
Purpose
The triage process in the emergency department is a complex decision-making task influenced by individual competence and a multitude of factors. Unlike patient-related factors, nurse-related factors can be improved through education. This study sought to determine the impact of grit, self-leadership, and communication skills of emergency department nurses on their triage competency.
Methods
We surveyed a convenience sample of 152 emergency department nurses to evaluate their grit, self-leadership, communication skills, and triage competency. The differences in these skills and competencies were analyzed according to the participants' general characteristics using the independent t-test and one-way analysis of variance. Hierarchical regression analysis was performed to identify the factors influencing nurses' triage competency.
Results
Triage experience, self-leadership, and communication skills influenced triage competency. Although triage competency can be positively impacted by knowledge gained from experience, expert assessment was identified as the least developed category of triage competency.
Conclusion
To improve nurses' triage competency, it is necessary to implement educational programs that utilize various methods to address self-leadership and communication skills. Moreover, reflective methods can be employed to help develop self-leadership, thereby improving triage competency. These findings can contribute to improving the work culture and the development of educational programs. Specifically, these programs should treat nurses' mistakes during work as learning opportunities rather than failures, thereby significantly advancing their competency.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
The triage process in the emergency department is a complex decision-making task influenced by individual competence and a multitude of factors. Unlike patient-related factors, nurse-related factors can be improved through education. This study sought to determine the impact of grit, self-leadership, and communication skills of emergency department nurses on their triage competency.
We surveyed a convenience sample of 152 emergency department nurses to evaluate their grit, self-leadership, communication skills, and triage competency. The differences in these skills and competencies were analyzed according to the participants' general characteristics using the independent t-test and one-way analysis of variance. Hierarchical regression analysis was performed to identify the factors influencing nurses' triage competency.
Triage experience, self-leadership, and communication skills influenced triage competency. Although triage competency can be positively impacted by knowledge gained from experience, expert assessment was identified as the least developed category of triage competency.
To improve nurses' triage competency, it is necessary to implement educational programs that utilize various methods to address self-leadership and communication skills. Moreover, reflective methods can be employed to help develop self-leadership, thereby improving triage competency. These findings can contribute to improving the work culture and the development of educational programs. Specifically, these programs should treat nurses' mistakes during work as learning opportunities rather than failures, thereby significantly advancing their competency.
The importance of the Emergency Department (ED) has grown in tandem with the rise in the number of ED users [1]. The ED plays a crucial role in classifying patients by severity and preventing overcrowding [1]. Moreover, the ED is instrumental in initially screening critically ill patients and effectively allocating appropriate medical resources and the flow within the ED. At present, ED nurses are responsible for performing triage in most EDs [2]. As the complexity and severity of patients visiting the ED increase, these nurses need triage competency to identify patients' clinical features early on and provide immediate intervention [2]. The Korean Triage and Acuity Scale (KTAS) was developed in 2012, coinciding with the emergence of triage in Korea. By January 2016, the KTAS was implemented in emergency medical centers nationwide for triage purposes [3]. The KTAS assesses patients who visit the ED based on process impression evaluation, infection confirmation, primary symptom selection, and primary or secondary considerations [3].
ED triage is a multifaceted decision-making process, influenced by individual competence and a variety of factors [2]—namely, patient-related, nurse-related, and environmental factors. Patient-related factors, as reported in the literature, encompass the primary complaint, underlying disease, vital signs, mode of transportation, physical appearance, pain level, and medical history, among others [4, 5, 6]. Nurse-related factors include experience, knowledge, beliefs, communication skills, and intuition [7, 8]. Environmental factors, on the other hand, involve ED overcrowding, human resources, and relationships with other hospital units [9].
Unlike patient-related factors, nurse-related and environmental factors can be improved; in particular, education can enhance nurse-related factors. Nurses are healthcare professionals who maintain direct and enduring relationships with patients. They have the crucial responsibility for accurately identifying clinically significant patient issues through patient communication and the establishment of mutual trust [10]. Factors such as self-leadership and communication skills have been identified as being related to nursing competency and nursing work outcomes [7, 8]. Bedside nurses often self-motivate by setting personal goals to improve their work performance or advance their skills [11]. Self-leadership, with its emphasis on self-management and intrinsic motivation, can equip nurses to proactively tackle problems and efficiently carry out tasks in emergency situations [8]. The communication skills of ED nurses significantly impact the effectiveness and accuracy of information exchange among healthcare providers. However, most research on self-leadership and communication has been primarily focused on their relationship with job performance or nursing work outcomes among general nurses [12, 13, 14]. Therefore, scarce evidence exists regarding the influence of self-leadership and communication on triage competency specifically among ED nurses.
Grit can also affect ED nurses' competence. Grit refers to consistent passion and effort toward a long-term goal. This implies continuously striving despite failure, adversity, frustration, and the plateau phenomenon in the process to achieve goals [15]. Importantly, people with high levels of grit demonstrate strong self-control. Therefore, these individuals can concentrate on imminent tasks and have a positive mindset. Consequently, they accept challenges and use them as learning opportunities, even if they fail [16].
Studies have examined the effect of ED nurses' critical thinking disposition on triage. However, to the best of our knowledge, no studies have considered self-leadership, communication skills, and grit, which are important factors for voluntarily and actively improving practical performance. Thus, this study aimed to identify the effect of ED nurses' self-leadership, communication skills, and grit on nurses' triage competency. Moreover, this study provides basic data for improving the quality of nursing at clinical sites.
This study used a descriptive correlational method to explore the associations of ED nurses' grit, self-leadership, and communication skills with their triage competency.
The study participants were nurses working at the EDs of 5 general and 2 tertiary general hospitals. In particular, this study targeted nurses with over 1 year of experience who had completed training on how to use the KTAS and had practical experience in conducting triage, in order to investigate the factors influencing triage competency. These participants were informed of the purpose of the research and participated voluntarily in the study after providing their written consent. The number of research participants was calculated using the G*Power 3.1.9 program. The effect size was determined by referencing the value (0.15) used in similar previous studies for calculating the required number of research participants [13, 14]. With a medium effect size of 0.15, power of .80, a significance level of .05, and 12 independent variables (grit, self-leadership, communication skills, and nine potential control variables) for linear multiple regression analysis, the minimum required sample size was 127 individuals. Considering possible attrition, we aimed to recruit 170 participants. Among the 163 collected responses, 11 were excluded due to not meeting the inclusion criteria, resulting in a final analysis of 152 survey responses.
This study was approved by the Institutional Review Board of G University on March 12, 2021 (no. 1044396-202102-HR-036-01). After reading an informative document detailing the study's objectives, contents, procedures, confidentiality measures, voluntary nature of participation, and the option to withdraw at any time, the participants were given the opportunity to take part in the survey. They were informed that the personal data collected during the study would remain strictly confidential and would solely be utilized to provide rewards for their participation, and that any identifiable information would be promptly destroyed after completion of the study. The data will be securely stored for a period of 3 years after the analysis and then will be properly disposed of.
The general characteristics of the participants included age, sex, educational background, ED clinical experience, and position. Their work-related characteristics consisted of questions about emergency nurse practitioner qualification, triage work experience, types of triage work situations, and experience with triage education and re-education. For the purpose of this study, an "emergency nurse practitioner" refers to a nurse who has obtained a master's degree and has qualifications recognized by the Ministry of Health and Welfare.
This study employed the instrument developed by Park et al. to measure grit [17]. This instrument comprises a self-report questionnaire based on several statements including "I have a clear goal to be a nursing professional," "I try to solve the problem that I have in my capacity as a nurse," and "I am happy when the patient's condition is improving." Specifically, this instrument has three sub-areas with a total of 14 questions: five questions on persistence to achieve long-term goals, five questions on respondents' passion to become a nursing expert, and four questions on patient-oriented internal motivation. Each question was assessed on a 4-point Likert scale with higher scores indicating higher grit. In this study, Cronbach's α was .81, while Park et al. reported a value of .72 [17].
This study used Kim's modified version of the questionnaire [18] developed by Manz [19] to measure self-leadership. This instrument comprises six sub-areas: self-expectation, rehearsal, goal-setting, self-compensation, self-criticism, and constructive thinking. Each subarea consists of three questions, yielding a total of 18 questions. Each question is measured on a 5-point Likert scale, with higher values reflecting higher self-leadership. Despite the long existence of this tool, the researchers used it after confirming that the content of the items did not pose any difficulties in measuring the self-leadership of nurses at present. In the current study, Cronbach's α was .74, whereas that found in Kim's study was .87 [18].
This study utilized Lee and Kim's [20] modified version of the Global Interpersonal Communication Competence Scale (GICC) to measure communication skills. The GICC was revised by Hur [21] according to the concept of 10 communication skills suggested by Rubin et al. [22]. The GICC consists of 15 questions, each of which measures one of 15 concepts: self-disclosure, empathy, social relaxation, assertiveness, concentration, interaction management, expressiveness, supportiveness, immediacy, efficiency, social appropriateness, conversational coherence, goal detection, responsiveness, and noise control. Each question is measured on a 5-point Likert scale, with a higher score indicating a higher degree of communication skills. Cronbach's α was .79 in the current study and .72 in Hur's study [21].
Finally, to assess triage competency, we used the instrument developed by Moon & Park [23]. This instrument is a self-report questionnaire that uses statements to investigate nurses' perceptions of specific triage competencies. Examples of items include "I can intuitively identify a patient experiencing a cardiac arrest," "During an interview with patients for triage, I can examine patients by scanning them from head to toe," and "I am aware of the types of medical resources available at the emergency room." In total, this instrument comprises 30 questions: 13 questions on clinical judgment, four questions on professional assessment, four questions on management, four questions on personal coping, and five questions on communication. The communication items within the subdomain of triage competencies are centered on effective communication during the triage. These items include statements such as "Patients understand well when I ask questions or provide explanations" and "I easily perceive what the patient intends." Each question is assessed on a 5-point Likert scale, with higher scores indicating a higher level of triage competency. Cronbach's α for the current study was .80, while Moon and Park reported a value of .91 [23].
The data were collected through an online survey using Google Forms from April 15 to May 5, 2021, with the permission of the nursing departments of the seven hospitals. ED nurses were recruited using announcements on the hospitals' social media platforms. Nurses who wanted to participate in the study voluntarily accessed the survey link and read an explanation of the study's purpose, after which they took part in the survey. Among the 163 responses received, 11 responses were from participants with less than 1 year of ED experience. Participants not trained on how to use the KTAS were also excluded. Finally, responses from 152 participants were included in the analysis.
Data analysis was performed using SPSS/WIN 21.0. The participants' general characteristics, grit, self-leadership, communication skills, and triage competency were analyzed using mean and standard deviations. Differences in grit, self-leadership, communication skills, and triage competencies according to the participants' general characteristics were analyzed using the independent t-test, one-way analysis of variance, and the Scheffé post-hoc test. After controlling for significant variables in the univariate analysis, hierarchical regression analysis was conducted to assess the incremental contribution of the predictor variables in explaining the variance of triage competency. Hierarchical regression allows the researcher to determine the order of variable entry based on their theoretical relevance. In this research, to explore new influencing factors, the first variable that was entered was grit, which has been relatively unexplored in previous studies on factors impacting triage competency among ED nurses. In contrast, communication skills, which have been more extensively investigated, were entered last.
Multicollinearity was assessed using the Variance Inflation Factor (VIF). A commonly used VIF cutoff is 5.0; however, some studies found that VIFs less than 5.0 indicate considerable collinearity [24, 25]. We selected a conservative VIF cut-off value of 3.0 to exclude variables based on a previous study [25]. In the first step of the analysis, position, education level, triage experience, and triage re-education were entered as control variables. Age, clinical experience, and emergency nurse practitioner qualification were also significant variables in the univariate analysis; however, these variables were excluded because their VIFs were greater than the cutoff of 3.0. In the second step of the hierarchical regression analysis, after entering grit as a predictor, self-leadership was added as another predictor in the third step. Finally, in the fourth step, communication skills were included in the model to examine their individual impact on the dependent variable.
Data from 152 participants were analyzed. The participants were mostly women (90.1%), and their average age was 30.20±5.53 years old. Furthermore, 117 nurses (77.0%) had a bachelor's or associate degree. Most participants were staff (61.8%) and charge nurses (30.9%) with an average clinical experience of 6.23±4.64 years. The majority of the participants had received triage education (87.5%), but most had not received re-education (84.2%), and only 10 nurses (6.6%) had the emergency nurse practitioner qualification. The average triage experience was 34.28±28.00 months (Table 1).
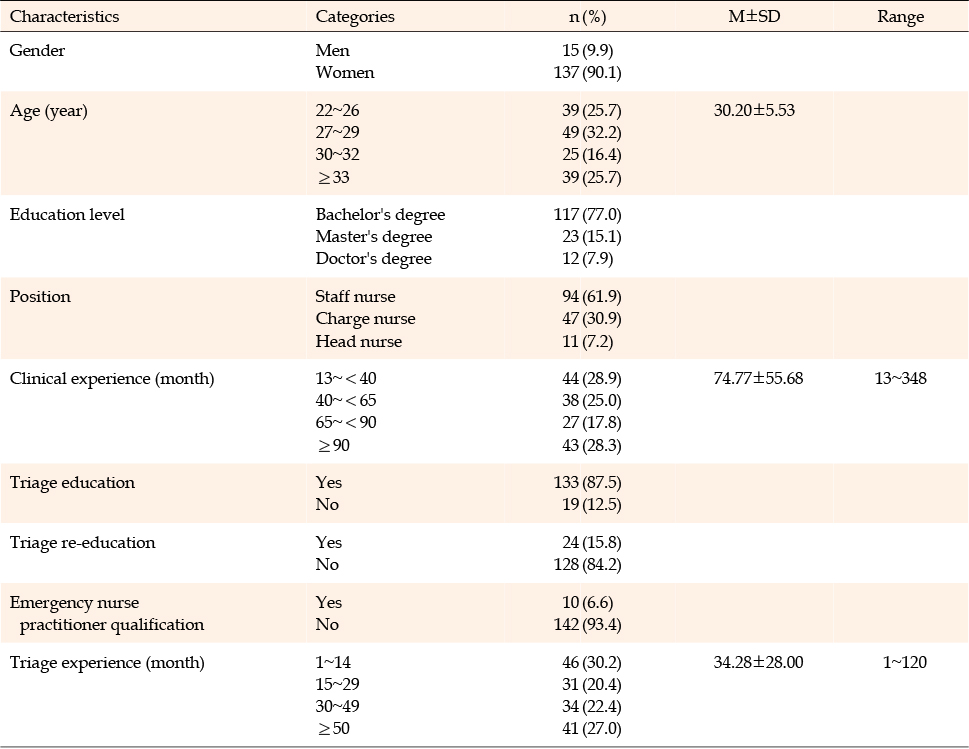
Table 1
General Characteristics and Triage-Related Factors of the Participants (N=152)
The mean score for grit was 2.94±0.47 out of 5. The highest-scoring sub-area of grit was "passion to become a nursing expert," with an average of 3.11±0.52. The self-leadership score was 3.43±0.51 out of 5. Among the subareas of self-leadership, "self-compensation" had the highest score (3.85±0.69), whereas "self-criticism" had the lowest score (2.52±0.78). The mean score for communication skills was 3.61±0.47 out of 5 (Table 2).
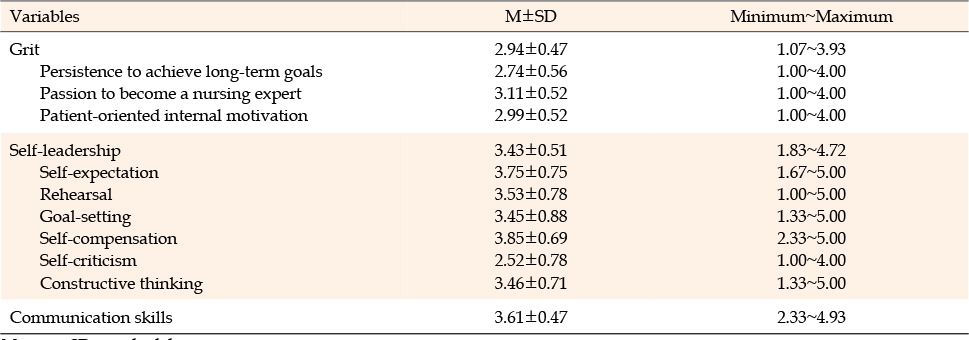
Table 2
Grit, Self-Leadership, and Communication Skills of the Participants (N=152)
The average score for triage competency was 3.66±0.70 of 5. Among the sub-categories, "management" scored the highest, followed by "communication," "personal coping," "clinical judgment," and "expert assessment" (Table 3).
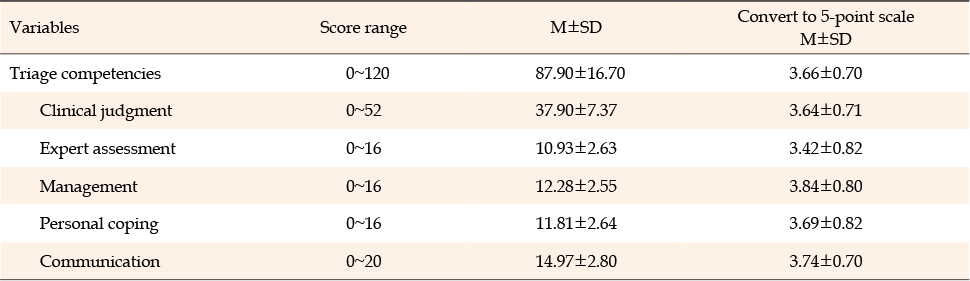
Table 3
Triage Competencies of Participants
Regarding the participants' general characteristics, self-leadership was significantly different according to age (F=3.43, p=.019), education level (F=10.60, p<.001), position (F=3.64, p=.014), and clinical experience (F=5.65, p<.001). A significant relationship was observed between communication skills and educational level (F=8.24, p<.001). Grit significantly differed according to age (F=6.61, p<.001), education level (F=17.82, p<.001), position (F=3.92, p=.010), and clinical experience (F=9.88, p<.001). Moreover, triage competency demonstrated significant associations with age (F=2.85, p=.040), education level (F=11.85, p<.001), position (F=3.34, p=.021), and clinical experience (F=6.91, p<.001) (Table 4).

Table 4
Differences in Self-Leadership, Communication Skills, Grit, and Triage Competency according to Participants' General Characteristics (N=152)
In the analysis of triage-related characteristics, self-leadership showed significant differences according to triage re-education (t=2.40, p=.018), emergency nurse practitioner qualification (t=2.63, p=.009), and triage experience (F=3.57, p=.016). Furthermore, communication skills had significant associations with triage re-education (t=2.69, p=.008) and emergency nurse practitioner qualification (t=2.98, p=.003). Grit significantly differed according to emergency nurse practitioner qualification (t=4.11, p<.001) and triage experience (F=4.21, p=.007). Moreover, triage competency presented significant associations with triage re-education (t=2.11, p=.044), emergency nurse practitioner qualification (t=3.96, p<.001), and triage experience (F=7.30, p<.001).
Hierarchical regression analysis was conducted to investigate the individual effects of each independent variable, while controlling for covariates, on triage competency in ED nurses. Specifically, grit, self-leadership, and communication skills were included as independent variables. Among the participants' characteristics, the VIFs of age (3.88), clinical experience (4.31), and emergency nurse practitioner qualification (3.18) exceeded the cutoff value of 3.0; thus, they were excluded. Consequently, education level, position, triage experience, and triage re-education were integrated into the final model for control variables. The VIFs ranged from 1.06 to 1.71 in Model I, from 1.10 to 1.76 in Model II, from 1.11 to 1.97 in Model III, and from 1.13 to 2.33 in Model IV. The Durbin-Watson statistic was calculated at 2.05, indicating no autocorrelation. Additionally, it was determined that the residuals satisfied the assumptions of homoscedasticity and a normal distribution.
Model I included the general characteristics affecting triage competency and resulted in an adjusted R2 of .18. Triage experience emerged as the most influential factor, with a coefficient (β) of .23. Model II incorporated grit as an independent variable, leading to an adjusted R2 of .25. Notably, high levels of grit were positively associated with triage competency, with a coefficient (β) of .30. In Model III, self-leadership was added as an independent variable to Model II. This model exhibited an adjusted R2 of .42, and self-leadership emerged as the most influential factor, with a coefficient (β) of .56. Lastly, Model IV incorporated general characteristics, grit, self-leadership, and communication skills. This comprehensive model demonstrated a total explanatory power of 47.0%. Notably, self-leadership remained the most influential factor, as higher levels of self-leadership were associated with increased triage competency, with a coefficient (β) of .41 (Table 5).
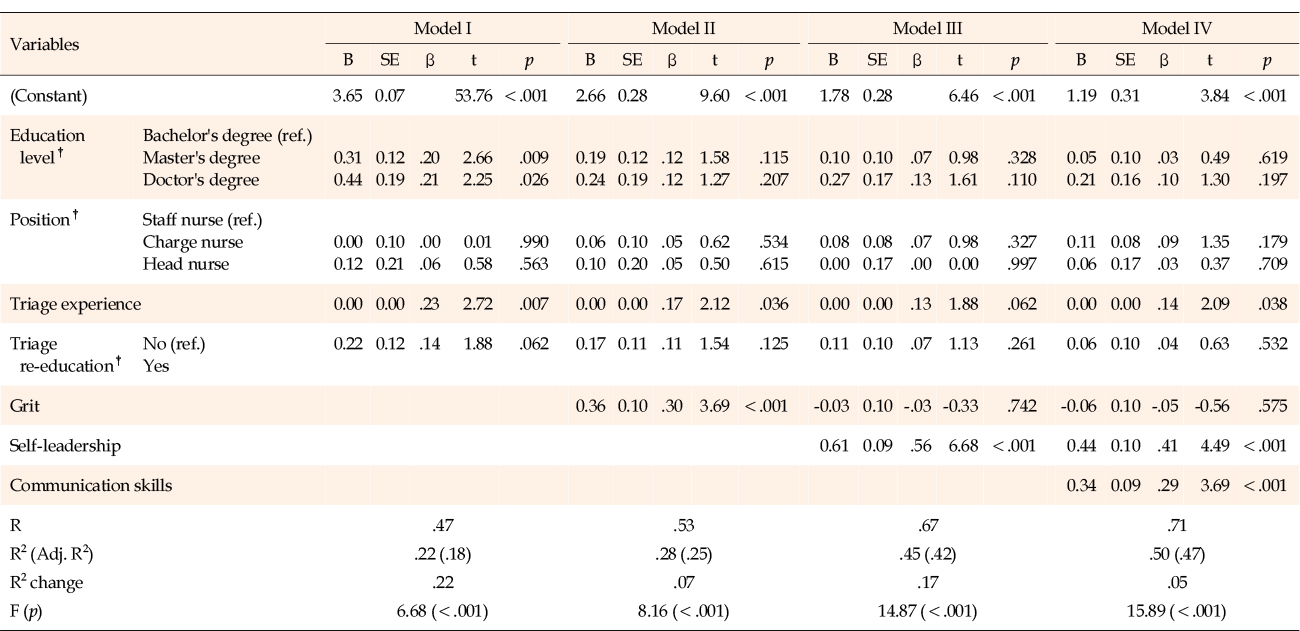
Table 5
Factors Influencing Triage Competency (N=152)
This study examined the relationship between ED nurses' triage competency and their grit, self-leadership, and communication skills. Importantly, self-leadership, communication skills, and triage experience were identified as explanatory factors of triage competency. The final model (Model IV) of hierarchical regression analysis showed an explanatory power of 47.0%. Among the predictor variables, self-leadership was found to be the most significant variable for explaining triage competency in ED nurses.
Previous studies conducted in Korea have reported that self-leadership influenced nursing job performance and nursing work outcomes [12, 13]. A previous study [12] found that improving the nursing work environment increased self-leadership, which in turn enhanced nursing performance. Therefore, establishing management strategies that improve the nursing work environment and enhance self-leadership, which is characterized by positive self-perception, responsibility, and autonomy, is necessary to improve nurses' performance [12].
This study confirmed that self-leadership not only affected nursing performance, but also significantly contributed to triage competency in ED nurses. Self-leadership focuses on self-efficacy and intrinsic motivation, guiding and leading oneself in a rational direction and emphasizing autonomy and responsibility. A previous study conducted in Korea showed a positive correlation between nurses' self-leadership and autonomy, self-efficacy, relationality, and stability [14]. Therefore, it is suggested that ED nurses who possess self-leadership exhibit a high level of engagement in the task of patient triage, which contributes to the improvement of their triage competency. To enhance triage competency, it is necessary to create a nursing work environment in the clinical setting that allows nurses performing the essential task of patient triage to fully demonstrate their autonomy and expertise.
Triage places a registered nurse in a position to evaluate the urgency of treatment. This task requires the psychological and social management of nurses due to time pressure. Self-leadership has the potential to improve psychological and social management [8], and investigating whether triage in the ED is enhanced by self-leadership practices can be a good starting point for future research.
Considering the sub-categories of self-leadership, "self-criticism" (i.e., critiquing oneself when something goes wrong) scored the lowest at 2.52 points. A study [18] found that although mild guilt can be effective, excessive or habitual guilt can lower one's motivation to try [18]. Therefore, it is important for individuals to reflect on their shortcomings through appropriate self-criticism. Furthermore, it is essential for individuals to analyze the causes of failure and learn from them to avoid repetition. However, it is just as important to avoid being excessively critical. To demonstrate self-leadership that emphasizes one's potential and autonomy, the problems faced by young ED nurses with limited experience in the clinical field need to be effectively mitigated.
During the handover process in the ED, the effectiveness and accuracy of information exchange between paramedics and triage nurses are influenced by their proficiency in communication skills. Communication skills also play a role in determining whether a patient can be accurately assessed within a limited timeframe [26]. The absence of bedside communication skills is a major factor contributing to underperformance among nurses [27]. The findings of this study indicate that communication skills are significant factors affecting ED nurses' triage competency. Triage involves making decisions based on the patient's condition, and previous studies conducted among Korean nurses have emphasized the importance of communication skills in the decision-making process [28], aligning with the results of this study.
When a surge in volume occurs, having access to the available resources is relevant for thoroughly assessing each patient and ensuring the correct treatment. This is of particular concern since poor or missing information may result in incomplete or faulty patient assessment [29]. Engagement with patients is a possible facilitator for accurate triage. Since the ED lacks information about patients compared to other departments, nurses' communication skills are important in terms of eliciting statements and opinions from patients.
In Model II, grit was identified as a factor influencing the triage competency of ED nurses. Grit motivates nurses to withstand challenges and succeed over time. Cultivating grit among clinical nurses is important to maintain their interest in emergency preparedness and to ensure that the needs of patients and caregivers are met [30]. At times, critical patients can be admitted to the ED's special work environment. grit can impact triage competencies as it enables nurses to approach triage with a sense of challenge rather than fear. A study conducted with Colombian healthcare providers corroborates our findings, indicating that grit negatively correlated with decision fatigue [31]. Grit is recognized as a personality trait that may serve as a protective factor against compassion fatigue and decision fatigue [31]. However, when self-leadership and communication skills were incorporated into the final model, grit did not emerge as a significant variable. A study suggests that there is no significant correlation between the disaster triage ability and grit of ED nurses in Korea [32]. Research on grit has been limited and the results have been inconsistent. Therefore, further research is warranted to gain a more comprehensive understanding of this topic.
The results showed that education level, and triage experience had explanatory power in Model I. Previous studies have suggested that higher education levels contribute to increased knowledge and experience in triage, enabling nurses to handle a wider variety of patients [33].
Despite their extensive clinical experience, nurses have reported encountering similar challenges when problem-solving within a resource-limited, comprehensive triage system [34]. Experienced nurses often rely on rapid observation or intuition, but the importance of data collection and confirmation has been emphasized [34]. Appropriate triage education programs should be implemented for both new and experienced nurses, with ongoing development at regular intervals. Practical guidelines and comprehensive classification processes should be included in educational programs, and simulation programs or standardized curricula have been identified as high-quality educational methods. Interactive and ongoing education and training are crucial due to the significant role of triage nurses in determining the treatment order [35], which affects patient safety and prognosis. Further research on the roles of knowledge and experience in triage competency could inform the development of education programs and improve decision-making outcomes.
Our study has implications for emergency clinical practice. Novice nurses may lack both experience and opportunities to improve their self-leadership and communication skills. This can present a major obstacle in terms of accurately determining the severity of a patient's condition in a short time. Therefore, improved work culture and educational programs can make it possible for nurses' mistakes during work to be seen as a learning opportunity rather than a failure, and this shift will further improve triage competency.
This study has several limitations. First, the study participants were ED nurses who worked on triage in EDs of general and tertiary general hospitals in an Incheon metropolitan area, which limits the generalizability of the findings to other EDs. The sample size was also relatively small (n=152), which may affect the statistical power and generalizability of the results. Second, since the triage competency survey instrument is self-reported, ED nurses may have overstated their responses; therefore, an objective evaluation of the accuracy of assigned triage scores may be necessary. Third, the study focused on the relationship between self-leadership, communication skills, grit, and triage competencies, and it did not explore other potential factors that could influence triage performance. Factors such as teamwork, organizational support, and workload could also play a role in nurses' triage competency. Future studies could incorporate a broader range of variables to gain a more comprehensive understanding of the factors influencing triage performance. Fourth, the cross-sectional design of the study limits the ability to establish causal relationships between the variables. Longitudinal or experimental studies would provide stronger evidence for understanding the impact of self-leadership, communication skills, and grit on triage competency. Fourth, two of the survey instruments utilized in this study—namely, those for self-leadership and communication skills—were originally developed in 1983 and 2003, respectively. Subsequently, modifications were introduced in 2002 and 2010 to enhance their applicability and relevance. However, since considerable time has elapsed since their original development, it is important to carefully consider their alignment with contemporary contexts while selecting these instruments for potential future measurements. Lastly, this study included head nurses, and it is not common for unit managers, such as head nurses, to perform patient triage in the ED. Additionally, among the study participants, some nurses reported not having received triage education. Considering that nurses typically perform triage after receiving relevant training, it cannot be ruled out that nurses who do not actually perform triage were included in the study. Therefore, careful interpretation of the study's results is necessary, and further research considering these limitations is needed.
The findings of this study highlight the significant role of self-leadership, communication skills, and triage experience in explaining ED nurses' triage competency, emphasizing the importance of improving self-leadership to enhance triage competency in nurses. Effective communication skills were identified as crucial factors influencing the triage competency of ED nurses, emphasizing the need for comprehensive communication training programs to ensure accurate patient assessment and decision-making within limited timeframes. While grit showed an initial influence on triage competency, its significance diminished when self-leadership and communication skills were considered, suggesting the need for further research to better understand the relationship between grit and triage competency in ED nurses and its potential role in addressing decision fatigue. The study provides valuable insights into the factors influencing triage competency and highlights the importance of continuous education, training, and creating a supportive work culture in EDs to enhance the skills and performance of ED nurses in triage settings.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - JG and LH.
Data collection - JG and LH.
Analysis and interpretation of the data - JG and LH.
Drafting and critical revision of the manuscript - JG and LH.
This manuscript is a revision of the first author’s master’s thesis from Gachon University. Year of 2021.
 E-SUBMISSION
E-SUBMISSION