
Purpose
Sarcopenia is significantly associated with frailty, readmission, and mortality in patients with heart failure. This review aims to provide an overview of the literature on sarcopenia in individuals with heart failure.
Methods
A comprehensive literature review was conducted regarding the current state of knowledge on assessment tools for the diagnosis, prognosis, and optimal management of sarcopenia in patients with heart failure.
Results
Sarcopenia can be defined as the loss of muscle mass with low muscle strength and/or poor physical performance. Sarcopenia has been officially listed as a disease in the eighth revision of the Korean Classification of Diseases in 2021. The causes of sarcopenia in patients with heart failure are multifactorial, including chronic inflammation, hormonal imbalances, nutritional deficiencies, low muscle blood flow, and endothelial dysfunction. The management of sarcopenia is primarily focused on exercise and/or nutritional management because there is no specific pharmacological therapy to treat sarcopenia.
Conclusion
Healthcare professionals should be aware of the significance of early detection and timely management of sarcopenia to avoid physical disability, long-term institutional care, and mortality in individuals with heart failure. Clinical trials are required to evaluate the effectiveness of interventions including exercise and nutrition, alone or in combination, on sarcopenia in patients with heart failure. In addition, more research is required to identify multidimensional risk factors and diagnostic biomarkers for sarcopenia.
Sarcopenia is significantly associated with frailty, readmission, and mortality in patients with heart failure. This review aims to provide an overview of the literature on sarcopenia in individuals with heart failure. Methods: A comprehensive literature review was conducted regarding the current state of knowledge on assessment tools for the diagnosis, prognosis, and optimal management of sarcopenia in patients with heart failure.
Sarcopenia can be defined as the loss of muscle mass with low muscle strength and/or poor physical performance. Sarcopenia has been officially listed as a disease in the eighth revision of the Korean Classification of Diseases in 2021. The causes of sarcopenia in patients with heart failure are multifactorial, including chronic inflammation, hormonal imbalances, nutritional deficiencies, low muscle blood flow, and endothelial dysfunction. The management of sarcopenia is primarily focused on exercise and/or nutritional management because there is no specific pharmacological therapy to treat sarcopenia.
Healthcare professionals should be aware of the significance of early detection and timely management of sarcopenia to avoid physical disability, long-term institutional care, and mortality in individuals with heart failure. Clinical trials are required to evaluate the effectiveness of interventions including exercise and nutrition, alone or in combination, on sarcopenia in patients with heart failure. In addition, more research is required to identify multidimensional risk factors and diagnostic biomarkers for sarcopenia.
Heart failure refers to a syndrome caused by structural and/or functional cardiac abnormalities, confirmed by increased natriuretic peptide levels and objective evidence of pulmonary or systemic congestion [1]. Heart failure is a global health problem, and its prevalence is expected to increase due to longer life expectancy brought about by advances in medical technology [2]. Notably, heart failure is a major cause of hospitalization in patients aged 65 and older, accounting for 1~2% of all hospitalizations [3]. The number of patients with heart failure in Korea is also expected to increase markedly because of the rapidly rising number of older people [4]. According to a report from the Korean Society of Heart Failure [4], the survival rate in Korea was 91% at 1 year after diagnosis of heart failure, but progressively declined to 79% at 5 years, 66% at 10 years, and 54% at 15 years. In this regard, a better understanding of the causes of negative health outcomes in patients with heart failure can contribute to developing preventive strategies and reducing the burden of healthcare costs.
Sarcopenia is characterized by reduced muscle mass, diminished muscle strength, and poor performance, and it is often aggravated by chronic diseases including cardiovascular diseases [5]. Sarcopenia has a particularly high prevalence (>20%) in patients with heart failure [6, 7]. Sarcopenia can lead to decreased exercise capacity and frailty [8]. More specifically, decreased muscle function due to sarcopenia can lead to physical frailty in patients with heart failure, which may increase their risk of physical disability and worsening symptoms of heart failure [9, 10, 11]. Thus, the purpose of this review was to describe the current knowledge in terms of the definition, mechanism, risk factors, assessment tools, and management of sarcopenia in individuals with heart failure.
To date, there is no consensus on a singular definition of sarcopenia. However, the definitions proposed by the European Working Group on Sarcopenia in Older People at their second meeting (EWGSOP2) in 2019 [12], and the Asian Working Group on Sarcopenia 2 (AWGS2) in 2019 [13], are commonly utilized. A recent review indicated that the EWGSOP2 definition has been extensively examined in a significant number of validity tests, compared to the sarcopenia definitions provided by other working groups [14]. According to the EWGSOP2 guideline, sarcopenia is characterized by (1) low muscle strength, which is deemed the most accurate indicator for assessing sarcopenia, (2) evidence of low muscle mass, and (3) an assessment of poor physical performance. If all three criteria are fulfilled, the sarcopenia is considered to be severe [12].
In 2016, sarcopenia was officially recognized as a muscle disorder in the International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10 CM) [15]. More recently, the Korean Standard Classification of Diseases-8 (KCD-8) also acknowledged sarcopenia as a disease, assigning it the code M62.5 in 2021 [16]. Sarcopenia can be categorized as either acute (i.e., occurring within 6 months of an immobilizing event such as acute illness or hospitalization) or chronic (i.e., a sarcopenic state that persists for longer than 6 months) [17]. Sarcopenia can also be classified based on its cause as primary or secondary [18]. Primary sarcopenia is an age-related process without an identifiable secondary cause [12, 17]. Conversely, secondary sarcopenia, also referred to as complex sarcopenia, is commonly found in individuals with chronic conditions such as cardiovascular disease, respiratory disease, renal failure, cancer, and dementia [12, 17].
Sarcopenia is a contributing factor to physical frailty [19]. However, frailty encompasses a much wider concept [20]. It is characterized by a decline in multiple physiological systems over a person's lifetime, resulting in adverse effects on physical, cognitive, and social levels [21]. Frailty can be described as a generalized decrease and loss of physiological storage capacity, impacting multiple organs and systems [22]. The Fried frailty phenotype is used to screen for frailty, requiring assessments of walking speed, grip strength, and physical activity [23]. The relationship between frailty and sarcopenia is not fully understood, but these conditions share many similar health outcomes and suggested pathophysiology [22]. Despite this, sarcopenia is viewed as a component of frailty or a precursor syndrome, whereas frailty is not considered a component of sarcopenia [23].
The global prevalence of sarcopenia is projected to rise from 50 million in 2010 to an estimated 200 million by 2050 [7]. Recent studies indicate that the prevalence of sarcopenia can greatly vary based on the definition and diagnostic method used, as well as factors such as gender, age, and medical conditions [12]. The reported prevalence ranges from 8% to 40% in individuals aged 60 and above, and this increases to between 11% and 50% in those over 80 years of age [24]. For community-dwelling individuals, the estimated prevalence of sarcopenia is around 11% in men and 9% in women. However, in hospitalized patients, the prevalence is estimated to be between 23% and 37% in men and 24% to 33% in women [25, 26]. Research on sarcopenia in Asian populations is still emerging, and epidemiological studies have found that the prevalence of sarcopenia in elderly Asian patients varies widely, from 7.8% to 35.3%, which is lower compared to Western populations [27]. In South Korea, the prevalence of sarcopenia varies from 6.3% to 21.8% in men and 4.1% to 22.1% in women [28].
Sarcopenia is commonly found in individuals with cardiovascular disease (31%), as well as other age-related conditions such as diabetes (18%) [29], chronic obstructive pulmonary disease (21.6%) [30], and mild cognitive impairment (20.5%) [31]. Notably, the prevalence of sarcopenia in patients with heart failure is reported to be 20% higher than in healthy individuals of the same age [6]. A recent meta-analysis study [5] revealed that the pooled prevalence of sarcopenia was 32% in patients with chronic heart failure, 61% in patients with acute decompensated heart failure, 43% in patients with coronary artery disease, and 30% in patients with cardiac arrhythmias.
To date, it is known that the onset and progression of sarcopenia are strongly linked to factors such as advanced age, lack of physical activity, malnutrition, chronic inflammation, hormonal imbalances, genetic predisposition, and chronic diseases [6]. In the context of heart failure, the mechanisms contributing to muscle wasting associated with this condition include hormonal shifts, malnutrition resulting from medication side effects, chronic low-grade inflammation, oxidative stress, and myonuclear apoptosis [7]. Furthermore, hemodynamic alterations can lead to reduced cardiopulmonary fitness due to physical inactivity, as well as diminished muscle blood flow resulting from low cardiac output [10].
The high prevalence of sarcopenia in heart failure patients may be attributed to a combination of risk factors. These include physical inactivity, systemic inflammation, and malnutrition, which compound the existing abnormalities associated with cardiac dysfunction [11]. These mechanisms can instigate a vicious cycle that further deteriorates heart function and accelerates muscle wasting. More specifically, the diminished muscle function resulting from sarcopenia is linked to limitations in daily activities. This can exacerbate the worsening of heart failure symptoms such as shortness of breath, fatigue, and edema [14].
A recent systematic review has suggested that risk factors for sarcopenia in patients with heart failure may include older age, a lower body mass index, higher B-type Natriuretic Peptide (BNP) levels, and a reduced Left Ventricular Ejection Fraction (LVEF) [6]. However, the mechanisms underlying the relationship between skeletal muscle loss and heart failure remain elusive. In evaluating the risk of sarcopenia in heart failure patients, it is crucial to take into account variations in data collection environments and the demographic characteristics of the study population [7]. Future research should aim to establish a causal link between sarcopenia and heart failure, as well as identify the causes of sarcopenia in patients suffering from heart failure.
Although a sarcopenia diagnosis code has been introduced in Korea, many healthcare providers in Korea are still unfamiliar with sarcopenia assessment tools. The most commonly used definitions for sarcopenia are those provided by the EWGSOP2 and the AWGS2 [11, 12].
As shown in Table 1, both the EWGSOP2 and AWGS2 recommend the use of the "Strength, Assistance with Walking, Rising from a Chair, Climbing Stairs, and Falls (SARC-F)" questionnaire for case identification. The SARC-F serves as a superior screening tool for functional measurement. If sarcopenia is suspected, an evaluation of muscle mass, muscle strength, and physical function is typically ordered for diagnosis [32]. Muscle mass is usually measured using Dual-Energy X-ray Absorptiometry (DEXA) and Bioelectrical Impedance Analysis (BIA). DEXA is a commonly employed imaging technique for estimating body composition, while BIA is used to measure lean body mass (kg) and is considered a valid alternative for body composition assessment [33]. Computed tomography and magnetic resonance imaging are regarded as the gold standard for non-invasive muscle mass assessment. However, they are not widely used due to their high cost, the requirement for highly skilled personnel, and the lack of well-established cutoff values that define low muscle mass [26].
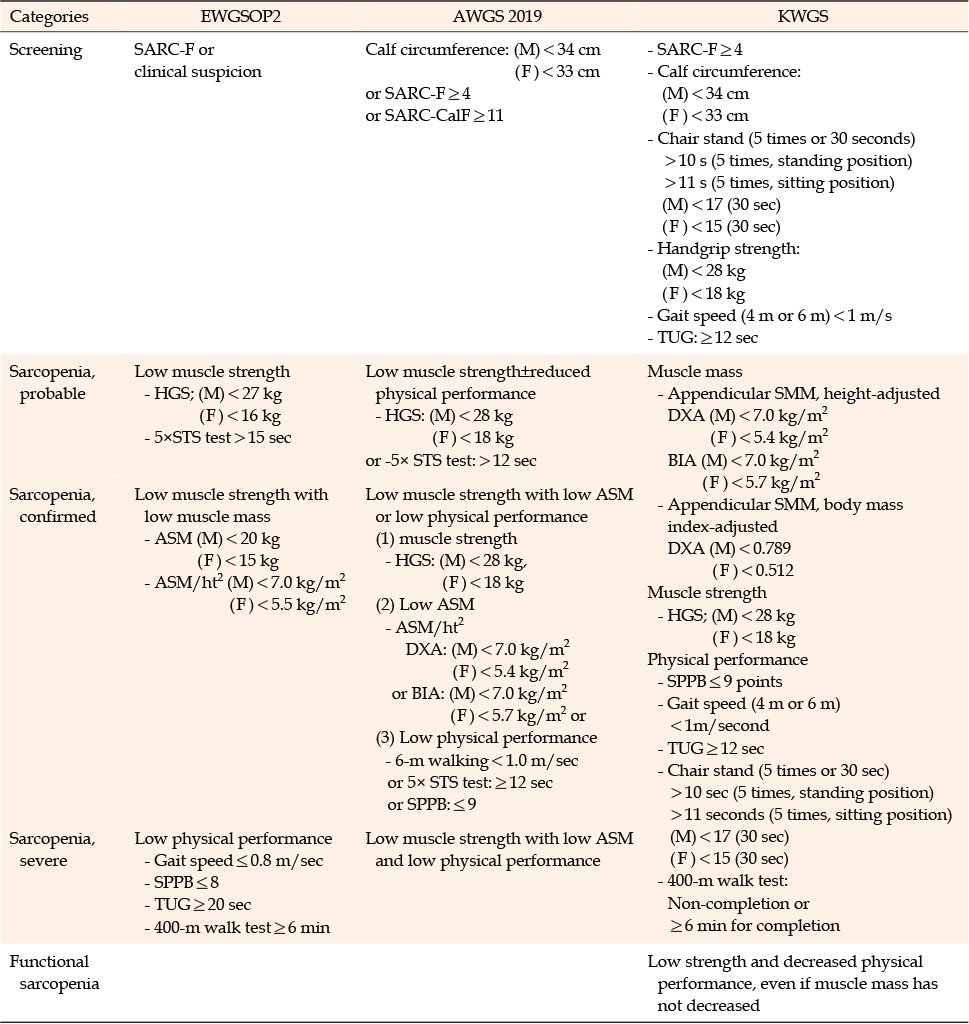
Table 1
Screening and Diagnosis of Sarcopenia by International and Korean Working Groups
The strength of skeletal muscles is measured by grip force, and physical performance is determined by gait speeds over distances of 4 or 6 meters [25]. Gait speed can be easily assessed in clinical settings by measuring the time it takes to walk a set distance, such as 4 meters, at a normal pace [25]. For assessing physical functioning, the Simple Physical Performance Battery (SPPB) is the recommended initial test, with the provision that up to two additional tests can be used in conjunction to identify any decline in physical functioning [18]. If the SPPB is not a viable option, alternatives such as gait speed or the Timed Up and Go (TUG) test can be considered. The TUG test incorporates several elements, including standing, walking, turning, and sitting, which mirror the movements encountered in daily living [18].
The Korean Working Group on Sarcopenia (KWGS) established guidelines in 2019 to introduce a nation-specific consensus on sarcopenia [16]. These guidelines were developed with consideration of the guidelines from both the EWGSOP2 and the AWGS2 [16], and they encompass a wide array of screening tools for individuals with sarcopenia. Both the EWGSOP2 and the AWGS2 utilize three categories: probable sarcopenia, confirmed sarcopenia, and severe sarcopenia. Severe sarcopenia is characterized by low physical performance, decreased muscle mass, and poor strength [12]. Notably, the KWGS guidelines redefine decreased muscle strength and poor physical performance, irrespective of muscle mass, as "functional sarcopenia," emphasizing their clinical relevance (Table 1).
Certain inflammatory biomarkers, including C-reactive protein, interleukin-6, and tumor necrosis factor-α, have been linked to sarcopenia [34]. More recently, the ratio of creatinine to cystatin C has been proposed as a potential marker for sarcopenia [35]. However, a comprehensive biomarker panel for the early detection of sarcopenia remains to be established [34, 36]. As a result, additional research is necessary to identify potential biomarkers for the early diagnosis of sarcopenia, particularly in patients with chronic diseases such as heart failure.
Sarcopenia is an important predictor of adverse health outcomes, including frailty, increased risk of falls, functional impairment, diminished quality of life, hospitalization, and all-cause mortality across various clinical settings [5]. Furthermore, sarcopenia is positively correlated with elevated healthcare costs and increased utilization of healthcare resources [6]. Recent research suggests that sarcopenia may be a modifiable condition [6, 7]. The prevention and optimal management of sarcopenia in heart failure patients typically involve regular exercise (including physical activity and resistance training), nutritional management, and multimodal interventions such as a combination of physical activity and nutrition [9]. We will discuss the positive effects of several interventions on sarcopenia in the following sections.
Exercise: Sarcopenia is associated with exercise capacity and restrictions in daily activities, contributing to disability and muscle loss [37]. Physical inactivity is prevalent among frail patients due to the progression of heart failure. Exercise is the most effective treatment for muscle wasting in heart failure, supported by ample clinical evidence [9]. Exercise physiologically impacts nearly all organ systems, particularly the musculoskeletal, endocrine, and immune systems [37].
Resistance exercise, which involves sustaining contraction or working against an applied force, is widely utilized to enhance muscle strength and boost physical performance [38]. Implementing interventions that incorporate resistance exercise training at least three times per week, with a progressive increase in difficulty, may prove effective [38]. In managing sarcopenia, it is advisable to promptly implement a multicomponent exercise program post-hospitalization. This program should include elements such as resistance, challenging balance, and functional training that mirrors activities of daily living [39]. Given that exercise intervention is an economical and cost-effective preventative measure, healthcare professionals need to comprehend the nature of sarcopenia and design exercise programs that cater to individual needs [37].
Cardiac rehabilitation has been demonstrated to enhance both physical and cognitive function in patients experiencing heart failure exacerbations. This results in an improved quality of life and a reduction in physical frailty [38]. At present, there are no standard guidelines for managing sarcopenia in patients with heart failure. Future studies are needed to provide more clinical evidence regarding effective exercise protocols, including the type, intensity, and volume of exercise required.
Nutrition: Protein plays a crucial role in the diet for sarcopenia, providing the necessary amino acids for muscle synthesis. Specifically, older adults are advised to increase their daily protein intake to 1~1.2 g/kg/day, which should include high amounts of essential amino acids such as leucine [40]. Leucine is a powerful regulator of protein turnover, especially protein anabolism [41]. It is recommended that at least two servings of leucine be consumed daily, not exceeding 2.8~3 grams [40]. High-quality Oral Nutritional Supplements (ONS) can be beneficial for older adults to ensure they receive adequate amounts of protein and amino acids [9]. ONS can be particularly useful for individuals with sarcopenia, as they often do not consume enough food. In addition, older individuals should be given vitamin D supplementation of 800~1,000 IU per day [40]. Vitamin D enhances protein anabolism in conjunction with leucine [42]. It also has the potential to improve physical activity and muscle function in older adults. Consequently, it is suggested that consuming protein, including leucine, and vitamin D supplements together may contribute to increased muscle mass and improved physical performance.
A recent systematic review and meta-analysis of 39 studies examined the impact of protein and essential amino acid supplementation on sarcopenia in older adults aged 65 and above. The findings indicated that nutritional interventions enhanced muscle strength and physical function in older adults suffering from sarcopenia [43]. Another systematic review of 29 studies revealed that vitamin D supplementation boosted muscle strength, especially in older adults with serum 25-(OH)D concentrations below 30 ng/mL, compared to those with levels above 30 ng/mL [42]. Regrettably, the evidence supporting the use of nutritional interventions as a strategy to reduce the risk of sarcopenia in individuals with heart failure is not sufficiently convincing [9]. In light of this, early nutritional assessment of patients with heart failure is crucial to prevent the onset of sarcopenia induced by heart failure or the exacerbation of heart failure symptoms due to sarcopenia. Furthermore, malnutrition assessment tools specifically for patients with heart failure should be developed.
Multimodal and/or pharmacological intervention: Currently, the primary combined interventions for sarcopenia and cardiovascular disease consist of physical exercise, appropriate nutrition, and pharmacological treatment [9]. Specifically, a combined approach that incorporates physical activity and nutritional supplements can potentially prevent the loss of lean body mass. This, in turn, contributes to a reduction in mortality rates and hospital readmissions.
To date, there has been no approved pharmacological treatment for sarcopenia. Specifically, pharmacological and hormone replacement therapies, including the use of vitamin D, testosterone, and growth hormone, have proven to be ineffective [11, 44]. It is crucial to fully consider the complexity of this condition by integrating pharmacological interventions with other existing treatments, such as exercise training or nutritional supplements, in future studies.
Figure 1 summarizes the definition, type, screening tools, prognosis, and management of sarcopenia. Implementing early screening and comprehensive management strategies for sarcopenia can effectively slow its progression and decrease adverse health outcomes, such as poor quality of life, physical disability, hospital readmissions, and mortality. It is crucial for healthcare professionals, particularly nurses, to have a thorough understanding and awareness of sarcopenia for its early prevention, diagnosis, and management in the heart failure population.
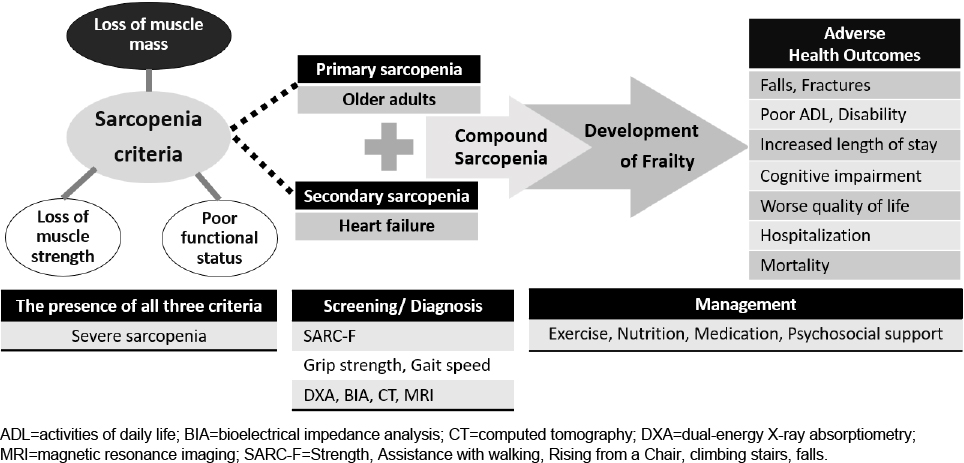
Figure 1
Definition, type, screening tools, prognosis, and management of sarcopenia.
Randomized controlled trials are necessary to determine whether a multicomponent intervention, encompassing exercise, nutrition management, and pharmacological treatment, or any of these components in isolation, is the optimal treatment for sarcopenia in various clinical settings.
Sarcopenia, a key component of frailty, is closely linked with physical disability, hospitalization, diminished quality of life, and mortality within the heart failure population. Fortunately, sarcopenia is both preventable and reversible. Therefore, it is crucial to educate healthcare professionals about the importance of prevention, early detection, and effective management of sarcopenia in patients with heart failure. Early and multifaceted interventions, such as various forms of resistance exercise and nutritional intervention, may prove beneficial in preventing adverse health outcomes in heart failure patients suffering from sarcopenia.
CONFLICTS OF INTEREST:The first author was the Editor-in-Chief of the KJAN in 2018-2020. She has currently jointed as the editorial board member of the Journal. Except for that, there is no potential conflict of interest relevant to this article.
AUTHORSHIP:
Data collection and analysis of the data - SY-J and PSH.
Interpretation of the data - SY-J and PSH.
Drafting of the manuscript - SY-J and PSH.
Critical revision of the manuscrip - SY-J and PSH.
 E-SUBMISSION
E-SUBMISSION