
Purpose
This study aimed to investigate the impact of physical performance and fear of falling on fall risk in patients with End-Stage Renal Disease (ESRD) undergoing hemodialysis.
Methods: This study included 132 patients who regularly received hemodialysis treatment at outpatient clinics in B City from January to April 2022. Data were collected on demographic and clinical characteristics, physical performance (the Short Physical Performance Battery [SPPB]), fear of falling (the Korean Falls Efficacy Scale-International [KFES-I]), and fall risk (the Morse Fall Scale [MFS]). The collected data were analyzed using hierarchical multiple regression in the SPSS/WIN 25.0 program.
Results: Thirty-eight patients (28.8%) had experienced accidental falls in the past year, with an average of 1.68 falls per patient. The average SPPB score was 7.89±3.55 (range, 0 to 12), the KFES-I score was 23.18±9.36 (range, 16 to 64), and the MFS score was 45.68±19.52 (range, 0 to 125). Fall risk showed a significant negative correlation with physical function (r=-.72, p<.001) and a significant positive correlation with fear of falling (r=.65, p<.001). Factors affecting the patients' fall risk included the level of serum intact parathyroid hormone (β=.15, p=.004), fear of falling (β=.24, p=.010), number of falls (β=.34, p<.001), and physical performance (β=-.41, p<.001). The regression model was statistically significant (F=22.71, p<.001), with an explanatory power of 64.9%.
Conclusion: To prevent accidental falls in ESRD patients undergoing hemodialysis treatment, it is necessary to develop and apply interventions that can enhance physical performance and reduce the fear of falling.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
This study aimed to investigate the impact of physical performance and fear of falling on fall risk in patients with End-Stage Renal Disease (ESRD) undergoing hemodialysis.
This study included 132 patients who regularly received hemodialysis treatment at outpatient clinics in B City from January to April 2022. Data were collected on demographic and clinical characteristics, physical performance (the Short Physical Performance Battery [SPPB]), fear of falling (the Korean Falls Efficacy Scale-International [KFES-I]), and fall risk (the Morse Fall Scale [MFS]). The collected data were analyzed using hierarchical multiple regression in the SPSS/WIN 25.0 program.
Thirty-eight patients (28.8%) had experienced accidental falls in the past year, with an average of 1.68 falls per patient. The average SPPB score was 7.89±3.55 (range, 0 to 12), the KFES-I score was 23.18±9.36 (range, 16 to 64), and the MFS score was 45.68±19.52 (range, 0 to 125). Fall risk showed a significant negative correlation with physical function (r=-.72, p<.001) and a significant positive correlation with fear of falling (r=.65, p<.001). Factors affecting the patients' fall risk included the level of serum intact parathyroid hormone (β=.15, p=.004), fear of falling (β=.24, p=.010), number of falls (β=.34, p<.001), and physical performance (β=-.41, p<.001). The regression model was statistically significant (F=22.71, p<.001), with an explanatory power of 64.9%.
To prevent accidental falls in ESRD patients undergoing hemodialysis treatment, it is necessary to develop and apply interventions that can enhance physical performance and reduce the fear of falling.
Chronic Kidney Disease (CKD) is a condition characterized by the deterioration of kidney function, which is essential for eliminating waste products and excess fluid and regulating electrolyte balance [1]. CKD can progress to End-Stage Renal Disease (ESRD), which is marked by an irreversible reduction in kidney function [2]. Additionally, 83.6% of patients with ESRD receive hemodialysis, making it the most common form of renal replacement therapy, ahead of peritoneal dialysis and kidney transplantation [2].
While hemodialysis is a safe and effective form of renal replacement therapy, it is not without its physical complications. Patients may experience issues such as hypotension and cramps due to the rapid decrease in blood flow rate during the dialysis process. These symptoms can lead to dizziness, increasing the risk of fall-related accidents [3, 4]. In Korea, the incidence of falls among hemodialysis patients is 17.6%, with 82% of these incidents resulting in serious outcomes such as fractures or brain hemorrhages [5]. Furthermore, international studies have found that 62.5% of hemodialysis patients are at high risk of falling [6], highlighting the significance of this issue within this patient population. Although detecting falls in patients receiving outpatient hemodialysis treatment is more challenging than in hospitalized patients, it is possible to predict falls through a risk assessment that incorporates a variety of visual information [7]. Considering that 70% of falls are preventable with proper risk assessment and identification of contributing factors [8], employing reliable assessment tools like the Morse Fall Scale is crucial in recognizing characteristics associated with falls.
Along with the risk of falls, the physical performance of patients undergoing hemodialysis is one of the strongest factors influencing the occurrence of falls [9]. Ambulation and balance abilities, considered indicators of physical performance, significantly affect the incidence of falls among these patients [10]. Specifically, it has been reported that patients with ESRD on hemodialysis exhibit markedly lower physical performance and a higher incidence of falls compared to those with CKD [11]. Moreover, the restrictions on fluid and diet necessary for effective hemodialysis treatment reduce total calorie intake. This reduction can lead to muscle loss, decreased exercise capacity, and an increased risk of falls [11, 12].
Despite having adequate exercise capacity, patients undergoing hemodialysis may limit their daily activities due to a fear of falling [13]. This highlights the need for precise analysis of fall-related fear, in addition to assessing fall risk and physical performance, as part of fall prevention strategies. Previous studies have shown that a higher level of fear of falling can lead to a 175% increase in the risk of impaired mobility and a 62% increase in the risk of reduced exercise capacity development. Consequently, the fear of falling—a psychological state characterized by ongoing concerns about falling—serves as an important clinical indicator that could help prevent or mitigate physical injuries [13, 14].
Earlier studies conducted with inpatients in Korea have identified diabetes and hypertension, which are typical diseases leading to ESRD, as well as vasodilators and diuretics— key medications for patients undergoing hemodialysis— as factors associated with falls [15, 16]. However, research on patients undergoing outpatient hemodialysis treatment has been limited. International studies have reported that a variety of factors, including age, education level, and comorbidities of patients receiving outpatient hemodialysis, affect the occurrence of falls among this population [12, 17]. Nonetheless, the mean ages of patients receiving hemodialysis and the causes of ESRD differ from one country to another [10]. Unlike in Korea, where patients must visit the hospital for dialysis, some countries have actively implemented policies that allow patients to receive dialysis at home [18]. Therefore, the risk of falls among patients receiving outpatient hemodialysis treatment in Korea warrants further investigation.
Patients with ESRD who receive outpatient hemodialysis treatment at medical institutions are at an elevated risk of falls due to the inherent characteristics of their condition and the nature of their treatment. Therefore, this study aimed to identify the factors that influence this risk by examining the incidence of falls, physical performance, fear of falling, and the overall risk of falls. Additionally, the study had the goal of providing foundational data that can be used to develop effective care and management strategies to prevent fall-related accidents in patients undergoing hemodialysis.
This descriptive survey study aimed to investigate the factors contributing to the risk of falls. It examined the incidence of falls among patients undergoing hemodialysis and sought to identify the impact of physical performance and fear of falling on fall risk.
This study included patients with ESRD who regularly received outpatient hemodialysis at two medical facilities in B City and fulfilled the inclusion criteria, according to which participants were required to be adults aged 19 or older, capable of comprehending and responding to the survey questions, and have undergone hemodialysis for a minimum of 3 months. The exclusion criteria ruled out patients who had been hospitalized or undergone surgery in the preceding three months, those with impaired consciousness, or those disoriented to time, place, and person.
The sample size for the multiple linear regression analysis was calculated using G*Power 3.1.9.7. We entered a median effect size (f2) of 0.15, a statistical test power (1-β) of 80%, and 10 potential predictors, which yielded a required sample size of 118. To account for an anticipated dropout rate of 15%, we set the target sample size at 140. Following the exclusion of 8 participants due to lost questionnaires or incomplete medical records, 132 participants were included in the final analysis.
The participants' demographics, including age, gender, education level, and occupation, were assessed through a self-report questionnaire. Clinical characteristics, including the cause of ESRD, the length of time on hemodialysis (year), dialysis frequency per week and the presence of a companion during dialysis clinic visit, were also investigated.
Among the clinical characteristics, participants' Body Mass Index (BMI) was calculated using their dry weight and height as recorded in their medical records. These values were then classified according to the criteria established by the Korean Society for the Study of Obesity [19]. Comorbidities were categorized into heart diseases, vascular diseases, liver diseases, and gastrointestinal diseases, following the classifications in the annual report of the Korean Society of Nephrology [2]. Medications were assessed based on the number of doses taken daily. For physiological indicators, serum albumin, calcium, phosphorus, and intact Parathyroid Hormone (iPTH) levels were measured. These are critical clinical data for assessing bone diseases in patients undergoing hemodialysis. The guidelines for these measurements were based on literature reviews targeting Koreans and the reference ranges published by the Korean Society of Nephrology [2, 20].
Falls, as defined in this study, refer to unintentional descents to a lower level or to the ground, as reported by the patient [21]. This definition excludes falls resulting from external forces, loss of consciousness, or sudden paralysis. Data on the fall history were collected through a self-report questionnaire, which examined frequency, time, place, cause, and activity at the time of the fall.
The Short Physical Performance Battery (SPPB), a concise assessment tool developed as part of the Established Populations for Epidemiologic Studies of the Elderly (EPESE) project by the National Institute on Aging, has been utilized to evaluate physical performance and is validated for research purposes [22]. The SPPB consists of three components: standing balance, gait speed, and repeated chair stands. Each component is rated on a scale of 0 to 4, with the scores combined to yield a total score that ranges from 0 to 12. A total score of 9 or below is indicative of physical frailty. The Cronbach's α coefficient was .93 during the development phase, .83 in a study with patients undergoing hemodialysis [23], and .90 in the current study. The Cronbach's α values for the subdomains were.84 for standing balance, .80 for gait speed, and .82 for repeated chair stands.
Standing balance is evaluated by the ability to maintain a standing position in three different stances: side-by-side with both feet together, semi-tandem, and tandem, each for a duration of 10 seconds. The side-by-side and semitandem stances are rated on a scale from 0 points (for less than 10 seconds or inability to maintain the stance) to 1 point (for maintaining the stance for 10 seconds or longer). The tandem stance is scored on a three-point scale: 0 points for less than 3 seconds or inability to maintain the stance, 1 point for maintaining it from 3 seconds to less than 10 seconds, and 2 points for 10 seconds or longer.
Gait speed is measured by calculating the time it takes for a participant to walk a distance of 4 meters at their normal pace. This is done twice, and the average time is determined. Scores are assigned based on the total time taken: 4 points for less than 4.82 seconds, 3 points for 4.82 to 6.20 seconds, 2 points for 6.21 to 8.70 seconds, 1 point for more than 8.70 seconds, and 0 points if the participant is unable to perform the activity.
For repeated chair stands, the participant crosses their arms in front of their chest, then sits down on and stands up from a chair of standard height (46 cm) five times. The time taken to complete this task is recorded. Scores are assigned based on the total time taken: 4 points for 11.19 seconds or less, 3 points for 11.20 to 13.69 seconds, 2 points for 13.70 to 16.69 seconds, 1 point for more than 16.70 seconds, and 0 points if the task takes over 60 seconds or if the participant is unable to perform the activity.
To assess the fear of falls, we utilized Kim's Korean translation of the Falls Efficacy Scale-International (KFES-I), a tool originally developed by Yardley et al. [24]. This instrument is designed to measure an individual's psychological fear of falling and is validated for research use [25]. The questionnaire consists of 16 items that assess an individual's confidence in performing daily and various social activities without falling. Each item is rated on a 4-point scale: 1 point indicates no problem, 2 points indicate slight difficulty, 3 points indicate quite a bit of difficulty, and 4 points indicate very difficult. Participants with a total score above 24 points are categorized as having a fear of falls, while those with a score of 24 or below are considered to have no fear of falls. The Cronbach's α for the original tool was reported as .96 [24], while it was .97 for the Korean version (KFES-I) [26], and .96 for the version used in this study.
The fall risk was measured using the Morse Fall Scale (MFS), a tool developed to evaluate the presence of risk factors for falls among patients [27]. The MFS consists of six items, each addressing a different risk factor. The MFS criteria are as follows: a history of falling within the last 3 months (yes: 25 points, no: 0 points), a secondary diagnosis (diagnosed with diseases other than ESRD: 15 points, no additional diagnoses: 0 points), the use of ambulatory aids (none, wheelchair, or bed rest: 0 points; crutches, cane, or walker: 15 points; reliance on walls or furniture without ambulatory aids: 30 points), the presence of an intravenous injection or heparin lock (yes: 20 points, no: 0 points), gait (normal or bed rest: 0 points; able to walk with balance but weak: 10 points; poor balance and unable to walk without aids: 20 points), and mental status (oriented to own ability: 0 points; overestimates or is unaware of own ability: 15 points). The total score can range from 0 to 125 points. Individuals are categorized based on their total score: those with less than 25 points are considered low-risk, those with 25 to 50 points are moderate-risk, and those with a score above 50 points are classified as high-risk.
During the development phase of the tool, it demonstrated a sensitivity of 78%, a specificity of 83%, and a consistency between researchers with a Cohen's κ of 0.96 [27]. The Intraclass Correlation Coefficient (ICC) for the tool in this study was 0.96 (95% Confidence Interval [CI], 0.82~0.98).
The data collection period of this study was January 2 to April 23, 2022. Data were collected with the cooperation of nephrology specialists and nurse managers at two hemodialysis facilities located in B Metropolitan City.
The physical performance of participants was assessed before their hemodialysis treatment, with the researcher and an assistant directly observing in a hallway outfitted with handles on both walls. Participants who were unable to walk independently were not evaluated for physical performance. This decision was made collaboratively by the researcher and the participants to avoid any potential accidents, and their performance was recorded as immeasurable. During the hemodialysis session, participants completed a questionnaire regarding their fear of falling. If a participant found it challenging to fill out the questionnaire, the researcher would read the questions aloud, and the participant would provide their responses verbally. For clinical characteristics such as hematology test results and medication details, the researcher retrieved the most recent information from medical records and recorded it. Additionally, nurses with a minimum of 10 years of experience in the hemodialysis unit conducted fall risk assessments.
Approval for this study was granted by the Institutional Review Board of P University (PNU IRB/2021_173_HR). Following this, permission was obtained from the management of two hemodialysis centers in B Metropolitan City to recruit participants. A notice inviting participation was then posted at these centers. Individuals who voluntarily expressed interest and met the inclusion criteria were enrolled in the study. Participants were fully informed about the study's objectives, duration, and their right to withdraw at any time before signing the informed consent form. To ensure confidentiality, all collected data were assigned a unique serial number and stored on an encrypted security device, preventing the identification of personal information.
The collected data were analyzed using SPSS/WIN version 25.0 (IBM Corp., Armonk, NY, USA) at a significance level of .05. We calculated the participants' demographic and clinical characteristics, as well as the occurrence of falls, using means, standard deviations, frequencies, and percentages. Similarly, we determined the participants' physical performance, fear of falling, and fall risk using the same statistical measures. We conducted a bivariate correlation analysis to examine the relationships between the three variables, utilizing Pearson correlation coefficients. To evaluate the risk of falling based on participants' characteristics, a post-hoc analysis for categorical variables was performed using either the independent t-test or one-way analysis of variance. For continuous variables, Pearson correlation coefficients were used. Finally, hierarchical multiple linear regression analysis was conducted to identify factors influencing the risk of falling among participants.
The mean age of the participants was 61.67 years. Male participants comprised 68.2% of the study population, which was more than double the percentage of female participants (31.8%). Diabetes was the most prevalent cause of ESRD, accounting for 45.4% of cases. On average, participants had 2.44±1.38 comorbid conditions in addition to ESRD, and they took an average of 16.48±5.62 doses of medication daily. The mean length of time on dialysis among the participants was 4.43±5.65 years. With respect to key clinical indicators, 71.2% of participants maintained serum albumin levels within the recommended range. Calcium, phosphorus, and intact parathyroid levels were within the target range for 63.7%, 48.5%, and 62.1% of participants, respectively (Table 1).
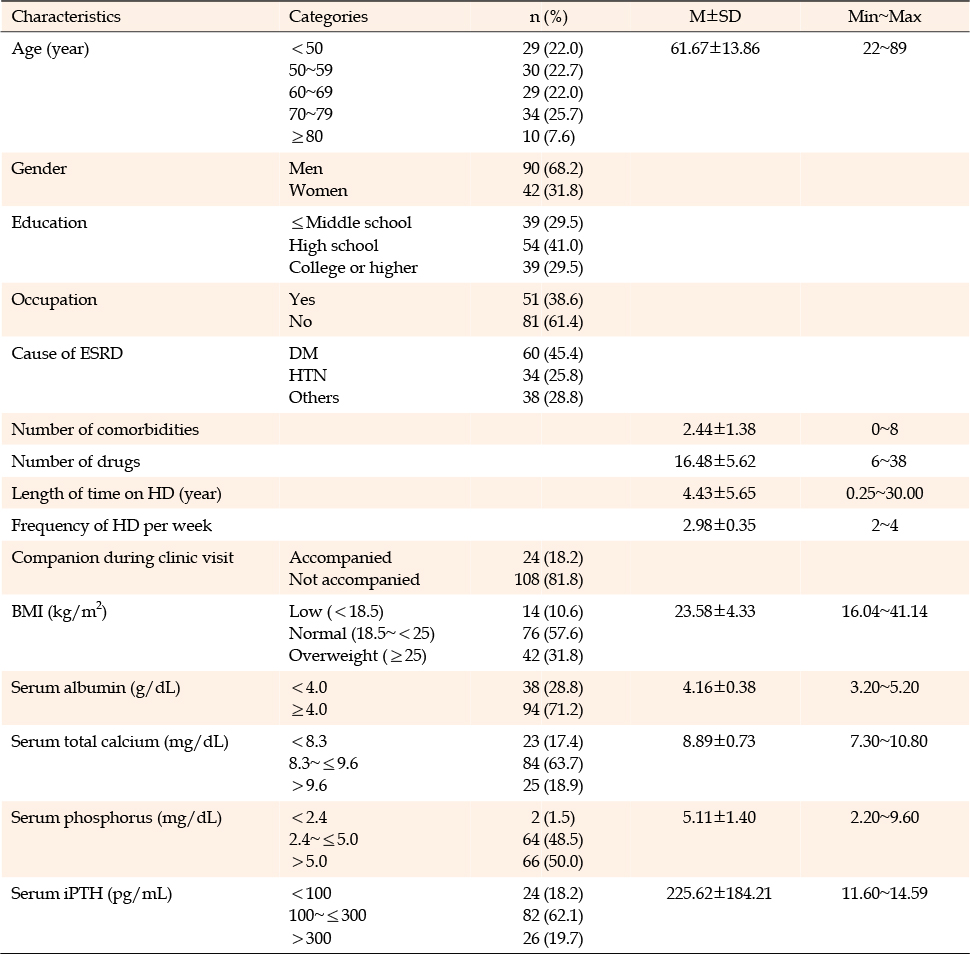
Table 1
Demographic and Clinical Characteristics (N=132)
Of the participants, 28.8% (38 individuals) reported experiencing falls in the past year. On average, they fell 1.68 times, with the highest number of falls reported by one participant being five within that year. Fall incidents (n=64) most frequently occurred outdoors (48.5%) and on days when hemodialysis treatment was not administered (56.2%) (Table 2).
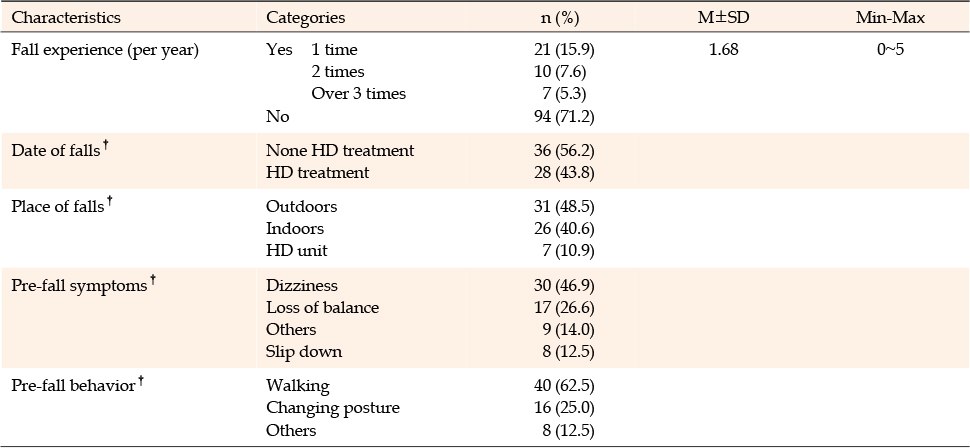
Table 2
Fall History in the Last Year (N=132)
The mean total score for physical performance among the patients was 7.89±3.55 points, with the weak group comprising 59.8% of the sample, outnumbering the nonweak group. The mean score for fear of falling was 23.18±9.36, and the majority of patients (73.5%) experienced this fear. Regarding the risk of falling, the mean score was 45.68±19.52 points. The majority of patients (68.9%) fell into the moderate-risk category, while 25.8% were classified as high-risk (Table 3).
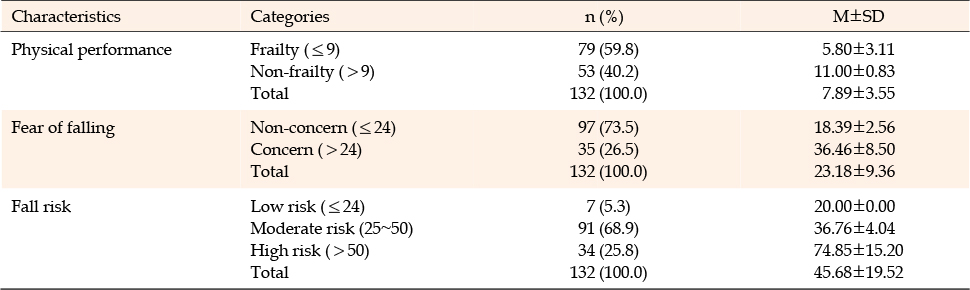
Table 3
Physical Performance, Fear of Falling, and Fall Risk (N=132)
There were significant differences in the risk of falls according to age (F=2.96, p=.007), gender (t=-3.89, p=.026), and education level (F=8.78, p<.001), among the general characteristics. The post-hoc analysis revealed that participants aged 80 and above were at a higher risk of falls than those aged less than 60 and that those who did not attend high school were at a higher risk of falls than those who attended high school.
A higher number of comorbidities (r=.36, p<.001) and a higher number of medications (r=.18, p=.045) were correlated with fall risk. Participants who were accompanied by someone while attending dialysis treatment were at a significantly higher risk of falls than those who visited by themselves (t=-5.00, p<.001). A lower serum albumin level was correlated with a higher risk of falls (t=2.44, p=.018), and those with a serum iPTH level lower than the recommended level were at a higher risk of falls than those with a serum iPTH equal to or higher than the recommended level (F=9.32, p<.001).
Lower physical performance (r=-.72, p<.001) and a greater fear of falls (r=.65, p<.001) were correlated with a higher risk of falls (Table 4).
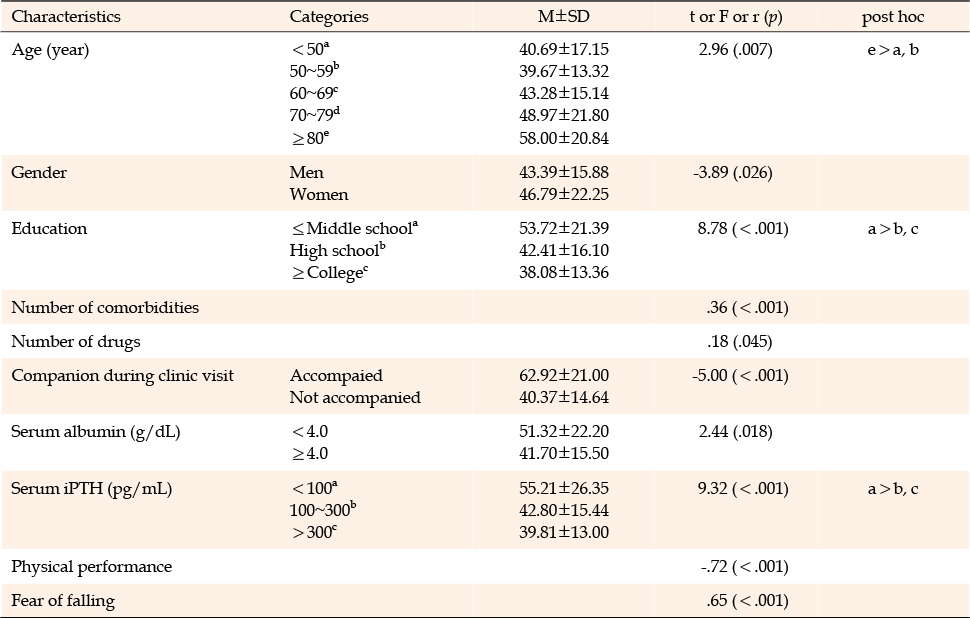
Table 4
Fall Risk according to Demographics and Clinical Characteristics (N=132)
A hierarchical multiple regression analysis was conducted to identify the primary factors influencing fall risk. The tolerance values, which ranged from 0.27 to 0.94 (all above 0.1), and the variance inflation factor values, which ranged from 1.05 to 3.65 (all below 10), indicated no issues with multicollinearity. The Durbin-Watson statistic was 1.97, close to the ideal value of 2, suggesting no autocorrelation among the residuals. Residual analysis confirmed that the assumptions of linearity, normality, and homoscedasticity were met.
Among the statistically significant variables, gender, education level, and the presence of a companion during dialysis clinic visit were included as dummy variables in the univariate analysis. Additionally, age and the number of falls within the past year were treated as continuous variables in the construction of Model I. The number of comorbidities and serum albumin levels were also included as continuous variables, while serum iPTH levels were converted into a dummy variable based on the recommended range for inclusion in Model II. Model III was then finalized by adding measures of physical performance and fear of falling.
In the final model, the following factors were identified as significantly influencing the risk of falls among hemodialysis patients: physical performance (β=-.41, p<.001), the number of falls within the past year (β=.34, p<.001), the fear of falls (β=.24, p=.017), and serum iPTH (β=.15, p=.006). These variables explained 65.4% of variance in the risk of falls, and the regression equation was statistically significant (F=22.71, p<.001) (Table 5).
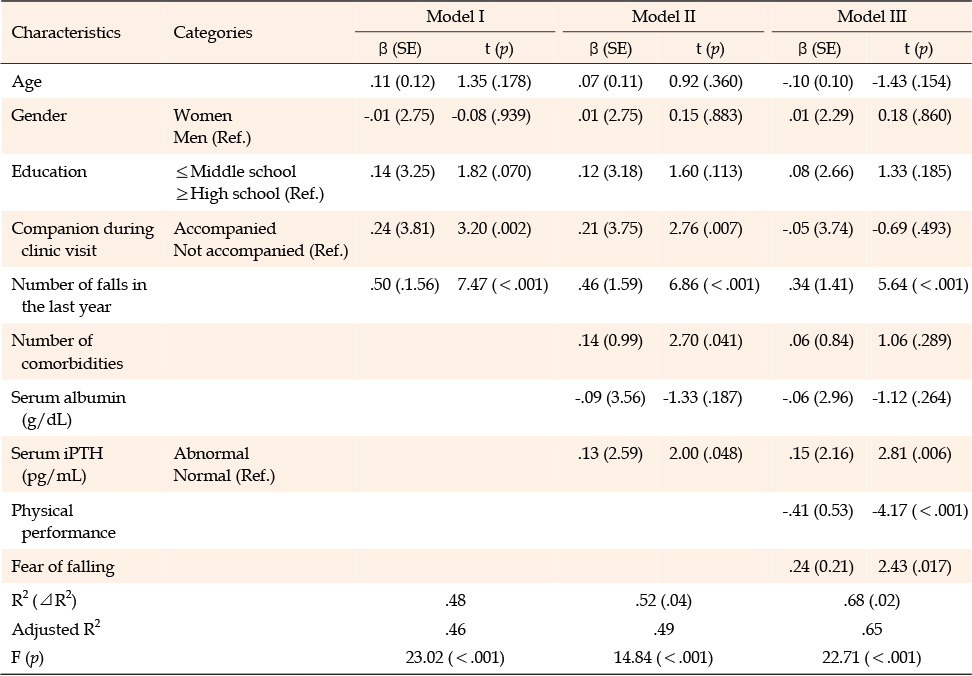
Table 5
Factors Affecting Fall Risk (N=132)
In this study, the following factors were identified as influencing fall risk among patients undergoing hemodialysis: the serum iPTH level, the fear of falls, the frequency of falls, and physical performance. iPTH is a critical hormone that aids in calcium reabsorption and phosphorus release in the kidneys, and it helps maintain calcium balance in the body by activating vitamin D [28]. Abnormal iPTH levels, either too low or too high, in hemodialysis patients may indicate disruptions in the calcium-phosphorus regulation mechanism, which can significantly affect bone formation and mineral balance [29]. Research on hemodialysis patients has shown that for every 10 pg/mL increase in iPTH, there is a 22% increase in the risk of falls. Those who experienced two or more falls had higher average iPTH levels than those who fell just once [18]. Since the serum iPTH level in patients with ESRD can be used for predicting bone diseases and preventing falls, it is important to maintain the recommended level through regular monitoring and appropriate drug therapy, including calcitriol, calcium analogues, and vitamin D analogues [2].
The mean score for fear of falls, as measured by the KFES-I, among participants in this study was 23.18 points. When categorized based on a threshold score of 24 points, 26.5% of participants were considered to have a fear of falls. This is comparable to a previous study on patients undergoing hemodialysis, which reported that 21.4% of patients had a fear of falls [30]. It is noteworthy that over 60% of elderly individuals who had a fear of falls tended to avoid activities due to this fear, leading to a decline in physical performance, including muscle atrophy. Consequently, the fear of falls may itself heighten the risk of experiencing falls [31]. A reduction in confidence in one's ability to move, stemming from this fear, proportionately increases the risk of falls. Therefore, it is anticipated that providing psychological support could help reduce the risk of falls.
This study showed that an increased frequency of falls is associated with a higher risk of falling. This finding is consistent with a previous study that identified a significant positive correlation between these two variables [32]. The majority of research on falls has concentrated on older populations [17, 32, 33]. However, while three out of seven participants who reported three or more falls in the past year were aged 80 or older, the individual with the most frequent falls was a woman in her 30s. This highlights the importance of broadening research to encompass younger patients undergoing hemodialysis. Notably, repeated falls tend to occur in those at high risk for falling. As health issues compound due to recurrent falls, physical performance deteriorates to a point where recovery may no longer be possible [33, 34]. Therefore, it is important to identify the characteristics of patients who experience repeated falls in order to prevent further incidents.
The factor most strongly correlated with predicting the risk of falls was physical performance. In our study, 59.8% of participants were classified as frailty, which is consistent with a previous study [23] that found 56.4% of patients undergoing hemodialysis were in the frail group. Falls, often caused by diminished muscular strength in these patients, can lead to serious physical injuries, including fractures and brain damage, as well as musculoskeletal disorders. Moreover, the fear of falling again can cause not only physical harm but also impair psychological function and, in some cases, result in death [11]. Exercise programs aimed at improving physical performance have been shown to reduce the risk of falls [35]. Furthermore, an international prospective cohort study found that individuals who fell had poorer gait and standing balance compared to those who did not fall [10]. Given that gait and standing balance are part of the physical performance assessments in this study, developing exercise programs to enhance these specific areas, along with providing education on them, will likely be beneficial in preventing falls.
In this study, we assessed participants' experiences of falls through a survey that relied on memory, which raises the possibility of memory bias. Therefore, it is believed that more accurate information regarding the incidence of falls could be obtained from prospective studies or by examining medical records. Moreover, community-dwelling individuals with chronic diseases who are undergoing regular outpatient treatments, such as hemodialysis, may present a different fall risk profile compared to acute inpatients. Despite this, the Morse Fall Scale, originally developed for inpatient populations, was employed in our research. This may not have accurately captured the specific characteristics of our participants. The development and implementation of a fall risk assessment tool tailored for the growing demographic of elderly patients with chronic conditions would likely improve both the validity and reliability of such assessments.
Despite these limitations, the study provides meaningful results because the participants' physical performance was directly measured by the researchers, avoiding reliance solely on subjective self-reports. Research on outpatient hemodialysis patients in Korea is scarce, despite an increasing number of cases. This study offers important insights into the prevalence and characteristics of falls among outpatients receiving hemodialysis. Understanding the factors that influence the risk of falls in patients undergoing regular outpatient hemodialysis, as identified in this study, can aid healthcare professionals in fall prevention within clinical settings.
The study found that 28.8% of participants had experienced falls in the previous year. Factors that increased the risk of falls included impaired physical function, a higher frequency of previous falls, an increased fear of falling, and serum iPTH levels that were outside the recommended range. These findings can inform strategies to reduce the risk of falls in patients undergoing hemodialysis and aid in the development of preventive measures against falls.
Based on these findings, we suggest the following steps. First, fall prevention programs that take into account the identified risk factors for falls among patients undergoing regular outpatient hemodialysis should be developed and implemented. Second, there is a need to develop tools for assessing fall risk that are specifically tailored to the unique characteristics of community-dwelling patients with chronic diseases, as opposed to inpatients. Additionally, further research that utilizes objective methods to investigate the experience of falls is recommended.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - CJ and HS-K.
Data collection - CJ.
Analysis and interpretation of the data - CJ and HS-K.
Drafting and critical revision of the manuscript - CJ and HS-K.
This article is a revision of the first author's master's thesis from Pusan National University.
 E-SUBMISSION
E-SUBMISSION