
Purpose
This study aimed to comprehensively understand the experiences of emergency nurses performing triage during the peak and plateau periods of the Coronavirus Disease 2019 (COVID-19) pandemic over the past two years.
Methods: Twenty triage nurses from three emergency medical centers were recruited through purposive and snowball sampling. Data collection occurred from February to May 2022 via focus group interviews and was analyzed using qualitative content analysis.
Results: The experiences of emergency nurses in triage revealed four themes: "changes in priorities due to infectious diseases", "barriers to tirage", "the emotional burden experienced by triage nurses", and "the journey toward growth". The pandemic heightened the focus on infection screening in triage. Triage nurses faced numerous challenges concerning their own safety and that of their patients and encountered difficulties in performing triage. Nonetheless, these experiences provided them with opportunities for professional growth.
Conclusion: The experiences of nurses performing triage during the peak and plateau periods of the COVID-19 pandemic provide valuable insights for future preparedness and coping strategies in the face of similar infectious disease outbreaks. It is necessary to establish integrated triage guidelines for patient safety, develop operations manuals for triage, implement policies on staffing standards, and provide mental health support for triage nurses during pandemics.
This study aimed to comprehensively understand the experiences of emergency nurses performing triage during the peak and plateau periods of the Coronavirus Disease 2019 (COVID-19) pandemic over the past two years.
Twenty triage nurses from three emergency medical centers were recruited through purposive and snowball sampling. Data collection occurred from February to May 2022 via focus group interviews and was analyzed using qualitative content analysis.
The experiences of emergency nurses in triage revealed four themes: "changes in priorities due to infectious diseases", "barriers to tirage", "the emotional burden experienced by triage nurses", and "the journey toward growth". The pandemic heightened the focus on infection screening in triage. Triage nurses faced numerous challenges concerning their own safety and that of their patients and encountered difficulties in performing triage. Nonetheless, these experiences provided them with opportunities for professional growth.
The experiences of nurses performing triage during the peak and plateau periods of the COVID-19 pandemic provide valuable insights for future preparedness and coping strategies in the face of similar infectious disease outbreaks. It is necessary to establish integrated triage guidelines for patient safety, develop operations manuals for triage, implement policies on staffing standards, and provide mental health support for triage nurses during pandemics.
The Coronavirus Disease 2019 (COVID-19) pandemic has significantly impacted people worldwide [1] and has placed considerable strain on the medical system [2]. In the midst of this public health crisis, the Emergency Department (ED) plays a critical role as the hospital's frontline defense [3, 4]. Triage, a system implemented within the ED, is designed to evaluate patients quickly and effectively, ensuring that they receive prompt and efficient treatment [5]. This system is crucial for maintaining the safety and efficiency of treatment procedures in emergency departments [6]. In response to the COVID-19 outbreak, nearly all EDs established protocols for screening, testing, and managing patients with suspected COVID-19 infections [7], including in the triage process [8].
Throughout the world, triage is mainly done by nurses [9], who account for approximately 91.9% of triage performers in South Korea [10]. These triage nurses are the frontline medical staff who first assess patients arriving at the ED and establish the priority for treatment [11]. Amid the COVID-19 pandemic, triage nurses have taken on the role of gatekeepers, tasked with identifying potentially infected individuals through evaluation criteria [12]. Nevertheless, accurately categorizing all patients, including those with COVID-19, within a constrained timeframe has proven to be a formidable challenge [13]. The introduction of additional protocols and guidelines that require strict adherence has further increased their job stress [1, 14].
This gatekeeping role led to "triage fatigue" among nurses, stemming from inadequate medical resources, limited space, and fluctuations in patient flow, which in turn caused more stress than that experienced by other ED staff [15]. Job-related stress has a detrimental impact on nurses' occupational mental health [16]. Prolonged exposure to such stressors can harm individual health and impair cognitive decision-making processes, which may, in turn, affect patient outcomes [17]. The increased workload and pressure brought on by the pandemic have led to physical and psychological burnout among triage nurses, influencing their ability to classify patients effectively [9, 10].
Previous studies have primarily focused on the experiences and challenges faced by triage nurses, as well as the impact on their mental health during the initial stages of the COVID-19 pandemic [9, 18]. However, as the COVID-19 pandemic has now persisted for over three years, there is a pressing need for further research. This research should explore how the prolonged nature of the pandemic has altered the triage environment, identify the problems that have arisen in the triage process, and propose effective solutions. In Korea, there have been six distinct epidemic periods due to COVID-19. Notably, the fifth epidemic period (January 30 to June 25, 2022), which was characterized by the emergence of the Omicron variant, saw the highest number of confirmed cases, with a rate of 35,141.1 per 100,000 population [19]. Therefore, studies investigating the experiences of triage nurses during the peak and subsequent plateau of the COVID-19 pandemic, especially in the context of the spread of the Omicron variant, are needed. Such research can help to identify the evolving challenges faced by these healthcare professionals and provide reliable solutions for managing the ongoing situation.
Thus, this study aimed to gain a comprehensive understanding of emergency nurses' experiences with triage tasks during the COVID-19 pandemic, particularly between the peak and plateau phases over the past two years. It also sought to identify various issues associated with the evolving work environment.
This qualitative study involved the use of content analysis after conducting a Focus Group Interview (FGI).
The inclusion criteria specified emergency nurses who held a Korean Triage and Acuity Scale (KTAS) certification and had at least one year of triage experience during the COVID-19 pandemic. Twenty nurses from three emergency medical centers were recruited through purposeful and snowball sampling methods. These participants were employed in two EDs of tertiary medical centers and one ED of a general hospital located in the Seoul and Gyeonggi-do metropolitan areas of South Korea. Hospital A has a 47-bed ED and handles approximately 75,000 emergency patients each year. Hospital B contains a 44-bed ED and manages the care of 35,000 emergency patients annually, while Hospital C, with a 24-bed ED, receives 40,000 emergency patients per year. Nurses who were able to share their experiences were recommended by their colleagues at these hospitals. The researcher reached out to potential participants with a brief overview of the study via email or messenger to confirm their willingness to participate. Twenty nurses agreed to take part in the study and remained actively involved throughout the research process.
This study was conducted after approval from the Institutional Review Board (IRB) (No.: DMC 2022-01-003-001). Participants received brief information about the study from the researcher before participating and gave voluntary consent to participate. Before the interview, all participants signed a consent form, which detailed the study's purpose, procedures, data storage, disposal methods, and the fact that the interview would be recorded. The form also stated that participants could withdraw from the study at any time. As a token of appreciation, participants received a gift certificate after the interview. To ensure privacy and confidentiality, all collected data were anonymized.
Data were collected through FGIs to facilitate participant interaction and in-depth discussions [20] from February 17 to May 11, 2022. This period spanned the peak and plateau phases of the COVID-19 pandemic in Korea. Four focus groups were established, each consisting of nurses working at the same hospital. The groups comprised five, six, five, and four participants, respectively. The interviews took place in a quiet seminar room within the hospital or a study cafe, chosen for the convenience and scheduling preferences of the participants. The average duration of each interview was approximately 60~70 minutes. A researcher, trained in qualitative research methods through graduate school courses, conducted the FGIs using a semi-structured questionnaire. The interview questions explored experiences such as "What have you encountered while working in triage during the last two years of the COVID-19 pandemic?", "Have there been any changes in the triage process since the onset of COVID-19?", "In your opinion, how has the COVID-19 pandemic impacted triage procedures?", and "What does your work experience over the past two years mean to you?". All interviews were audio-recorded using the CLOVA Note app (Naver Co., Korea) after obtaining consent from the participants at the beginning of each session. The researcher ensured an accurate understanding of the participants' statements and observed non-verbal cues, including facial expressions, hand gestures, and intonation, which were noted in observation records. Transcriptions of the interviews were completed promptly, within two to three days following each session.
The collected data were analyzed using Hsieh and Shannon's conventional content analysis method [21]. Initially, the overall meaning was discerned through multiple readings of the transcribed data. Subsequently, the content of the interviews was thoroughly examined, with significant words, phrases, and sentences being identified, highlighted, and organized into themes. These themes were then delineated and grouped by assessing the similarities and distinctions among the categorized content. Ultimately, the experience of performing triage tasks during the COVID-19 pandemic was articulated using more nuanced wording, derived from the relationships between the identified themes.
This study considered the following criteria defined by Sandelowski [22] to establish rigor. To establish credibility, the researcher presented the analysis results to the participants for validation, ensuring that the reported contents and experiences were accurate and that the identified themes and examples were appropriate for the research findings. For auditability, the study's objectives, participant selection criteria and methods, data collection procedures, and approaches to data analysis and interpretation were systematically recorded. To achieve fittingness, data collection continued until theoretical saturation was attained, at which point no additional novel information emerged from the participants' statements. Regarding conformability, the researcher endeavored to reduce bias and preserve objectivity by directly querying participants about any ambiguities during the interviews to clarify their intended meanings.
In this study, 20 nurses who performed triage tasks in the ED participated (Table 1). Analysis of the emergency nurses' experiences with triage during the COVID-19 pandemic yielded four themes, 10 sub-themes, and 27 codes from 457 meaningful sentences. The four derived themes were "changes in priorities due to infectious diseases", "barriers to triage", "the emotional burden experienced by triage nurses", and "the journey toward growth" (Figure 1).
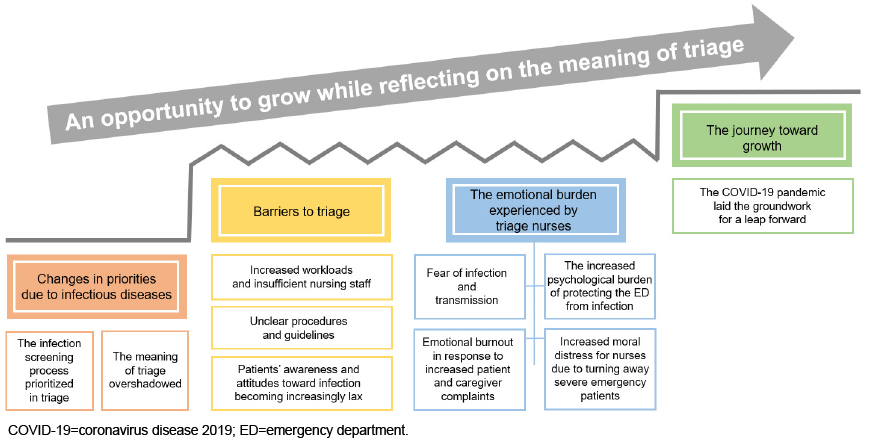
Figure 1
The experiences of emergency nurses performing COVID-19 triage.
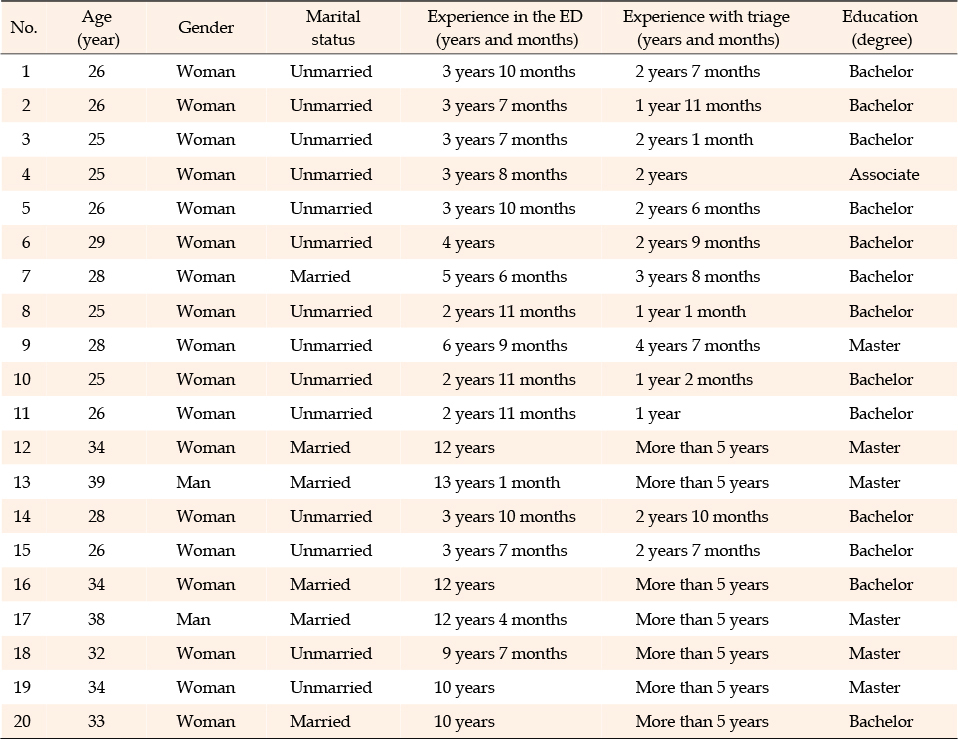
Table 1
General Characteristics of the Participants (N=20)
COVID-19 made it essential to determine whether preemptive isolation should be carried out through an infection screening process when performing triage. The priorities typically applied in triage changed as the infection screening process became critical. Participants tried to collected comprehensive patient information by asking detailed questions and made a habit of wearing Personal Protective Equipment (PPE) during triage. They viewed this as an opportunity to recognize the importance of the infection screening process and PPE.
I try to understand the patient's history in detail. And I try to better understand the patient's condition by conducting a more detailed history taking. (Participant 3)
Before COVID-19, unless there were visible indicators of infection, we didn't prioritize infection concerns during triage. But, now, the first question we ask is whether the patient has respiratory symptoms, and we take preemptive action. (Participant 8)
COVID-19 has lasted over two years, and we habitually wear PPE. (Participant 17)
Triage is a system that prioritizes emergency patients based on severity and urgency to ensure rapid medical examination and treatment. However, due to COVID-19, if there was no immediate quarantine space available, emergency patients often had to wait outside until the risk of infection could be ruled out. As the ability to provide timely treatment to severe emergency patients was reduced, participants felt that the true meaning of triage and their role had become diminished.
Before COVID-19, if a patient was classified as severe by a triage nurse, they would be quickly assigned a bed and receive prompt treatment. However, if a patient exhibits suspected COVID-19 symptoms, X-ray tests are necessary even for emergency cases, and treatment may be delayed depending on the availability of isolation rooms. So, it is challenging to treat emergency patients. (Participant 16)
Due to COVID-19, the information required to be confirmed with the patient and the procedures that must be carried out during triage have increased. Furthermore, the process of donning and doffing PPE has extended the time needed for triage with each patient. Participants reported feeling pressured by the heightened workload during triage.
During triage, we also need to conduct infection screening to determine whether this patient requires isolation. Triage takes longer because PPE must be changed after attending to a suspected COVID-19 patient. We have more work and many things to pay attention to, so it is harder than before. (Participant 3)
The triage nurse has to decide whether to isolate the patient, check if there is room in the negative pressure isolation room, and, if not, send the patient to the screening clinic or return them. The triage nurse has to manage this task alone. This left us with an overwhelming workload. (Participant 18)
During the middle phase of the pandemic, basic guidelines were established. However, as these guidelines were repeatedly revised in response to emerging new mutations, some participants reported feeling confused and struggled with the frequent changes. Participants expressed skepticism about the establishment of a transparent infection control system up to the time of the study.
I have been working for almost two years so far, but I don't think an exact infection control system has been established. I think it's still a little hard because new mutations develop, and new contents are added and changed every time. (Participant 8)
In the early stages of the COVID-19 outbreak, patients were cooperative when responding to questions during history taking. However, as time progressed, it appeared to participants that patients had become indifferent to infectious diseases. More recently, discrepancies between government and hospital infection control guidelines posed challenges for participants during the triage process, as they must ensure that both patients and their caregivers comprehend these guidelines.
In the beginning, patients responded cooperatively when asking questions. However, I think I started to get rough answers as I entered the middle stages [of the pandemic]. The patients seem to be growing indifferent, and their awareness seems to have disappeared. (Participant 14)
Patients say, "The country doesn't do that, so why are you doing it?". Whenever that happens, I explain that this is a hospital and that the infection screening process needs to be done based on a risk assessment. While some people agree with this, others do not, making this a difficult point now. (Participant 15)
In the early stages of the COVID-19 outbreak, the participants performed triage with the fear of contracting an unfamiliar infectious disease and potentially infecting their families. However, over time, understanding of the virus's transmission pathways and medical treatments improved, and the development of vaccines helped to alleviate these fears over time.
In the beginning, I was terrified that I could be infected. It felt like a terrible disease at first. Now there are vaccines and treatments, and the symptoms are mild, so I'm not very afraid anymore. (Participant 5)
I have a family, so I'm worried that if I get infected, my children will get infected. (Participant 13)
Due to COVID-19, participants took on greater responsibility as gatekeepers to prevent the spread of infection in ED during triage. From the outset, they were tasked with the critical role of screening patients for infection. Concurrently, they handled the burden of ensuring that no infected patients were missed during the triage process, which could result in the transmission of the virus within the ED.
I'm the one who determines whether a patient enters the emergency room, so I feel a lot of pressure about whether an infected patient would make it inside if I miss something… I feel like I have become more responsible. (Participant 7)
Participants provided patients and their caregivers with thorough explanations of the changes to the triage process due to COVID-19, the challenges of treatment without an isolation room, and the anticipated waiting times. Despite these thorough explanations, patients and caregivers expressed complaints and dissatisfaction to the participants, with some patients even making outright threats. As a result, participants experienced heightened emotional distress due to the aggressive responses from patients and caregivers.
It's emotionally exhausting. If I don't explain why they are doing this, why they have to wait, why they are following this procedure, I will later face further complaints and dissatisfaction. (Participant 13)
Whenever a patient behaves violently and curses at us, asking why they have to wait so long. Whenever that happens, we get emotionally exhausted. (Participant 15)
Moral distress refers to the adverse emotional responses or reactions experienced by nurses who recognize the morally appropriate action to take but are constrained from doing so by obstacles such as institutional structures and values [23]. During the triage process after the COVID-19 outbreak, participants faced considerable difficulties when they were forced to send home or transfer emergency patients requiring immediate care in an isolation room due to infection risks. With the increase in COVID-19 cases, such situations have become more common. Consequently, participants reported experiencing moral distress and struggling with feelings of anxiety, sorrow, compassion, and guilt.
Recently, with the rapid increase in the number of COVID-19 patients, we had to send back emergency patients requiring immediate treatment to other hospitals due to the lack of quarantine space. So I felt very worried as I sent the patient back. We felt great guilt when that happened. I think this was the hardest part. (Participant 18)
Reflecting on their journey over the past two years, the participants faced the challenge of safeguarding the ED against the new infectious disease amidst physical and psychological burnout, as well as moral distress, in a tumultuous environment. In the initial phase of the outbreak, they were beset by negative emotions. Yet, as they navigated and persevered through the evolving work landscape brought on by COVID-19, they grew professionally. This period also provided them with an opportunity to reflect on their role as a triage nurse.
When I look back on it, I don't think I used to perform triage as meticulously as I do now. The role of screening emergency patients and isolating and managing suspected COVID-19 patients was very difficult, but I think it'll remain a good memory. (Participant 10)
Through the pandemic, we learned to cope with the infection situation. It was a difficult time, but it became an opportunity for us to grow. (Participant 20)
This study comprehensively explored emergency nurses' experiences with triage work during the COVID-19 pandemic over the past two years. The data revealed four themes that encapsulate the physical and psychological challenges encountered during the triage process.
The first theme identified was "changes in priorities due to infectious diseases". Most participants agreed that infection screening became a priority in triage due to COVID-19, causing the basic triage process to be somewhat overshadowed. These shifts in triage priorities were inevitable and had both positive and negative impacts on patient safety. On one hand, the infection screening process was acknowledged as a critical component of triage to enhance patient safety. The Middle East Respiratory Syndrome (MERS) outbreak in Korea led to improvements in infection management, such as the establishment of a screening system [24]. However, once the MERS crisis subsided, medical staff's vigilance towards stringent infection control measures gradually diminished. Therefore, it is imperative to maintain ongoing preparedness for infection management, even after the current pandemic has been overcome, to ensure readiness for future infectious disease scenarios. On the other hand, the COVID-19 pandemic has led to the saturation of isolation beds and overcrowding in ED, with many patients experiencing deterioration while awaiting a bed [25]. The study also highlighted delays and restrictions in the timely treatment of emergency patients with high-severity conditions. Such medical delays pose significant risks to patient safety. It is essential to find a balance between meeting the urgent needs of patients and sustaining efforts to control the spread of infection. Consequently, there is a need to develop guidelines that prioritize treatment while also emphasizing infection prevention and control measures.
The second theme was "barriers that make the triage process difficult". These barriers emerged as participants grappled with increased workloads and insufficient nursing staff, unclear procedures and guidelines, and patients' indifferent attitudes. The increased workloads and shortage of nursing staff, which have been well-documented [26, 27], were exacerbated by the COVID-19 pandemic. This heavy workload led to physical and mental exhaustion, as well as task burnout among participants, which in turn impacted the quality and efficiency of triage [9]. To address this, the government should implement flexible staffing standards during a pandemic to ensure that medical institutions can adequately staff their nursing teams. In addition, following the outbreak of COVID-19, EDs in Korea quickly adapted their response to infectious diseases based on existing guidelines [28]. However, due to the unique characteristics of COVID-19, which differ from those of MERS [29], procedures were frequently revised, leading to confusion among the participants. The indifference of patients towards the triage process further complicates the situation for COVID-19 triage. When medical professionals have confidence in institutional protocols, it can help reduce stress levels and boost motivation [30]. Therefore, it is crucial for hospitals to develop multiple versions of a systematic infection response system that not only protects ED nurses by clarifying their roles but also secures patient cooperation.
The third theme was "the emotional burden that triage nurses undergo during triage". At the onset of the pandemic, through its peak and subsequent plateau, participants have consistently reported psychological distress stemming from concerns about infection, increased responsibilities, and emotional exhaustion. Echoing findings from previous studies [9, 18], the nurses in this study expressed worry about the possibility of contracting the disease themselves or transmitting it to their families due to their exposure to patients with COVID-19. They also faced significant pressure to prevent the spread of infection within the ED and coped with emotional exhaustion as a result of managing complaints from patients and their caregivers. The pandemic's challenging work conditions presented both direct and indirect risks to the participants' safety. Nurse managers must recognize these difficult work environments, proactively seek ways to improve them, and provide emotional support to triage nurses. During the peak and plateau phases of the COVID-19 pandemic, the influx of patients to the ED created challenges in promptly attending to those with urgent needs. Nurses experienced moral distress when they had to turn away emergency patients due to a lack of isolation space. Healthcare professionals, especially nurses, faced significant psychological and moral distress during the pandemic, with nurses being more vulnerable than other healthcare providers [31, 32]. Prioritizing the mental health of nurses is essential, as it impacts their own well-being, patient care outcomes, and the healthcare system's capacity to handle infectious diseases [26]. At a specialized coronavirus hospital in Korea, the Resilience through Individual and Systematic Empathy (RISE) program was established to strengthen the resilience of staff members [33]. This program successfully reduced employees' stress levels by continuously managing psychological well-being, offering targeted psychological support to high-risk individuals, and providing relaxation activities such as healing concerts and stress-relief meditation [33]. Similarly, hospitals in China implemented psychological evaluations and provided counseling services and training through psychological support programs, leading to a decrease in depression and anxiety among medical staff [34]. Therefore, it is critical for healthcare institutions to implement Employee Assistance Programs (EAPs) to help alleviate the buildup of negative emotions among nursing staff.
The fourth theme was "the journey for growth". Consistent with the findings of Sun et al. [35], our study showed that participants initially experienced negative emotions while grappling with numerous challenges during the early stages of the COVID-19 pandemic. However, as they persevered and developed coping strategies, these negative feelings gradually gave way to positive emotions, including a sense of progress and personal growth. Many nurses reported experiencing significant physical and mental stress in their response to COVID-19, yet they also acknowledged a concurrent sense of pride and accomplishment [36]. The personal growth of the participants has the potential to enhance their professional competence and self-esteem, which, in turn, can have a direct and positive impact on patient safety and health.
The generalizability of this study's findings to other regions and countries is limited, as it was conducted only among nurses working in South Korea. Nevertheless, the sample may be representative of triage nurses in Korea, despite the use of purposive and snowball sampling methods, because the participants were employed in hospitals located in metropolitan areas and had more than two years of career experience. The study is significant in that it has implications for COVID-19 triage work based on the perspectives and experiences of triage nurses during the pandemic.
From the onset of the pandemic to its peak and subsequent plateau, participants have faced ongoing physical and psychological issues stemming from the fear of infection, increased workloads, and emotional exhaustion. During the peak and plateau of the pandemic, the influx of patients to the ED created difficulties in providing timely care to those in urgent need. Despite encountering obstacles related to their work environment during the triage process, participants persevered in their efforts to differentiate between urgent and non-urgent patients and to safeguard the emergency department as the frontline defense against the pandemic. The peak and plateau periods of COVID-19 represented a period of professional growth for triage nurses. The insights gained from nurses' experiences during COVID-19 triage offer valuable lessons for managing and preparing for similar challenges in future infectious disease outbreaks. First, it is essential to develop integrated guidelines or protocols that can be adapted to changing situations to ensure the safety of critically ill patients. Second, the creation of operational manuals for patient triage during an infectious disease emergency is imperative. Third, the government should implement policies for staffing standards during a pandemic, enabling medical institutions to hire additional staff and ensure proper triage staffing levels. Fourth, nursing organizations should establish an Employee Assistance Program (EAP) to support the mental health and well-being of triage nurses during a pandemic. Based on the findings of this study, we propose further research to develop an enhanced strategy for future responses to infectious diseases by creating integrated triage guidelines and establishing a program to improve nurses' mental health.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - HY and YY.
Data collection - HY.
Data analysis & Interpretation - HY.
Drafting & Revision of the manuscript - HY and YY.
 E-SUBMISSION
E-SUBMISSION