korean citizens suffer from chronic diseases, and the proportion of medical expenses dedicated to managing these conditions has grown from 26.8% of total medical costs in 2003 to 41.0% in 2017 [3]. Furthermore, seven of the top 10 causes of death are chronic diseases, which account for 79.8% of all deaths [3]. This underscores the increasing need for health-promoting behaviors, such as adopting proper lifestyle habits and health practices throughout adulthood, to prevent chronic diseases [4].
Health Promotion Behavior (HPB) refers to active participation in disease treatment and management, harmonized with positive emotional states and attitudes towards life, all aimed at maintaining and enhancing health conditions. These behaviors can be enhanced when they are incorporated into a healthy lifestyle over the course of a lifetime, potentially leading to improved health outcomes [4]. It is crucial to investigate various factors associated with HPB to enhance the health behaviors of young adults, who are beginning to lead independent lives, as well as those older than them. In order to stay relevant in the digital age, the relationship between these factors and HPB must be examined, and strategies for boosting HPB need to be developed.
The fourth industrial revolution and advancements in information technology have led to the widespread application of digital technologies in various aspects of our lives [5]. This shift has underscored the importance of Information & Communication Technology (ICT) in the contact-free environment necessitated by Coronavirus Disease 2019 (COVID-19), and the digital competency of individuals is becoming increasingly crucial. Moreover, the use of online health information services has significantly influenced individual health behaviors [6], bringing the concept of digital literacy to the forefront as a potential solution [7]. Digital literacy refers to an individual's ability to critically understand and interpret digital content, based on their skills and knowledge of ICT [2, 8]. In today's society, people of all ages have unrestricted access to online information through various means, such as smartphones. As such, digital literacy in managing online information is expected to influence how individuals apply and implement health-related information. Indeed, there are concerns about varying interpretations of health-related information due to differing levels of individual digital literacy [9]. A study involving 2,115 adults in Japan examined the correlation between digital literacy and health behaviors. The results showed that those with higher levels of digital literacy exhibited more positive health behaviors than those with lower levels [9]. However, the study also highlighted a lack of research on the correlation between digital literacy and health behaviors [9]. Therefore, exploring how digital literacy impacts the HPB of adults is a worthwhile endeavor.
While a multitude of factors influence HPB, one aspect worth investigating in the digital age is Attitudes toward Internet Health Information (AtIHI) [6]. AtIHI refers to an individual's perception or belief about the vast array of health information available online, which can impact people's health [10]. Generally, attitudes are known to shape behaviors, a concept that also applies to HPB. Ajzen and Fishbein's theory of reasoned action posits attitude as a crucial variable in altering health behaviors [11]. When individuals who utilize health information maintain a positive attitude toward online health information, it encourages them to continue seeking such information [8]. This, in turn, strengthens their initiative to actually implement health behaviors [10]. The recent expansion of the online environment has made accessing health information more convenient. Therefore, it is timely to explore the correlation between digital-related variables, including AtIHI, and HPB.
Another important concept in the relationship between internet information and health is e-Health literacy (eHEALS) [5]. eHEALS is defined as the capacity to locate, comprehend, and evaluate health information, extending beyond the realm of digital literacy. It also includes the ability to apply the health information obtained to health issues and resolve them [12]. The current widespread use of eHEALS can be seen as an expansion of the ability to understand health information within the framework of digital technology [13]. Digital literacy is a multifaceted concept that includes cognitive, physical, social, and emotional skills needed to adapt and respond appropriately to the digital environment. It involves sharing and applying information and knowledge, as well as freely expressing opinions on digital platforms. Conversely, eHEALS pertains to the ability to seek out health information, locate, understand, evaluate, and apply health information online, and use digital applications related to health management [13]. It is a concept distinct from digital literacy [12]. A prior study found that individuals with lower levels of digital literacy had a reduced ability to apply, understand, and disseminate medical information, which impacted their HPB [14]. Another study involving older participants found that younger age and higher education levels were associated with a greater likelihood of making health-related decisions based on health information obtained from the internet [15]. Given the increasing role of the internet as a primary source of health information in today's world, people are easily exposed to a vast amount of health information of varying quality [6]. It is crucial to locate and apply accurate health information, as the use of incorrect health information in healthcare settings can lead to serious health issues [16]. In this context, eHEALS is anticipated to have a correlation with HPB.
Much of the existing research on adult HPB and the use of digital information has focused on the individual characteristics, emotions, and behaviors of adolescent and elderly participants [17, 18]. However, there is a noticeable lack of studies involving adults across all age groups. Furthermore, no research has been conducted on the correlation between digital literacy, AtIHI, eHEALS, and HPB in adults. This study, therefore, sought to examine the levels of digital literacy, AtIHI, eHEALS, and HPB, and to identify the factors influencing adult HPB. The findings are anticipated to provide the foundational data necessary for developing strategies to enhance the HPB of adults in Korea.
Therefore, this study explored the levels of digital literacy, AtIHI, eHEALS, and HPB, and investigated differences in HPB according to the general characteristics of adults and digital equipment. In addition, it aimed to identify their relationships and ultimately identify factors affecting HPB in adults.
This cross-sectional survey study aimed to investigate the impact of digital literacy, AtIHI, and eHEALS on the HPB of adults.
This study involved adult participants aged 19 and above, residing in J City of C Province and W City of G Province. Participants were required to understand the study's objective, agree to participate, and independently read and comprehend the questionnaire. Individuals with cognitive impairments such as dementia or mild cognitive impairment were excluded from the study. It is important to consider multi-level factors by lifecycle when developing digital-related health management services. In line with the theory of human development developed by Levinson et al. [19], which categorizes a person's life from conception to death into early, midlife, and late adulthood stages, the participants in this study were grouped accordingly. Those aged 19 to less than 44 were classified as early adulthood stage, those aged 45 to less than 65 as middle adulthood stage, and those aged 65 and above as late adulthood stage, with the elderly included in this group. A sample size of 217 was determined using G*Power 3.1.9.4, with a confidence level (α) of .05, a test power (1-β) of .95, a medium effect size of 0.15, and 19 predictor variables (12 items of general characteristics, 4 items of digital device-related characteristics, and 3 independent variables). The medium effect size was established based on a previous study [20]. A total of 260 participants were conveniently sampled, accounting for a projected dropout rate of 20% due to COVID-19. The questionnaires were distributed offline, and as there were no omitted answers in any of the 260 collected questionnaires, all were included in the final analysis, representing a 100% response rate.
Twelve items elicited information on participants' general characteristics: gender, age, education level, spouse, occupation, self-perceived socio-economic status, alcohol drinking, smoking history, frequency of exercise, self-perceived health status, previously diagnosed diseases, and current diseases under treatment.
The characteristics of digital devices were analyzed in terms of the recent period of computer usage, the recent period of internet usage, the duration of internet usage, and the average daily internet usage. These four components are derived from five questionnaire items about device usage that were utilized in a previous study [20].
For digital literacy, Kim and Jeon's [20] Korean translation of "Digital Literacy toward ICT for Learning," a tool developed by Ng [21] for laborers, was used after revision. Kim and Jeon's [20] tool consists of 10 items across three domains: technical (6 items), cognitive (2 items), and social-emotional (2 items). However, the item "I often get help from my friends for assignments through the internet (e.g., Skype, Facebook, and blogs)" from the social-emotional domain was excluded, as it was deemed relevant only to students. Consequently, a total of 9 items were used, including 6 from the technical domain, 2 from the cognitive domain, and 1 from the social-emotional domain. Four experts, specifically two nursing informatics professors and two adult nursing professors, assigned an Item-level Content Validity Index (I-CVI) score of .95 to all items in the tool, following the removal of one item. The tool employs a 5-point Likert scale, ranging from 1 point for "strongly disagree" to 5 points for "strongly agree." The total score can range from a minimum of 9 points to a maximum of 45 points, with a higher score indicating a higher level of digital literacy. Cronbach's α as an indicator of the tool's reliability, was .89 in Ng's study [21], .87 in Kim and Jeon's study [20], and .94 in this study.
AtIHI was measured using a tool developed by Kim et al. [8] based on the model of internet health information seeking proposed by Noh et al. [10] for adults. This model reflects an individual's attitude towards internet health information. According to a study by Kim et al. [8], the model consists of 12 items in total: perceived usefulness (3 items), perceived ease of use (3 items), information reliability (3 items), and information utilization of internet health information (3 items). The tool employs a 5-point Likert scale, ranging from 1 point for "strongly disagree" to 5 points for "strongly agree". The total score can range from a minimum of 12 points to a maximum of 60 points, with a higher score indicating a more positive attitude towards internet health information. In the study of Noh et al. [10], the Cronbach's α for the reliability of the tool was.82 for perceived usefulness, .78 for perceived ease of use,.85 for information reliability, and .75 for information utilization. The total reliability was not presented at the time of development. In contrast, the total Cronbach's α in the study of Kim et al. [8], which utilized this tool, was.90. In the current study, the Cronbach's α was .91 for perceived usefulness, .94 for perceived ease of use, .91 for information reliability, and .88 for information utilization, with a total Cronbach's α of .94.
We utilized the Korean e-Health Literacy Scale (KeHEALS), a Korean translation by Chang et al. [22] of Norman and Skinner's eHEALS tool, which has been validated [12]. The eHEALS tool comprises 10 items, but the final two items, which inquire about the significance and utility of the internet in making health-related decisions, are not factored into the scoring process as they serve as supplementary questions regarding the participant's interest in using internet health information [12]. The scoring process includes eight items that assess the ability, evaluation, knowledge, and use of internet health information. These items are scored on a 5-point Likert scale, ranging from 1 point for "strongly disagree" to 5 points for "strongly agree." The minimum score is 8 points, the maximum is 40, and a higher score indicates a higher level of eHEALS. The reliability of the tool, as measured by Cronbach's α was .88 in Norman and Skinner's study [12], .89 in the study of Chang et al. [22], and .96 in this study.
HPB were measured using the Health Promoting Lifestyle Profile-II (HPLP-II) tool developed by Walker et al. [23] and adapted by Yun and Kim [24]. This tool comprises 52 items across six categories: interpersonal support, spiritual growth, nutrition, health responsibility, stress management, and exercise, with nine items each for the first four categories and eight items each for the last two. Each item is scored on a 4-point Likert scale, where 1 point signifies "never" and 4 points signify "always." The total score can range from a minimum of 52 to a maximum of 208, with higher scores indicating a higher level of HPB. When the measurement tool was initially developed by Walker et al. [23], Cronbach's α was .92. It was .91 in the study by Yun and Kim [24], and .95 in this study.
Data for this study were collected from September 1 to September 22, 2022. The decision was made to conduct the survey offline, as it was anticipated that conducting it online could skew the results by favoring participants with easier internet access. Given the global prevalence of COVID-19, data were collected from regions in Korea with few or no confirmed cases of the virus. Individual surveys were administered after participants had used hand sanitizer and donned masks to mitigate the risk of COVID-19 transmission, all while maintaining social distancing.
Data were collected by the research team, which included both researchers and research assistants, at various locations such as hospitals (Administrative Unit), libraries, banks, community centers, churches, supermarkets, and fitness centers. Prior to conducting the survey, permission was obtained from the relevant authority at each public office. The purpose and procedure of the study, as well as the estimated time required to complete the questionnaire, were clearly explained to potential adult participants. Written consent was then obtained from those who voluntarily agreed to participate in the survey. Participants completed the survey items themselves. If they had any questions or needed assistance while filling out the survey, the researchers or research assistants were on hand to provide help. After the questionnaires were collected, they were checked for any omitted items. If any omissions were found, the participants were asked to complete the missing items. On average, the survey took about 20 minutes to complete.
Data were analyzed using SPSS for Windows version 25.0 (IBM Corp., Armonk, NY, USA). The general characteristics of the participants and the characteristics of digital devices were analyzed using mean, standard deviation, frequency, and percentages. The participants' digital literacy, AtIHI, eHEALS, and HPB were also analyzed using means and standard deviations. The normality of all variables was assessed using skewness and kurtosis. Differences in HPB, based on the general characteristics of the participants and the characteristics of the digital devices, were analyzed using the independent t-test and one-way analysis of variance.
The Scheffé test was performed for post-hoc analysis. Correlations between the participants' digital literacy, AtIHI, eHEALS, and HPB were analyzed using Pearson's correlation coefficients. Hierarchical multiple regression analysis was conducted to investigate the effects on HPB.
Data were collected following the review and approval of the study's protocol and questionnaire (GWNUIRB-2020-12) by the Institutional Review Board (IRB) of G University. The instruments utilized in the study were used with permission, obtained via email, from the original authors. Participants provided written consent after reading an offline information sheet detailing the study's purpose, personal information protection measures, and their right to withdraw from the study at any point, even after giving consent. It was explicitly stated that they could withdraw their participation at any time if they no longer wished to be involved in the study, regardless of prior consent. Furthermore, all collected data were anonymized to ensure they could only be used for research purposes. Each questionnaire was also encoded for additional security. All study-related data will be securely stored in a locked cabinet for three years post-analysis, after which it will be responsibly discarded. As a token of appreciation for their participation, each participant received a reward valued at 5,000 KRW.
The study included 131 men (50.4%) and 129 women (49.6%). The average age was 50.03 (±16.70), with the majority (44.2%) being between 19 and 45 years old. The majority of participants (n=170; 65.4%) had a spouse, making up the majority. In terms of education, 116 participants (44.6%) held university graduate degrees, which was the largest proportion. As for occupation, 90 participants (34.6%) were office workers or professionals. A total of 168 participants (64.6%) self-identified as middle class, which was the largest socio-economic group. There were 118 participants (45.4%) who reported not drinking alcohol at all, and 155 participants (59.6%) who reported never smoking. Regarding exercise frequency, 105 participants (40.4%) exercised 1~2 times per week. In terms of self-perceived health status, 137 participants (52.7%) considered themselves to be in moderate health, followed by 69 (26.5%) who considered themselves healthy, and 54 (20.8%) who considered themselves unhealthy. When asked about previously diagnosed diseases, 172 participants (66.2%) reported none, which was the largest proportion. Similarly, for diseases currently under treatment, the majority, 186 participants (71.5%), reported none. Regarding digital device usage, 157 participants (60.4%) reported using a computer within the last week, and 221 (85.0%) reported using the internet within the same period. When asked about total internet usage, 124 participants (47.7%) reported using the internet for 20 or more years. For average daily internet usage, 124 participants (47.7%) reported 1 to less than 3 hours, which was the largest proportion (Table 1).
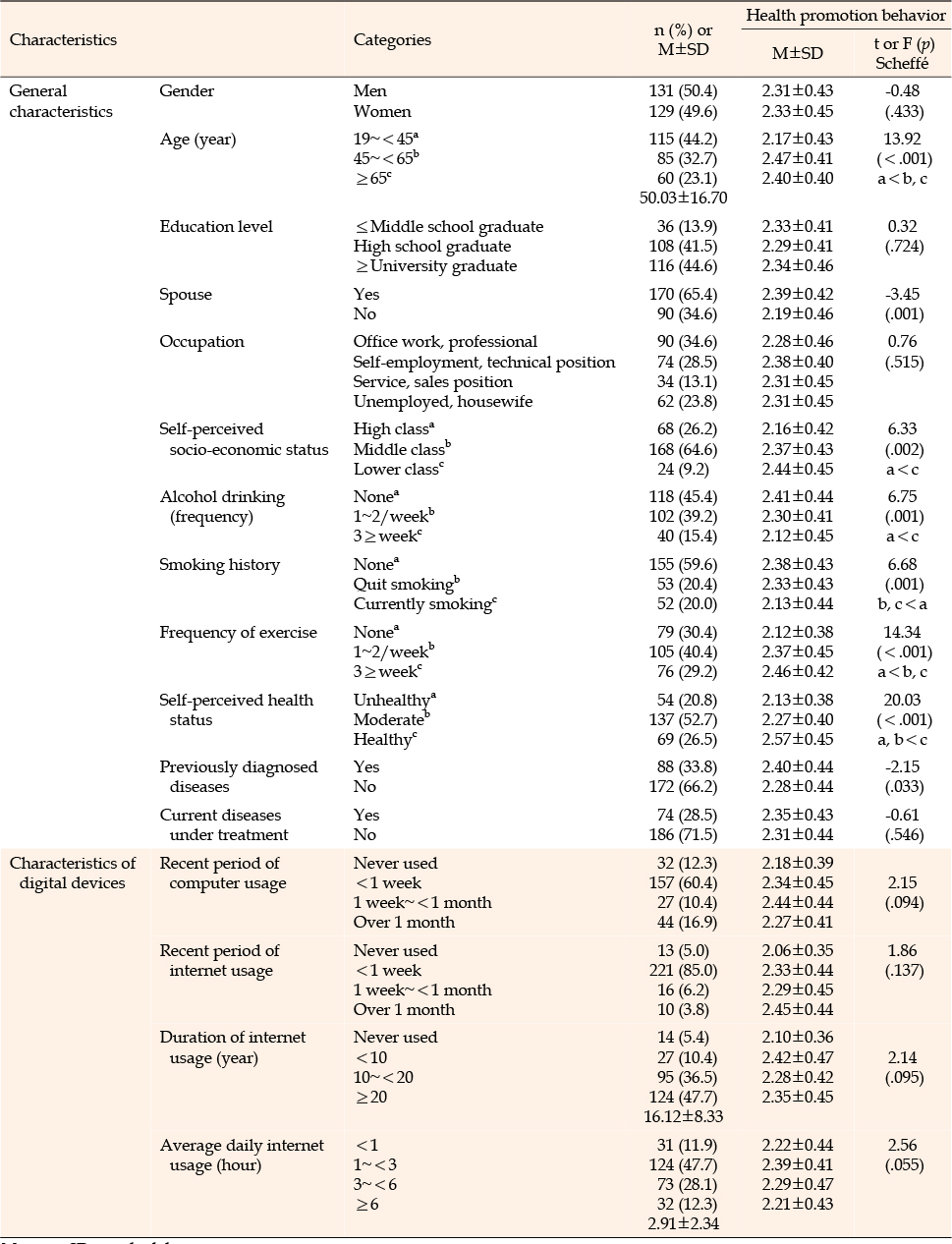
Table 1
Levels of Health Promotion Behavior according to the Characteristics of the Subjects and Digital Devices (N=260)
The mean score for the digital literacy of the participants was 2.83±0.81 out of 5. The cognitive domain scored 2.89±0.95, followed by the social-emotional domain at 2.85±1.12, and the technical domain at 2.80±0.80. The AtIHI scored 3.28±0.75 on a scale of 5, with the perceived ease of use achieving the highest score of 3.56±0.97, and information reliability scoring the lowest at 3.04±0.76. The eHEALS score was 3.19±0.78 on a scale of 5. The average HPB score for the participants was 2.32±0.44 on a scale of 4. The sub-factor scores were as follows: Interpersonal support scored 2.64±0.49, followed by spiritual development at 2.45±0.58, nutrition at 2.34±0.58, stress management at 2.26±0.50, health responsibility at 2.10±0.52, and exercise at 2.10±0.65 (Table 2).
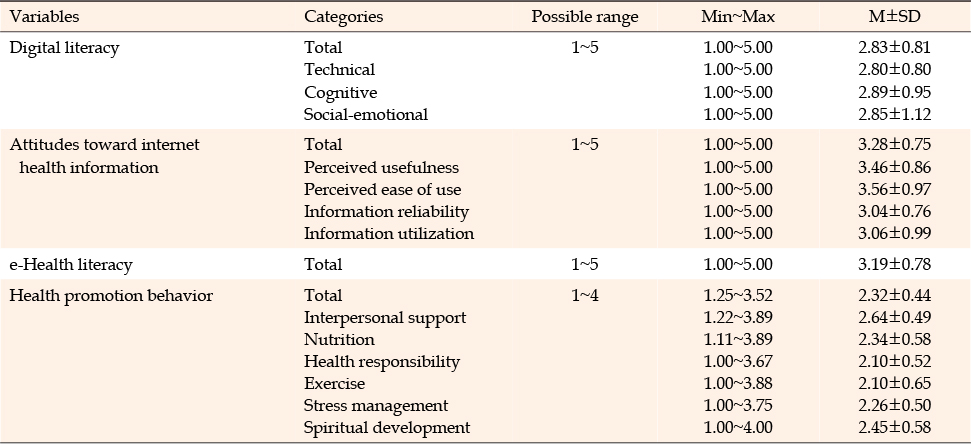
Table 2
Scores of Digital Literacy, Attitude towards Internet Health Information, e-Health Literacy, and Health Promotion Behavior (N=260)
HPB showed significant differences according to age (F=13.92, p<.001), spouse (t=-3.45, p=.001), self-perceived socio-economic status (F=6.33, p=.002), alcohol drinking (F=6.75, p=.001), smoking history (F=6.68, p=.001), the frequency of exercise (F=14.34, p<.001), self-perceived health status (F=20.03, p<.001), and previously diagnosed diseases (t=-2.15, p=.033). The post-hoc test revealed that participants aged 45 and above had higher HPB scores than those under 45. Participants with a lower self-perceived socio-economic status had higher HPB scores than those with a higher self-perceived socio-economic status. In terms of alcohol consumption, non-drinkers had higher HPB scores than those who consumed alcohol three or more times per week. Non-smokers had higher HPB scores than smokers, and regular exercisers had higher HPB scores than non-exercisers. Regarding self-rated health status, those who rated their health status as high had higher HPB scores than those who did not. However, no significant differences were observed in HPB scores based on the characteristics of the participants' digital devices (Table 1).
HPB had significant positive correlations with digital literacy (r=.22, p<.001), AtIHI (r=.22, p<.001), and eHEALS (r=.25, p<.001) (Table 3).
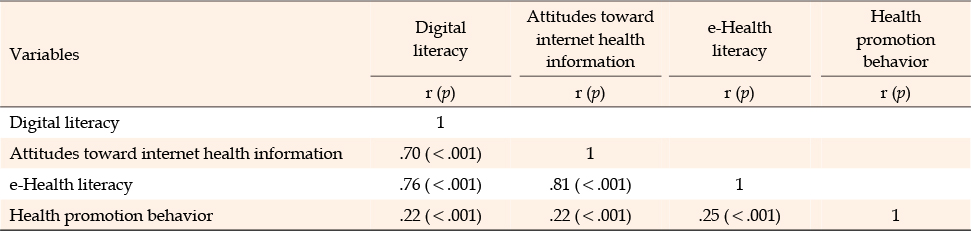
Table 3
Correlations between Digital Literacy, Attitude towards Internet Health Information, e-Health Literacy, and Health Promotion Behavior (N=260)
To identify the factors influencing the participants' HPB, we treated the following eight variables as controls: age, spouse (yes), self-perceived socio-economic status (either high class or middle class), frequency of alcohol drinking (either none or 1~2/week), smoking history (either none or quit smoking), frequency of exercise (either 1~2/week or≥3/week), self-perceived health status (either healthy or moderate), and previously diagnosed diseases (yes). All variables, with the exception of age, were transformed into dummy variables and incorporated into the stage 1 multiple regression analysis. Furthermore, digital literacy, AtIHI, and eHEALS, which showed a significant correlation with HPB, were additionally included in stage 2, and a hierarchical multiple regression analysis was performed.
Before testing the regression models, multicollinearity was examined. The tolerance of Model 1 was found to be 0.1 or higher, specifically ranging from 0.66 to 0.95. Its Variance Inflation Factor (VIF) was between 1.06 and 1.51, which did not surpass the reference value of 10. This indicates that there was no issue of multicollinearity. Similarly, the tolerance of Model 2 was 0.1 or higher, with a range from 0.26 to 0.93. The VIF for this model was between 1.08 and 3.91, which also did not exceed the reference value of 10, suggesting that there was no multicollinearity problem with the data. Furthermore, a residual analysis was conducted, revealing that the Durbin-Watson test statistic was 1.89, a value close to 2. This suggests that there was no autocorrelation problem among the model errors. Consequently, the assumption of a normal distribution of the residuals was satisfied.
The regression model of Model 1 was statistically significant (F=8.29, p<.001), and among the general variables entered in stage 1, self-perceived health status (healthy) (β=.33, p<.001), the frequency of exercise (≥3/week) (β=-.21, p=.002), the frequency of exercise (1~2/week) (β=-.20, p=.003), and smoking history (none) (β=.18, p=.016) explained 27% of variance in HPB.
Model 2's regression model was also statistically significant (F=10.63, p<.001), accounting for 37.0% of variance in HPB, which was a 10.0 percentage point increase in explanatory power compared to Model 1. The most significant factor influencing the participants' HPB was age (β=.28, p<.001), followed by self-perceived health status (healthy) (β=.26, p<.001), frequency of exercise (≥3/week) (β=.24, p<.001), frequency of exercise (1~2/week) (β=.21, p=.001), digital literacy (β=.19, p=.022), and smoking history (none) (β=.17, p=.011). Among these factors, age had the most significant impact on HPB. In other words, a higher HPB level was associated with older age, better self-perceived health status, exercising 3 times or more a week or 1~2 times a week as opposed to not exercising, higher digital literacy, and no smoking history (Table 4).
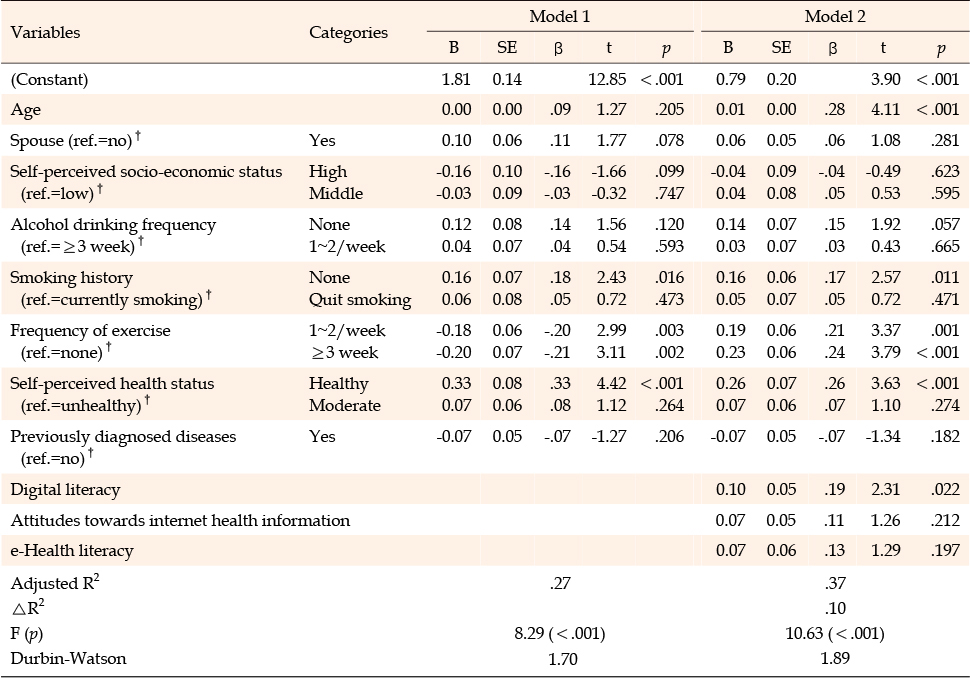
Table 4
Factors Influencing Health Promotion Behavior (N=260)
This study investigated digital literacy, AtIHI, eHEALS, and HPB among adults and aimed to identify the factors that affect HPB. In this study, the HPB score was 2.32 out of 4, falling around the midpoint. This score is comparable to that found by Lee et al. [14], which examined the effects on the HPB of adults aged 20 to 50. The results of both studies indicated that interpersonal support received the highest score, while exercise received the lowest. However, our score was slightly higher than the 2.22 points reported by Hong et al. [25], whose study involved adults aged 18 and older. A commonality among these three studies, including ours, is that the participants were all from regions outside of metropolitan areas. The average age of the participants in our study was 50.03 years. Of these, 44.2% were aged 19 to 45, 32.7% were 45 to 65, and 23.1% were over 65 years old. In contrast, Lee et al. [14] reported that 24.6% of the participants were in their 20s, 24.0% in their 30s, 33.2% in their 40s, 17.9% in their 50s, with no participants in late adulthood (the elderly). In the study of Hong et al. [25], 45.5% of participants were aged 18 to 39, 51.8% were aged 40 to 59, and 2.7% were aged 60 and above, indicating a relatively small number of participants in late adulthood. Interestingly, a higher age correlated with a significantly higher HPB, a finding that aligns with other studies [13, 25]. In other words, despite a higher self-perceived health status correlating with a lower frequency of HPB, interest in health tends to increase with age. The elderly, in particular, show a high level of interest in their health compared to other age groups and demonstrate a strong willingness to engage in HPB [26]. This is thought to reflect the findings mentioned above. However, the HPB score of community-dwelling adults was lower than the 3.68 points [27] reported in a study conducted with nurses at medium to small-sized hospitals. It has been suggested that individuals who frequently use health information or show a high interest in it tend to exhibit better health behaviors than those who do not, as they possess more disease-related information [28]. Therefore, the HPB level of the general adult population in this study is considered lower than that of nurses. The HPB score in this study equates to 58 out of 100, which is on the lower side. Given that HPB is a concept that includes interpersonal support, spiritual growth, nutrition, health responsibility, stress management, and exercise [23], there is a clear need for improvement in the HPB of adults.
This study found a correlation between adult HPB and digital literacy, AtIHI, and eHEALS. Hierarchical regression analysis revealed that higher age, improved self-perceived health status, more frequent weekly exercise, increased digital literacy scores, and a shorter history of smoking were all associated with higher levels of HPB. As individuals age, they often become more health-conscious and face an increased risk of chronic diseases [28]. Therefore, active implementation of HPB is necessary, and the correlation between higher age and higher levels of HPB observed in this study is seen as a positive outcome. The study also found that self-perceived health status influenced the level of HPB, a finding that aligns with the results of Lee et al. [14]. Furthermore, research on the self-perceived health status and HPB of university students indicated that students who view themselves as healthy are more likely to engage in HPB. There was a significant positive correlation between the self-perceived health status of university students and HPB [29]. This is thought to be due to the fact that a higher self-perceived health status leads to more positive attitudes towards health [30], resulting in more frequent HPB. Given that regular exercise is a form of HPB, it is unsurprising that it is a contributing factor. Similar findings were reported in studies conducted with Public Health university students, who are frequently exposed to health-related information [31], and with university students in general [32]. Since changes in HPB often begin with exercise [30], strategies should be developed to encourage adults to consistently engage in HPB, starting with regular exercise habits.
The most striking finding from this study is that digital literacy emerged as the primary factor influencing the HPB of adults. The participants' level of digital literacy was measured at 2.83 out of 5 points. When broken down by age, participants aged 19 to 45 scored 3.10, those aged 45~65 scored 2.91, and those aged 65 and above scored 2.17. The digital literacy score was statistically significantly higher in participants under 65 years of age than in those aged 65 and above. This aligns with another study's findings [5] that age is as influential as income level in determining digital literacy. Among studies that utilized the same measurement tool, Kim and Jeon's study [20] with university students reported a score of 3.36 points. Kim's study [33] with nurses reported scores of 3.70 for participants aged 20 to 29, 3.62 for those aged 30~39, and 3.42 for those aged 40 and above. These scores were all higher than those found in this study, likely due to the younger age of the participants in those studies. A study conducted with university students using a different measurement tool reported a score of 3.75 out of 5 points [34], and a study with elderly participants reported a score of 3.58 points [35]. Both of these scores were higher than those found in this study, but they varied by age. In other words, while the level of digital literacy may fluctuate depending on the measurement tool used, higher scores generally correspond to younger ages, with particularly low levels of digital literacy observed among the elderly. However, a study conducted with middle-aged workers found that the average level of digital literacy was higher than that of the younger group aged 20 to 30 [7]. Furthermore, the elderly aged 60 and above demonstrated higher literacy than adolescents in terms of information appraisal and understanding of medical properties [36]. This suggests that a higher age does not necessarily equate to lower digital literacy. While there are limitations to comparative analysis due to the scarcity of studies comparing the digital literacy of all age groups, it is important to note that a low level of digital literacy may negatively impact health management and health status [35]. Therefore, it is suggested that efforts to enhance the digital literacy of adults are necessary.
Digital literacy refers to the cognitive skills, attitudes, and abilities required to identify, engage with, manage, integrate, evaluate, analyze, and synthesize digital resources. The appropriate use of digital tools for communication and the creation and expression of new knowledge is also a key component of digital literacy [21]. A learner's level of digital literacy can significantly impact their learning, interaction, and communication using information and communication technologies [37]. It has been identified as a major factor influencing the eHEALS of nursing college students [20]. Furthermore, digital literacy has been shown to positively affect the learning process and outcomes by enhancing learners' self-efficacy [38]. However, this study appears to be the first to identify digital literacy as a variable that directly impacts HPB. In other words, it suggests that an individual's digital literacy will be a crucial factor for HPB in the future. Given this, it is necessary to develop programs and educational initiatives to enhance adults' digital literacy in the era of the fourth industrial revolution, where online informatization is rapidly advancing. This will enable them to identify, evaluate, and analyze the information they need from the vast amount of online information available, thereby enhancing their HPB [37]. It is important to note that the level of digital literacy can vary according to an adult's age and their specific circumstances. Therefore, education should be customized to cater to the needs of various adults. Some studies have reported that a person's attitude towards online learning can affect their digital literacy [20]. As such, improving attitudes towards online learning should be considered a key strategy for enhancing digital literacy.
On the contrary, it was observed that AtIHI or eHEALS do not directly influence HPB. In conclusion, the quality of information holds more significance than acquiring a vast amount of health information [6]. Even with proficient interpretation of health information from the internet, expert interventions are necessary to translate this information into actions, a task that exceeds their capabilities. While these variables did not directly impact adults' HPB, further studies are needed to determine if they indirectly affect it by influencing digital literacy.
This study yields meaningful findings as it involved adults from all age groups to measure the level of HPB, and it pinpointed the factors influencing HPB, particularly those reflecting the characteristics of informatization. Enhancing the HPB of adults, who constitute the majority of a nation's population, is directly linked to the country's future prosperity. As such, efforts to boost the HPB of adults, from those in early adulthood just entering society to those in late adulthood, should be undertaken not only at the individual level but also at the national level. In this regard, young adults, as well as those who do not regularly exercise or who smoke, require sustained attention and effort to encourage voluntary engagement in HPB, as suggested by this study's findings. A key insight from this study is the identification of digital literacy as a factor influencing adults' HPB. Consequently, there is a need for programs aimed at enhancing adults' digital literacy and for active education utilizing such programs, tailored to the specific characteristics of different adult age groups.
The limitations of this study are as follows. First, the study analyzed a convenience sample of 260 adults from two medium-sized to small cities, making it challenging to generalize the results to the entire adult population of Korea. Second, while the HPB tool used in this study was designed for adults, it primarily focuses on general, everyday health behaviors. As such, there is a need to develop a tool that measures HPB using internet health information. Third, this study, being cross-sectional, has limitations in identifying causal relationships. Therefore, these relationships should be explored through a longitudinal study. Fourth, the data were collected from various locations, and the researchers did not consider that participant characteristics might vary based on the data collection site. Therefore, future research should identify participant characteristics according to the data collection location and investigate any differences in HPB.
This descriptive survey study aimed to identify the effects of digital literacy, AtIHI, and eHEALS on the HPB of individuals in early, middle, and late adulthood. The study's findings indicate that increased age, improved self-perceived health status, regular exercise (either "3 times or more a week" or "1~2 times a week"), higher digital literacy scores, and a shorter history of smoking are all correlated with increased HPB in adults. Notably, digital literacy emerged as the primary factor influencing adult HPB. As such, particular attention should be given to those in early and middle adulthood, individuals who do not exercise regularly, and smokers to enhance adult HPB. Furthermore, strategies to boost adult digital literacy should be considered. To achieve this, it is recommended to develop age-differentiated educational programs and provide personalized education. The implementation of these efforts should not be left to individuals alone, but should be undertaken on a national level in a systematic manner.
Based on the findings of this study, we propose the following recommendations. First, to minimize the potential influence of regional characteristics on the results, future studies should employ randomized sampling to select adult participants from a variety of regions. This will necessitate repeated studies to ensure a diverse sample. Second, as part of the strategies to enhance the HPB of adults, we recommend conducting research to develop programs aimed at improving adults' digital literacy, taking into account their diverse characteristics. Third, to further improve the HPB of adults, it is important to focus on participants associated with the various factors identified in this study, such as young age, lack of exercise, and smoking habits. Studies that evaluate the effectiveness of HPB improvement programs specifically designed and implemented for these groups are also needed.
CONFLICTS OF INTEREST:Jaehee Jeon has been the Associate Editor of the Korean Journal of Adult Nursing since 2022. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - SHJ and JJH.
Data collection - SHJ.
Analysis and interpretation of the data - SHJ and JJH.
Drafting and critical revision of the manuscript - SHJ and JJH.
This study is an abbreviated version of the master's thesis of the first author HeeJin Shin.
 E-SUBMISSION
E-SUBMISSION