
Purpose
This study was conducted to identify factors affecting person-centered care among tertiary hospital nurses caring for patients with COVID-19.
Methods
Study participants comprised 152 tertiary hospital nurses with experience caring for patients with COVID-19. Data were collected from September 1 to October 5, 2022 and analyzed using independent t-test, correlation coefficient, and hierarchical multiple regression with SPSS/WIN 26.0.
Results
Person-centered care showed a statistically significant positive correlation with the nursing work environment (r=.46, p<.001) and teamwork (r=.49, p<.001). Hierarchical multiple regression analysis revealed that the variables of position (β=.20 p=.014) in model 1 (F=6.20, p=.014), teamwork (β=.47 p<.001) in model 2 (F=24.94, p<.001), and teamwork (β=.33 p=.002) in the final model influenced person-centered nursing (F=18.19, p<.001), and the explanatory power was 25.5%.
Conclusion
The significance of nurses' teamwork has been emphasized because of the COVID-19 pandemic. Teamwork can be promoted by reviewing protocols for responding to severely ill patients with infectious diseases, which were revised during the COVID-19 period, and establishing appropriate systems to follow.
This study was conducted to identify factors affecting person-centered care among tertiary hospital nurses caring for patients with COVID-19.
Study participants comprised 152 tertiary hospital nurses with experience caring for patients with COVID-19. Data were collected from September 1 to October 5, 2022 and analyzed using independent t-α, correlation coefficient, and hierarchical multiple regression with SPSS/WIN 26.0.
Person-centered care showed a statistically significant positive correlation with the nursing work environment (r=.46, p<.001) and teamwork (r=.49, p<.001). Hierarchical multiple regression analysis revealed that the variables of position (β=.20 p=.014) in model 1 (F=6.20, p=.014), teamwork (β=.47 p<.001) in model 2 (F=24.94, p<.001), and teamwork (β=.33 p=.002) in the final model influenced person-centered nursing (F=18.19, p<.001), and the explanatory power was 25.5%.
The significance of nurses' teamwork has been emphasized because of the COVID-19 pandemic. Teamwork can be promoted by reviewing protocols for responding to severely ill patients with infectious diseases, which were revised during the COVID-19 period, and establishing appropriate systems to follow.
Person-centered care means providing individualized care that focuses on the patient's needs, involves them in decision-making, and respects their αs and autonomy [1]. It positively impacts patients by reducing length and frequency of hospital stays and outpatient visits, generating economic benefits through lower healthcare costs [2] and improving quality of care and patient satisfaction [1].
Coronavirus Disease 2019 (COVID-19) has spread rapidly with its high transmission rate, greatly impacting the health and lives of people worldwide and changing the social, economic, and healthcare systems of many countries [3]. As quarantine, control, and prevention measures for COVID-19 were implemented, confirmed patients were transferred to negative pressure wards, and they experienced physical symptoms such as fever, cough, shortness of breath, and side effects of medications due to the disease, as well as psychological distress due to negative attitudes from others and society and loneliness, fear, and anxiety due to isolation [4]. Hospitalized patients did not receive individualized care to meet their needs owing to the focus on diagnosis and treatment; family and visitor access was restricted owing to the use of isolation rooms that were cut off from the outside world; and communication and autonomous decision-making was limited because of the isolated environment and protective gear worn by healthcare workers, making it difficult to provide person-centered care [5]. The rapid spread of COVID-19, inadequate infectious disease training, frequently changing work standards, work division with dispatched healthcare workers who have exacerbated workloads, and a lack of communication with patients has highlighted the need for efficient and accurate communication [6]. With conflicts intensifying because of poor communication and patient care issues emerging, teamwork has become important to enhance team members' abilities and positively contribute to their performance and achievement of goals; teamwork based on trust through effective communication is crucial for successful crisis response, as it ensures effective, quality care and promotes patient safety [7].
Nurses responding to COVID-19 have experienced stress due to increased workload and psychological strain, which can lead to nurse burnout and jeopardize patient safety [8]. Because nurse stress is a barrier to advancing person-centered care [9], it is important to determine the impact of COVID-19 stress on person-centered care.
The pandemic has highlighted the importance of Personal Protective Equipment (PPE) for healthcare workers and led to the use of Powered Air Purifying Respirators (PAPRs) in combination with high-flow oxygen therapy and aerosol-generating treatments [10]. Healthcare workers perform various tasks while wearing PPE, and nurses who wear PPE for long periods experience increased fatigue from it [11]. This nurse overload can hinder execution of person-centered care [5].
The nursing work environment during the COVID-19 pandemic has worsened owing to increased workloads for environmental management and infection prevention [6]. A good nursing work environment is essential for nurses when treating COVID-19 [12]. The more positively nurses perceive their nursing work environment, where person-centered care can be performed, the more likely they will be to provide quality nursing care [13].
During an infectious disease crisis, collaborative and trusting teamwork through effective communication among healthcare providers plays a critical role in successful crisis response by strengthening relationships, maintaining individual health, and ensuring delivery of safe and effective patient care [7]. As positively perceived teamwork promotes and enables person-centered care, it is key to implementing person-centered care [14]. Against this backdrop, it is important to understand the relationship between teamwork and person-centered care among nurses in tertiary care hospitals, who play a central role in the care of COVID-19 patients, to effectively implement person-centered care.
Tertiary hospitals are medical institutions that specialize in providing difficult medical treatment for severe diseases according to the Ordinance of the Ministry of Health and Welfare [15]. Since the first COVID-19 case was confirmed in Daegu on February 18, 2020, beds have been categorized according to severity owing to the increase in the number of confirmed cases, and a system has been established to transfer patients to tertiary hospitals for severe pneumonia symptoms and a temperature of 38 degrees or higher lasting for more than three days [16]. As the number of cases increased nationwide, the Central Disaster and Safety Countermeasure Headquarters issued the first bed reserve order on December 18, 2020, requiring tertiary hospitals to reserve at least 1% of their licensed beds for dedicated treatment of severe cases of COVID-19 [17]. Compared with nurses in nursing hospitals, where mildly ill patients requiring long-term care are usually hospitalized [9], nurses in tertiary hospitals have a high proportion of severely ill patients and simultaneously perform complex tasks, such as communication for work coordination, work improvement, and customer satisfaction [18]. Additionally, during treatment for COVID-19, nurses in tertiary hospitals experience infectious disease stress and emotional fatigue, compounded by the burden of caring for critically ill patients who require complex and challenging treatment and care [19]. In a large-scale disaster such as the COVID-19 pandemic, there is a need for reliable support and efficient management of the nursing workforce, who are the first on the front lines [8], and it is especially important to identify factors related to person-centered care among nurses in tertiary hospitals, who play an important role in halting the spread of COVID-19 and isolating and treating severely infected patients [19], to improve the quality of care for patients with severe infectious diseases in the future.
Studies related to person-centered care in the context of COVID-19 have explored factors related to person-centered care among nursing home nurses in the context of COVID-19 [9] and dedicated COVID-19 hospital nurses [6, 20]. However, there is a paucity of research exploring person-centered care influencers and developing interventions for nurses caring for severely ill COVID-19 patients in tertiary hospitals [15], which provide specialized and challenging care for severely ill patients, unlike nursing hospitals, where long-term care patients are mainly hospitalized [9], and dedicated hospitals, which are public hospitals temporarily designated as dedicated hospitals to care for COVID-19 patients owing to the increase in cases during the pandemic [6, 20].
In this study, we aim to analyze the relationship between COVID-19 stress, infection control fatigue, nursing work environment, and teamwork and its effect on person-centered care among nurses in tertiary hospitals by identifying the structure and hierarchy of the factors through a hierarchical regression model. This study analyzed the abovementioned relationship among tertiary hospital nurses caring for COVID-19 patients and identified factors affecting person-centered care to provide a basis for improving the person-centered care offered by tertiary hospital nurses caring for patients with severe infectious diseases.
This study aims to identify factors influencing person-centered care among tertiary hospital nurses caring for patients with COVID-19.
This is a descriptive study to identify the factors influencing the person-centered care of tertiary hospital nurses caring for COVID-19 patients.
The subjects of this study are tertiary hospital nurses who have been directly involved in the care of COVID-19 patients for at least one month, wearing a LEVEL D or PAPR. They understand the study's purpose and voluntarily consented to participate. The required number of subjects was calculated using the program G*Power 3.1.9.7 to calculate the sample size required for multiple regression analysis. Based on previous research [20], the minimum sample size required was 147, with a significance level of.05, power of .90, effect size of 0.15, and 10 predictor variables (6 general and job-related characteristics: age, total clinical experience, educational attainment, position, total time spent caring for COVID-19 patients, average number of patients per nurse on duty, and 4 independent variables: COVID-19 stress, infection control fatigue, nursing work environment, and teamwork). Considering the high turnover of nurses due to COVID-19, 187 questionnaires were distributed accounting for a possible dropout rate of 20%. After excluding 31 responses from non-tertiary general hospitals, 2 responses from subjects with no experience wearing PPE, and 2 incomplete responses, 152 responses were used for statistical analysis.
This study was conducted following review and approval (IRB No. 2206-004-509) by the Institutional Review Board (IRB) of C University Hospital, where the researcher is affiliated. Participants were allowed to participate in the survey after reading an instruction sheet regarding the purpose, contents, procedures, confidentiality, voluntary participation, and withdrawal of participation and agreeing to participate in the study. Personal information collected for the study will not be used outside of the study, and personally identifiable information will only be used to provide a reward for participation in the study and will be destroyed immediately afterwards. The data will be stored in a secure location for three years after analysis and then disposed of. After data collection was completed, the research participants were provided with a small reward.
COVID-19 stress was measured using an instrument developed by Lee et al. [21] to measure stress among Taiwanese nurses during the Severe Acute Respiratory Syndrome (SARS) pandemic, which was adapted by Heo [22] to fit the Korean COVID-19 context and modified by assessing content validity. The instrument comprises 23 items and is based on a 5-point Likert scale (1: not at all; 5: very much so), with higher scores indicating higher levels of COVID-19 stress. The Cronbach's α score (used to judge instrument reliability) was .86 at the time of development, .90 in a study by Heo [22], and .92 in this study.
For the measurement of infection control fatigue, the tool developed by Gu [23] was used with approval. The tool comprises 39 questions and five domains: Complex procedures and personnel shortage (12 questions), Conflicts from uncertain situations and insufficient support (11 questions), Patients' worsening conditions and insufficient knowledge (7 questions), Difficulties due to a new role and demands (5 questions), and Concern about infection and burdens from excessive attention (4 questions). It uses a 5-point Likert scale (1: not at all ~5: very much so), with higher scores indicating higher infection control fatigue. In the study by Gu [23], the Cronbach's α α was .96, as it was in this study.
Nursing work environment was assessed using the Practice Environment Scale of Nursing Work Index (PES-NWI) developed by Lake [24], which was adapted by Cho et al. [25], and the Korean version of this instrument (K-PES-NWI), which was verified for reliability and validity, was used with permission. The tool comprises 29 questions and five domains: Nurse participation in hospital affairs (9 questions); Nursing foundations for quality of care (9 questions); Nurse manager ability, leadership, and support of nurses (4 questions); Staffing and resource adequacy (4 questions); and Collegial nurse-physician relations (3 questions). It uses a 4-point Likert scale (1: not at all ~4: very much so), with higher scores indicating more positive perceptions of the nursing work environment. The Cronbach's α score was .82 at the time of development,.93 in the study by Cho et al. [25], and .95 in the present study.
We used the TeamSTEPPS Teamwork Perception Questionnaire (TPQ) developed by the Agency for Healthcare Research and Quality (AHRQ) and the Department of Defense in the United States [26], translated into Korean by Hwang and Ahn [27], and validated for application in the Korean environment. It comprises 35 questions, organized into five domains: Team structure, Leadership, Situation monitoring, Mutual support, Communication, each with 7 questions. It is based on a 5-point Likert scale (1: not at all; 5: very much so), with higher scores indicating more positive perceptions of teamwork. The Cronbach'sα α was .91 at the time of development, .96 in the study by Hwang and Ahn [27], and .96 in this study.
Person-centered care was assessed using the Person-centered Critical Care Nursing (PCCN) instrument developed and validated by Kang et al. [28]. The instrument comprises 15 questions and 4 domains: Compassion (4 questions), Individuality (4 questions), Respect (4 questions), and Comfort (3 questions). It uses a 5-point Likert scale (1: not at all ~5: very much so), with higher scores indicating higher levels of person-centered care. The instrument's Cronbach's α score was .84 in the study by Kang et al. [28] and .88 in this study.
The data were collected from September 1 to October 5, 2022. One actively operating online nurse community with more than 100,000 members was selected to post a notice to recruit study participants and conduct an online survey for those who expressed their willingness to participate. Participants agreed to participate in the survey through an online link. The online questionnaire was made available to the participants through a hyperlink at the end of the recruitment notice. The questionnaire was organized sequentially, with an introductory statement on the first page and a sequence of questions following it, so that respondents could complete them in order. The questionnaire responses were organized by specifying mandatory questions that needed to be answered without omissions, and only one response per question was allowed to prevent multiple responses. The questionnaire took an average of 10~15 minutes to complete.
The collected data were analyzed using the SPSS/WIN 26.0 program, and the following methods were used. The general characteristics of the subjects were calculated as frequencies, percentages, means, and standard deviations. COVID-19 stress, infection control fatigue, nursing work environment, teamwork, and person-centered care were calculated as means and standard deviations. Differences in person-centered care according to general characteristics were analyzed by independent t-α. Correlations between COVID-19 stress, infection control fatigue, nursing work environment, teamwork, and person-centered care were analyzed with Pearson's correlation coefficients. Factors affecting person-centered care were analyzed using hierarchical multiple regression.
The general characteristics of the subjects and the differences in person-centered care according to the general characteristics are presented in Table 1. The total number of subjects was 152 (132 women [86.8%] and 20 men [13.2%]. The average age was 30.68 years, with 80 (52.6%) in their 20s and 60 (39.5%) in their 30s, and 120 respondents (78.9%) were unmarried. The total clinical experience was 5 years less for 75 respondents (49.3%) and 5 years or more for 77 (50.7%), with average clinical experience being 6.79 years. Regarding education level, 115 (75.7%) were 4-year college graduates. Regarding position, 136 (89.5%) were staff nurses and 16 (10.5%) were charge nurses or above. In terms of current department, 62 (40.8%) were in the Intensive Care Unit (ICU) and 45 (29.6%) were in the ward. In total, 55 (36.2%) had been involved in caring for COVID-19 patients for 3~5 months and 35 (23.0%) for 6~11 months, with a mean of 7.34 months. The difference in person-centered care according to the participants' general characteristics was significant by position (t=2.49, p=.014). The mean score of charge nurses and above was 3.81±0.72, higher than that of staff nurses (3.42±0.57).
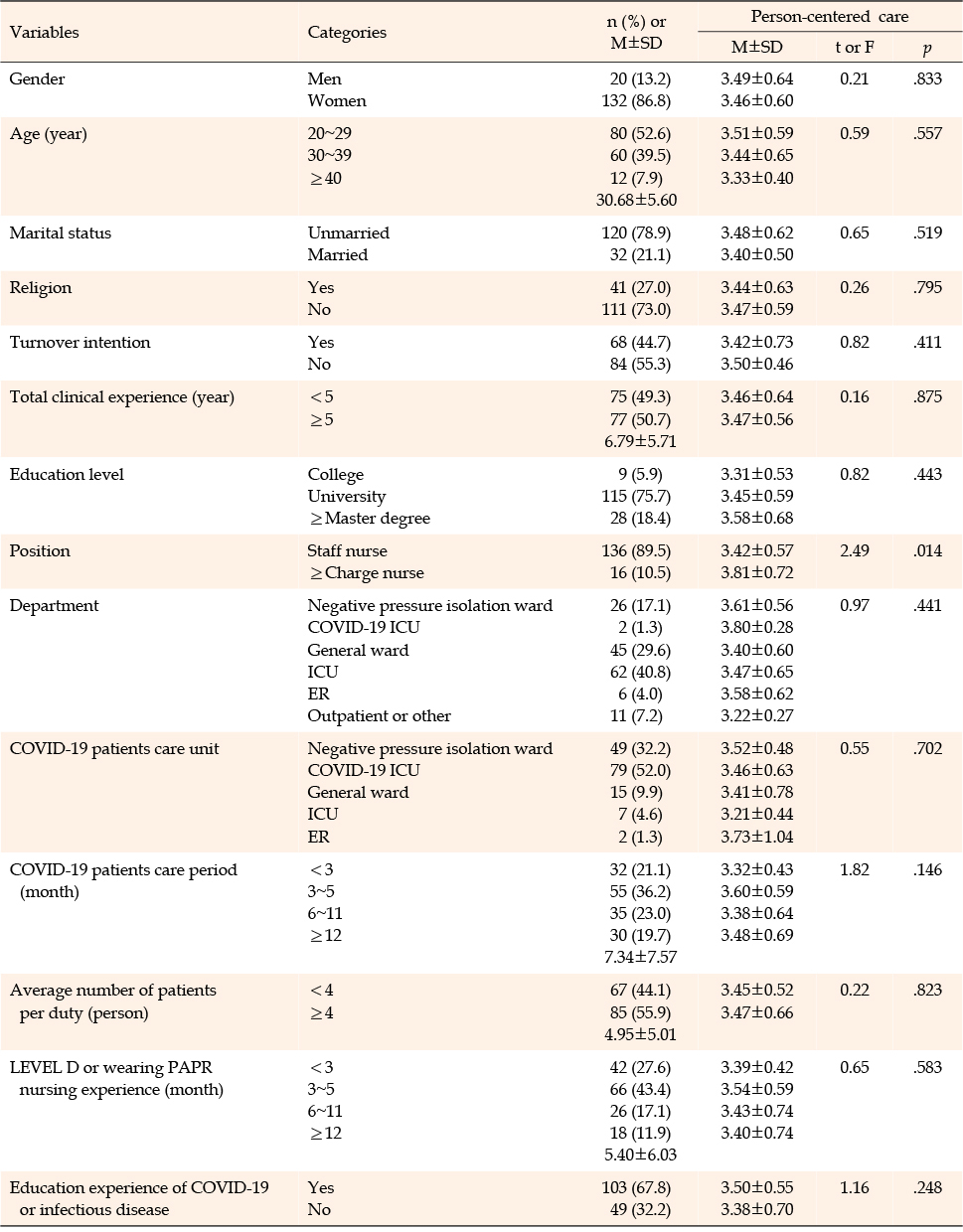
Table 1
General Characteristics and Person-Centered Care (N=152)
Participants' levels of COVID-19 stress and infection control fatigue and nursing work environment, team work, and person-centered care scores are shown in Table 2. COVID-19 stress had a mean of 3.33±0.63 out of 5; infection control fatigue, 3.64±0.62 out of 5; nursing work environment, 2.39±0.54 out of 4; and team work, 3.48±0.58. Person-centered care had a mean of 3.46±0.60 out of 5, and among the subdomains, comfort had the highest mean (3.75±0.74 out of 5), followed by respect (3.65±0.72), compassion (3.45±0.76), and individuality (3.08±0.77).
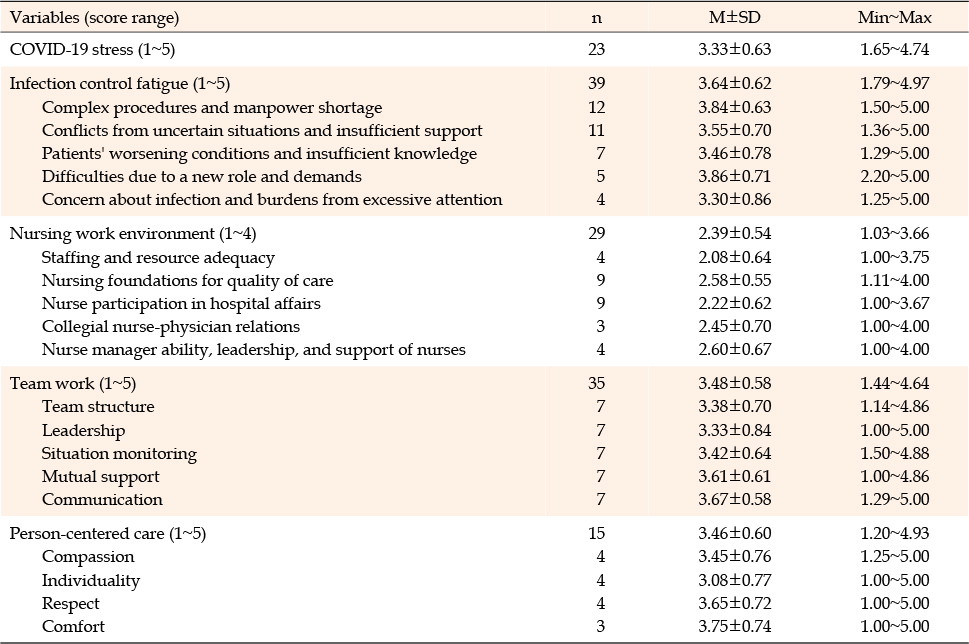
Table 2
COVID-19 Stress, Infection Control Fatigue, Nursing Work Environment, Team Work, and Person-Centered Care (N=152)
Correlations among COVID-19 stress, infection control fatigue, nursing work environment, team work, and person-centered care are shown in Table 3. Person-centered care had a statistically significant positive correlation with nursing work environment (r=.46, p<.001) and team work (r=.49, p<.001).
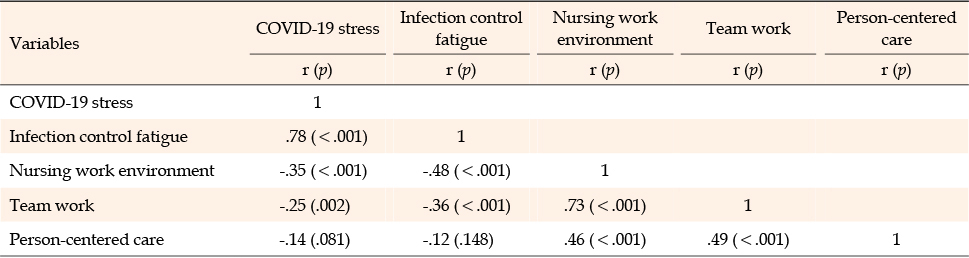
Table 3
Correlation among COVID-19 Stress, Infection Control Fatigue, Nursing Work Environment, Team Work, and Person-Centered Care (N=152)
To identify factors affecting person-centered care among nurses in tertiary hospitals caring for COVID-19 patients, we entered position variables significantly associated with person-centered care among the general characteristics as dummy variables based on staff nurses. The results of the hierarchical multiple regression analysis with nursing work environment and team work, which showed a statistically significant correlation with person-centered care based on the statistical significance level (p<.050), are shown in Table 4.
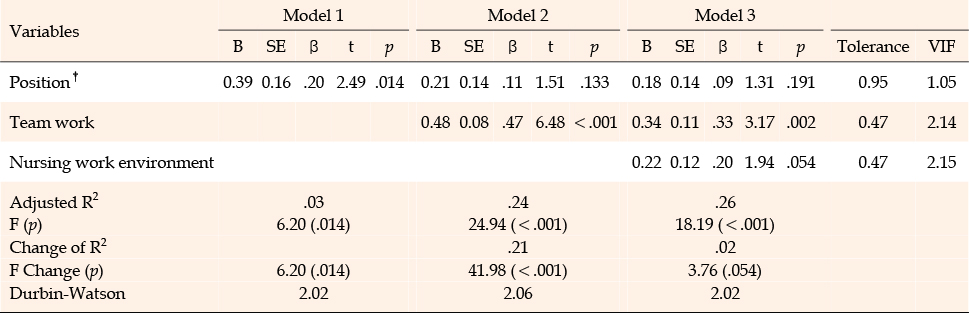
Table 4
Factors Influencing Performance of Person-Centered Care (N=152)
To perform the hierarchical multiple regression analysis, we checked multicollinearity to determine whether the basic assumptions are met, and the Durbin-Watson α was close to 2 (2.02), so there is no problem of autocorrelation of errors. To check the normality and equidispersion of the residuals, we checked the normal probability graph and scatter plot of the residuals. The residuals were close to a 45-degree straight line, and the scatter plot of the residuals was evenly distributed around 0, so the normality and equidispersion of the residuals are satisfied. The tolerance margins ranged from 0.47 to 0.95 (above 0.1), and the variance expansion factors ranged from 1.05 to 2.15 (not above 10), indicating no multicollinearity among the independent variables.
Hierarchical multiple regression analysis revealed that in Model 1, which included "position" among the general characteristics that showed a significant difference in person-centered care, position (β=.20 p=.014) was a factor affecting the performance of person-centered care (F=6.20, p=.014), with an explanatory power of 3.3%.
When team work was additionally entered in Model 1, team work (β=.47 p<.001) was found to be a significant factor influencing person-centered care in Model 2 (F=24.94, p<.001). The explanatory power of Model 2 increased by 20.8% from Model 1, with an explanatory power of 24.1% and a significant F change (F=41.98, p<.001).
Finally, to check if nursing work environment influences person-centered care, we added nursing work environment to Model 2 and found that team work (β=.33 p=.002) influences person-centered care in Model 3 (F=18.19, p<.001). The explanatory power increased by 1.4% from Model 2, resulting in an explanatory power of 25.5%. Model 3 had the highest explanatory power for person-centered care, and based on Model 3, the factor affecting person-centered care is team work (β=.33, p=.002). In other words, positive perceptions of team work increased the subjects' performance of person-centered care.
This study aimed to identify factors affecting the person-centered care of nurses in tertiary hospitals caring for patients with COVID-19 to provide a basis for the promotion of person-centered care. With the aim of improving nurses' person-centered care in the context of an infectious disease epidemic, we will discuss the following based on the results of the study.
In this study, the person-centered care scores of tertiary hospital nurses caring for COVID-19 patients were an average of 3.46 out of 5. This finding is similar to the mean of 3.51 obtained in a study of ICU nurses [14]. By subdomain of person-centered care, comfort scored highest, followed by respect, compassion, and individuality. This finding concurs with previous studies [13, 14]. The highest scoring domain, comfort, relates to environmental comfort, such as ensuring that there are no unnecessary noises in the room, working to reduce unpleasant odors, and adjusting lighting at night to help patients sleep. The highest scores in the comfort subdomain seem to be resulting from nurses' efforts to make the environment as comfortable as possible for patients. The lowest scoring domain was Individuality, which involves allowing patients to bring their usual items and participate in daily activities and family visits for personal hygiene and meals. Individuality scoring lowest can be explained by the environmental context, as hospitals have tightened their guidelines owing to the spread of COVID-19.
Person-centered care according to the general characteristics of subjects differed significantly by position (t=2.49, p=.014). Charge nurses and above scored 3.81 on average, higher than the mean score of 3.42 among staff nurses. The finding is consistent with a study [20] that identified the influencing factors of person-centered care among nurses in dedicated hospitals. A study [29] comparing the resilience of new and experienced nurses found that new nurses were unskilled in performing nursing tasks, experienced psychological pressure related to work and interpersonal relationships, and had lower resilience than experienced nurses, indicating that they had lower clinical competence in the identification of patient conditions, clinical judgment, and consideration of various aspects of patients when performing nursing care. Findings that clinical core competencies improved after receiving training in a program for new nurses [30] and a study that reported improved self-efficacy and reduced anxiety in nurses who received COVID-19 training [31] indicate the need to develop educational programs to promote the practice of person-centered care to effectively respond to infectious diseases and improve nursing competencies. Nurses in tertiary hospitals have the burden of caring for patients with infectious diseases, and they care for critically ill patients who require challenging treatment and skilled care [19]. Therefore, it is critical to establish a customized system and education program for tertiary hospital nurses.
It was found that nurses experienced significantly higher levels of stress due to the COVID-19 situation in a study of Polish nurses [32] and a study of frontline nurses' stress in Wuhan and Shanghai [8]. However, in this study, COVID-19 stress was not found to be a factor affecting person-centered care. Nurses used numerous coping strategies to solve problems, adapt to situations, and manage stress in the context of COVID-19 [32]. Stress was not found to be a factor affecting person-centered care, probably because nurses developed many coping strategies as the pandemic prolonged, and their ability to adapt increased as changes in routines became familiar and stimuli became more common.
A study exploring infection control fatigue in nurses caring for COVID-19 patients found it to be a predictor of depression [11], and a subset of infection control fatigue, conflict with uncertainty and lack of support, was a predictor of burnout [33]. In this study, however, infection control fatigue was not a factor affecting person-centered care among tertiary hospital nurses caring for patients with COVID-19. A study of nurses in a dedicated COVID-19 hospital [20] did not find infection control fatigue to be a factor in person-centered care either, supporting the findings of this study. This study included tertiary hospital nurses who wore LEVEL D or PAPR for at least 1 month of direct nursing care of patients with confirmed COVID-19. 57.3% of the nurses had worked for 5 months or less, and 71.0% had worked for 5 months or less wearing PPE during their nursing duties. Many subjects in this study had a total service length of 5 months or less because although bed adjustments were made owing to the increase in critically ill patients due to the pandemic [3], trained infectious disease specialists were insufficient for the number of beds, resulting in abrupt rotation of existing nurses and temporary assignments [34]. Thus, the high proportion of new nurses in COVID-19 isolation wards and short length of service may have had reduced the impact of infection control fatigue. Distancing measures were lifted in late March 2022 after the outbreak began to decline, and on May 2, 2022, the requirement to wear a mask outdoors was lifted, as the guidelines were eased [35]. The reason infection control fatigue did not appear to be a factor affecting person-centered care is likely the time frame of the study, September-October 2022, when relaxed guidelines simplified the use of PPE and reduced fatigue associated with wearing it, as opposed to the early days of COVID-19, when all nurses were required to wear PPE.
In this study, nursing work environment had a statistically significant positive correlation with person-centered care (r=.46, p<.001). Hierarchical multiple regression analysis identified nursing work environment (β=.20, p=.054) as a variable worth considering (p=.054), although it was not significant at the significance level of p<.05 in this study. Nursing work environment has been found to be significantly and positively correlated with person-centered care among ICU nurses [13], and in a study of nurses in a dedicated COVID-19 hospital, it was shown to be a factor influencing person-centered care [6]. It is necessary to develop strategies for positively perceiving the nursing work environment and increasing the practice of person-centered care in disaster response [12].
Team work was identified as a factor influencing person-centered care among tertiary hospital nurses caring for patients with COVID-19. The same was confirmed in a study of ICU nurses [14], supporting the finding of this study that the more positive the perception of team work, the more person-centered care is practiced. The highest-scoring component of team work was communication, with an average score of 3.67, followed by mutual support (3.61), situation monitoring (3.42), team structure (3.38), and leadership (3.33). During the COVID-19 pandemic, nurses could communicate with their colleagues about the challenges they faced in caring for patients and work together to resolve them, increasing their trust in their colleagues, confidence in their work, and the effectiveness of their nursing practice [7]. Team work, based on the cooperation of colleagues, can help tertiary hospital nurses make decisions and perform tasks promptly [18]. The finding that team work affects the person-centered care of tertiary hospital nurses caring for COVID-19 patients suggests that it is important to improve team work competence through educational programs to enhance nurses' person-centered care performance.
Several limitations need to be acknowledged: First, although bed adjustments were made owing to an increase in the number of severely ill COVID-19 patients [3], there were insufficient trained infectious disease specialists to cover the number of beds, resulting in an abrupt rotation of nurses who had previously worked in general wards to negative pressure wards and temporary assignments [34]. In this study, 57.3% of nurses had worked for 5 months or less in total, and 71.0% of nurses had worked with PPE for 5 months or less. Therefore, there are limitations in generalizing the results of this study to all tertiary hospital nurses. Moreover, the study did not distinguish between nurses in wards with existing COVID-19 patients and nurses who were seconded from other departments, so this should be addressed in further studies.
Since COVID-19 was declared an international public health emergency by the World Health Organization in January 2020, there have been numerous cases and deaths, and the fifth wave of the pandemic, in which the number of confirmed cases increased drastically owing to the spread of the omicron mutant virus, led to a shift to a response system centered on critically ill patients and intensified quarantine policies, but the number of confirmed cases is now declining and most quarantine policies have been relaxed [35]. Faced with the easing of the epidemic environment, tertiary hospitals should confirm the protocols established during the pandemic and organize appropriate programs and strategies based on the situation and characteristics to solidify the foundation of the health care system. Nurses in tertiary hospitals should explore ways to enhance person-centered care through the development of intervention programs and institutional arrangements that can promote positive perceptions of the nursing work environment and enhance teamwork.
This descriptive study of tertiary hospital nurses caring for patients with COVID-19 was conducted to identify factors affecting person-centered care. The most significant factor affecting person-centered care among tertiary hospital nurses was perceived team work, with an explanatory power of 25.5%.
This study was conducted with a convenience sampling of tertiary hospital nurses who had experience caring for patients with COVID-19, so it may not be representative of the characteristics of all tertiary hospital nurses. As the study did not distinguish between nurses who were already working in wards with COVID-19 patients and nurses sent from other departments to care for confirmed patients, future studies would benefit from a comparison of the groups. Despite these limitations, this study has clinical α as a source of evidence for tertiary hospital nurses to practice person-centered care in the context of COVID-19. According to the study results, tertiary hospital nurses should identify the severe patient infectious disease response protocols developed during the pandemic to adapt to the changing environment of emerging infectious diseases with relaxed epidemic prevention policies, establish a system tailored to the situation, and promote team work to efficiently respond to emerging infectious diseases. The importance of team work among tertiary hospital nurses makes it necessary to improve the working environment for collaborative work, develop educational programs to promote team work, and verify their effectiveness.
CONFLICTS OF INTEREST:Kisook Kim has been the Editor-in-Chief of the Korean Journal of Adult Nursing since 2022. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - KK and KS.
Data collection - KK and KS.
Analysis and interpretation of the data - KK and KS.
Drafting and critical revision of the manuscript - KK and KS.
 E-SUBMISSION
E-SUBMISSION