
Purpose
Patients with hepatocellular carcinoma may experience poor sleep quality following Transarterial Chemoembolization (TACE). This study aimed to identify factors influencing sleep quality in patients undergoing transarterial chemoembolization.
Methods
The study participants comprised 49 patients who underwent TACE and 45 nurses who cared for them. Patient data were collected through a face-to-face survey before and after TACE, as well as a review of electronic medical records. Data from nurses were collected using an online survey.
Results
The mean sleep quality score of patients with hepatocellular carcinoma undergoing TACE was 5.04±1.76. Sleep quality was negatively correlated with the number of antipyretics used (r=-.31, p=.029), anxiety (r=-.40, p=.004), postembolization syndrome (r=-.30, p=.034), and fatigue (r=-.63, p<.001), and positively correlated with the nurse’s perception of patient’s fatigue (r=.45, p=.001). In multiple regression analysis, fatigue (β=-.47, p=.001) and the number of antipyretics used (β=-.33, p=.005) explained 43.5% of the variance in patients’ sleep quality.
Conclusion
The sleep quality of patients undergoing TACE was found to be relatively low. Fatigue affects sleep quality, with more fatigued patients exhibiting poorer sleep quality. Therefore, nurses must pay attention to patient fatigue and anxiety and provide more comfortable nursing care.
Patients with hepatocellular carcinoma may experience poor sleep quality following Transarterial Chemoembolization (TACE). This study aimed to identify factors influencing sleep quality in patients undergoing transarterial chemoembolization.
The study participants comprised 49 patients who underwent TACE and 45 nurses who cared for them. Patient data were collected through a face-to-face survey before and after TACE, as well as a review of electronic medical records. Data from nurses were collected using an online survey.
The mean sleep quality score of patients with hepatocellular carcinoma undergoing TACE was 5.04±1.76. Sleep quality was negatively correlated with the number of antipyretics used (r=-.31, p=.029), anxiety (r=-.40, p=.004), postembolization syndrome (r=-.30, p=.034), and fatigue (r=-.63, p<.001), and positively correlated with the nurse’s perception of patient’s fatigue (r=.45, p=.001). In multiple regression analysis, fatigue (β=-.47, p=.001) and the number of antipyretics used (β=-.33, p=.005) explained 43.5% of the variance in patients’ sleep quality.
The sleep quality of patients undergoing TACE was found to be relatively low. Fatigue affects sleep quality, with more fatigued patients exhibiting poorer sleep quality. Therefore, nurses must pay attention to patient fatigue and anxiety and provide more comfortable nursing care.
Hepatocellular Carcinoma (HCC) is the third leading cause of mortality worldwide [1]. The challenging nature of HCC, characterized by compromised liver function and extensive tumor involvement, renders Transarterial Chemoembolization (TACE) the preferred treatment option over surgery. TACE is a two-step process: initially, one or more chemotherapeutic agents are emulsified in a viscous carrier such as lipiodol; then, embolic agents are introduced into the artery that supplies the tumor [2]. While TACE effectively limits tumor cell growth and improves survival rates, its success depends on regular monitoring and repeated interventions [3]. A significant side effect of TACE is Postembolization Syndrome (PES), which includes symptoms such as abdominal pain, nausea, vomiting, and fever, arising from mechanisms different from those associated with chemotherapy [2].
PES frequently induces disruptions in daily life that are difficult to alleviate, including fatigue, poor sleep quality, and activity impairment [4]. PES typically appears 1 to 3 days after TACE, but sleep disturbances can occur both immediately after TACE and last until 2 weeks afterward [3]. PES is a physical symptom, and poor sleep quality is both a physical and psychological symptom that interferes with daily life due to PES [5]. Improving sleep quality is an important strategy to improve overall patient comfort. Poor sleep quality encompasses various aspects, including difficulty falling asleep, night-time awakenings, short sleep duration, and shallow sleep [6], all of which constitute both physical and psychological health problems. Many patients undergoing TACE have also reported poor sleep quality [3]. Additionally, they exhibit a pattern of symptoms similar to those observed in patients receiving chemotherapy, including elevated levels of depression, anxiety, fatigue, and low levels of energy and concentration [7]. While 89.3% of patients with HCC [8] and the majority of those undergoing TACE experience frequent poor sleep quality [9], this is not considered life-threatening due to its short duration and mild severity [3].
Multiple factors, including clinical characteristics, therapeutic factors, and health status, influence sleep quality in patients undergoing chemotherapy. The clinical characteristics that influence PES include serum albumin and bilirubin levels [10]. Moreover, therapeutic regimens employed in the TACE procedure or in the treatment of patients with PES affect sleep quality. High doses of lipiodol and doxorubicin can result in severe PES, and PES and sleep disorders share common risk factors and symptoms [8]. The use of analgesics for pain management can induce daytime drowsiness and nocturnal sleep disturbances [11]. Chemotherapy-induced or postoperative symptoms have been found to disrupt nocturnal sleep [12], and the use of antiemetics and antipyretics has been shown to have an indirect impact on the status of nausea/vomiting and fever, respectively. Furthermore, antiemetics combined with analgesics reduce effective sleep [13]. The psychological status of the patient, including the presence of depression and anxiety, has also been reported to be associated with sleep quality [14]. Furthermore, physical health status, including PES, can influence sleep quality. Fatigue has been recognized as both a cause and a consequence of impaired sleep quality. However, a recent study reported that objective sleep measures were not related to general fatigue, and that mental fatigue resulted in reduced subjective sleep quality [15]. Because patients undergoing TACE may feel mental fatigue due to anxiety and depression, fatigue may be a relevant factor influencing sleep quality.
Based on the conceptual model of perceived symptoms and comfort care grounded in comfort care theory, the role of nurses in providing comfort care is a critical variable [16]. Comfort care encompasses nursing activities that address the physical, psychological, social, and environmental needs of patients during stressful situations [17]. Nurses who care for patients undergoing chemotherapy must provide comprehensive care, including continuous comfort, once specific symptoms are identified [9]. Assisting patients in overcoming stress-inducing conditions, such as poor sleep quality, is an essential aspect of nursing care [17]. For instance, environmental factors such as lighting and noise significantly contribute to nursing care and can impact sleep quality. The degree of symptom awareness among nurses can influence the care provided and help reduce symptoms; however, patients undergoing TACE often report symptoms passively, believing they can endure the pain [8], which poses challenges in delivering comfort care. Interestingly, nurses caring for patients undergoing TACE were found to have lower awareness of sleep quality issues than the patients themselves and provided less physical, psychological, and environmental care [18]. Both patient characteristics and nurse awareness were identified as significant factors in enhancing sleep quality, though further research is needed [16]. Therefore, this study aimed to assess the symptoms experienced by patients and nurses' perceptions of these symptoms, and to identify the factors influencing sleep quality in patients undergoing TACE.
This study employed a cross-sectional design.
There were two groups of participants: patients and nurses. After undergoing TACE, patients were admitted to a tertiary hospital in a metropolitan city in South Korea. The inclusion criteria for patients were as follows: 1) age ≥ 19 years and 2) consent to participate in this study. The exclusion criteria included additional treatments such as radiofrequency ablation or sedation post-procedure, and missing data from electronic medical records. The inclusion criteria for nurses were as follows: a) having cared for the participating patients for more than three months, b) providing direct care to these patients, and c) voluntarily agreeing to participate in this study. Nurses who were on long-term vacation or sick leave for more than a week were excluded. The total number of staff nurses from three gastrointestinal wards was 62 (eligible nurses). Of these, 17 chose not to participate in the survey, leaving 45 nurses who completed the survey and whose data were included in the analysis (Figure 1).
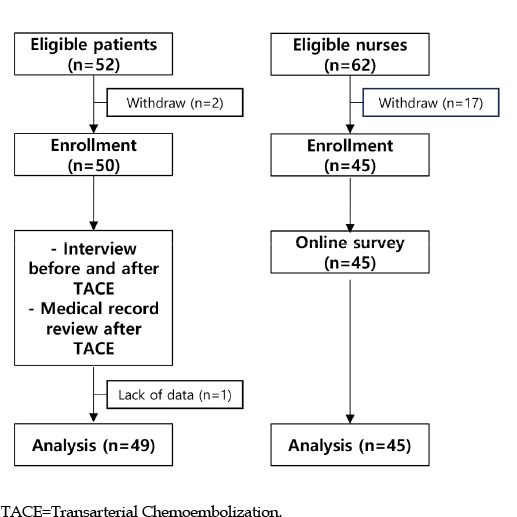
Figure 1
Flow chart of the study.
The sample size for the multiple linear regression analysis was determined using Cohen's rule for effect estimation. This calculation considers several factors: the effect size, the number of predictors, the desired power, and the significance criterion. We adopted large effect sizes (γ=0.30~0.45) from a previous study [19], a two-tailed Significance level of .05, a power of .80, and nine variables. Although 19 potential variables were identified, we hypothesized that approximately nine would be significant, based on findings from previous studies [2, 3, 5, 8]; however, these studies did not consistently identify factors affecting sleep quality after TACE. Therefore, the required sample size was estimated to be between 44 and 49 patients. After excluding three patients from the initial group of 52 due to withdrawals and non-responses, 49 participants were included in the final analysis. Post-data collection, the power was confirmed to be adequate at .99, with five predictors, 49 participants, and an R2 value of 0.435.
Seven demographic factors were recorded: age, gender, marital status, religion, occupation, smoking status, and drinking status. Additionally, 11 therapeutic characteristics were evaluated. Before TACE, laboratory data including levels of albumin, bilirubin, Aspartate Transaminase (AST), Alanine Transaminase (ALT), the international normalized ratio, and C-reactive protein were collected. The quantities of lipiodol and doxorubicin, as well as the number of medications used, including analgesics, antiemetics, and antipyretics, were also documented. Patients undergoing TACE typically spent one night in the hospital, during which their medication status was recorded. The dosages of lipiodol and doxorubicin used in the TACE procedure were adjusted based on the patient's status and were carefully documented. Medications were classified as analgesics, antiemetics, or antipyretics according to the patients’ symptoms as noted in the nursing records. The number of additional prescriptions, excluding routine general analgesic prescriptions, was calculated.
Anxiety and depression levels were assessed using specific tools. The Generalized Anxiety Disorder 2-item (GAD-2) questionnaire [20] was utilized to evaluate anxiety. This questionnaire includes two items that reflect the core criteria from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV). Patients rated each item on a 0- to 3-point Likert scale, ranging from "absolutely disagree" (coded as 0) to "absolutely agree" (coded as 3). Cronbach’s α for this scale was .95. To assess depression, the Patient Health Questionnaire-2 (PHQ-2) [21] was used. This tool focuses solely on depressive mood and apathy, which are also components of the PHQ-9. The Korean version of the PHQ-2 [22] had previously been evaluated using a 0- to 3-point Likert scale, and we adopted the same scale for consistency. Higher scores on this scale indicate higher levels of depression. Cronbach’s α for this measure was .80.
The levels of PES, fatigue severity, and sleep quality were assessed. To determine the level of PES, patients were asked if they had experienced abdominal pain, nausea, vomiting, and fever following TACE, as outlined in a previous study [3]. An 11-point Numeric Rating Scale (NRS) was employed, where "no symptoms" was scored as 0 and "very symptomatic" as 10. The cumulative score represented the PES level, with higher scores indicating more severe symptoms. To evaluate fatigue severity, which includes both psychological and physical aspects, patients were asked, "How much fatigue did you feel after TACE?" An 11-point visual analogue scale for fatigue was utilized, with higher mean scores reflecting higher levels of fatigue. This scale serves as a straightforward alternative to more complex tools, facilitating agreement between the patient and physician [23].
Sleep quality was evaluated using the Korean version of the Verran and Synder-Halpern Sleep Scale [6], which is divided into four subdomains: sleep fragmentation (three items), length (one item), latency (one item), and depth (three items). Here, fragmentation describes the frequency of arousal or movement during sleep, length denotes the total duration of sleep, latency refers to the time it takes to fall asleep, and depth indicates the intensity of sound sleep. An 11-point Likert scale (0~10) was employed for the evaluation, where a higher average score signifies better sleep quality. The overall reliability of the scale was shown by a Cronbach’s α value of .82, with the sleep fragmentation and depth subdomains scoring .73 and .83, respectively.
Nurse assessments of patient anxiety, depression, PES, and fatigue levels were evaluated. To gauge the anticipated levels of anxiety and depression in patients, nurses employed the same assessment tools as the patients, using the question, "In general, how much of these symptoms do you expect the patient to feel before TACE?" A 4-point Likert scale facilitated this assessment, with higher scores reflecting more severe levels of anxiety and depression as perceived by the nurses. The Cronbach’s α values for anxiety and depression were .70 and .83, respectively. The anticipated severity of PES was evaluated with the question, "How much abdominal pain (or nausea, vomiting, fever) did you expect the TACE patient to experience?" Higher scores on the 11-point NRS indicated that nurses expected more severe symptoms. Similarly, the expected severity of fatigue was assessed using the same question format and the visual analogue scale for fatigue.
Data were collected from both patients and nurses. After receiving approval from the Institutional Review Board, permission was obtained from gastroenterologists, the chief manager of the nursing department, and unit managers at a tertiary hospital with 1,300 beds in Busan metropolitan city, South Korea. Data collection occurred from September to November 2022, during two patient visits and a document review. During the initial visit, a researcher explained the study's purpose and protocol, obtained written consent from the patient, and assessed their levels of anxiety and depression before TACE. PES, fatigue, and sleep quality were reassessed the day after TACE. A document review was conducted by one of the authors, which included electronic medical records (progress notes from physicians, findings from the picture archiving communication system, various laboratory data sheets) and nursing records (physiological data sheets, nursing information sheets, nursing assessment sheets, and nursing notes). To gather data from nurses, an online questionnaire was distributed to those working in gastroenterology wards. Participation rewards were provided to all participants.
This study received approval from the Institutional Review Board of the first author's institution (No. 1041386-202207-HR-43-01). Additionally, the president of the research institute granted approval for the review of electronic records. Participants were informed about the purpose of the study, the need to access electronic medical and nursing records, the voluntary nature of their participation, the methods used in the study, and the guarantees of anonymity and confidentiality. This information was provided on the first page of both the online and offline surveys. Written informed consent was obtained from all participants.
SPSS version 27.0 (IBM Corp., Armonk, NY, USA) was used for data analysis. The methodology for data analysis in this study mirrored that of a previous study, particularly in the way datasets from patients and nurses were combined [24]. Data from three to five nurses involved in TACE care were aggregated to create 49 cases per patient. For example, if patient A was hospitalized for 2 days following TACE and was attended by five nurses across three shifts, the average score from the survey completed by these nurses was recorded for patient A. The combined dataset thus created was probabilistically equivalent to a randomly selected combination. The hospital where the research was conducted employs various care delivery systems, such as the team approach, functional care, and total patient care, depending on the ward. The three wards involved in this study utilized the functional care method. As a result, nurses are responsible for providing care to all patients admitted to these wards.
As these data manipulation methods have a high potential for bias, we implemented three types of resampling to mitigate this risk. Initially, non-parametric regression analysis was conducted over 100 times, each time randomly selecting 45 patients from a total of 49 and pairing their data with that of 45 nurses. We then used the Shapiro-Wilk test to ensure that the variables in the sampled data met the normality requirement for regression analysis. Next, we applied k-fold cross-validation. Here, the data were split into training and validation sets, which were further divided into 10 random groups to assess error rates. The findings indicated consistent performance across the majority of the results. Lastly, we employed the bootstrap method, executing 5,000 iterations.
Descriptive statistics, the independent t-test, and one-way analysis of variance were employed to assess the characteristics of the variables and to explore differences in sleep quality based on patient characteristics. Nonparametric statistics were utilized when the assumptions of parametric tests were not met. The Spearman rank test was applied to evaluate the relationships between study variables. Stepwise multiple regression analysis was conducted to identify predictors of sleep quality.
The mean age of the nurses was 28.82 years, and all were women. All but one nurse held a Bachelor of Science in Nursing, with an average total nursing experience of 5.30 years. Approximately 77.6% of the patients were men, with an average age of 69.13 years. The proportion of patients who were married and living with their spouse was 83.8%, those who regularly consumed alcohol was 8.2%, and smokers constituted 14.3%. The sleep quality score was highest among those in their 60s at 5.14±1.91, followed by those in their 60s or younger and those in their 70s or older (F=0.06, p=.944). There were no significant differences in sleep quality according to marital status (F=0.30, p=.767), religion (t=-1.52, p=.135), job status (t=-0.24, p=.811), alcohol drinking (t=0.32, p=.749), or smoking (F=1.00, p=.378) (Table 1).
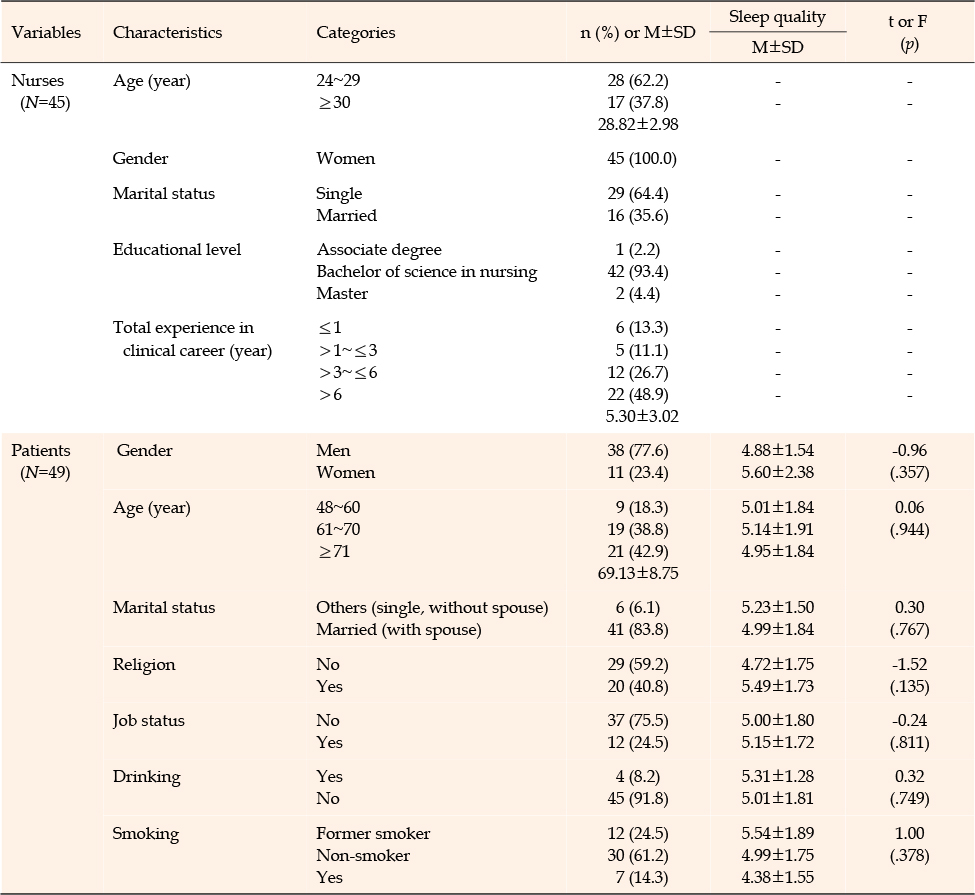
Table 1
Nurses’ Characteristics and Sleep Quality According to the Patients’ Characteristics
Table 2 presents the TACE-related patient characteristics. Before TACE, the albumin and bilirubin levels were 4.06±0.59 g/dL and 0.78±0.50 mg/dL, respectively. The AST and ALT levels were normal at 35.41±17.78 U/L and 22.39±11.56 U/L, respectively. The mean levels of lipiodol and doxorubicin were 5.55±4.30 mL and 20.61±12.27 mg, respectively. After TACE, the average score for patients’ sleep quality was 5.04±1.76 points. Analgesics were the most frequently prescribed drugs, at 0.90±0.80 times, and antiemetics and antipyretics showed similar usage rates at 0.14±0.41 and 0.14±0.50 times, respectively. The anxiety and depression scores were 1.50±0.98 and 0.94±0.87, and the score for PES was 0.94±0.24 points. The nurses’ expectation for fatigue has the highest score, at 3.38±0.69 points, while the score for fatigue according to the patients was 4.10±2.78 points.
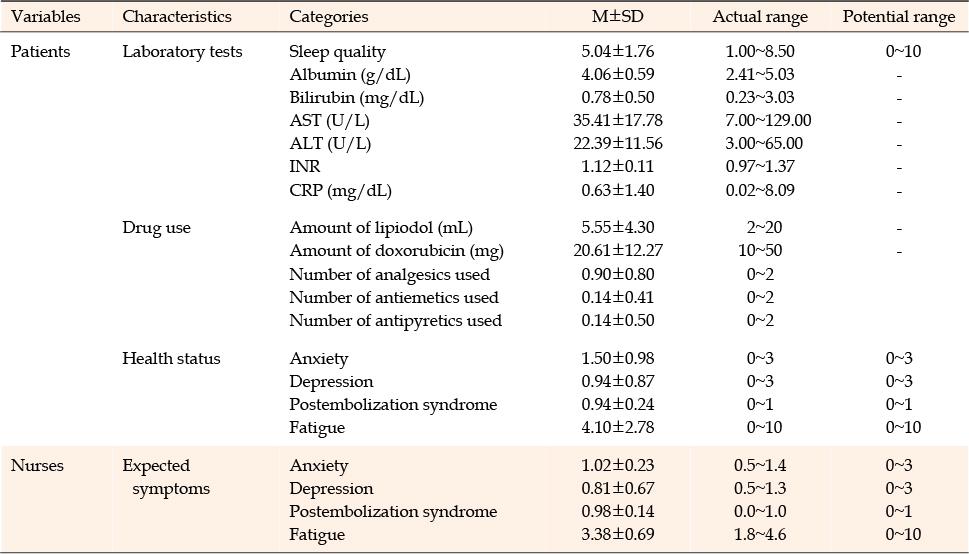
Table 2
Patients’ Characteristics and Nurses’ Perceptions of Patients’ Symptoms (N=49)
Sleep quality was negatively associated with the number of antipyretics used (r=-.31, p=.029), anxiety (r=-.40, p=.004), PES (r=-.30,=.034), and fatigue (r=-.63, p<.001). Conversely, there was a positive correlation between sleep quality and expected fatigue as assessed by the nurses (r=.45, p=.001) (Table 3).
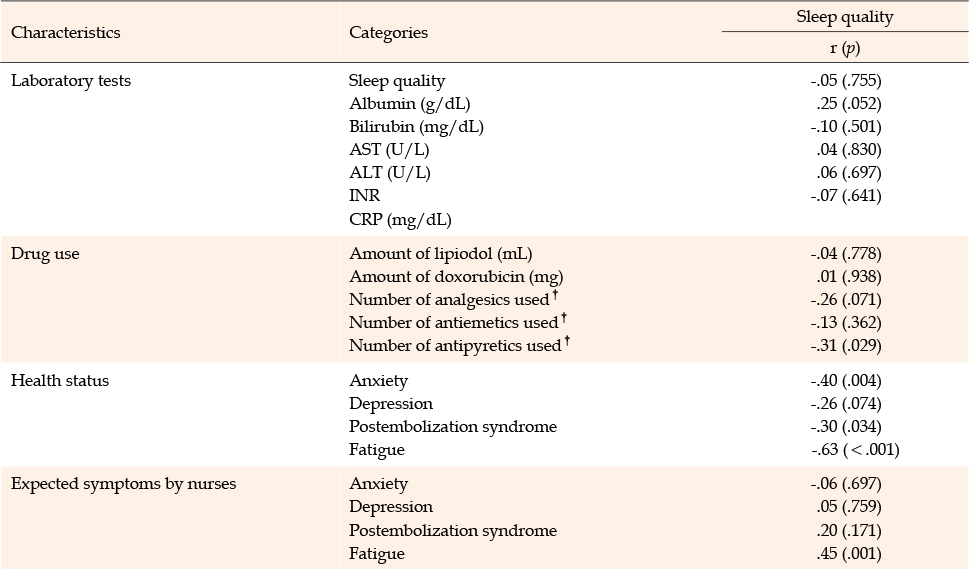
Table 3
Correlation of Variables with Patients’ Sleep Quality (N=49)
In the multiple regression analysis, two of the five input variables emerged as significant factors influencing patient sleep quality (F=8.39, p<.001), explaining 43.5% of the variance in sleep quality (Table 4). Specifically, the results indicated that more severe fatigue in patients (β=-.47, p=.001) and increased use of antipyretics (β=-.33, p=.005) were associated with poorer sleep quality. The Durbin-Watson level indicated no significant self-correlation, registering at 1.89, which is close to the ideal value of 2.0.
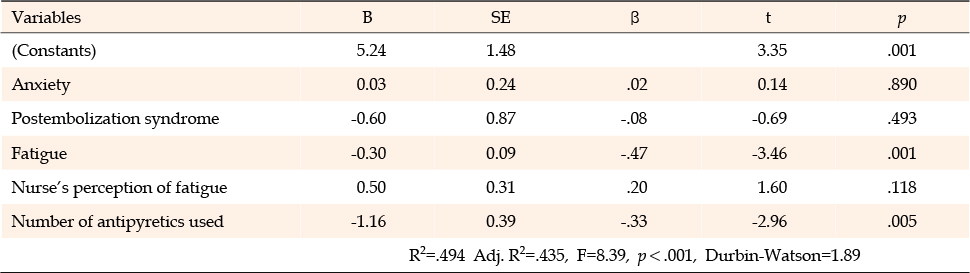
Table 4
Factors Influencing the Sleep Quality of Patients Undergoing TACE (N=49)
This study aimed to evaluate patients' symptoms, nurses' perceptions of these symptoms, and factors influencing sleep quality. Descriptive comparisons showed that, unlike anxiety, depression, and fatigue, patients reported lower levels of PES than those anticipated by nurses. Laboratory results showed no clear relationships with sleep quality and were not considered significant. Stepwise multiple regression analysis identified patient fatigue and the number of antipyretics used as statistically significant predictors of sleep quality in patients undergoing TACE.
Patients' sleep quality, with a score of 5.04, was lower than that of general ward patients, who scored 6.42 [25], indicating poorer sleep quality. Cancer patients often experience higher rates of sleep disturbance, with over half of those undergoing chemotherapy reporting reduced sleep quality [19]. The TACE procedure, which involves the occlusion and embolization of the hepatic artery following the injection of a cytotoxic drug, leads to congestion and necrosis of the lesion [3] and disrupts nocturnal sleep due to PES. The sleep quality observed in TACE patients was comparable to that of colon cancer patients as measured using the Pittsburgh Sleep Quality Index [26], and it was relatively lower than that of patients with other cancers, including breast cancer. Additionally, factors such as light, noise, and frequent medical staff visits [25], known to disrupt sustained sleep in general wards, pose challenges for patients undergoing TACE. Despite the relatively low sleep quality observed in TACE patients in this study, this issue has received limited attention, and there is a scarcity of evidence-based research in this area, indicating a lack of focus on comfort care. Therefore, more attention should be directed toward comfort care, including sleep quality, for patients undergoing TACE.
Patients experienced PES to a lesser extent than what nurses expected, contrasting with the usual situation where nurses tend to underestimate patient pain [27]. This discrepancy may be due to nurses' improved understanding of their patients' PES, fostered by increased familiarity with TACE and the prominent role of PES within the symptom cluster. Given the significant negative impact of TACE on sleep quality [3], which subsequently affects patients' mood and activity levels, it is essential to enhance educational content and efforts to improve patient comfort [9]. Moreover, effective symptom recognition by nurses is vital for preventing sleep disorders. Implementing an ongoing clinical education model that focuses on recognition, explanation, action, and learning could resolve clinical communication issues affecting patients with physical symptoms [28]. In essence, enhancing nursing care involves timely recognition of symptoms and understanding the nature of PES, explaining these symptoms to patients, and implementing strategies for relief. Therefore, ongoing access to educational resources and training through the adoption of educational programs is necessary to enable healthcare professionals to better understand and address issues related to sleep quality, ultimately enhancing overall care and patient well-being.
Fatigue emerged as a significant factor influencing sleep quality in patients. Typically, the onset of patient fatigue occurs 1-2 days after TACE [7], persists at a moderate level for up to 6 days [29], and contributes to additional symptoms such as sleep disorders, physical weakness, and loss of appetite [30]. Previous studies have indicated that patients with breast cancer often experience a sequence of fatigue, sleep disorders, and depression, with exercise and diet programs showing potential to alleviate both fatigue and depression [31]. Numerous studies have established a negative relationship between fatigue and sleep quality, although fatigue and sleepiness were often considered synonymous in the past. Fatigue is closely associated with anxiety and depressive mood [32], which can, in turn, contribute to poor sleep quality [33]. Patients with anxiety and depression tend to take longer to fall asleep, sleep less, and take longer to reach the REM stage, all of which indicate higher levels of fatigue. While evidence supporting these results is limited, fatigue can still be a significant factor in poor sleep quality. During chemotherapy, fatigue is also linked to depression, anxiety, and distress about symptoms [5], and is expected to indirectly affect sleep quality. Since fatigue and sleep quality are key comfort-related challenges for patients undergoing TACE during hospitalization, it is crucial to implement various interventions, including psychological support, education, and counseling, to address chemotherapy-related adverse events.
Anxiety can negatively impact sleep quality, and depression also affects various aspects of sleep, including its architecture and efficiency, according to a previous study [15]. Moreover, poor sleep quality in patients with anxiety can lead to significant negative outcomes in daily life, including cognitive disorders, highlighting a bidirectional relationship between them [34]. In this study, depression and anxiety were not influencing factors, possibly due to the longitudinal data collection method used. The unique approach of assessing depression and anxiety at a predetermined time point, along with the immediate evaluation of sleep quality after TACE, may provide a more accurate understanding of patients' emotions. Increased levels of anxiety and depression are directly linked to the burden of a cancer diagnosis, the stress associated with ongoing checkups and hospital visits, and the side effects of various treatments. The results of this study showed relatively low levels of anxiety and depression among patients, in contrast to other studies that have relied on patients’ simultaneous recall of their mood status. This was often assessed at the same time as sleep quality before chemotherapy, which could have led to an overestimation.
An unexpected factor influencing sleep quality was the number of antipyretics used. At the study hospital, non-steroidal anti-inflammatory drugs are commonly employed as antipyretics, though they were not previously known to directly affect sleep. It is crucial to investigate whether the administration of antipyretic drugs directly or indirectly contributes to poor sleep quality. In this scenario, the primary concern is the fever itself, rather than the antipyretic drugs. Discomfort from the fever or the nursing interventions required for fever monitoring could disrupt sleep, potentially leading to the erroneous belief that sleep disturbances are directly caused by antipyretics. Considering that fever often occurs alongside abdominal pain and nausea/vomiting, it has been noted that dexamethasone, which has anti-inflammatory and anti-immune properties, can be used to manage these symptoms and reduce fever [35]. Therefore, it is important to monitor for discomfort following the use of alternative drugs, and employing a non-contact thermometer for silent monitoring could be beneficial.
Symptoms that nurses typically anticipate, such as anxiety, depression, PES, and fatigue, were not found to be influencing factors. Despite the anticipated positive correlation between sleep quality and fatigue as expected by nurses, the significant predictors differed from these expectations. Two potential explanations exist for this discrepancy. First, patients often report their fatigue and sleep quality passively [14], which may prevent nurses from accurately assessing these conditions. Second, nurses might not view fatigue as a factor that deteriorates sleep quality, nor adjust their nursing management strategies to enhance sleep during short hospital stays. Proper detection of fatigue and appropriate preparation for sleep are essential for improving sleep quality.
The strength of this study is that it offers foundational data for practical comfort care, which was achieved by gathering accurate patient information before and after TACE. However, there are some limitations to this method. First, the results may have inadequate statistical power due to the restricted data collection caused by the resurgence of coronavirus disease-19 (COVID-19). Second, the lack of wearable devices to objectively evaluate sleep quality in relation to inflammation necessitated reliance on subjective data, which may limit the generalizability of the findings. Therefore, further analysis of sleep quality using broader objective measures and longitudinal data is warranted.
This descriptive study aimed to assess sleep quality and the factors influencing it in patients with HCC who underwent TACE. The study identified patients' fatigue levels and the frequency of antipyretic drug use as significant variables affecting sleep quality. Specifically, higher fatigue after chemoembolization and more frequent antipyretic use were associated with poorer sleep quality. These findings highlight the importance of aligning nurses' perceptions of patients' symptoms in the delivery of comfort care and emphasize the need for environments that alleviate patient fatigue. Additionally, the study suggests the need for further research on the causal relationship between antipyretic use and sleep quality, as well as exploring the link between nurses' perception of anxiety and patients' symptoms, which presented conflicting results compared to prior studies.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design - PJY and KMS.
Material preparation, data collection and analysis - PJY, KMS, and LHB.
draft and critical revision of the manuscript - PJY, KMS, and LHB.
All authors read and approved the final manuscript.
This article is an extended study based on the first author's master's thesis from Pukyong National University.
 E-SUBMISSION
E-SUBMISSION