
Purpose
To explore the nature of psychological resistance to the initiation of antihypertensive medication.
Methods
Participants were 13 adults with hypertension who were refusing or had refused to take antihypertensive drugs from July 2016 to October 2016. The data were collected through face-to-face in-depth interviews, and analyzed according to Braun and Clarke’s 6 steps of thematic analysis.
Results
Analysis of the psychological resistance experience to drug therapy in hypertensive patients resulted in 5 themes and 10 sub-themes from a total of 42 free codes. Participants were “holding out as much as possible without medication” without taking antihypertensive drugs due to “psychological opposition to starting treatment” and “situational barriers related to medication”. However, they were “coming to grips with reality” that they were not taking medication but would take it someday, and they gained “momentum for change” to start taking it.
Conclusion
The 5 themes derived from the data analysis of the experiences of 13 participants are interrelated and suggest the direction of intervention to lower psychological resistance. In particular, we propose the development of an intervention to assist patients in self-decision regarding taking antihypertensive medication. Additional research into the role of medical staff in lowering the psychological resistance of young hypertensive patients is needed.
To explore the nature of psychological resistance to the initiation of antihypertensive medication.
Participants were 13 adults with hypertension who were refusing or had refused to take antihypertensive drugs from July 2016 to October 2016. The data were collected through face-to-face in-depth interviews, and analyzed according to Braun and Clarke's 6 steps of thematic analysis.
Analysis of the psychological resistance experience to drug therapy in hypertensive patients resulted in 5 themes and 10 sub-themes from a total of 42 free codes. Participants were “holding out as much as possible without medication” without taking antihypertensive drugs due to “psychological opposition to starting treatment” and “situational barriers related to medication”. However, they were “coming to grips with reality” that they were not taking medication but would take it someday, and they gained “momentum for change” to start taking it.
The 5 themes derived from the data analysis of the experiences of 13 participants are interrelated and suggest the direction of intervention to lower psychological resistance. In particular, we propose the development of an intervention to assist patients in self-decision regarding taking antihypertensive medication. Additional research into the role of medical staff in lowering the psychological resistance of young hypertensive patients is needed.
Hypertension is a major risk factor for cardiovascular and cerebrovascular diseases, which are the leading causes of death in adults [1]. According to a Korean National Health and Nutrition Examination Survey in 2015, 29.6% of adults aged 30 years or older had hypertension, and 40.3% of hypertensive patients were not treated for hypertension [2]. The risk of cardiovascular disease in patients with uncontrolled hypertension is greater, which can lead to an economic burden on the entire society [3].
To prevent complications of hypertension, lifestyle changes, such as limitation of sodium intake, proper exercise, and stress control, should be attempted. However, the use of antihypertensive agents is recommended for patients with blood pressure of 140/90 mmHg or more [4]. It has been reported that antihypertensive medication is effective in lowering the incidence of cardiovascular disease and the mortality of the hypertensive adults [5]. In addition, the timing of initiation of hypertension medication is important. Xu et al. [6] reported an increase in the incidence of cardiovascular disease and mortality in patients who started taking medication at a systolic blood pressure greater than 150 mmHg.
The World Health Organization (WHO) defines medication adherence as the continuous use of medication in accordance with a physician's recommendations [7]. Personal experience, beliefs, autonomy, social support, and socioeconomic factors can influence medication adherence [8, 9, 10]. A variety of educational and behavioral interventions, such as a team approach, motivational interviews, direct observation, and self-monitoring, have been introduced to improve medication adherence [11, 12, 13, 14]. The result of a meta-analysis of medication adherence [15] suggested that it was important to consider various characteristics of the participants rather than to provide fixed interventions to improve compliance in patients with hypertension. The majority of these studies focused on patients who had initiated medication but not sustained it for some reason.
Meanwhile, some hypertensive patients refuse the initiation of antihypertensive agents and seek traditional remedies even though they were recommended for drug therapy [10]. Hypertensive patients are reluctant to take medication because they are skeptical about lowering blood pressure, have concerns about side effects and dependencies, and have a reaction to the patient identity [16, 17]. In a similar vein, Jang et al. [18] have defined the concept of psychological resistance to antihypertensive drugs as “a phenomenon of denial of being diagnosed with hypertension, avoiding the need to take the drug itself, expressing the reluctance, opposing the use of the drug according to the physician's decision, and seeking alternative measures to control blood pressure”. This is not only a simple rejection of the drug but also a complex phenomenon that includes various psychological and social factors of the individual involved in the drug therapy.
As seen above, effective hypertension management requires the development of appropriate strategies for those who are refusing medication despite the knowledge of their own hypertension. To do so, a thorough understanding of psychological resistance to hypertensive medication should be prioritized. We intended to understand the substantial nature of psychological resistance, and provide basic data necessary for resolving psychological resistance using a qualitative thematic analysis method. The purpose of this study was to conduct an in depth investigation of the nature of psychological resistance to the initiation of drug treatment in hypertensive patients, and the key question was, “What is the psychological resistance experience to starting medication in hypertensive patients?”
This was a qualitative study exploring the psychological resistance experience to drug treatment in hypertensive patients using in-depth interviews and thematic analysis. We have adhered to the consolidated criteria for reporting qualitative research (COREQ) [19].
In this study, the participants were 13 patients who were diagnosed with hypertension but refused to take hypertensive drugs. To recruit participants, recruitment notices were posted on the outpatient waiting room board at D University hospital. Interviews were conducted with participants who expressed their intention to participate in the study. The mean age of the participants was 52.4 years, and they consisted of 6 men and 7 women. Of the total participants, 5 had experienced refusing medication but were currently taking hypertensive medication, and the remaining 8 were not taking medication at the time of the interview. All the participants had no other disease when they were diagnosed with hypertension (Table 1).
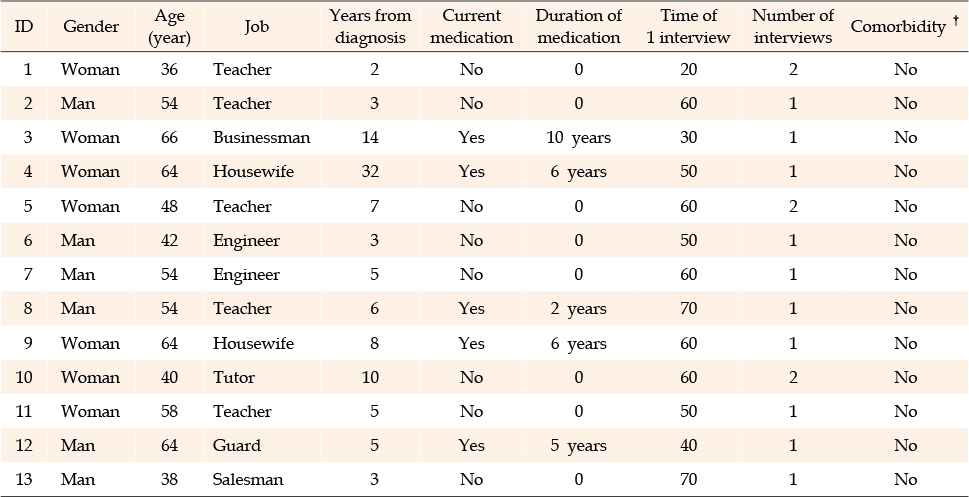
Table 1
Participants Characteristics (N=13)
Data were collected from July 2016 to October 2016 using face-to-face in-depth interviews. If further interviews were required, a telephone interview was conducted. Each participant was interviewed 1~2 times (20~70 minutes per interview). Suitable places for interviewing were selected while considering the accessibility to the participants. All interviews were conducted by one of the authors (JYJ), who is experienced in conducting interviews for qualitative study and in nursing patients with hypertension.
The interviews were conducted through semi-structured questions. The interviewer began the interviews with general questions, such as, “When did you know that you were hypertensive?” and “Tell me how you felt when you first got diagnosed”. Once a familiar atmosphere was created, the interviewer proceeded to the main question, “Tell me about your experience of refusing medication”. Finally, the interviewer summarized the contents of the interview and requested the confirmation of the participant.
All interviews were recorded using 2 audio recorders with the consent of the participants. The interviewer wrote the field and debriefing notes for each interview. The participants were interviewed until there was saturation of data. The authors found that the content of the interviews was repeated after the twelfth interview. Thus, we completed the data collection after confirming the repetition at the thirteenth interview.
The protocol of this study was reviewed and approved by the Institutional Review Board of Dong-A University (approval number: 2-104709-AB-N-01-201607-HR-027-02). We recruited participants publicly. Prior to beginning the study, we explained to the participants the purpose of the study, how the data were collected and how the collected data were kept, how to withdraw from the study, and compensation, and received written consent.
The interview and data analysis were carried out simultaneously. After the analysis of each interview, additional telephone or messenger interviews were conducted if necessary.
In the current study, we attempted to understand the phenomenon by analyzing the data using thematic analysis. We followed the 6 steps that Braun and Clarke [20] suggested for thematic analysis: (1) becoming familiar with the data, (2) generating codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) writing the report. First, both authors repeatedly read the transcribed contents of the interviews, field notes, and debriefing notes. Subsequently, we derived codes through words, phrases, and sentences that reflected the participants' perceptions, feelings, or experiences related to psychological resistance to antihypertensive medication. The codes were chosen as those that appeared repeatedly in the interviews, described psychological resistance well, or were related to other codes. The derived codes were compared with each other and generated into sub-themes and themes. The themes were classified according to the frequency and patterns that appeared throughout the interview data, and were named so as to give meaning to the data. This analysis started shortly after the first participant's interview, and we continued to add or revise themes from the additional interview data. When no new theme was identified, the data collection was discontinued, and the themes drawn up to that point were refined to shape the theme diagram (Figure 1).
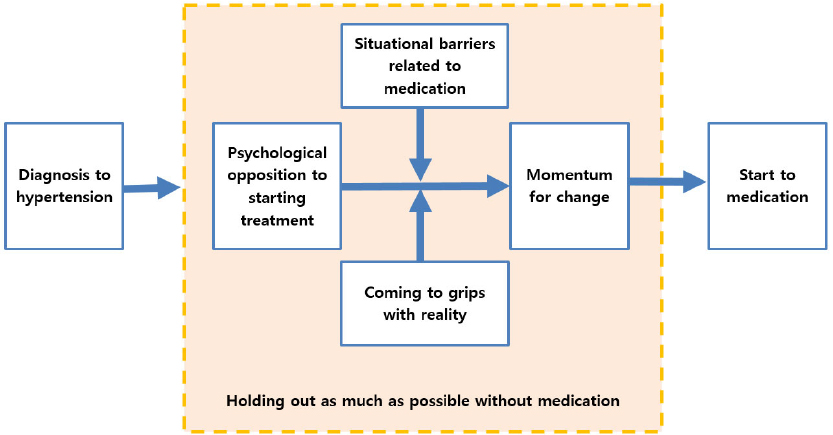
Figure 1
Theme diagram of psychological resistance to antihypertensive medication.
We followed the 4 criteria by Guba and Lincoln [21] to maintain the rigor of the study. First, to keep the true value, the interviewer summarized the contents of the interview and confirmed them with the participant immediately after each interview. In addition, the author who conducted the interviews transcribed the contents of the interviews through repeatedly listening to the recordings, and the other author randomly selected transcripts and verified them with the voice files to ensure accuracy. Second, to increase the applicability, we invited participants who were either currently refusing or had refused the use of medication to collect abundant data on the research topic. Furthermore, the themes that we derived were confirmed by 2 nursing professors who were diagnosed with hypertension but were reluctant to take medication. Third, to maintain consistency, the authors aimed to keep thinking about the main research questions during the whole process while simultaneously ensuring that the data collection and analysis proceeded cyclically. Through a series of consultation meetings with a number of graduate students and nursing professors who were familiar with qualitative analysis, we exchanged opinions about the research topic, analysis process, data saturation, and the themes that were derived. Finally, to ensure neutrality, we tried to exclude our prejudices related to the topic by describing our understanding, assumptions, and prejudices in a journal.
In the current study, psychological resistance to drug therapy in hypertensive patients was qualitatively analyzed, and as a result, 5 themes and 10 sub-themes were derived from 42 codes (Table 2). The 5 themes included “psychological opposition to starting treatment”, “situational barriers related to medication”, “holding out as much as possible without medication”, “coming to grips with reality”, and “momentum for change”. Resistance to antihypertensive medication can be described as follows.
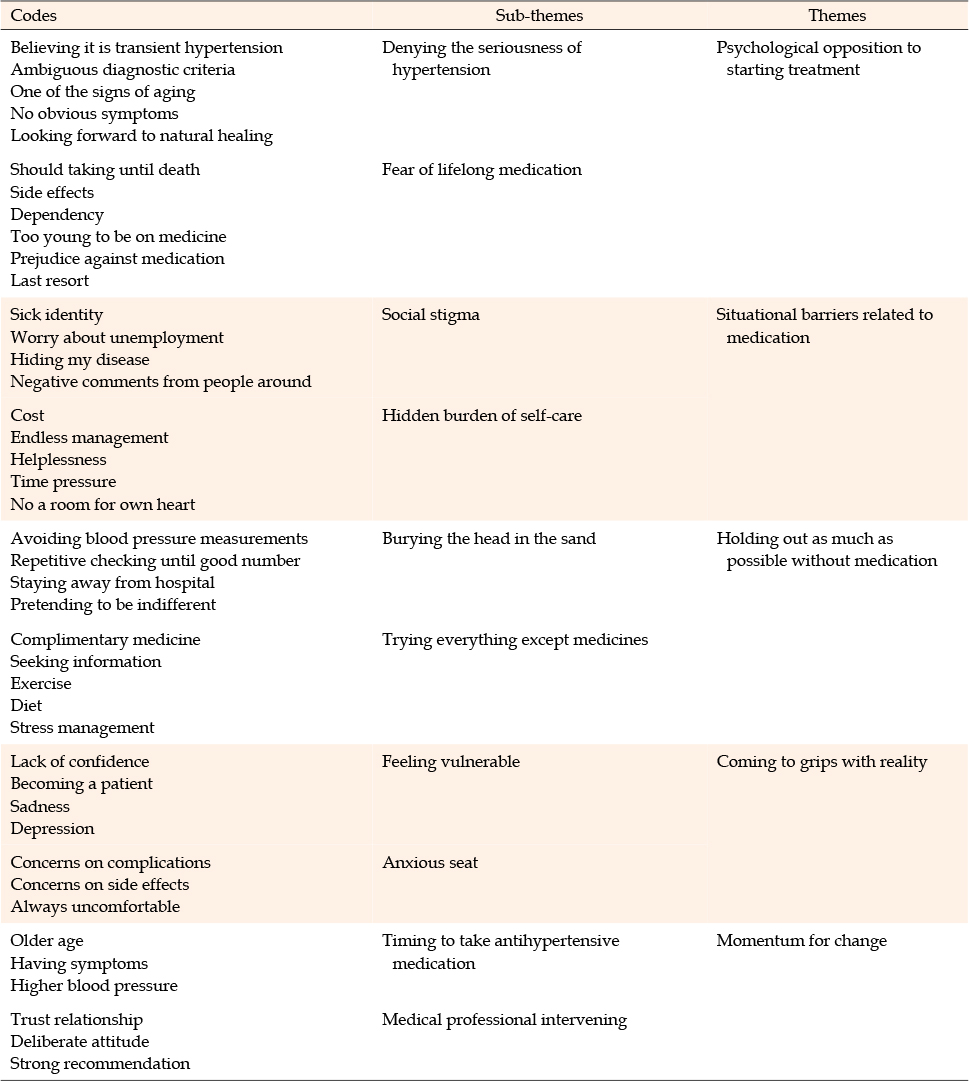
Table 2
Themes for Psychological Resistance to Antihypertensive Medication
Although the participants were aware that they had hypertension, they did not acknowledge the seriousness of the disease and refrained from taking medication due to their opposition to it. This phenomenon was related to the negative perception toward hypertension from the people around them, and the situational constraint of the burden of lifelong management. The participants were holding out for as long as possible without hypertensive medication; instead, they were ignoring the fact that they were diagnosed with hypertension or actively searching for alternative measures. In this situation, the participants were coming to grips with the reality of feeling vulnerable to the fact of becoming patients, and were worried about the possible complications of the drug, or the side effects if they took medications. They knew that they would eventually have to take antihypertensive medication if they reached a certain point such as having blood pressure that was too high, or getting old enough to be taking antihypertensive drugs. They were also willing to start if the healthcare experts strongly and deliberately recommended the taking of medication. The specific contents of each theme are as follows.
The participants were unaware of the severity of their disease and, concurrently, had a strong sense of repulsion to taking medication for the rest of their lives. As a result, they were psychologically resistant to starting medication even after being diagnosed with hypertension.
The participants did not know exactly what the diagnostic criteria for hypertension were, and some believed that their hypertension could be a temporary phenomenon or could be lowered through self-management. In addition, some believed that hypertension was not a disease but that it was a kind of aging, and because it had no symptoms, medication would not be needed, and it might improve naturally.
My blood pressure is 150 or a little higher… but I do not feel sick anywhere… I do not have any symptoms at all. I do not think I need to take medicine yet with this level of blood pressure (Participant 2).
Yes, it was high because I was not in good shape on that day(hahaha)… wasn't I tired? Didn't I sleep late, last night? Right, it might be high because I drank yesterday… (Participant 13).
The participants felt that dependency and side effects would be severe as antihypertensive agents should be taken for a lifetime once begun. Some participants did not want to take antihypertensive medication because they were too young to be taking medication, and some expressed a vague repulsion and distrust of the medication itself. Participants would choose to be taking medication as a last resort when they could no longer avoid it.
I am still young, so I think my blood pressure would be all right if I changed my lifestyle, such as diet or exercise (hahaha)… because of the burden of lifelong medication… I am concerned about the side effects from long-term use. I am young, I am not going to take medicine until I am 40 years old. I totally wish to hold off the medication as much as possible (Participant 1).
The participants did not want to expose their hypertension to others because of the social stigma of the disease. In addition, time and economic efforts for blood pressure management are burdensome, and these situational constraints are factors that hinder the use of hypertension drugs.
The participants were reluctant to be recognized as hypertensive patients. They presumed that when taking antihypertensives, they would be known as people with high blood pressure and people would treat them with prejudice. Contract workers, in particular, refused to take drugs because they predicted that high blood pressure would have a negative impact on employment.
I'm a little embarrassed (that I'm a hypertensive patient) because I'm still young… Especially, I am a contract teacher. How do I renew my contract with a disease like hypertension?… if I had taken medication, they would notice that I was a patient. It sure will affect my negotiation for contract renewal… I hate it because it proves that I am a hypertensive patient when I take blood pressure medicine (Participant 5).
Some participants were worried about the cost of medication, the time that it would consume, and the need to manage the situation over their lifetime. In particular, one of the female participants expressed that she could not afford to take care of herself.
I happened to know that I was hypertensive. But I did not take medicine because I was busy living. I knew I had to go on once I started going to the hospital to be medicated… (Participant 10).
Instead of taking antihypertensive drugs, some participants tended to avoid the fact that they were hypertensive patients. On the other hand, some participants actively attempted various alternatives to lower their blood pressure. Both can be observed as efforts to endure for as long as possible without taking the medication.
The participants were aware that they had hypertension but were not intentionally measuring their blood pressure, or avoided visiting the hospital. On the other hand, there were participants who repeatedly measured their blood pressure until the desired lower number was reached. Some also consciously attempted to be indifferent to the fact that they were hypertensive.
I have always had a headache (touching the back of his head)… whenever I experience stiffening in my head and neck muscles, my blood pressure would go up too… but I will not go to the hospital. I'm really scared that a doctor would say my blood pressure is too high (Participant 11).
I often measure my blood pressure. When my blood pressure is higher than I expect, I keep checking again until I get the number I want. In the meantime, I take a deep breath, take a little break, and re-check the blood pressure… until a lower number comes out (Participant 12).
Contrary to those who neglected and avoided hypertension, some participants actively tried complementary therapies such as dietary supplements, folk remedies, and oriental medicine therapies. They also worked on self-care such as diet, exercise, and stress management, and they sought and studied information related to hypertension.
I just love fried chicken rather than roast chicken … (hahaha). But I have tried so hard not to eat fried chicken, sweets, white bread, or any junk food. Since I did not want to take medicines, I walk around the playground a few times at lunchtime… in the sun. I have to walk around. I have to walk for at least 30 minutes (Participant 5).
The participants were consistently opposed to taking medication; on the other hand, they were sad and depressed about the fact that they were hypertensive patients, and were always worried about complications of the disease. In other words, they did not want to take medications; however, they were nervous about the possibility of complications.
The participants who had been diagnosed with hypertension and who were recommended to take medication felt that they were getting older and expressed sadness about the negative signals in their body. They were not confident, and were depressed because they felt like they were becoming patients.
I feel like I'm a walking hospital (hahaha). This fact alone is enough to make me sad… I could not bear it if I had to take medicine… I would become useless (Participant 12).
The participants were afraid that hypertensive complications would occur since they were not taking the medication. If they took the medication, they might suffer from its side effects, and this situation always made them uncomfortable. They also presumed that they might be misdiagnosed, or the medical staff might not manage their medication properly.
As for hypertension… since my mother passed away of a stroke, I have always thought it might happen to me… as my blood pressure got higher, my fears grew bigger… fear that I should take blood pressure medicine someday. However, even if I took medicine, it could not bring peace of mind. I would think I became a hypertensive patient finally… even if I take the medicine, I will take it with fear of the side effects (Participant 7).
Although the participants were refusing to take medication, they knew they would be taking medication someday. In particular, they were expecting the medical experts to be more cautious and actively involved in the initiation of their medication.
The participants stated that they would be taking medication when they got older or if their hypertension worsened.
I would take the medicine if I had noticed an abnormality in my body… not right now… I have no symptoms… it is annoying… if symptoms such as a continuous headache, an abnormal sensation in my arms and legs, or any other symptoms in my body appear, I will eventually take the medicine (hahaha), but I do not want to take the pills beforehand (Participant 6).
The participants pointed out that the medical staff only diagnosed hypertension; however, they did not provide appropriate information about medication and other treatment options. In addition, if someone actively recommended treatment with caution, they were willing to start treatment.
I was prescribed an antihypertensive drug when I went to a public health center for an annual checkup. The doctor just told me the numbers (of blood pressure) and prescribed medicine. That was not so good… well, if he had been good at explaining about my hypertension and treatment at the health center, I would have been taking medicine now… (Participant 2).
I did not take medicine and thought it would get better. But my blood pressure remained at 140, 150. So, my doctor advised me, “Anti-hypertensive drugs are not bad drugs. Let's start medication”. So, I started taking medicine. I have been taking medicine for 10 years (Participant 3).
The current study explored the nature of the psychological resistance to antihypertensive medication through a thematic analysis of interviews with hypertensive patients who refuse or have refused medication. As a result, we were able to derive 10 sub-themes and 5 themes that explained the psychological resistance to antihypertensive drugs. Of the 5 themes derived, “psychological opposition to starting treatment” and “holding out as much as possible without medication” are similar to “rejection, rejection and alternative finding”, which are attributes in the study by Jang et al. [18]. The second theme, “situational barriers relating to medication” can be said to be a leading factor as proposed by Jang et al. [18]. However, “coming to grips with reality” and “momentum for change” are new topics that have not been identified in the review of existing literature, and can be used to express the psychological state of participants as well as provide direction for intervention.
The first theme, “psychological opposition to starting treatment”, consists of “denying the seriousness of hypertension” and “fear of lifelong medication”. Inaccurate beliefs about illness and medication are some of the major factors in the WHO's non-compliance for long-term treatment regimen [7]. According to a systematic review of the barriers to compliance with antihypertensive drug medication [22], the most frequently studied factor was the patient's belief in hypertension or antihypertension medication. Factors affecting decisions to take hypertensive drugs include beliefs about how individuals perceive the necessity of the drugs, their effects, and the side effects [23]. Of these, “necessity” is associated with “denying the seriousness of hypertension”, which is a sub-theme of this study. It is important for patients with hypertension to recognize that hypertension is a serious disease that can lead to various life-threatening complications; therefore, education or cognitive intervention is needed for patients to clearly recognize the severity of hypertension.
The biggest obstacle to discovering and diagnosing adolescent hypertension may be their identity of being “sick”. Taking an antihypertensive drug modifies young people's “young” identity and makes them feel older than their peers [24, 25]. This is associated with the second theme of this study, which is “situational barriers related to medication”. The participants in the current study were reluctant to let people know that they were hypertensive, and they presumed that the sign of being a patient would have a number of negative effects on them. These situational constraints can be considered as socioeconomic factors among WHO's barriers to long-term treatment compliance. Socioeconomic factors include social norms and customs, cultural characteristics, and the health literacy of members [7]. Khatib et al. [26] refer to these disorders as social influences, which can affect not only patients but also the general public, negatively affecting the proper management of hypertension. Therefore, there is a need for improved social awareness of the use of hypertension drugs.
The third theme of this study was “holding out as much as possible without medication”. Instead of taking drugs, the participants were tempted to actively seek alternative measures or avoid their hypertension. This theme can be said to be psychological resistance expressed in behavior. Benson and Britten [16] interviewed 38 hypertensive patients and reported avoidance of medication, suggesting that many patients are seeking alternatives to antihypertensive drugs, which is similar to our theme. Saleem et al. [10] also reported that hypertensive patients strongly supported the use of complementary and alternative medicines.
The fourth theme derived from the current study, “coming to grips with reality” and the fifth theme, “momentum for change” can provide direction when planning interventions for hypertensive patients with psychological resistance to medication. This is consistent with the study by Marshall and colleagues [27] that reported that most hypertensive patients are anxious and afraid of hypertension while, concurrently, reluctant to take medication due to its side effects and concerns of dependency. In the current study, the participants also expressed their expectations for intervention by the medical staff, which was similar to the results of a previous study [8] in which the communication pattern with the medical staff was an important factor in determining drug therapy. According to previous studies [9, 16, 17], confidence in the healthcare system and the healthcare staff plays a key role in the process of compliance to drug therapy by hypertensive patients.
The interventions for improving medication compliance that have been attempted so far have mainly focused on the habituation of drug use, feedback on compliance, self-monitoring of blood pressure, or dispensing drugs with different packaging [28]; it has been difficult to find an attempt that can lower psychological resistance to medication. According to the medication adherence model [23], the first step of compliance is purposeful behavior, and deliberate decision-making is required for purposeful behavior. A team approach that was attempted in a recent study [13] included several motivational interviews. Through these interviews, the patient could fully discuss with the medical staff the necessity for medication, the importance of compliance, side effects, and his/her concerns, and make his/her own decisions. As one of the bases of psychological resistance is the suppression of individual autonomy [18], providing a condition for self-decisionmaking regarding the medication could lower the psychological resistance. Kravetz and Walsh [13] reported the effect of this intervention of self-decision-making only on blood pressure control; thus, it is necessary to study the effect of this intervention on psychological resistance in the future. When considering new interventions to promote compliance, one should take into account the different causes of the patients' psychological resistance. For example, younger patients with hypertension may be reluctant to be involved in a self-management program using social media or a text message service because they are afraid of losing their identity as young people, and do not want to be exposed to the fact that they are patients [25]. Therefore, they need to be provided with interventions that can reduce the “patient identity”, which is the biggest cause of psychological resistance, and maintain their “young identity”.
Most studies of psychological resistance in patients with chronic disease have focused on improving drug compliance since the beginning of drug therapy [29]. The significance of this study was to explore psychological resistance and to start drug therapy, and to present a new direction to reduce psychological resistance at the start of treatment so that drug therapy could begin at the appropriate time. However, this study also has limitations. We did not reflect the experiences of participants with other diseases, along with hypertension. Problems need to be explored from the perspective of participants with diverse disease backgrounds.
In the current study, we explored the psychological resistance experience of 13 hypertensive patients who have current or past experiences of medication refusal. The results of the thematic analysis indicate that the participants were “holding out as much as possible without medication” because of “psychological opposition to starting treatment” and “situational barriers related to medication”. However, they were “coming to grips with reality” that they were not taking medication, and they knew they would start drug therapy someday. The participants experienced “momentum for change” to start taking medication. These results are expected to be useful for the development of interventions that are different from the previous medication compliance strategies. In particular, we propose that future research should develop a measure to promote patients' self-decision regarding the use of hypertensive drugs, and that it should search for a desirable role of medical staff that could assist in lowering the psychological resistance of younger patients with hypertension.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - KJ and JYJ.
Data collection - JYJ.
Analysis and interpretation of the data - KJ and JYJ.
Drafting and critical revision of the manuscript - KJ and JYJ.
This study was supported by the research fund from Dong-A University.
 E-SUBMISSION
E-SUBMISSION