
Purpose
The purpose of this study was to investigate the moderating role of positive psychological capital on the effects of clinical nurses' responses to violence on burnout and to provide basic date for an intervention program that reduces nurse burnout.
Methods
The participants in this study were 172 nurses recruited through convenience sampling at one general hospital in Seoul. Data were collected from June 5 to 10, 2023 using structured questionnaires. The collected data were analyzed using SPSS/WIN 26.0.
Results
Burnout was positively correlated with violence responses and negatively correlated with positive psychological capital among clinical nurses. Verbal violence experience (β=.14, p=.014), job satisfaction (β=.31, p<.001), social violence response (β=.15, p=.035) and positive psychological capital (β=-.39, p<.001) were identified as factors significantly influencing clinical nurses' burnout. The interaction term between social violence response and positive psychological capital significantly influenced burnout (β=.18, p=.044).
Conclusion
Social violence response affected burnout among clinical nurses, and positive psychological capital was identified as a moderating factor in burnout. Therefore, hospital and nursing organizational efforts such as fostering an appropriate organizational atmosphere, providing social support that encourages trust and creativity among organizational members, and implementing various educational and mentoring programs are required to reduce nurses' social violence response and enhance positive psychological capital.
The purpose of this study was to investigate the moderating role of positive psychological capital on the effects of clinical nurses' responses to violence on burnout and to provide basic date for an intervention program that reduces nurse burnout.
The participants in this study were 172 nurses recruited through convenience sampling at one general hospital in Seoul. Data were collected from June 5 to 10, 2023 using structured questionnaires. The collected data were analyzed using SPSS/WIN 26.0.
Burnout was positively correlated with violence responses and negatively correlated with positive psychological capital among clinical nurses. Verbal violence experience (β=.14, p=.014), job satisfaction (β=.31, p<.001), social violence response (β=.15, p=.035) and positive psychological capital (β=-.39, p<.001) were identified as factors significantly influencing clinical nurses' burnout. The interaction term between social violence response and positive psychological capital significantly influenced burnout (β=.18, p=.044).
Social violence response affected burnout among clinical nurses, and positive psychological capital was identified as a moderating factor in burnout. Therefore, hospital and nursing organizational efforts such as fostering an appropriate organizational atmosphere, providing social support that encourages trust and creativity among organizational members, and implementing various educational and mentoring programs are required to reduce nurses' social violence response and enhance positive psychological capital.
Hospital violence, which includes verbal and physical violence, physical threats, sexual violence, harassment, and bullying, poses a significant threat to the safety and well-being of staff in all work-related situations [1]. The high expectations for quality service in healthcare, coupled with patient anxiety and concerns about illnesses, as well as dissatisfaction with treatment outcomes, can often lead to expressions of anger and frustration from patients and their families. Nurses, who are tasked with maintaining therapeutic relationships, frequently find themselves on the receiving end of such violence [2, 3]. Moreover, nurses' interactions with various hospital staff members can also lead to conflicts due to excessive workloads and the constant state of readiness for emergencies, resulting in different forms of violence [4]. A staggering 95.5% of clinical nurses in South Korea have reported experiencing verbal violence, physical threats, and physical violence across various departments. The main instigators of this violence were identified as patients (83.5%) and their families (90.8%). However, physicians and fellow nurses also contributed significantly to these incidents, accounting for 78.2% and 62.3% respectively [5].
Nurses who have been subjected to violence often display emotional reactions such as anger, irritation, and depression. They may also experience physical symptoms including headaches, insomnia, and general tension. These individuals may find it challenging to attend work, notice changes in their relationships with colleagues, and even develop a fear of patients [6]. As these violence responses accumulate, they can lead to increased stress levels, which in turn can contribute to nurse burnout [7]. Furthermore, this burnout can extend to other nurses, resulting in decreased job satisfaction, diminished enthusiasm for work, a heightened intention to leave the job, reduced organizational productivity, and widespread organizational burnout [1, 3, 7, 8]. This situation has serious implications for the management of the nursing workforce and the quality of nursing care. It can lead to an increase in patient safety errors and negatively impact the patients who are receiving nursing services [1, 7]. As such, interventions are necessary to mitigate nurse burnout caused by violence responses and to improve the quality of nursing care.
Various strategies are employed to prevent hospital violence, including the development of violence prevention policies, training for violence prevention and response, and enhancements to the work environment [3]. However, these strategies may not fully alleviate the negative reactions and burnout that individuals experience when violence occurs. Even with rigorous implementation of violence prevention measures, unexpected violence can still occur, potentially intensifying negative reactions [8]. To prevent and reduce burnout, it is important to consider both external factors, such as the nursing work environment, social support, and salary satisfaction, and internal factors, such as self-efficacy, resilience, professional self-concept, and interpersonal skills. However, research suggests that internal factors may have a more positive effect on reducing burnout than external factors [7]. Therefore, it is crucial to identify and strengthen nurses' internal resources.
Positive psychological capital, an internal resource of an individual, comprises four interconnected positive psychological states: self-efficacy, hope, optimism, and resilience [9]. This form of capital positively influences job stress, anxiety, and turnover intention by reducing them, while simultaneously enhancing organizational commitment, job satisfaction, and job performance [10]. Furthermore, positive psychological capital can be enhanced through development and training [9], which can serve as a crucial strategy for mitigating nurse burnout, decreasing turnover rates, and sustaining a proficient nursing workforce [11]. A meta-analysis [12] revealed that positive psychological capital had the most substantial effect on reducing nurse burnout. It encourages nurses to fulfill their nursing responsibilities, assists them in overcoming challenges, and fosters positive perceptions, thereby diminishing negative attitudes and burnout towards patients. Consequently, positive psychological capital can serve as a factor in enabling nurses to effectively manage negative violence responses, foster positive perceptions of patients, and motivate them to carry out their nursing duties, ultimately reducing burnout.
Prior studies focused on nurses have noted that an elevated level of positive psychological capital correlates with a decrease in burnout [13]. Additionally, increased resilience is associated with diminished negative responses to violence and a reduction in burnout [14]. Resilience also moderates the effects of post-traumatic stress disorder [15], while self-efficacy influences the regulation of burnout [16]. Both resilience and self-efficacy are subcomponents of positive psychological capital [9]. Given that post-traumatic stress is a contributing factor to burnout [7], it can be inferred that positive psychological capital may moderate nurse burnout. Moreover, research [17] investigating the correlation between customer misbehavior and burnout suggests that positive psychological capital can help manage burnout. This supports the notion that positive psychological capital can assist nurses in controlling burnout that may arise in situations where they encounter violence. Consequently, it is crucial to evaluate the emotional, physical, and social responses to violence, as well as the levels of positive psychological capital and burnout in clinical nurses. This evaluation will provide the foundation for the development of nurse burnout reduction programs that leverage positive psychological capital, by elucidating the moderating effect of positive psychological capital on the relationship between responses to violence and burnout.
The aim of this study was to investigate the responses of clinical nurses to violence and burnout, as well as their levels of positive psychological capital. Additionally, we aimed to verify the moderating role of positive psychological capital in the relationship between responses to violence and burnout.
This descriptive survey-based study aimed to investigate the moderating effect of positive psychological capital on responses to violence and burnout among clinical nurses.
The participants in this study were nurses with over a year's experience working in a general hospital in Seoul, which has a capacity of 700 beds. The participants were chosen through convenience sampling from those who understood the research objectives and voluntarily agreed to participate. Nurses who worked in administrative departments were not included in the study due to their limited patient contact and reduced interaction with other medical staff, which lessens their likelihood of experiencing violence. The G*Power 3.1 program was used to determine the study's sample size. Based on previous research [15], a medium effect size of 0.15, a significance level of .05, and a power of .80 for hierarchical regression analysis were considered. Taking into account a total of 15 predictor variables, including responses to emotional, physical, and social violence, positive psychological capital, and general characteristics, the study required a sample size of 139 participants. To allow for a dropout rate of 20%, 174 participants were recruited. After excluding 2 participants due to inadequate responses, a total of 172 participants were included in the final data analysis.
The general characteristics of the participants and characteristics related to violence experiences were investigated, including age, gender, marital status, education, total clinical experience, work department, work type, position, job satisfaction, social support, exposure to violence in hospitals, and perpetrators of violence.
The Korean version of the Assault Response Questionnaire (ARQ-K) was utilized to gauge responses to violence. This tool, translated into Korean by Jang and Lee [18], is based on Lanza's [19] Assault Response Questionnaire (ARQ). The ARQ-K underwent testing for construct validity and reliability. Permission to use this tool was granted via email. The ARQ-K comprises 26 items, divided into categories of emotional responses (13 items) following a violent incident in a hospital setting. These emotional responses are further divided into immediate responses (10 items) and delayed responses (3 items). The tool also measures physical responses (10 items) and social responses (3 items). Each item is scored on a 5-point Likert scale, with responses ranging from "not at all" (1) to "very much" (5). The total score can range from 26 to 130, with higher scores indicating more adverse responses to violence. The reliability of this tool was reported in the study by Jang and Lee [18], where the overall scale's Cronbach's α was .94. The Cronbach's α values for each subdomain were as follows: immediate emotional response, .91; delayed emotional response, .77; physical response, .93; and social response, .80. In this study, the overall scale's Cronbach's α was .95. For each subdomain, the Cronbach's α values were as follows: emotional response, .91; physical response, .93; and social response, .78.
Burnout was measured using 10 related items from a tool modified by Kim and Yom [20]. This tool was based on Stamm's [21] Professional Quality of Life (ProQOL) Scale Version 5, which was adapted to suit the circumstances of Korean nurses. We obtained permission to use the ProQOL from the Professional Quality of Life Measure, and Kim and Yom [20] also granted permission via email. Each item on the scale is rated from "not at all" (1) to "very much" (5). Five items (1, 2, 5, 6, 10) are reverse-scored. The total score can range from 10 to 50, with higher scores indicating a greater degree of burnout. The original instrument demonstrated a Cronbach's α of .75 according to Stamm [21] and Cronbach's α of .74 according to Kim and Yom [20], while in this study, Cronbach's α was .81.
The Psychological Capital Questionnaire (PCQ), developed by Luthans et al. [9], was used to measure positive psychological capital. This instrument was translated into Korean by Lee and Choi [22], who also confirmed its content validity and reliability. We obtained permission to use the PCQ from Mind Garden, the copyright holder, as well as from Lee and Choi [22] via email correspondence. The PCQ comprises 24 items in total, divided into four categories: self-efficacy (6 items), hope (6 items), resilience (6 items), and optimism (6 items). Each item is scored on a 6-point Likert scale, ranging from "not at all" (1) to "very much" (6). Three items (13, 20, 23) are reverse-scored. The total score can range from 24 to 144, with higher scores indicating a greater level of positive psychological capital. When the PCQ was first developed, Luthans et al. [9] reported a Cronbach's α .89, with subdomain Cronbach's α values of .85 for self-efficacy, .75 for hope, .71 for resilience, and .74 for optimism. In the study by Lee and Choi [22], the overall Cronbach's α was .93, with subdomain Cronbach's α values of .71 for self-efficacy, .93 for hope, .97 for resilience, and .91 for optimism. In the current study, the overall Cronbach's α was .94, with subdomain Cronbach's α values of .92 for self-efficacy, .88 for hope, .83 for resilience, and .75 for optimism.
Data collection for this study was conducted after obtaining approval from the Institutional Review Board (IRB) of the researcher's affiliated institution. The data collection period was from June 5 to June 10, 2023. Prior to data collection, the researcher visited each nursing department to explain the research purpose, methods, and survey content, and obtained permission to conduct the research. Data for this study were gathered via a web-based survey. Recruitment posters were distributed to each department's head nurse. After explaining the research objectives, methodologies, and survey content, and obtaining their cooperation approval, the data collection process was initiated. These recruitment posters contained links and QR codes that led to explanatory and instructional materials about participating in the research. Participants were required to fully understand this information and provide informed consent before proceeding with the survey. All collected data were coded and managed anonymously. To prevent participants from participating multiple times, their contact information, which was collected to provide tokens of appreciation upon survey completion, was used to cross-check for any duplicate participation.
This study received approval from the IRB of the researcher's affiliated institution (IRB No. 2023-04-041-001), as well as an exemption from written consent due to the web-based nature of the survey. The research informed consent statement clearly stated that the collected data would be used solely for research purposes. It also guaranteed the confidentiality of participants' personal information, underscored their right to withdraw from the research at any time, and detailed the compensation for research participation. The researcher's contact information, along with that of the Research Participant Protection Center, was provided to ensure participants could easily reach out with any questions or concerns related to their participation in the research. The collected data were coded and stored in electronically locked files, accessible only to the researcher, to maintain restricted access. Moreover, these data will be permanently disposed of three years after the research concludes. To facilitate compensation for research participation, the phone numbers of research participants were promptly deleted after the tokens of appreciation were distributed.
The collected data were analyzed using IBM SPSS/WIN 26.0 software, and the specific analytical methods were as follows:
• Descriptive statistics were used to analyze the general characteristics of participants, violence responses, positive psychological capital, and burnout levels.
• Differences in violence responses, positive psychological capital, and burnout based on participants' general characteristics were analyzed using the independent t-test and one-way ANOVA, with the Scheffé test employed for post hoc analysis.
• Pearson correlation coefficients were calculated to examine the correlations between violence responses, positive psychological capital, and burnout.
• Hierarchical regression analysis was conducted to determine the moderating effect of positive psychological capital on the impact of violence responses on burnout.
The participants' average age was 32.10±7.34 years, with women making up 95.3% of the group and men comprising 4.7%. Single participants represented 64.5% of the sample, and the highest level of education achieved by most was either a bachelor degree, accounting for 76.2% of the total. The average amount of total clinical experience was 9.01±7.34 years. The work departments were divided into 38.4% in general wards, 24.4% in operating and recovery rooms, and 23.3% in intensive care units. The majority of participants were shift workers, at 79.1%, and most held the position of a staff nurse (90.7%) rather than a charge nurse (9.3%).
In total, 74.4% of participants reported experiencing violence within the hospital setting. Specifically, 73.3% of participants reported encountering verbal violence. Those who had experienced verbal violence identified multiple sources; patients were the primary perpetrators (78.6%), followed by caregivers (54.0%), doctors (41.3%), and nurses (27.8%). Nearly half of the participants, 47.7%, reported experiencing physical threats, with the majority identifying patients (91.5%) as the patients, and caregivers following at 28.0%. Lastly, 34.9% of participants reported instances of physical violence, with patients again being the primary perpetrators (Table 1).
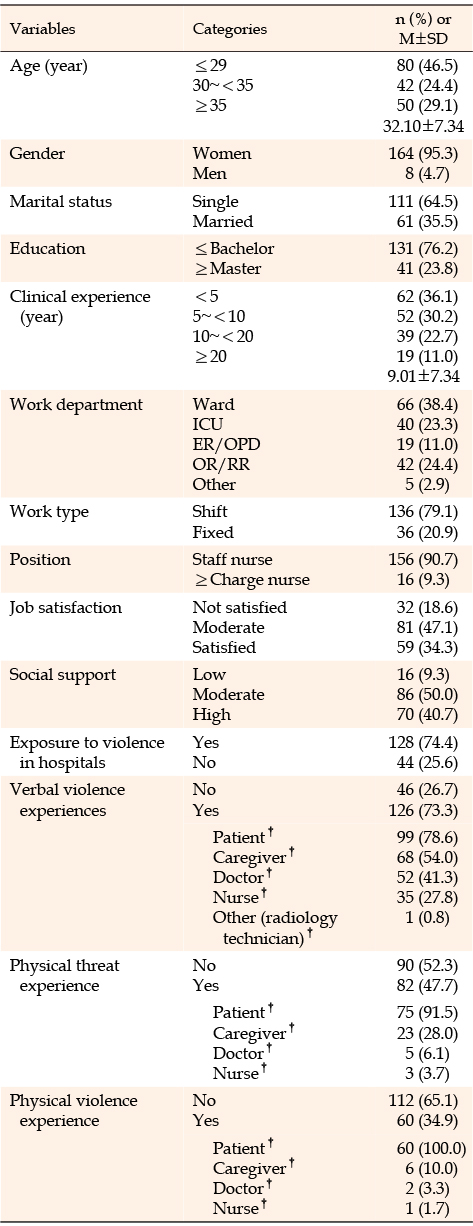
Table 1
Characteristics of Participants (N=172)
The mean total score for participants' responses to violence was 75.63±20.10, out of a possible maximum of 130, and the mean score for each item was 2.91±0.77. The mean scores for the sub-scales were as follows: emotional responses, 3.34±0.83; physical responses, 2.64±0.95; and social responses, 1.97±0.82. The average level of burnout was 30.70±5.65, while the average level of positive psychological capital was 93.25±16.08 (Table 2).
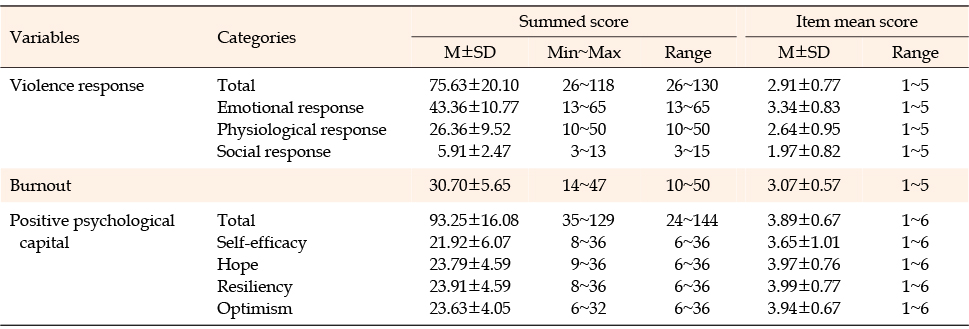
Table 2
Violence Response, Burnout, and Positive Psychological Capital of Nurses (N=172)
Violence responses showed statistically significant differences based on age (F=4.64, p=.011), clinical experience (F=3.88, p=.010), work type (t=-2.19, p=.030), and job satisfaction (F=7.15, p=.001). Nurses aged 35 and older had higher violence response scores than those aged 29 and younger. Nurses with clinical experience between 10 and 20 years had higher violence response scores than those with less than 5 years of experience. Full-time staff members had higher violence response scores than shift workers, and those with job dissatisfaction had higher violence response scores than their counterparts.
Burnout exhibited statistically significant relationships marital status (t=2.25, p=.026), job satisfaction (F=36.17, p<.001), social support (F=16.72, p<.001), and experience of verbal violence (t=3.01, p=.003). Participants who were unmarried, dissatisfied with their jobs, perceived average or lower social support, or experienced verbal violence reported higher burnout scores.
Positive psychological capital showed statistically significant differences in terms of age (F=5.94, p=.003), marital status (t=-2.40, p=.018), educational level (t=-2.05, p=.042), job satisfaction (F=12.74, p<.001), and social support (F=19.73, p<.001). Nurses aged 30 to 34 had higher positive psychological capital scores than those aged 29 or younger. Married participants and those with postgraduate-level education had higher positive psychological capital scores. Participants who were satisfied with their jobs or perceived higher social support had higher positive psychological capital scores (Table 3).
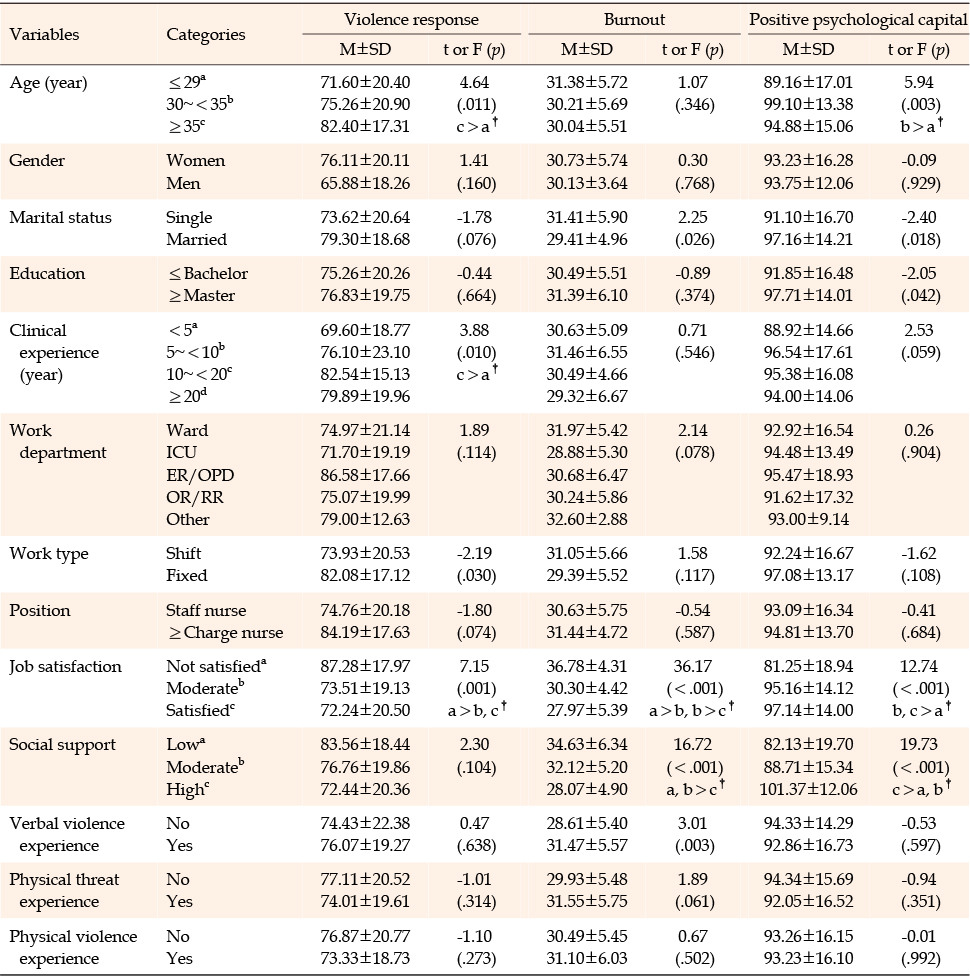
Table 3
Differences in Violence Response, Burnout, and Positive Psychological Capital according to Characteristics of Participants (N=172)
Emotional violence responses among nurses showed significant positive correlations with physical violence responses (r=.67, p<.001), social violence responses (r=.50, p<.001), and burnout (r=.32, p<.001). Physical violence responses were positively correlated with social violence responses (r=.58, p<.001) and burnout (r=.37, p<.001). Social violence responses exhibited positive correlations with burnout (r=.42, p<.001) and a negative correlation with positive psychological capital (r=-.24, p=.002). Burnout was negatively correlated with positive psychological capital (r=-.57, p<.001) (Table 4).
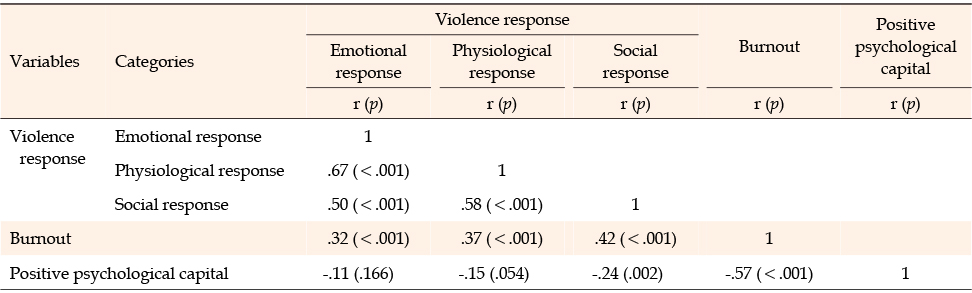
Table 4
Correlation among Violence Response, Burnout, and Positive Psychological Capital (N=172)
To examine the moderating effect of positive psychological capital on the impact of violence responses on burnout, hierarchical regression analysis was conducted. The analysis incorporated demographic variables such as age, along with factors related to burnout, including job satisfaction, social support, and experiences of verbal violence as control variables in the first step to isolate the effects of the independent variables. In the second step, the primary independent variables-namely, emotional violence responses, physical violence responses, and social violence responses-were incorporated. The third step involved the addition of the moderating variable, positive psychological capital. In the fourth step, interaction terms between each violence response and positive psychological capital were included to ascertain their potential significant impact on burnout (Table 5). To mitigate potential multicollinearity issues between the independent and moderating variables, the variables were mean-centered prior to analysis. The assumptions of normality, homoscedasticity, and linearity were verified and met. All variance inflation factors were below 10, indicating the absence of multicollinearity, and the Durbin-Watson value of 2.16 suggested no autocorrelation.
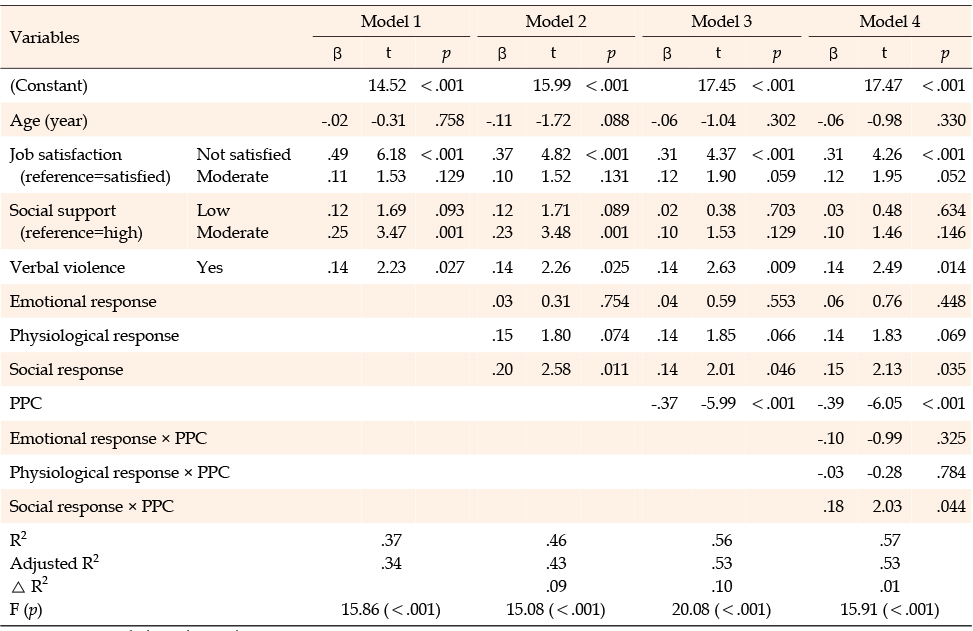
Table 5
Moderating Role of Positive Psychological Capital in the Effect of Violence Response on Burnout (N=172)
Model 1 included control variables-namely, age, job satisfaction, social support, and experiences of verbal violence- and explaining 36.6% of the variance (F=15.86, p<.001). Job dissatisfaction (β=.49, p<.001), moderate social support (β=.25, p=.001), and the presence of experiences of verbal violence (β=.14, p=.027) were significant predictors of burnout. Model 2 added the primary independent variables (emotional violence responses, physical violence responses, and social violence responses), explaining an additional 9.0% of the variance for a total of 45.6% (F=15.08, p<.001). Job dissatisfaction (β=.37, p<.001), moderate social support (β=.23, p=.001), the presence of experiences of verbal violence (β=.14, p=.025), and social violence responses (β=.20, p=.011) were significant predictors of burnout. Model 3 added positive psychological capital and explained an additional 9.9% of the variance, for a total of 55.5% (F=20.08, p<.001). Job dissatisfaction (β=.31, p<.001), the presence of experiences of verbal violence (β=.14, p=.009), social violence responses (β=.14, p=.046), and positive psychological capital (β=-.37, p<.001) were significant predictors of burnout. Model 4, which included the interaction term of emotional, physical, and social violence responses with positive psychological capital, showed a 1.2% increase in explanatory power compared to Model 3, accounting for a total of 56.7% of the variance (F=15.91, p<.001). Job dissatisfaction (β=.31, p<.001), the presence of experiences of verbal violence (β=.14, p=.014), social violence response (β=.15, p=.035), positive psychological capital (β=-.39, p<.001), and the interaction term between social violence response and positive psychological capital (β=.18, p=.044) significantly influenced burnout. This analysis indicates that positive psychological capital played a moderating role in the effect of social violence responses on burnout.
This study investigated the responses of clinical nurses to emotional, physical, and social violence. It also aimed to assess their levels of positive psychological capital and burnout. Furthermore, the study aimed to comprehend the moderating effects of positive psychological capital on the relationship between each type of violence response and burnout.
In this study, clinical nurses reported the highest scores for emotional violence responses (3.34 points), followed by physical violence responses (2.64 points) and social violence responses (1.97 points). These findings align with previous studies that used the same measurement tool with emergency room nurses [23, 24]. Those studies reported scores for emotional violence responses between 3.19 and 3.57 points, physical violence responses between 2.39 and 2.75 points, and social violence responses between 1.72 and 2.28 points. However, our results differ from those of Hwang and Han's study [14] with emergency room nurses, where the highest scores were reported for social violence responses. This discrepancy suggests that violence responses among nurses may vary based on factors such as the healthcare institution's characteristics, the department of work, and individual factors. This underscores the need for ongoing studies on nurses' violence responses. While most previous research on nurses' violence responses has focused on emergency room nurses due to their increased risk of exposure to violence, our study found no significant differences in violence responses between clinical nurses and emergency room nurses. Therefore, it is important to consider and manage violence responses among nurses across various departments.
The mean burnout level among clinical nurses in this study was 3.07 points. This aligns closely with the findings of Ju et al. [24], which utilized the same measurement tool and focused on emergency room nurses, yielding a score of 2.99 points. However, our results were higher than those reported by Kim [13], which centered on psychiatric ward nurses and reported a score of 2.75 points. Despite these differences, our study found no significant variation in burnout levels based on the nurses' department of work. This suggests that predicting nurse burnout levels based solely on their department may not be feasible due to the influence of various complex factors. According to the criteria established by Stamm [21], the nurses in our study, as well as those in the studies by Kim [13] and Ju et al. [24], experienced moderate levels of burnout. Consequently, it is crucial to devise strategies to prevent and mitigate burnout among nurses.
The relationships between responses to violence, burnout, and positive psychological capital were examined. It was found that emotional, physical, and social responses to violence were positively correlated with burnout. Conversely, positive psychological capital was negatively correlated with burnout. These findings are consistent with previous research, such as the studies conducted by Hwang and Han [14] and Ju et al. [24], which identified a positive correlation between responses to violence and burnout among emergency room nurses. Similarly, research by Kim [13], focusing on psychiatric ward nurses, and Cho [25], focusing on nurses in small-sized hospitals, both reported a negative correlation between positive psychological capital and burnout. These findings suggest a significant interrelationship between burnout, responses to violence, and positive psychological capital in the nursing profession. It can be inferred that nurses with high responses to violence and low positive psychological capital are at an increased risk of experiencing burnout.
Job satisfaction and experiences of verbal violence were identified general characteristics and factors related to experiences of violence in hospitals that contribute to burnout among clinical nurses. This aligns with the findings of Lim and Shin's study [26], which focused on operating room nurses and identified job satisfaction and verbal violence as significant contributors to burnout. In our study, we found that lower job satisfaction correlated with higher levels of burnout. This underscores the importance of identifying and enhancing various factors that can improve nurses' job satisfaction in order to mitigate burnout. Furthermore, we found that experiences of verbal violence were associated with increased burnout. Nurses reported that they most frequently experienced verbal violence from patients, family members, and various medical staff. This is consistent with previous studies conducted on clinical nurses in South Korea [5, 6]. Given that verbal violence often occurs without the perpetrator recognizing it as such [6], healthcare organizations should implement institutional measures to address this issue. Such measures could include fostering a culture of mutual respect and empathy among healthcare professionals, and providing training on effective communication and violence prevention.
This study's analysis of the relationship between violence responses and burnout showed that social violence responses significantly contributed to burnout. This aligns with the results of a study on emergency room nurses, which also identified violence responses as key factors in burnout [14]. Interestingly, while emotional violence responses scored highest among the sub-factors of violence responses, it was social violence responses that had the greatest effect on burnout. This means that while nurses perceived the intensity of emotional violence responses, which reflect their feelings and emotional reactions postviolence, as the most severe, it was social violence responses (i.e., changes in their behavior and relationships post-violence) that were perceived as less severe but had the most significant impact on burnout. In light of previous research suggesting that increased social support leads to better violence coping mechanisms and lower burnout levels [27, 28], reducing social violence responses could be a crucial strategy in mitigating burnout among nurses. Furthermore, an organizational culture that views violence as an inevitable consequence of nurses' inadequate performance and the high-pressure nature of patient care, rather than addressing the emotional difficulties stemming from violence, may result in unresolved negative emotions post-violence. This could ultimately lead to changes in social responses, impacting relationships with colleagues, family, and friends, and thereby influencing burnout [18]. Indeed, a study by Kang and Park [6] found that nurses who experienced violence most often adopted a passive coping strategy, reacting as if nothing had happened when violence occurred. Therefore, it is vital to accurately identify the sources of violence, develop proactive coping strategies, and cultivate an organizational culture that encourages immediate emotional support and empathy from colleagues and superiors. Proactive management and intervention at the hospital level are necessary to decrease violence responses among clinical nurses.
The moderating role of positive psychological capital in the effect of violence responses on burnout was examined. It was determined that positive psychological capital does indeed moderate the relationship between social violence responses and burnout. Positive psychological capital is a positive internal resource of an individual, comprising four elements: self-efficacy, hope, resilience, and optimism. These elements work together synergistically, creating a more significant combined effect [9, 10]. Individuals with high levels of positive psychological capital tend to view situations optimistically, have confidence in their ability to overcome obstacles, and actively problem-solve to achieve their objectives [22]. Moreover, positive psychological capital is seen as a crucial factor in mitigating burnout [12] and can be improved through training and development [9]. As such, nursing organizations should strive to implement interventions and efforts to boost the positive psychological capital of clinical nurses, thereby maintaining a high-quality nursing staff.
Cho's study [25] the importance of an organizational culture that promotes active interaction, trust, and creativity among its members. Such a culture can bolster positive psychological capital, thereby motivating individuals to problem-solve and boosting their self-esteem. Furthermore, positive psychological capital can be enhanced through high social support from various sources [29], the provision of educational programs designed to improve individual capabilities [30], and the regular offering of mentoring programs where experienced employees share their knowledge and experience [31]. In this study, an analysis of the differences in positive psychological capital based on general characteristics revealed that individuals who were older, more satisfied with their job, had higher social support, were married, or had a master's degree or higher education level, exhibited higher positive psychological capital. This aligns with the findings of previous research [13, 29, 32]. Kim's study [13] and Kang and Kwon's study [32] discovered that as career experience and job positions increased, so did positive psychological capital. When considering both age and job satisfaction, it was found that nurses with more clinical experience and higher job positions tend to possess increased competence and problem-solving abilities in clinical practice. This results in higher self-confidence, increased job satisfaction, and ultimately, higher positive psychological capital. Moreover, being married may contribute to higher positive psychological capital due to the emotional support received from a supportive spouse. Therefore, nursing organizations should implement strategies at the organizational level to assess the level of positive psychological capital among nurses. For those nurses with low positive psychological capital, interventions should be aimed at enhancing individual positivity and fostering a supportive social environment to reduce social violence responses.
In conclusion, this study found a positive correlation between burnout in clinical nurses and their responses to emotional, physical, and social violence. Conversely, a negative correlation was observed with positive psychological capital. Notably, among the various dimensions of violence responses, social violence responses significantly influenced burnout. Positive psychological capital was found to moderate the relationship between social violence responses and burnout. This implies that positive psychological capital can lessen the detrimental effects of social violence responses, making it a key factor to consider when developing programs to support nurses in effectively managing violent situations and preventing future burnout. Consequently, organizations should offer violence prevention education, accurately identify violence causes, and promptly address them when they occur. They should also establish institutional mechanisms to minimize negative violence responses. Moreover, efforts should be made to identify accessible support methods for nurses who have experienced violence. To boost positive psychological capital and empower individuals to positively tackle challenges when problems or difficulties arise, nursing managers should cultivate a work environment and atmosphere that promotes individual positivity based on trust among organizational members. They should also foster and support innovative ideas and regularly offer various programs to enhance individual capabilities.
The significance of this study lies in its provision of foundational data for the creation of intervention programs aimed at reducing nurse burnout, based on its findings regarding the moderating role of positive psychological capital in the relationship between responses to violence and burnout. However, it is important to acknowledge that the instrument used in this study to gauge responses to violence was somewhat limited. It consisted of only three items pertaining to social violence responses and restricted the assessment of these responses by confining the item format based on the presence or absence of changes in social relationships. Consequently, there is a need for further research to develop a more comprehensive tool that can accurately measure nurses' responses to social violence. This improved tool should then be utilized in future studies.
This study's findings indicate that responses to social violence significantly influence burnout, and that positive psychological capital can moderate the relationship between these responses and burnout. Therefore, to prevent and mitigate burnout among nurses, it is vital to strategically promote the reduction of responses to social violence and the enhancement of positive psychological capital. This can be achieved by establishing a support system that fosters a culture within organizations that acknowledges and addresses negative social responses following violent experiences. Furthermore, burnout prevention programs for nurses should incorporate strategies that minimize threats to positive psychological capital and maximize factors that bolster it, thereby fostering individual positivity at an organizational level.
Building upon the results of this study, the following recommendations are made. First, a tool should be developed that can classify and measure social violence responses in a more detailed and specific manner. Subsequent research should then utilize this tool for more comprehensive investigations. Second, it would be advisable to develop programs aimed at enhancing nurses' positive psychological capital and conduct research to validate their effectiveness.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - CH and SS.
Data collection - CH, KSJ and KSR.
Analysis and interpretation of the data - CH, SS and KSJ.
Drafting and critical revision of the manuscript - CH, SS and KSR.
 E-SUBMISSION
E-SUBMISSION