
Purpose
The purpose of this study was to investigate the awareness and educational demand regarding Vancomycin-Resistant Enterococci (VRE) infection control among nurses in wards with cohort isolation rooms.
Methods
A mixed-methods design was applied. Quantitative data were collected via structured questionnaires and data from 61 nurses and analyzed using SPSS for Windows version 23.0. An Importance-Performance Analysis (IPA) was conducted. Qualitative data were collected through focus groups with 12 nurses who worked in wards with VRE cohort isolation rooms, and content analysis was conducted.
Results
All items had lower performance scores than their importance scores, with significant differences. In the qualitative/descriptive analysis, the barriers to implementing VRE infection control were a lack of awareness of infection control, increased work burden, and lack of resources.
Conclusion
The findings indicate that it is necessary to develop systematic education tailored to nurses in wards with cohort isolation rooms. Furthermore, adequate resource support, distinct from the general infection control practices in other wards, is necessary. This includes considering additional infection control tasks and procedures when staffing the ward, as well as supplying equipment in accordance with cohort isolation requirements.
The purpose of this study was to investigate the awareness and educational demand regarding Vancomycin-Resistant Enterococci (VRE) infection control among nurses in wards with cohort isolation rooms.
A mixed-methods design was applied. Quantitative data were collected via structured questionnaires and data from 61 nurses and analyzed using SPSS for Windows version 23.0. An Importance-Performance Analysis (IPA) was conducted. Qualitative data were collected through focus groups with 12 nurses who worked in wards with VRE cohort isolation rooms, and content analysis was conducted.
All items had lower performance scores than their importance scores, with significant differences. In the qualitative/descriptive analysis, the barriers to implementing VRE infection control were a lack of awareness of infection control, increased work burden, and lack of resources.
The findings indicate that it is necessary to develop systematic education tailored to nurses in wards with cohort isolation rooms. Furthermore, adequate resource support, distinct from the general infection control practices in other wards, is necessary. This includes considering additional infection control tasks and procedures when staffing the ward, as well as supplying equipment in accordance with cohort isolation requirements.
Bacterial antimicrobial resistance has emerged as a significant global health issue [1]. A report on antimicrobial resistance suggests that if this problem continues unabated until 2050, an estimated 10 million people worldwide could die annually due to complications related to antimicrobial resistance [2]. Vancomycin-Resistant Enterococci (VRE) have developed resistance to glycopeptide antibiotics, including vancomycin [3]. The incidence of VRE infections is on the rise, correlating with an increase in the number of chronic and immunocompromised patients, as well as the frequency of invasive procedures and surgeries [4]. In Asian countries, the prevalence of VRE infections is 10.8%, a rate lower than that of the USA but higher than Europe [5]. In South Korea, the incidence rate increased from 0.05 per 1,000 patient-days in 2013 to 0.07 in 2020 [6]. Furthermore, approximately 30% of healthcare-associated enterococcal infections are known to be resistant to vancomycin [7].
The current guidelines set forth by the Korea Disease Control and Prevention Agency (KDCA) recommend preemptive isolation for patients infected with VRE, Vancomycin-Resistant Staphylococcus Aureus (VRSA), Vancomycin Intermediate Staphylococcus Aureus (VISA), and Carbapenem-Resistant Enterobacteriaceae (CRE) [3]. Given that the isolation rate for VRE is the highest among these [3], the majority of cohort isolation rooms in wards are occupied by VRE patients. VRE infections are a significant contributor to various types of nosocomial infections and are associated with high mortality rates and poor prognoses [7]. VRE inherently resists many antibiotics, and its antimicrobial resistance gene can be easily transferred to other strains. Furthermore, there are few second-line antibiotics available to treat VRE infections. Therefore, the proliferation of VRE infections is causing concern among healthcare providers [8]. This concern extends beyond the immediate issue, as there is a growing worry about the diminishing effectiveness of antibiotics in treating VRE infections due to the increasing resistance of VRE to other antibiotics.
If VRE are isolated from an inpatient, the isolation in a single-occupancy room is required according to the KDCA Guidelines [3]. If no private room is available, the patient is isolated in a cohort isolation room with other patients from whom the same bacteria have been isolated [3]. Therefore, it is crucial that nurses working in wards with cohort isolation rooms, who frequently interact with infected patients and are at a high risk of transmitting the diseases to other patients in the same ward, fully comprehend the guidelines and implement them accurately to maintain and enhance patient health. Hospitals have recognized the significance of nurses' preventive behaviors in preventing nosocomial infections and have provided training for nurses, resulting in a relatively high level of awareness about nosocomial infections among nurses [9, 10]. However, the performance of nurses in infection control is lower than their level of awareness [11], and their practice of self-assessment and observation assessment is less than their knowledge and awareness of infection control [12]. This suggests that ongoing, systematic, hands-on training that reflects infection control guidelines and can enhance nurses' performance is necessary.
Previous studies on the awareness and performance of infection control have primarily focused on specific groups: nurses in Intensive Care Units (ICU), who are at high risk of exposure to multidrug-resistant strains [9, 11, 13], and those in long-term care hospitals, who care for older adults or patients with chronic diseases [10, 14, 15]. Despite the need for more rigorous infection control and additional training in wards with cohort isolation rooms, where patients infected with multidrug-resistant strains are housed, there has been little research examining the status of infection control or training needs specifically targeting nurses in these wards. Considering that nurses in general wards have lower knowledge and awareness of infection control [12], and that no additional infection control training is provided in wards with cohort isolation rooms, it is crucial to identify the current status of infection control and the training needs of nurses in these wards.
Importance-Performance Analysis (IPA) is a method used to evaluate the importance and performance of each attribute, and the results are presented in a matrix, divided into four quadrants for evaluation and analysis, with performance plotted on the x-axis and importance on the y-axis [16]. These four quadrants display the mean values of performance and evaluation, and a graph provides a visual comparison of relative performance and evaluation, allowing for the identification of priorities. The objective of this study was to examine the understanding of VRE infection control and its implications. This was achieved by analyzing the importance and performance of each VRE infection control attribute and evaluating the four quadrants: "Keep up the Good Work" area with high performance and high importance, "Concentrate Here" area with low performance and high importance, "Low Priority" area with low performance and low importance, and "Possible Overkill" area with high performance and low importance.
In addition to this, the study incorporated a qualitative research method, utilizing focus group interviews to explore potential improvements in each area. This mixed-method approach leveraged both qualitative and quantitative data to provide a detailed explanation of the obstacles hindering optimal infection control performance in healthcare settings, as well as areas requiring improvement. This is because awareness and performance regarding the importance of infection control are often insufficient in practical settings. Consequently, the aim of this study was to identify the significance and performance of VRE infection control in wards equipped with VRE cohort isolation rooms, investigate the barriers and areas needing development in implementing VRE infection control, and advocate for improvements in training and infection control within wards containing cohort isolation rooms.
The study employed a mixed-methods research approach, featuring an exploratory sequential design. IPA was used to assess their awareness and performance regarding VRE infection control. Additionally, a qualitative research method (specifically, focus group interviews) was used to identify barriers and potential areas for improvement in VRE infection control practices.
The participants of this study were nurses employed in tertiary hospital wards with cohort isolation rooms in B Metropolitan City. Specifically, the selected nurses had over three months of experience in these settings, understood the study's objective, and voluntarily agreed to participate. This selection criterion was based on a previous study, which highlighted the challenges of evaluating the work performance of newly hired nurses with less than three months of experience due to their lack of practical experience [17]. Consequently, these nurses were excluded to ensure an accurate assessment of importance and performance. Unit managers were also excluded, as they do not directly provide patient care and their job responsibilities differ significantly.
The G*Power program was used to calculate the minimum sample size with statistical validity, using an effect size of 0.5, which was chosen with reference to the effect size of 0.46 from a previous study that measured the difference between awareness and performance of hospital infection control among ICU nurses [18]. The type I error was set at .05 and the power at .80, which resulted in a required sample size of 51 for the paired t-test. Accounting for a potential dropout rate of 20%, the questionnaire was distributed to 61 subjects. Ultimately, all 61 completed questionnaires were analyzed.
The study participants were nurses working in tertiary hospital wards equipped with cohort isolation rooms in B Metropolitan City. These participants were selected using a purposive sampling method. Given that a nurse's performance may vary based on their experience, we divided the focus groups into three categories as per Jang's clinical career development model [19]: the novice group (comprising nurses with less than 2 years of experience), the advanced beginner group (comprising nurses with more than 2 years but less than 4 years of experience), and the proficient group (comprising nurses with more than 4 years of experience). Each group consisted of four individuals, resulting in a total of 12 interviewees. The participants' ages ranged from 23 to 41 years, with an average age of 27.8 years. Ten of the nurses held a bachelor's degree or higher. On average, the participants had been working in wards with cohort isolation rooms for a period of 3 years and 1 month.
For this study, a new tool was developed to assess the importance and performance of VRE infection control. This tool was based on the Management of Multidrug-Resistant Organisms in Healthcare Setting [20] issued by the Centers for Disease Control and Prevention (CDC) and the Guidelines for the Prevention and Control of Healthcare Associated Infections [3] published by KDCA. While tools for measuring infection control in healthcare settings have been utilized in numerous studies [9, 12, 14], this particular tool was created due to the lack of tools specifically focusing on VRE infection control and cohort management. The newly developed questionnaire comprises 16 questions: 4 pertain to hand hygiene, 8 to cohort control, and the remaining 4 to environmental management. A 4-point Likert scale is incorporated, allowing participants to indicate the level of importance and their personal performance. The questionnaire underwent a content validity test, verified by two physicians specializing in infectious diseases and two infection control experts in tertiary hospitals located in Busan, and two nursing professors. They were requested to assign a score to each question and provide feedback on any areas that might need correction or could be considered invalid. Their comments were then used as a reference to finalize the questionnaire. Every question achieved a Content Validity Index (CVI) of over 80%, with the total CVI being .98.
The significance of VRE infection control was evaluated using the following scale: 1 point for "not at all important," 2 points for "not very important," 3 points for "somewhat important," and 4 points for "very important." The tool's Cronbach's α was .74. The execution of VRE infection control was assessed similarly: 1 point for "never do it," 2 points for "rarely do it," 3 points for "often do it," and 4 points for "always do it." The tool's Cronbach's α for this measure was .78.
The questionnaire included six questions to gather general information about the participants: their age, educational level, total years of work experience, years of experience in current department, job position, and prior experience with infection control training.
Based on the findings of quantitative research, we selected questions related to nurses' awareness of VRE infection control in wards with VRE cohort isolation rooms for use in focus group interviews. The study employed open-ended questions such as, "What is the current state of nurses' VRE infection control?", "What obstacles exist in implementing VRE infection control?" and "What do you believe is necessary for effective and efficient VRE infection control?"
Data for quantitative research were collected from November 16 to 21, 2020. The nursing department of a tertiary hospital in B Metropolitan City granted permission for the study. After obtaining written consent and explaining the purpose and methodology of the study, questionnaires were distributed in person. The completed questionnaires and consent forms were then collected and sealed in envelopes for confidentiality.
Data for qualitative research were collected from December 1 to 15, 2020. Among the nurses who participated in the study, those recommended by the head nurse in the ward were selected. This selection was based on their understanding of the study and their ability to provide appropriate responses. These nurses were then contacted to gauge their willingness to participate in the interview. They were provided with an explanation about the study's objective and process, and were asked to complete a written consent form. Only those who agreed to these terms were interviewed. The interviews took place in a conference room within the ward. Each group participated in a single interview, with the novice group taking 35 minutes, the advanced beginner group taking 50 minutes, and the proficient group taking 1 hour.
The data were analyzed using SPSS for Windows version 23.0 (IBM Corp., Armonk, NY, USA) program, in line with the objectives of this study. We analyzed the general characteristics of the participants using frequency and percentage. The importance and performance of VRE infection control were evaluated using mean and standard deviation. We analyzed the differences between the importance and performance of VRE infection control using paired t-test analysis. The priority given to VRE infection control by the participants was determined using the IPA method.
Each interview was recorded and transcribed for the purpose of data analysis, with the transcribed data being examined through the use of a qualitative content analysis method [21]. One researcher involved in this study had previously conducted qualitative research on multiple occasions, while two others had experience working in wards with VRE cohort isolation rooms and implementing infection control measures. This provided the researchers with a heightened sensitivity to understanding the context and content of the interviews regarding participants' experiences with infection control. The specific methods of data analysis were as follows: 1) the researchers thoroughly read the data multiple times to fully grasp the context and uncover the essence of the content; 2) the researchers individually identified and noted words or phrases that encapsulated core thoughts or concepts, thereby establishing units of analysis; 3) the researchers grouped similar words or phrases into sub-categories; and 4) the researchers then synthesized and abstracted the categorized content to derive the final topics.
This study received approval (No. 20-0163) from the Bioethics Review Committee at B Hospital, ensuring the protection of all participants. For the quantitative research component, questionnaires were gathered using a collection box, which was retrieved by the researchers themselves. Participants were informed that all materials related to the study, including questionnaires, recordings, transcribed data, and anonymized personal information, would be securely stored on a password-protected computer and responsibly discarded after three years. Prior to the focus group interviews, the researchers took additional steps to safeguard participants' ethical rights. They thoroughly explained the study's objectives, research methods, and recording procedures to all participants. Furthermore, they assured participants that their anonymity would be maintained and that they had the right to withdraw from the study at any time.
The average age of participants in this study was 28.16±5.29 years. Regarding educational level, 12 participants held an associate degree (19.7%), 47 held a bachelor's degree (77.0%), and 2 held a master's degree (3.3%). The average total work experience was 5.86±5.20 years, while the average work experience in the current department was 3.65±2.41 years. In terms of job titles, 50 participants were general nurses (82.0%) and 11 were head nurses (18.0%). Of the total, 44 participants (72.1%) had received training on VRE infection control, while 17 (27.9%) had not (Table 1).
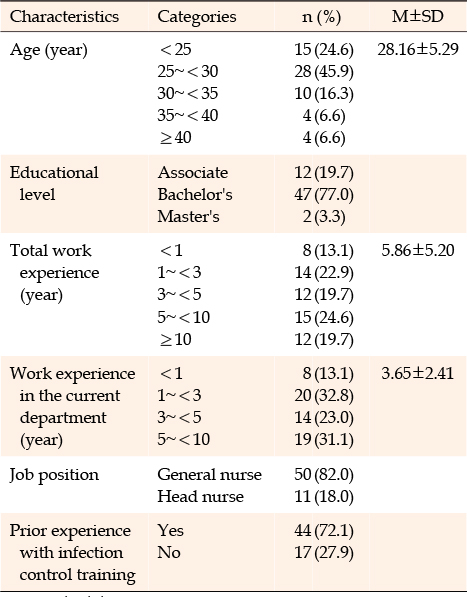
Table 1
Characteristics of the Participants (N=61)
On average, participants rated the importance of VRE infection control at 3.80±0.19 out of a possible 4 points per question. Their performance, however, was rated lower at 2.73±0.24 out of 4 points per question. The perceived importance was significantly higher than the performance across all items (Table 2).
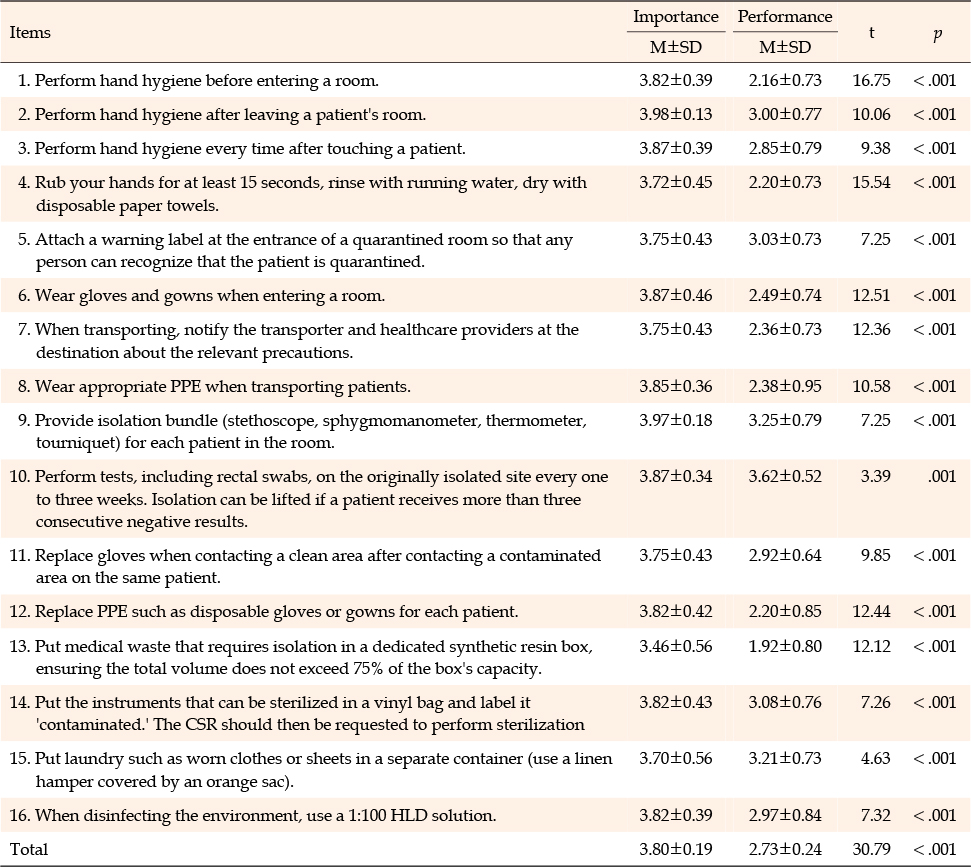
Table 2
Differences between Importance and Performance of VRE Infection Control (N=61)
In terms of importance, item No. 2, "Perform hand hygiene after leaving a patient's room," received the highest average score of 3.98±0.13. Conversely, item No. 13, "Place medical waste that requires isolation in a dedicated synthetic resin box, ensuring the total volume does not exceed 75% of the box's capacity," received the lowest average score of 3.46±0.56. Regarding performance, the item No. 10, "Perform tests, including rectal swabs, on the originally isolated site every one to three weeks. Isolation can be lifted if a patient receives more than three consecutive negative results," received the highest average score of 3.62±0.52. However, item No. 13, "Place medical waste that requires isolation in a dedicated synthetic resin box, ensuring the total volume does not exceed 75% of the box's capacity," received the lowest average score of 1.92±0.80.
The results from the IPA analysis are displayed in Table 3 and Figure 1. The importance and performance values were segmented into four quadrants, based on an average score of 3.80 for importance and 2.73 for performance, and are presented in a matrix format. These four quadrants are labeled as follows: "Keep up the Good Work" (first quadrant), "Concentrate Here" (second quadrant), "Low Priority" (third quadrant), and "Possible Overkill" (fourth quadrant). Notably, no items fell into the Possible Overkill quadrant.
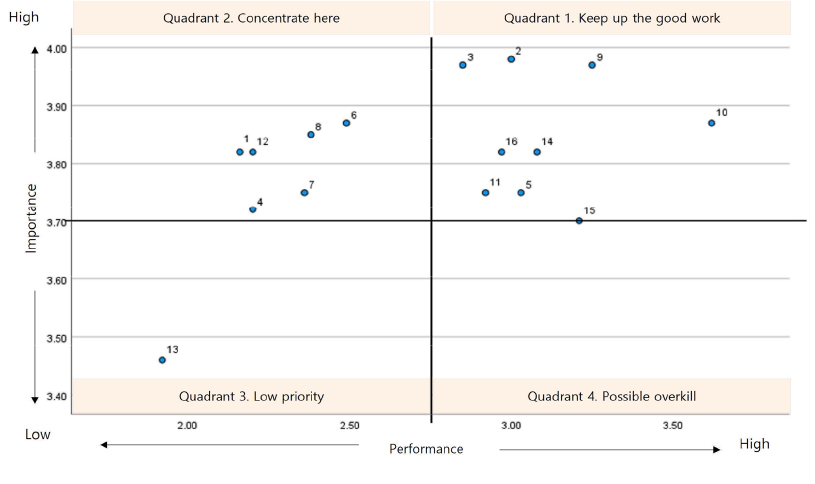
Figure 1
Importance-performance analysis matrix for vancomycin-resistant enterococci infection control.
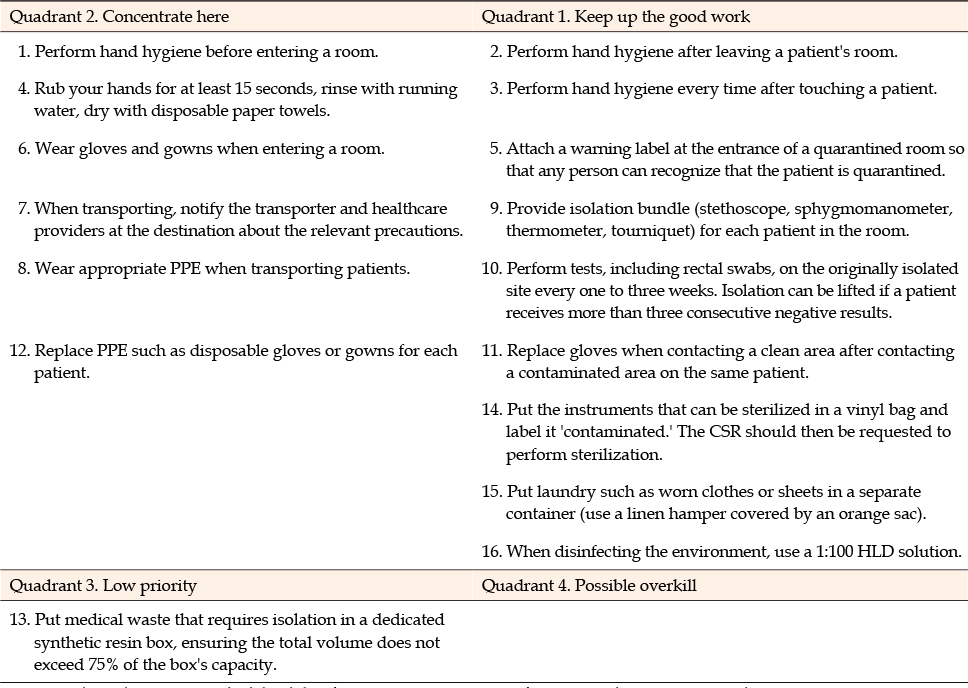
Table 3
IPA Matrix for VRE Infection Control
The "Keep up the Good Work" area (first quadrant), which showed high performance and high importance included the following items: No. 2. "Perform hand hygiene after leaving a patient's room," No. 3. "Perform hand hygiene every time after touching a patient," No. 5 "Attach a warning label at the entrance of a quarantined room so that any person can recognize that the patient is quarantined," No. 9 "Provide an isolation bundle (stethoscope, sphygmomanometer, thermometer, tourniquet) for each patient in the room," No. 10 "Perform tests, including rectal swabs, on the originally isolated site every one to three weeks. Isolation can be lifted if a patient receives more than three consecutive negative results," No. 11 "Replace gloves when contacting a clean area after contacting a contaminated area on the same patient," No. 14. "Put the instruments that can be sterilized in a vinyl bag and label it'contaminated.' The Central Supply Room (CSR) should then be requested to perform sterilization." No. 15 "Put laundry such as worn clothes or sheets in a separate container (use a linen hamper covered by an orange sac), and No. 16 "When disinfecting the environment, use a 1:100 HLD solution."
The "Concentrate Here" area (the second quadrant), which showed high importance but low performance, included items No. 1 "Perform hand hygiene before entering a room," No. 4 "Rub your hands for at least 15 seconds, rinse with running water, dry with disposable paper towels." No. 6 "Wear gloves and gowns when entering a room," No. 7 "When transporting, notify the transporter and healthcare providers at the destination about the relevant precautions," No. 8 "Wear appropriate Personal Protective Equipment (PPE) when transporting patients," and No. 12 "Replace PPE such as disposable gloves or gowns for each patient."
The "Low Priority" area (the third quadrant), with low importance and low performance, included item No. 13 "Put medical waste that requires isolation in a dedicated synthetic resin box, ensuring the total volume does not exceed 75% of the box's capacity."
According to the results, three general categories including six subcategories were derived as obstacles to the performance of VRE infection control. The three general categories were: "lack of awareness about VRE infection control," "increased workload," and "lack of resources." The six subcategories were: "complacency regarding the risk of infection transmission," "uncertainty about infection control activities due to the lack of systematic training," "burden of providing nursing care for patients from various divisions," "lack of space," and "lack of infection control resources." The specifics for each category are detailed below. To maintain anonymity, each participant's name has been replaced with a combination of their group name and a unique number assigned to them. The groups were denoted as 1 (novice), 2 (advanced beginner), and 3 (proficient).
Participants recognized the importance of infection control measures, including hand washing, maintaining hand hygiene, and managing medical equipment and supplies when caring for patients in VRE cohort isolation. However, they admitted there were instances when they did not adhere to these guidelines, under the mistaken belief that their actions would not contribute to the spread of infection.
Even though I know about the basics of infection control, I believe not all instructions are consistently followed due to a mindset of 'this should be fine.' For example, when I'm rushed during a blood test, I know I should use a new tourniquet for each patient. However, if I don't see a tourniquet nearby and I'm in a hurry, I might use another patient's tourniquet. (P1-1)
I understand that each patient requires a fresh gown and gloves. However, when I put on gloves, I often think, 'It should be fine as long as I don't directly touch the patient.' Likewise, sometimes I don't wash my hands. (P2-1)
Participants expressed concern that they had not received specific instructions or guidelines for caring for patients infected with multidrug-resistant bacteria, despite encountering such cases daily. There was evident uncertainty among participants about whether their infection control measures met the standard. They expressed a desire for more systematic training, particularly because their primary patients were infected with VRE.
It seems there are no guidelines or training materials I can refer to when caring for VRE patients. There are some cyber trainings, but I usually ask senior nurses to do things for infection control. More systematic training materials or guidelines would help explain VRE to patients and their families… (P1-2)
There are general guidelines I can refer to, but the details of the instructions for clinical practice are not very specific. So, I get confused and wonder whether I'm doing it right. (P3-1)
Participants expressed that an excessive workload was an obstacle. They noted that the workload associated with caring for VRE patients is greater than that for general patients, yet the same number of nurses are assigned to VRE patients' rooms as per the guidelines for general patients. This discrepancy was identified as a factor contributing to their passive approach towards infection control activities, as they feel overwhelmed by time constraints and psychological stress. Participants expressed a desire for the assignment of an appropriate number of nurses, taking into account the actual workload for VRE-infected patients.
When caring for patients in general rooms, I can disinfect my hands for each patient, but when caring for patients in VRE cohort isolation rooms, I need to replace my gown, disinfect my hands, and do it really quickly since there are so many patients to take care of. These infection control activities take so much time, so I think that's why I can't properly replace my gown or perform hygiene activities. (P2-2)
The severity of VRE-infected patients is different from that of general patients. They have different conditions. There is a lot of work to provide them proper care, but the number of patients we are assigned to per person in VRE cohort isolation rooms is the same as for general patients' rooms. I think this is the burden. (P3-2)
According to KDCA guidelines [9], a patient diagnosed with a VRE infection should be isolated in either a single-occupancy room or a cohort isolation room. Consequently, the cohort isolation room may house patients transferred from various divisions. Participants particularly expressed difficulty in communicating with diverse medical staff from different divisions and in implementing unfamiliar prescriptions.
The infected patients are usually from different divisions, but I still have to care for them, so there is a burden due to the workload. When implementing directions or prescriptions, as different divisions order different things, I need to ask again and again, I still have to take care of other general patients at the same time. (P2-2)
Participants indicated that the spacing between beds in VRE cohort isolation rooms adheres to guidelines, but the limited space poses challenges for preventing patient contact and facilitating transportation. Additionally, they expressed concerns about housing general patients and those infected with VRE in the same ward, as it hinders the effective implementation of infection control measures.
VRE-infected patients tend to have a lot of drainage tubes and their conditions are quite severe. But the space is limited. It happens that patients' beds bump into each other, but there should be more distance for infection control. But due to the lack of space, it doesn't work well. (P2-3)
The instructions dictate that patients can leave the room only when getting a treatment or undergoing surgery, but that doesn't make sense in reality. Even though we repeat the instructions over and over, VRE patients try to get out of the room and walk places. Then it's impossible to prevent them from contacting other patients. (P3-1)
Infection control guidelines state that any item to be shared among VRE-infected patients must be thoroughly cleaned and disinfected. However, certain high-cost equipment, such as oxygen saturation measuring machines or Personal Digital Assistants (PDAs), cannot be disinfected, and their exclusive use for VRE patients is challenging due to resource limitations. Consequently, the participants expressed a desire for an adequate supply of dedicated equipment for VRE-infected patients in cohort isolation rooms, to facilitate effective infection control.
PDAs and SpO2 machines are not exclusively assigned to VRE patients. So after using them, we are supposed to disinfect them for general patients. This is not practically possible and inconvenient. I hope there will be more supplies dedicated to VRE-infected patients. (P1-3)
The study aimed to provide basic data to aid in the development of VRE infection training programs. This was achieved by examining the understanding and implementation of VRE infection control measures, as well as identifying potential barriers and areas for improvement. The results, obtained through the IPA analysis method, revealed varying levels of importance and performance regarding VRE infection control. Out of 16 items, six fell into the "Concentrate Here" category, nine into the "Keep up the Good Work" category, and one into the "Low Priority" category. In addition to quantitative research, the study also employed qualitative research methods, specifically focus group interviews. The interviews identified three main obstacles to infection control: "Lack of Awareness about VRE Infection Control," "Increased Workload," and "Lack of Resources," each of which was further divided into two subcategories.
All infection control measures for VRE demonstrated significantly lower performance levels compared to their perceived importance. These findings align with previous studies that examined the awareness of multidrug-resistant bacterial infection control among ICU nurses [9, 11], long-term care hospital nurses [22], and tertiary hospital nurses [12, 23]. These studies suggest that the execution of infection control is influenced by various conditions and practical limitations, despite nurses' recognition of its importance. Numerous studies have identified contributing factors at the personal level, such as knowledge, awareness, personal beliefs, and empowerment [12, 13, 23, 24]. However, as highlighted by this study's qualitative findings, a combination of factors is at play. In addition to personal factors such as a lack of awareness, relevant environmental factors include workload and a lack of infection control resources [25, 26], and structural contributors include the lack of systematic training [27, 28].
The study utilized the IPA analysis method to examine the understanding and implementation of VRE infection control measures. The results revealed that the "Concentrate Here" area (the second quadrant) contained two items related to hand hygiene: "Perform hand hygiene before entering a room," and "Rub your hands for at least 15 seconds, rinse with running water, dry with disposable paper towels." Hand hygiene was consistently practiced upon exiting a room, but was less frequently observed before entering a room. This discrepancy could potentially increase the risk of superinfection, whereby patients infected with VRE could also contract other multidrug-resistant bacteria. The Guideline for Isolation Precautions in Healthcare Settings, published by the Hospital Nurses Association, emphasize the importance of performing hand hygiene both before and after patient contact, assigning it a high priority level (Recommendation Priority Level A) and strongly advocating for its implementation in practical settings [25]. Despite this, the results indicate that hand hygiene is not consistently practiced before entering a room, and the prescribed method is not always adhered to, even though it is a fundamental aspect of nursing. The qualitative research results suggest that a complacent attitude, such as thinking "it should be fine," contributes to this low performance, despite a high awareness of its importance. This awareness needs to be enhanced by emphasizing the potential consequences of poor hand hygiene during infection control training sessions. The perception of risk plays a significant role in promoting healthy behaviors [29]. Given previous research findings that improved hand hygiene practices can effectively reduce the incidence of multidrug-resistant bacterial infections [27], it is crucial to emphasize to nurses in cohort isolation rooms that hand hygiene is a top priority in infection prevention.
The "Concentrate Here" area related to PPE usage included items such as "Wear gowns and gloves when entering a room," "Wear proper PPE when transporting a patient," and "Replace PPE (disposable gloves or gowns) for each patient." PPE serves as a protective barrier for both healthcare providers and patients, and it is crucial to replace it after each interaction with a patient who has an infectious disease to prevent the spread of infections [3]. Zachary et al. [30] found that 23% of patients who initially tested negative became infected with VRE after receiving care. The study also revealed that 63% of healthcare workers' gloves and 73% of their gowns tested positive for VRE. These findings suggest a high risk of infection transmission via the PPE used by healthcare staff. The qualitative research component of this study identified factors such as nurses struggling to change masks, gloves, or gowns due to heavy workloads and the demanding nature of the process, despite understanding the importance of properly wearing and changing PPE when entering rooms or transporting patients. This finding is supported by previous studies, in which 73.5% of respondents reported feeling pressed for time to comply with all standards [26]. Jackson et al. [31], in their prospective cohort study of VRE patients, identified independent risk factors for transmitting VRE to healthcare staff, including skin contact with patients and the process of transporting patients. They emphasized the importance of proper safety measures to minimize contact. Therefore, it can be concluded that monitoring systems or policy-level interventions are needed to ensure that all healthcare staff correctly use PPE.
In this study, the "Keep up the Good Work" area included 9 out of 16 items, on topics such as hand hygiene after touching a patient, hand hygiene when touching a patient, preparing patients' individual supplies, creating marks for patients with infectious diseases, VRE test standards, disinfection, and cleaning standards. Regarding hand hygiene, 88.8% of hospitals monitor hand hygiene practices, and 88.1% actively promote the importance of hand hygiene [32]. It is inferred that medical staff generally adhere well to hand hygiene guidelines. Notably, given the potential for hand contamination after contact with VRE patients, there appears to be a high level of awareness that hand hygiene practices, such as hand washing, are essential. The marking of patients with infectious diseases, preparation of individual patient supplies, VRE testing, and disinfection and cleaning are primarily conducted in accordance with hospital guidelines. These practices are influenced by the availability of disinfection and cleaning supplies and equipment [28]. The qualitative data from this study corroborates these findings, with nurses reporting that space and infection control supplies are insufficient for adhering to the guidelines. To enhance the performance in the " Keep up the Good Work " area, it is necessary to improve the medical staff's infection control capabilities. Additionally, medical institutions should provide adequate resources and monitor infection control status.
The "Low Priority," area with a low awareness of importance and a low level of performance, included one item: "Put medical waste that requires isolation in a dedicated synthetic resin box, ensuring the total volume does not exceed 75% of the box's capacity" According to the Guideline for Isolation Precautions in Healthcare Settings, the waste generated by quarantined patients should be dumped in a dedicated synthetic resin box; however, the evidence basis for this statement is categorized as Level II, which refers to insufficient or unclear evidence [25]. While this rule is currently recommended for implementation in clinical settings, further research is necessary to adequately substantiate the safe treatment of medical waste.
Twelve nurses employed in wards with VRE isolation rooms participated in the focus group interviews for this study. The analysis of the results revealed the first category, "lack of awareness about infection control," which included items such as "complacency regarding the risk of infection transmission," and "uncertainty about infection control activities due to the lack of systematic training." As new infectious diseases emerge globally, South Korea revised its medical laws in 2016. This revision mandated that tertiary hospitals and medical institutions with more than 100 beds establish an infection control committee and an infection control center. It also required medical staff responsible for infection control to complete 16 hours of infection control training annually [6]. However, the participants in this study, who are nurses working in wards with VRE isolation rooms, expressed a desire for more practical and systematic training. Kim et al. [28] reported in a focus group interview with nurses in the infection control division that training combining theoretical and hands-on courses, as well as systematic training that includes introductory, basic, and advanced courses, was found to be beneficial. It is suggested that for nurses directly interacting with and caring for VRE cohort patients, more structured and practical training should be developed. By providing high-quality training to nurses responsible for caring for VRE-infected patients, these nurses can gain a better understanding of infection control, enhance their knowledge and skills, and strengthen their confidence in performing their duties. This will ultimately contribute to the improvement of patient health.
The second category, "increased workload", included "burden of providing nursing care for patients from various divisions" and "work overload due to added infection control activities." According to Korean medical law, the required number of nurses for a ward is determined by the hospital's bed count [28], and this rule also applies to wards with cohort isolation rooms. Despite the heavier workload in wards with cohort isolation rooms compared to general wards-due to additional processes and duties imposed by infection control guidelines-the law inadvertently leads to nurse overwork. This issue stems from the lack of a standard for assigning nurses to care for patients infected with multidrug-resistant bacteria. A policy-level change is necessary to thoroughly examine staffing status and improve working conditions. Moreover, for cohort isolation rooms, an analysis of nurses' duties is needed to ensure the appropriate number of nurses are assigned to these wards and that their workload is properly distributed.
The third category, "lack of resources," contained the subcategories of "lack of space" and "lack of infection control resources." Despite recommendations for patients to utilize their personal items, there are limitations due to the insufficiency of some resources for all patients. Jung and Park [33] conducted a study on the barriers to infection control among hemodialysis patients and reported that one of the primary obstacles was a "lack of PPE." This finding aligns with the results of our study. This hurdle cannot be surmounted solely through the efforts of individual nurses; support at the hospital level is necessary. Medical institutions should gather feedback directly from the medical staff who are actively caring for patients with VRE infections, and foster an environment that enables the medical staff to work efficiently.
This study, which employed a convenience sampling method, focused on nurses in wards with VRE cohort isolation rooms in a tertiary hospital located in City B. As such, its findings may not be universally applicable to all hospitals in Korea. Consequently, further research encompassing various hospital sizes and regions is necessary. Despite these limitations, this study investigated nurses' understanding of infection control and identified barriers to high performance in this area. It also proposed potential causes for subpar performance and suggested methods for improvement. These findings provide foundational data for the development of VRE infection control training programs.
This study conducted a comprehensive investigation of nurses' awareness of VRE infection control in wards with VRE cohort isolation rooms. The review was carried out through quantitative research using the IPA analysis method and qualitative research using focus group interviews. The study's significance lies in its ability to bridge the gap between infection control guidelines and actual practice. It also identified the direction for infection control training suitable for wards with VRE cohort rooms by pinpointing the obstacles to low awareness and poor performance of VRE infection control in these wards. Overall, the results showed that while nurses have a high level of awareness of VRE infection control, their performance level is low. The barriers to high performance were found to be a complacent attitude towards infection control, an increased workload, and a lack of resources. Existing training programs need to be enhanced to emphasize the risk of transmission of infectious diseases and to eliminate complacent attitudes. Additionally, new systematic training programs, tailored for nurses in wards with cohort isolation rooms whose primary responsibilities involve infection control, should be developed. Lastly, wards with cohort isolation rooms need to be managed differently from general wards, taking into account actual practice. The placement of nursing staff should consider the additional tasks of infection control and its processes, and adequate supplies must be provided for cohort isolation rooms.
CONFLICTS OF INTEREST:Jeonghyun Cho has been the Associate Editor of the Korean Journal of Adult Nursing since 2022. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - WY, CJ and PE.
Data collection - WY and PE.
Analysis and interpretation of the data - WY, CJ and PE.
Drafting and critical revision of the manuscript - WY, CJ and PE.
 E-SUBMISSION
E-SUBMISSION