
Purpose
This study investigated the knowledge, performance, and barrier awareness of Intensive Care Unit (ICU) medical staff concerning the prevention and management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption (PADIS) in critically ill adult patients, and aimed to identify the factors influencing the performance of evidence-based PADIS management.
Methods
This cross-sectional and correlational study included 189 medical staff (17 physicians, 172 nurses) working in ICUs in two hospitals and recruited between July 13 and 31, 2022. Multiple linear regression analysis was performed to identify the factors associated with the PADIS-related performance of medical staff.
Results
The evidence-based performance level for PADIS prevention and management had a mean score of 3.55±0.37 out of 5 points, and the mean knowledge score was 28.23±3.00 out of 33 points. The mean awareness score for barriers to implementing PADIS prevention and management guidelines was 2.91±0.39 out of 5 points. Multiple regression analysis indicated that knowledge of delirium (β=.19, p=.014) and awareness of barriers within the individual domains of medical staff (β=-.20, p=.034) significantly influenced PADIS-related performance.
Conclusion
To implement evidence-based practices for the prevention and management of PADIS, steps should be taken to improve the knowledge and awareness of medical staff regarding PADIS. This could be improved through organizational support, such as systematic education and staffing. Specifically, an education program centered on delirium could significantly improve PADIS-related knowledge and performance.
This study investigated the knowledge, performance, and barrier awareness of Intensive Care Unit (ICU) medical staff concerning the prevention and management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption (PADIS) in critically ill adult patients, and aimed to identify the factors influencing the performance of evidence-based PADIS management.
This cross-sectional and correlational study included 189 medical staff (17 physicians, 172 nurses) working in ICUs in two hospitals and recruited between July 13 and 31, 2022. Multiple linear regression analysis was performed to identify the factors associated with the PADIS-related performance of medical staff.
The evidence-based performance level for PADIS prevention and management had a mean score of 3.55±0.37 out of 5 points, and the mean knowledge score was 28.23±3.00 out of 33 points. The mean awareness score for barriers to implementing PADIS prevention and management guidelines was 2.91±0.39 out of 5 points. Multiple regression analysis indicated that knowledge of delirium (β=.19, p=.014) and awareness of barriers within the individual domains of medical staff (β=-.20, p=.034) significantly influenced PADIS-related performance.
To implement evidence-based practices for the prevention and management of PADIS, steps should be taken to improve the knowledge and awareness of medical staff regarding PADIS. This could be improved through organizational support, such as systematic education and staffing. Specifically, an education program centered on delirium could significantly improve PADIS-related knowledge and performance.
Each year, an average of 220,000 patients are admitted to the Intensive Care Unit (ICU), a figure that continues to rise annually. However, there has been a consistent decrease in mortality rates, dropping from 58.6% in 2008 to 33.8% in 2018 [1]. This data suggests an increasing number of patients are being discharged from the ICU after successful treatment. These patients, having been exposed to a variety of medical devices and equipment in an environment characterized by bright lights and noise, and isolated from their families, often experience a range of physical and emotional distress beyond their primary illnesses [2]. Consequently, survivors of the ICU frequently face health issues such as cognitive decline, muscle weakness, anxiety, and depression. These problems were collectively termed Post-Intensive Care Syndrome (PICS) by the Society of Critical Care Medicine (SCCM) in 2020 [3]. Furthermore, the burden placed on family members caring for these patients can lead to their own psychological and cognitive issues, diminish their quality of life, and even result in Post-Intensive Care Syndrome-Family (PICS-F) [4]. Therefore, the quality of care for ICU survivors and the reduction of associated complications have become significant topics of discussion.
Indeed, patients in the ICU may encounter a range of issues, including pain, agitation, delirium, immobility, muscle weakness, sleep disruption, anxiety, and depression. Primarily, due to the various monitoring devices, critical care patients have restricted physical activities [5]. They also undergo a variety of invasive and non-invasive treatments, routine position changes in the ICU, airway suctioning, wound disinfection, and intubation removal, all of which can cause pain and discomfort [6]. Consequently, assessing pain and managing it appropriately can alleviate patients' stress and facilitate procedures, using measures such as sedation when necessary [7]. Maintaining patient calmness is beneficial for their stability and safety as it reduces discomfort and anxiety, and enhances their coordination with respirators [8].
In addition to pain, patients may experience agitation, delirium, and sleep disruption if environmental stimuli, such as bright lights and noises, are not adequately controlled [6]. Delirium, characterized by cognitive impairment and behavioral disorders, is commonly observed in medical institutions. The incidence of delirium varies widely, ranging from 22.4% to 86.8% depending on the patient population, with the highest rates found among ICU patients [9, 10]. Critical care patients, in particular, often suffer from sleep insufficiency due to both environmental and non-environmental factors, including psychological elements (such as anxiety and fear) and medication use [11, 12]. These factors significantly contribute to the onset of delirium. Furthermore, sleep deprivation can lead to a compromised immune system, cognitive dysfunction, fatigue, reduced physical activity, and respiratory disorders [13]. Therefore, it is crucial to identify and address the factors causing delirium and sleep insufficiency early on, and to implement appropriate interventions. Various pharmacological and non-pharmacological treatments should be provided based on clinical judgment [11, 14].
Issues such as the use of restraining bands due to delirium, and reduced physical activity resulting from insufficient sleep, can lead to muscular weakness [15]. It is estimated that between 25 to 80% of patients admitted to the ICU experience a loss of muscle mass and a decrease in limb muscle strength, even in the absence of diseases that directly impact muscle strength [15, 16]. Furthermore, this muscular weakness may persist even if the patients' underlying conditions improve [17].
To mitigate the numerous complications experienced by adult critical care patients, the SCCM issued guidelines for the management of Pain, Agitation, and Delirium (PAD) [18]. A randomized controlled trial found that assessing PAD and implementing evidence-based management significantly reduced the length of ICU stays, duration of respiratory support, and mortality rates, demonstrating the significant impact of PAD guidelines on ICU patient health outcomes [19]. Moreover, it was observed that an integrated management program linking PAD management guidelines to spontaneous awakening, breathing exercises, early ambulation, and sleep programs improved patient prognosis and reduced medical costs [20]. In 2018, the SCCM released the Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption (PADIS) Guidelines, an updated and more comprehensive version of the PAD guidelines, which now includes immobility and sleep disruption [11]. In Korea, the Korean Society of Critical Care Medicine (KSCCM) translated and published these guidelines [21], and recently released the 2021 KSCCM Clinical Practice Guidelines for Pain, Agitation, Delirium, Immobility, and Sleep Disturbance in the Intensive Care Unit, which are adapted to local conditions [22]. Despite recommendations for these clinical practice guidelines to be applied in the ICU, there is a lack of sufficient research, both in Korea and internationally, to determine whether the PADIS guidelines are actually being implemented, the level of understanding among medical staff, and the potential issues if the guidelines prove difficult to implement [23, 24]. Given that medical staff often place greater emphasis on experiential knowledge in clinical practice and struggle to keep up with the latest evidence [25], it is crucial to determine their level of familiarity with the most recent guidelines. However, possessing knowledge of the guidelines and applying them in practice are two different things, as various individual, interdisciplinary, and organizational factors can impede implementation, or it may be perceived as such [26]. Therefore, it is deemed necessary to identify these challenges in order to enhance the quality of critical care and improve patient outcomes.
This study aims to explore the clinical performance, knowledge, and barrier awareness of medical staff regarding PADIS care in adult critical care patients based on the latest PADIS guidelines and identify the factors influencing the level of PADIS-related performance. The results of this study will be used as basic data for establishing and applying clinical practice strategies for improving the care of critical care patients.
This is a cross-sectional, correlational study to assess ICU medical staff's evidence-based performance, knowledge, and awareness of potential barriers in PADIS prevention and management, and to investigate factors affecting the performance of PADIS prevention and management.
The participants in this study were medical staff, specifically nurses and physicians, who personally managed patients in the ICU of tertiary hospitals and consented to participate in this study. We excluded newly hired nurses with less than one year of experience and nurse managers who did not personally participate in patient care. Given that physicians operate within a different career system, managing ICU patients only after having managed ward patients, we included all physicians with ICU experience, barring those with less than one year of clinical experience.
G*Power (version 3.1.9) [27] was used to calculate the sample size for this study. A multiple regression analysis was performed to examine the factors influencing the final PADIS performance. The minimum sample size of 172 was calculated based on 10 predictive factors: age, gender, education level, job, clinical career, ICU career, working department, whether education was provided, knowledge, and barrier awareness. We also considered a moderate effect size of 0.15, a significance level of .05, and a test power of 95%. We further calculated a final sample size of 197, taking into account potential data inaccuracies and a dropout rate of 15%. Approximately 200 questionnaires were distributed, taking into account the number of ICUs and the medical staff at the two tertiary hospitals under study. After excluding eight participants who met the exclusion criteria and three who did not complete the survey faithfully, we used the data from a total of 189 participants for the analysis.
The measure for assessing the evidence-based performance of PADIS prevention and management in this study was developed based on the KSCCM's translated version [21] of the Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU [11] developed by the SCCM in 2018, as well as the 2021 KSCCM Clinical Practice Guidelines for Pain, Agitation, Delirium, Immobility, and Sleep Disturbance in the Intensive Care Unit [22]. The 2018 PADIS guidelines include 37 recommendations, two appropriate clinical practice plans, and 32 suggestions without specified recommendation levels. The 2021 clinical practice guidelines consist of 42 recommendations, which are divided into three levels of recommendations. Performance measures the effectiveness of medical staff in implementing these items in actual clinical practice. Therefore, the verbs were altered to action-oriented terms, such as "use" or "conduct." Recommendations that only apply to specific ICU patients or patients undergoing specialized surgery (for example, thoracic surgery patients), interventions not implemented in Korean clinical practice, items where performance cannot be measured (such as prognoses, treatment results, cases without recommendations, etc.), and repetitive recommendations were excluded.
The principal investigator, who has over 10 years of clinical experience, collaborated with a professor of adult nursing to draft 40 items for the tool through a series of discussions. Subsequently, five experts, including two ICU specialists, a nursing professor who specializes in measuring tool development, and two nurses with over a decade of ICU experience and at least a master's degree, validated the content relevance of the created items. A 4-point scale, ranging from 1 point for "very inappropriate" to 4 points for "very appropriate," was utilized to assess the content validity of each item. The content validity index was then calculated. Only items with an Item-Content Validity Index (I-CVI) of 0.8 or higher were selected. Following the initial content validity assessment, it was observed that six items scored 0.8 or less. After further discussions, two items (one about pain and another about delirium) were eliminated, while four items were revised and supplemented for the second content validity assessment. Upon completion of the second assessment, all items achieved an I-CVI of 0.8 or higher, and the Scale-Content Validity Index (S-CVI) of the final 38 items was 0.93. The final tool includes 15 items related to pain performance, 5 items on agitation/sedation, 7 items on delirium, 2 items on immobility, and 9 items on sleep disruption (see Appendix 1). Each item is evaluated using a 5-point Likert scale, with 5 points indicating "always" and 1 point indicating "never." A higher score corresponds to a higher level of evidence-based performance in PADIS prevention and management. The Cronbach's α of the tool in this study was .91.
In this study, the same guidelines used for performance were also applied to assess knowledge about PADIS prevention and management. The content validity of these guidelines was confirmed by the same group of experts. Initially, a draft tool consisting of 50 items was created. The relevance of these items was then evaluated by five experts to calculate the first Content Validity Index (CVI). Ten items with a first CVI of 0.8 or less were identified, and an additional seven items were removed based on the experts' additional feedback. This feedback pertained to the items' applicability in actual clinical practice, the clarity of the evidence they provided, and their similarity to the performance items. For instance, items related to treatment factors such as inhaled anesthetics, nonsteroidal anti-inflammatory drugs (NSAID topical gel), and cybertherapy like Virtual Reality (VR) were removed. Items suggesting that family members could conduct pain assessments for patients unable to self-report were also removed, as were items considered controversial, such as those about the treatment of delirium in critical care patients and therapy for subsyndromal delirium. After this process, a total of 33 items were selected for the final tool. Upon the second CVI assessment, all items scored 0.8 or higher, and the S-CVI was 0.89. The final tool includes 11 items about pain-related knowledge, 5 items about agitation/sedation, 9 items about delirium, 2 items about immobility, and 6 items about sleep disruption (Appendix 2). Each item offers three possible responses: "yes," "no," and "unknown." Correct answers are awarded one point, while incorrect answers and "unknown" responses receive no points. This results in a total score range of 0 to 33 points, with higher scores indicating a greater level of knowledge about PADIS prevention and management. The reliability of the tool in this study, as measured by the Kuder-Richardson Formula 20 (KR-20), was .65.
In this study, we developed a tool to assess awareness of potential barriers to the implementation of the PADIS prevention and management guidelines. This tool was based on various potential barrier factors associated with the implementation of evidence-based clinical practice, as outlined in "Interpreting and Implementing the 2018 Pain, Agitation, Sedation, Delirium, Immobility, and Sleep Disruption Clinical Practice Guideline" by the SCCM's medical professionals [23]. A review of the literature identified several barrier factors, including the complexity of applying clinical practice guidelines, organizational support, resource accessibility, the clinical period of evidence-based practice, the provision of education, financial support, team communication, the ICU's organizational culture, and individual self-efficacy. The principal investigator and a professor of adult nursing initially agreed on 26 items that could potentially act as barriers within these factors. These items were then categorized into three groups: individual factors, ICU team factors, and hospital organization factors. After five experts calculated the first CVI for 25 of these items, it was found that three items had a CVI of less than 0.8. One item, "education is provided in a multimodal way to facilitate knowledge transfer for individuals with different learning styles," was deemed similar in meaning to "education is provided at different times and in different methods." As a result, this item was removed, and two items were revised and supplemented based on expert feedback. When the second CVI was calculated by the same group of experts, all items scored 0.8 or higher, with an S-CVI of 0.94. The final tool consisted of 25 items: 8 items related to individual factors such as self-efficacy, belief, and attitude towards PADIS implementation; 6 items related to ICU team factors such as team members' knowledge and skills, attitude towards PADIS, and experience in quality improvement activities; and 11 items related to organizational factors such as resources, educational support, compensation, and culture (Appendix 3). Each item was scored on a 5-point Likert scale, ranging from 1 point ("strongly agree") to 5 points ("strongly disagree"). The seven positive items were reverse-coded, meaning a higher score indicated greater awareness of potential barriers to PADIS prevention and management. The tool's Cronbach's α in this study was .80.
The general characteristics of the participants were investigated, including age, gender, level of education, and job (either physician or nurse). Additional factors examined were total clinical career, ICU career, current working department, and prior experience of education on adult ICU patients.
The data used in this study were collected at two tertiary hospitals between July 13 and July 31, 2022. The research team visited the nursing departments at both hospitals, where they explained the study's purpose, procedure, inclusion and exclusion criteria, and secured their cooperation. Each ICU received envelopes containing the subject information sheet, informed consent form, and a self-questionnaire, delivered by the ICU Team Leader. Nurses who voluntarily agreed to participate in the study after reviewing the information sheet signed the consent form, placed it back in the envelope, and sealed it. Given the difficulty of arranging face-to-face meetings with physicians, the questionnaires were left in the ICU following discussions with several professors overseeing the ICU. Additionally, an online questionnaire was created. Physicians received a URL to the Google Form, and after understanding the study's purpose, they were free to complete the survey if they consented. The survey took approximately 20 minutes to complete, and participants were given a small gift upon completion. All completed questionnaires were collected by the nursing department and statistically analyzed alongside the results from the online survey, which included responses from 11 physicians.
This study received approval (IRB No. CNUH-2021-439) from the Institutional Review Board (IRB) of a hospital before it was conducted. The purpose and procedure of the study, as well as the anonymity and confidentiality of the participants, were thoroughly explained to the participants via a subject information sheet. The survey was then carried out with those who provided their written consent and completed the online consent procedure, based on their willingness to participate. To safeguard the personal information within the survey data, each questionnaire was assigned a serial number. The data collected online were downloaded and stored on the researchers' personal computers, secured with an encrypted code. The data analysis was performed using these personal computers. All data will be disposed of three years after the conclusion of the study, following a retention period.
All collected data were analyzed using SPSS/WIN 21.0. Descriptive statistics, including frequency, percentage, mean, and standard deviation, were calculated to describe the general characteristics of the participants, their performance, knowledge, and awareness of barriers related to PADIS prevention and management. To examine the differences in PADIS prevention and management performance based on the participants' general characteristics, the independent t-test or a one-way ANOVA was employed. Pearson's correlation was utilized to analyze the relationship between age and career (continuous variables of general characteristics) and knowledge, barrier awareness, and performance in PADIS prevention and management (major independent variables). To identify the independent factors influencing performance in PADIS prevention and management, a multiple linear regression analysis was conducted. As a prerequisite, normality was assessed using skewness and kurtosis before conducting the regression analysis. A distribution was considered normal if the absolute value was less than 3 for skewness and less than 8 for kurtosis [28]. The independence of the independent variables was evaluated using variance and the Variance Inflation Factor (VIF), which indicate the correlation between independent variables and the presence of multicollinearity. The Durbin-Watson index was used to assess the autocorrelation of the dependent variables. All analyses were conducted as two-sided tests, with statistical significance only considered if p<.05.
Out of the 189 participants in this study, 172 (91.0%) were nurses and 17 (9.0%) were physicians. The mean age was 29.99±4.25, with 146 (77.2%) of the participants being women. The majority of participants, 176 to be exact, held a bachelor's degree as their highest level of education, while 13 (6.9%) had a master's degree or higher. The mean length of clinical career was 5.63±4.14 years, and the mean ICU career was 3.91±2.90 years. A total of 125 participants (66.1%) reported having received training in adult critical care patient management (Table 1).
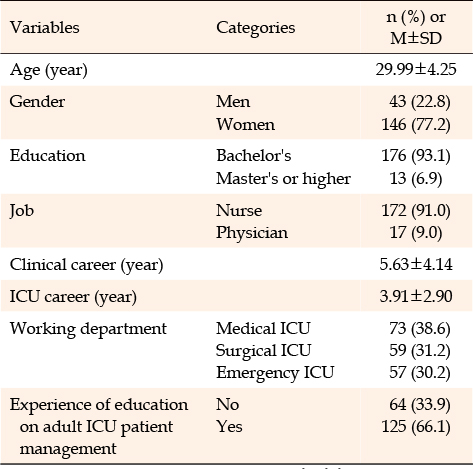
Table 1
General Characteristics of Participants (N=189)
The mean score for participants' evidence-based performance was 3.55±0.37 out of a possible 5 points. Among the five sub-factors, the highest scoring was agitation/sedation, with a score of 3.74±0.54 points. This was followed by immobility, which scored 3.70±0.72 points, and sleep, which scored 3.65±0.51 points. The sub-factor with the lowest score was delirium, with 3.12±0.43 points (Table 2). The two items that demonstrated the highest performance were both related to pain assessment. The first item, "When evaluating pain in critically ill patients who are able to self-report pain, I use a valid and feasible pain scale (e.g., the 0~10 Numeric Rating Scale [NRS]) to express it verbally," scored 4.40±0.71 points. The second item, "When evaluating pain in critically ill patients who cannot self-report pain but exhibit observable behaviors, I use the Behavioral Pain Scale in Intubated (BPS) and Nonintubated (BPS-NI) patients and the Critical-Care Pain Observation Tool (CPOT)," scored 4.30±0.91 points. The two items with the lowest performance were both reverse items. The first, "I use vital signs (e.g., Heart Rate [HR], Blood Pressure [BP], Respiratory Rate [RR], Oxygen Saturation [SpO2], and end-tidal CO2) as pain indicators in critically ill patients," scored 1.47±0.64 points. The second, "I consider the use of dexmedetomidine (e.g., Dextomin, Precedex premix) or propofol (e.g., Fresofol) at night to improve sleep," scored 1.96±0.73 points. These items were part of the sleep factor (Appendix 1).
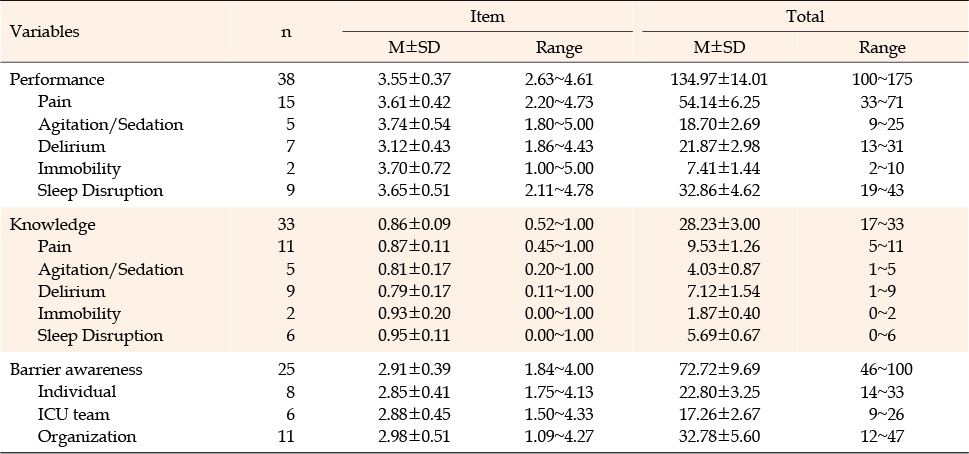
Table 2
Performance, Knowledge, and Barrier Awareness of Medical Staff in PADIS Prevention and Management (N=189)
The mean knowledge score of participants regarding PADIS prevention and management was 28.23±3.00 out of a possible 33 points. Among the sub-factors, the highest score was for knowledge related to sleep, with a mean score of 0.95±0.11 points. This was followed by immobility at 0.93±0.20 points, pain at 0.87±0.11 points, and agitation/ sedation at 0.81±0.17 points. The lowest score was for knowledge related to delirium, with a mean score of 0.79±0.17 points (Table 2). The items with the lowest knowledge scores were "In critically ill patients under mechanical ventilation, light sedation should be prioritized over deep sedation" in the agitation/sedation category (0.44±0.50 points), and "The prognosis for patients whose delirium rapidly and reversibly improves is similar to that of patients who have not experienced delirium" in the delirium category (0.44±0.50 points) (Appendix 2).
The mean score of the barrier awareness for implementing the PADIS prevention and management guidelines was 2.91±0.39 out of 5 points. The lowest mean score (2.85±0.41 points) was for awareness of barriers related to individual beliefs, attitudes, and self-efficacy regarding evidence-based clinical practice. The mean score for awareness of barriers related to communication among ICU team members and their experience was 2.88±0.45 points. The highest mean score (2.98±0.51) points, was for awareness of barriers related to organizational culture and policies, such as support and compensation (Table 2). The three items perceived as the most significant barriers were: "Documentation burden will increase." (3.61±0.83 points), "There are many other tasks in the ICU that take precedence over PADIS adoption" (3.45±0.80 points), and "Additional personnel will be allocated to monitor progress, provide feedback, and make necessary changes to the electronic health records" (3.41±0.98 points) (Appendix 3).
Upon analyzing the correlation between the participants' general characteristics, their knowledge of PADIS prevention and management, their awareness of barriers to implementation, and their performance in PADIS prevention and management, it was found that both knowledge of PADIS prevention and management (p<.001) and barrier awareness (p<.001) were statistically correlated with performance. The general characteristics of the participants, such as age, career, and job, showed no correlations (Table 3). Specifically, among the sub-factors of knowledge of PADIS prevention and management, pain (p=.036), delirium (p<.001), immobility (p=.015), and sleep disruption (p=.011) were significantly correlated with performance in PADIS prevention and management. Similarly, all subfactors of barrier awareness, namely individual (p<.001), team (p=.002), and organization (p=.002), were significantly correlated with performance in PADIS prevention and management.
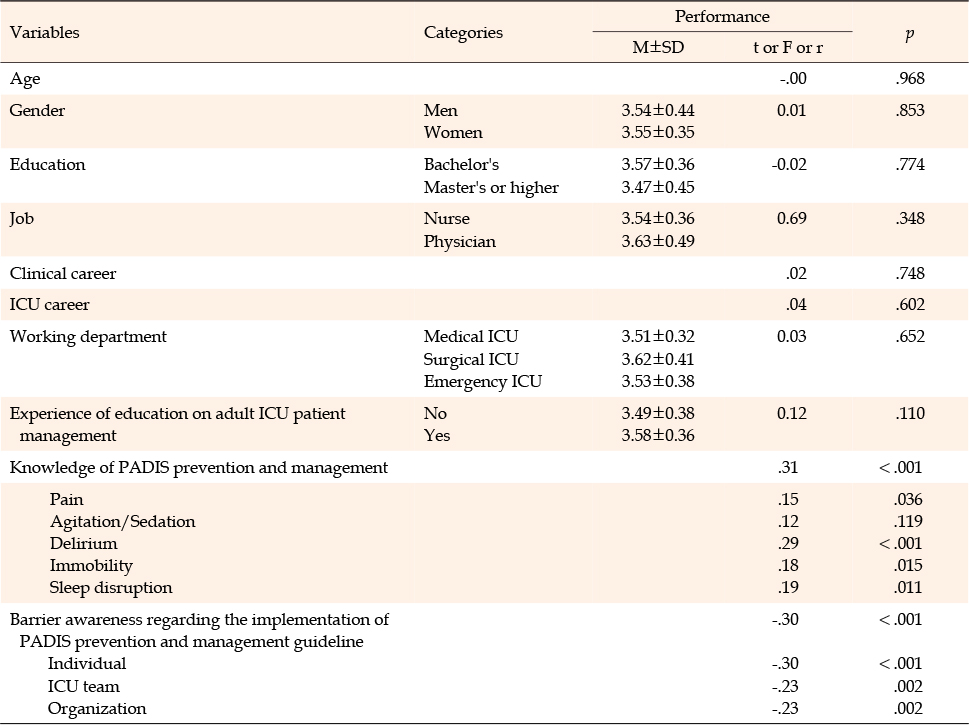
Table 3
Relationships between Performance and Study Variables (N=189)
The statistically significant variables (at a level of p<.050) in the univariate analysis were all entered into the multiple linear regression analysis. Upon examining the correlations between the independent variables, it was observed that none of the variables had a correlation coefficient of 0.8 or higher. The tolerance values ranged from 0.54 to 0.98, exceeding 0.1, and the VIF varied between 1.02 and 1.83. As this value was less than 10, it indicated the absence of multicollinearity among the independent variables. The Durbin-Watson index was calculated to be 1.97 (dU=1.84<d<4-dU=2.16), suggesting that the variables were independent, irrespective of the autocorrelation of the dependent variables. Therefore, all assumptions for the multiple linear regression analysis were met. Post-analysis, it was determined that a higher level of delirium knowledge (β=.19, p=.014) and a lower level of individual barrier awareness among medical staff (β=-.20, p=.034) were associated with a higher evidence-based performance of PADIS prevention and management (F=5.84, p<.001). The model's explanatory power for the performance of PADIS prevention and management was 16.3% (Table 4).
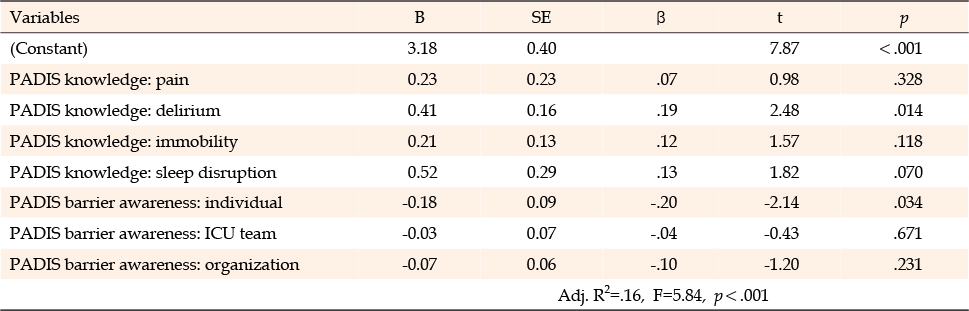
Table 4
Factors Affecting Evidence-based Performance of PADIS Prevention and Management
This study investigated the performance and knowledge of ICU medical staff in preventing and managing PADIS in adult critical care patients. It also aimed to explore the awareness of barriers involved in the implementation and to identify the factors influencing performance in PADIS prevention and management. The study found that a higher level of knowledge about delirium and a lower level of individual medical staff's awareness of barriers were correlated with improved performance.
The mean score for each factor in the knowledge of PADIS prevention and management was as follows: 0.87 points for pain, 0.81 points for agitation/sedation, 0.79 for delirium, 0.93 for immobility, and 0.95 for sleep disruption. Of these five factors, agitation/sedation and delirium scored relatively lower. Upon evaluating the items within the agitation/sedation and delirium factors, it became apparent that there is a lack of understanding regarding the purpose and maintenance of sedation levels, as well as the risk factors and prognosis of delirium. A previous study that assessed the knowledge of existing ICU nurses about sedation reported a mean score ranging from 17.80 to 17.97 out of 20 points [29, 30]. The sub-factors of sedation knowledge, based on the 2013 PAD guidelines, had a mean score of 7.23 to 7.27 out of 9, which is relatively low. The most frequently incorrect response was related to understanding the purpose of sedation levels in mechanically ventilated patients. This finding aligns with previous studies [29, 30], which also reported this as the most common error. In essence, the score for knowledge of sedation levels in this study reflects a lack of understanding about the protocols necessary to achieve and maintain these levels. The knowledge related to the delirium factor was assessed as the lowest in this study. This is consistent with a previous study that examined ICU nurses' understanding of delirium, where the mean score was a low 31.39 out of 45 points (a mean rating of 2.16 points) [31]. In this study, the understanding of the risk factors and prognosis of delirium was evaluated as low. This is similar to the findings of another study [32] conducted with nurses at a hospital that used the delirium assessment tool in the ICU. That study found that there is limited knowledge about its potential to increase mortality and preventability, despite it being perceived as an important issue requiring active interventions [32]. Limited understanding of the delirium factor can hinder the effective management of critical care patients. Given that knowledge of the delirium factor was significantly related to performance in PADIS prevention and management in this study, an improved understanding of the causes, prognosis, and management of delirium is crucial for the quality management of critical care patients.
In this study, the mean awareness score of medical staff regarding barriers to PADIS prevention and management was 2.91 points. The most significant barrier, as perceived by the staff, was due to organizational factors, followed by team factors, and then individual factors. The three items with the highest barrier awareness scores were: the individual concern about an increased documentation burden, the team perception that other tasks in the ICU take precedence over PADIS adoption, and the organizational need for additional personnel if PADIS guidelines are to be implemented. This suggests that the adoption of PADIS guidelines would increase the workload and that the current workforce is insufficient to adopt these guidelines. While a direct comparison is challenging due to this study's inclusion of physicians in addition to nurses, a previous study with ICU nurses also reported that excessive workload, difficulties in delirium assessment based on patient characteristics, and time-intensiveness act as barriers to delirium assessment [33]. These barriers result in delirium assessment not being prioritized over other assessment factors by ICU nurses [32]. Moreover, mirroring a previous study that identified inadequate knowledge, excessive workload, lack of equipment, and absence of protocols or guidelines as barriers to early mobilization [33], this study found that concerns about excessive workload or work burden and insufficient organizational support are major obstacles to the application of evidence-based clinical practice.
Although the medical staff in this study perceived organizational barriers as more significant, it was the individual barriers that showed a substantial correlation with actual performance. In other words, individual knowledge, attitudes, and beliefs significantly influenced the implementation of PADIS prevention and management. Among the individual barriers, the item scoring highest was the belief that " (I think that) documentation burden will increase," and the item with the lowest score was " (I think that) ICU team members are considered capable of practicing the PADIS recommendations." This suggests that individual medical staff members believe that, despite the ICU team's capability to adopt the PADIS guidelines, there is concern about the potential increase in workload resulting from this adoption. Therefore, organizational support, including the provision of systems, workforce, and guidelines, is crucial for evidence-based practice. It is equally important for each medical staff member to acknowledge the significance of organizational support and to maintain positive attitudes and beliefs.
The mean score for performance in PADIS prevention and management was 3.55 out of 5 points. The delirium factor scored the lowest among the sub-factors, with a score of 3.12 points. This suggests that there are insufficient preventive measures for delirium, as well as inadequate responses when it does occur. In contrast, issues related to pain, agitation/sedation, immobility, and sleep are relatively well prevented or managed. Within the delirium factor, the items that scored lower than the mean were the use of a valid tool (for example, the Confusion Assessment Method for the ICU [CAM-ICU] or the Intensive Care Delirium Screening Checklist [ICDSC]) for delirium in critically ill patients, and pharmacologic interventions for the prevention and treatment of delirium. These items reflect a lack of regular delirium assessments using a valid tool and insufficient use of appropriate therapeutic drugs. These issues need to be addressed not just at an individual level, but also at the level of the ICU team or the organization as a whole. Preventive interventions based on the use of a valid tool have been shown to reduce the incidence of delirium, the length of hospital stay, the length of ICU stay, and mortality [34]. Therefore, organizational efforts are needed, such as implementing a valid tool that can bring about changes in practice and establishing treatment protocols based on these study results. A previous study reported that the implementation of a delirium educational program improved knowledge and performance related to delirium and increased the rate of delirium assessments [35]. Building on these findings, the development and implementation of educational programs related to PADIS could enhance the knowledge and performance of medical staff in PADIS prevention and management, thereby reducing the incidence of PADIS-related problems.
Although this study was conducted among the medical staff of two tertiary hospitals, it only included staff from one region and investigated a relatively small number of physicians. These limitations may hinder the generalizability of the findings to all medical staff. The potential influence of using both online and offline questionnaires, due to accessibility issues, on the results cannot be dismissed. Furthermore, despite the items being developed based on the most recent guidelines and literature related to PADIS in Korea and abroad, the tool was not validated in several aspects, including construct validity, which is another limitation. Despite these constraints, this study provides significant insights as it explores the performance and knowledge of ICU medical staff regarding the latest guidelines on the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult critical care patients, and addresses the challenges of practicing.
The results of this study suggest that intervention strategies, such as educational programs aimed at enhancing the knowledge of ICU medical staff about PADIS prevention and management, are necessary. These programs should particularly focus on improving understanding of delirium to enhance clinical practice performance based on PADIS Guidelines for critical care patients. The development and implementation of interventions to boost the knowledge of nurses, who constitute the majority of medical staff and provide round-the-clock patient care, are expected to directly influence the prevention and management performance of PADIS in critical care patients. In addition to improving knowledge, these intervention programs should also consider strategies for achieving positive outcomes from the medical staff's PADIS practice and for decreasing awareness of potential barriers. Furthermore, the efficient establishment of evidence-based management for critical care patients in the clinical field can be achieved if these intervention programs are offered to all ICU medical staff. This can be further enhanced by improving communication among ICU team members and by fostering a supportive organizational culture and system.
CONFLICTS OF INTEREST:Sung-Hee Yoo has been the Editorial board member of the Korean Journal of Adult Nursing since 2018. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - SH-G and YS-H.
Data collection - SH-G.
Analysis and interpretation of the data - SH-G, CD, and YS-H.
Drafting and critical revision of the manuscript - SH-G, CD, and YS-H.



 E-SUBMISSION
E-SUBMISSION