
Purpose
This study investigated differences in inner strength, multiple identities, and quality of life among colorectal cancer survivors, considering gender and the presence of an ostomy. It also focused on identifying factors that influenced their quality of life.
Methods
In this cross-sectional study, 170 colorectal cancer survivors were recruited.
Inner strength, multiple identities, and quality of life were assessed through an online survey. Within each subgroup, comparisons were made in two ways: (a) between women and men; and (b) between ostomy and non-ostomy groups.
Results
The quality of life for colorectal cancer survivors was higher among men than women. For inner strength, men reported higher levels of anguish and searching, whereas women showed higher levels of connectedness. The quality of life was higher in the non-ostomy group than the ostomy group. However, the non-ostomy group had a higher level of anguish and searching than the ostomy group. Inner strength emerged as the most powerful factor influencing quality of life after adjusting for age and gender.
Conclusion
This study emphasizes the significance of inner strength in colorectal cancer survivors. It provides a deeper understanding of quality of life in colorectal cancer survivors by examining factors that influence it and considering how these effects differ based on gender and the presence of an ostomy. To improve the quality of life of colorectal cancer survivors, it is essential to comprehend the roles of factors such as gender and ostomy and develop individualized interventions tailored to their specific characteristics.
This study investigated differences in inner strength, multiple identities, and quality of life among colorectal cancer survivors, considering gender and the presence of an ostomy. It also focused on identifying factors that influenced their quality of life.
In this cross-sectional study, 170 colorectal cancer survivors were recruited. Inner strength, multiple identities, and quality of life were assessed through an online survey. Within each subgroup, comparisons were made in two ways: (a) between women and men; and (b) between ostomy and non-ostomy groups.
The quality of life for colorectal cancer survivors was higher among men than women. For inner strength, men reported higher levels of anguish and searching, whereas women showed higher levels of connectedness. The quality of life was higher in the non-ostomy group than the ostomy group. However, the non-ostomy group had a higher level of anguish and searching than the ostomy group. Inner strength emerged as the most powerful factor influencing quality of life after adjusting for age and gender.
This study emphasizes the significance of inner strength in colorectal cancer survivors. It provides a deeper understanding of quality of life in colorectal cancer survivors by examining factors that influence it and considering how these effects differ based on gender and the presence of an ostomy. To improve the quality of life of colorectal cancer survivors, it is essential to comprehend the roles of factors such as gender and ostomy and develop individualized interventions tailored to their specific characteristics.
Colorectal Cancer (CRC) is the third most common cancer worldwide, accounting for 1,880,725 of 19,292,789 newly diagnosed cases in 2020 [1]. In Korea, the age-standardized incidence rate of CRC per 1,000 people rose from 20.6 in 1999 to 31.9 in 2021, while the 5-year relative survival rate for patients from 2017 to 2021 was 74.3% [2]. Although the incidence rates of CRC were previously increasing, this trend has notably reversed, with declines beginning in 2010 and 2004, respectively [2]. The Quality of Life (QOL) of CRC survivors has become a significant global health concern, paralleling the rise in CRC incidence and improvements in the survival rates.
CRC survivors experience physical symptoms such as pain, fatigue, and sleep disorders in their daily lives, long after their diagnosis. Additionally, they must adhere to a strict long-term diet to manage their intestinal health [3]. Psychological issues, including depression and anxiety, often arise from large surgical scars or ostomies in the lower abdomen, which can significantly alter their body image [4]. Ostomies also negatively impact patients' physical appearance and QOL [5]. Living with an ostomy can lead to psychological atrophy in CRC survivors, complicating their ability to resume normal daily activities. To summarize, various issues that arise after CRC treatment can significantly diminish the well-being and QOL of CRC survivors.
Some factors that influence the QOL of CRC survivors include age, gender, and occupation [6, 7]. Additionally, the number and severity of symptoms resulting from CRC are associated with lower QOL [8]. CRC survivors who have ostomies face a range of physical, mental, and social challenges that adversely impact their QOL. The presence of an ostomy itself is associated with a decrease in the overall QOL of CRC survivors [9].
Gender is also an important factor affecting the QOL of CRC survivors. Generally, the QOL of female survivors is lower than that of male survivors [10]. Additionally, research has indicated that the factors impacting QOL differ between male and female CRC survivors [11]. For instance, female survivors tend to have lower QOL in physical and sexual aspects compared to their male counterparts, whereas male survivors are more likely to experience psychological symptoms, including stress, depression, and problems with sexual arousal [12].
Inner strength is increasingly recognized as a valuable strategy for cancer survivors to manage negative experiences and foster positive changes that improve their QOL [13, 14]. It is characterized by an individual's capacity to navigate adversity and promote personal well-being during transformative events [14, 15]. Studies indicate that inner strength plays a crucial role in improving the QOL for patients with breast and lung cancers [16, 17]. The exploration of inner strength began with research on patients with early-stage breast cancer. This concept was formalized by Lewis and Roux [18], who created a questionnaire to assess the inner strength of women battling the disease. Smith [19] notes that while inner strength was initially focused on women's experiences, it is equally significant for men.
Similar to inner strength, social identity plays a crucial role in determining how individuals respond and adapt to life changes [20]. Multiple identities have been recognized as a method for assessing the extent to which individuals perceive themselves as part of various social groups. During the transition period following treatment, cancer survivors often participate in a range of social group activities, including spending time with friends, engaging in workplace activities, attending gatherings, and observing religious traditions. Specifically, cancer survivors exchange medical information and life experiences, which helps alleviate their pain by sharing their experiences of living with the disease [21].
Considering the limited literature available and the scant knowledge about the inner strength of cancer survivors, this study aimed to understand how inner strength, multiple identities, and QOL vary based on gender and the presence of an ostomy. With the ultimate goal of improving the QOL of CRC survivors, this study sought to determine the impact of inner strength and multiple identities on their QOL.
This study utilized a cross-sectional descriptive design. Data collection occurred from June 1 to June 30, 2021, among members of an online CRC survivor community in Korea. The inclusion criteria included a diagnosis of CRC at least 3 months prior to the study, being 18 years of age or older, possessing clear communication, reading, and writing skills, and having no diagnosed mental health conditions. The ideal sample size was predetermined using G*Power 3.1.9 software. A power analysis indicated that a minimum of 168 participants was necessary for multiple regression analysis. This calculation took into account an effect size of 0.15, a significance level (α) of .05, seven independent variables, a desired statistical power (1-β) of .95, and a 10% anticipated dropout rate. Ultimately, 171 participants were recruited; however, after excluding those who did not meet the inclusion criteria, data from 170 participants were used in the final analysis.
Information about the participants’ demographic and clinical characteristics was collected using a questionnaire developed by the authors. The clinical data were self-reported. We collected data on demographic characteristics (age, gender, Employment status, religion, and marital status) and clinical characteristics (pathological diagnosis, stage, metastatic status, surgical history, time since diagnosis, ostomy status, treatment modality, and comorbidities).
The Korean version of the Inner Strength Questionnaire (ISQ) was utilized to assess the inner strength of CRC survivors [18, 22]. The ISQ consists of 27 items divided into four subscales: 7 items in the "anguish and searching" subscale, which explores the transition from initial fear and shock to acceptance during challenging life events; 7 items in the "connectedness" subscale, focusing on the development of supportive relationships; 6 items in the "engagement" subscale, which deals with participation in self-determination and life possibilities; and 7 items in the "movement" subscale, concerning relaxation and the balance of body and mind. Responses to all ISQ items are recorded on a 5-point Likert-type scale, where 1=strongly disagree and 5=strongly agree. Items in the "anguish and searching" subscale are reverse-scored. The total ISQ score is calculated by summing the scores of the four subscales, with possible scores ranging from 27 to 135 points. Higher scores on the subscales and the total score indicate greater inner strength [18, 22]. The internal consistency coefficient (Cronbach’s α) for the ISQ in this study was .87.
Multiple identities were measured using the Korean version of the Exeter Identity Transition Scales (EXITS) [23]. Participants responded to four items, each rated on a 7-point scale ranging from 1 (do not agree at all) to 7 (agree completely). These items assessed whether participants had maintained their pre-cancer group memberships following their diagnosis (e.g., "After my cancer, I still participate in the same group activities as before my cancer"). The total scores could range from 4 to 28, with higher scores indicating stronger social connections. Cronbach’s α for this study was .96.
QOL was assessed using the Functional Assessment of Cancer Therapy - General - 7 Item Version (FACT-G7) [24]. The FACT-G7 includes seven high-priority items from the FACT-G that address physical well-being ("I have a lack of energy," "I have nausea," and "I have pain"), emotional well-being ("I worry that my condition will get worse"), and functional well-being ("I am able to enjoy life," "I am sleeping well," and "I am content with the quality of my life right now") [25]. Each item is rated on a 5-point Likert scale, which ranges from 0 (not at all) to 4 (very much). The total score can range from 0 to 28, with higher scores indicating better QOL. Cronbach’s α for this scale was .80 in this study.
Data were gathered via an online survey (Google Forms) administered in online communities (Naver Band, Self-help group) for CRC survivors. The researcher provided detailed information about the study, including its purpose, on the initial screen of the survey link. Participants voluntarily accessed the questionnaire by clicking on the link, and this action was considered as giving informed consent.
This study received approval from the institutional review board of the authors' affiliated institution (approval no: 1041078-202104-HRSB-096-01), and this approval was linked to the online survey. Participation in the survey was limited to those who consented to be part of the study. Respondents who experienced difficulty in completing the survey, such as those of advanced age, were allowed to do so with assistance from their caregivers. The online survey required approximately 10~15 minutes to complete, and participants were compensated with a KRW 10,000 coffee voucher for their participation.
Data were analyzed using SPSS version 26.0 (IBM, Armonk, NY, USA). The general characteristics of the participants, disease-related characteristics, and study variables were assessed using descriptive statistics, including frequency, percentage, mean, and standard deviation. The normality of the study variables was verified using the Kolmogorov-Smirnov test. Differences in inner strength and QOL among CRC survivors, based on gender and the presence of ostomies, were examined using the independent t-test. Pearson’s correlation coefficient was utilized to evaluate the relationship between inner strength, multiple identities, and QOL in CRC patients. A hierarchical multiple regression analysis was conducted to identify factors that influence QOL. Given the limited sample size, Hedge’s g [26] was used as the effect size estimator. This metric is preferred as it provides a more accurate correction for bias in studies with small samples compared to other metrics like Cohen's d. For these analyses, the significance level was set at α=.05.
The characteristics of CRC survivors are presented in Table 1. Over half of the participants were men (54.1%), and the mean age of the total sample was 53.09 years. Approximately half of the participants were working at the time of the survey (43.5%) and were secular (50.6%), and most of them were married (81.8%). Thirty-one (18.2%) participants had an ostomy and 139 (81.8%) did not. Approximately 30.0% of the patients had comorbidities, including hypertension, diabetes mellitus, Cardio-cerebrovascular disease, and other diseases, such as benign prostate hypertrophy, hypothyroidism, and herniated lumbar disc.
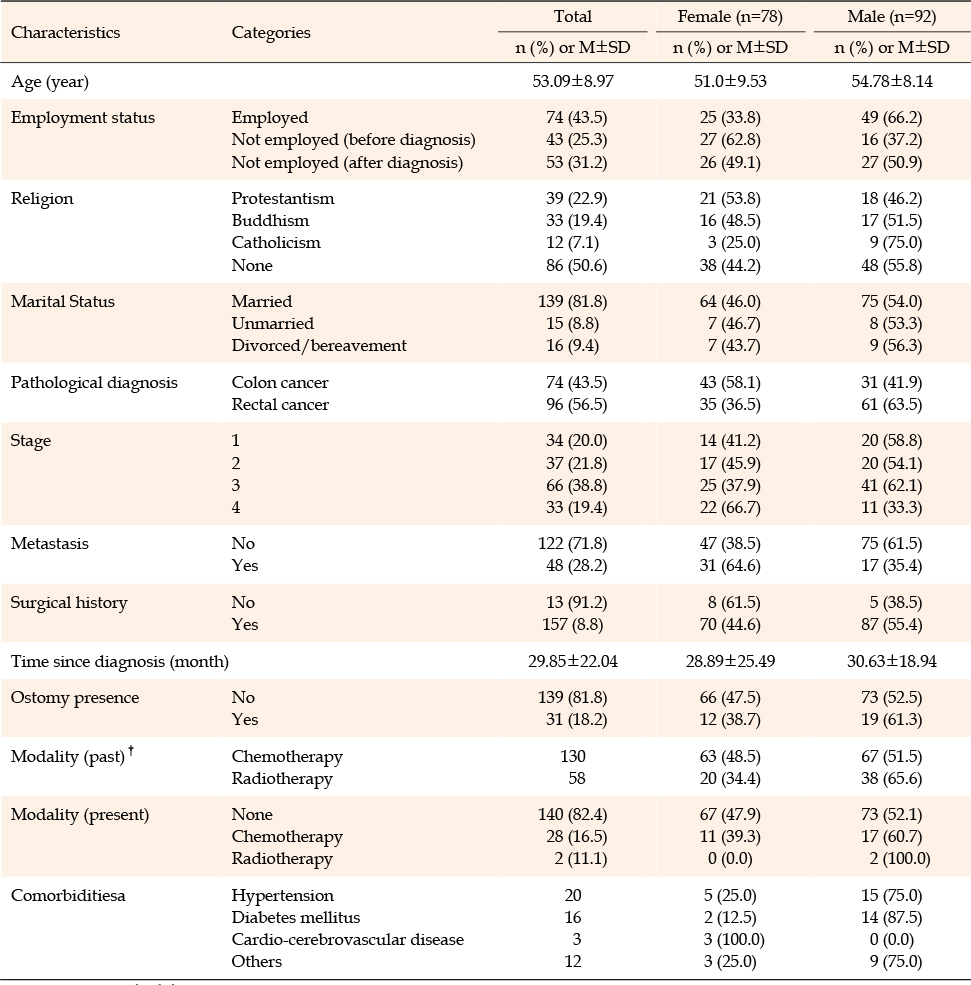
Table 1
Demographic and Clinical Characteristics of Study Participants (N=170)
Among the sub-categories of inner strength, male participants had statistically significantly higher scores for anguish and searching (t=-3.91, p<.001, g=0.60) and lower scores for connectedness (t=3.42, p=.001, g=0.53) than their female counterparts in Table 2. There was also a significant difference in QOL according to gender (t=-2.06, p=.041, g=0.32). Furthermore, male participants scored higher than female participants on multiple identities; however, the difference was not statistically significant.
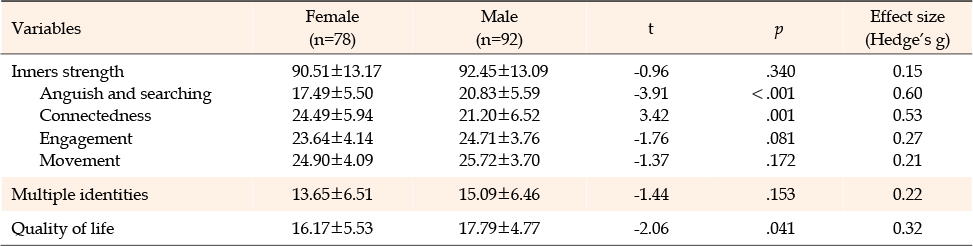
Table 2
Comparison of Study Variables According to Gender (N=170)
As shown in Table 3, there was a significant difference in connectedness (t=2.02, p=.046, g=0.40) according to the presence or absence of an ostomy. The mean score for connectedness was 20.61 in the ostomy group and 23.17 in the non-ostomy group. Inner strength was also higher in the non-ostomy group than in the ostomy group. The mean score for multiple identities was higher in the non-ostomy group than in the ostomy group; however, the difference was not statistically significant. QOL exhibited a significant difference according to the presence or absence of an ostomy; the QOL score was 15.29 in the ostomy group and 17.44 in the non-ostomy group (t=2.10, p=.036, g=0.42).
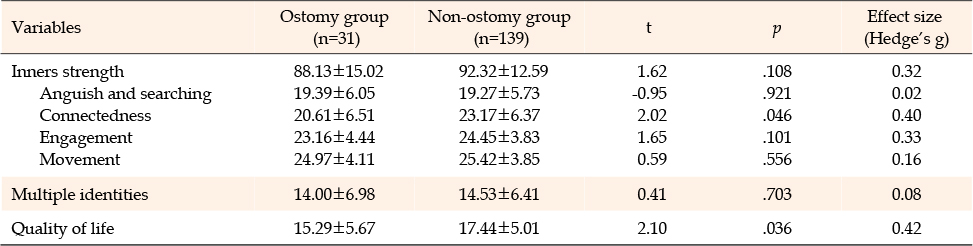
Table 3
Comparison of Study Variables According to Ostomy Presence (N=170)
Initially, we evaluated the assumptions of linear regression. Scatterplots were visually inspected to confirm linearity between the independent and dependent variables. The Durbin-Watson statistic was used to evaluate autocorrelation, yielding a value of 1.977. This value is close to the ideal of 2, indicating no significant autocorrelation issues [27]. Homoscedasticity and normality of residuals were verified through visual inspection of standardized residual scatterplots and p-p plots. Multicollinearity among the independent variables was assessed using correlation coefficients, which ranged from 0.01 to 0.52. This range indicates the absence of strong correlations (|r|>0.9) [27]. The variance inflation factors ranged from 1.072 to 1.759, all below the recommended threshold of 2, suggesting no concerns of multicollinearity [27].
QOL showed a statistically significant positive correlation with inner strength (r=.52, p<.001), and multiple identities (r=.35, p<.001). Hierarchical regression was performed to identify factors affecting the QOL of CRC survivors (Table 4). The independent variables for the regression model were selected based on the literature review conducted for this study [6, 7, 9, 10]. The selected variables were age, gender, employment status, presence of an ostomy, inner strength, and multiple identities. Employment status was operationalized as a dummy variable, depending on current employment status as "Yes" and "No". And cases without employment were divided into "unemployment after CRC diagnosis" and "not related to CRC diagnosis and employment status".
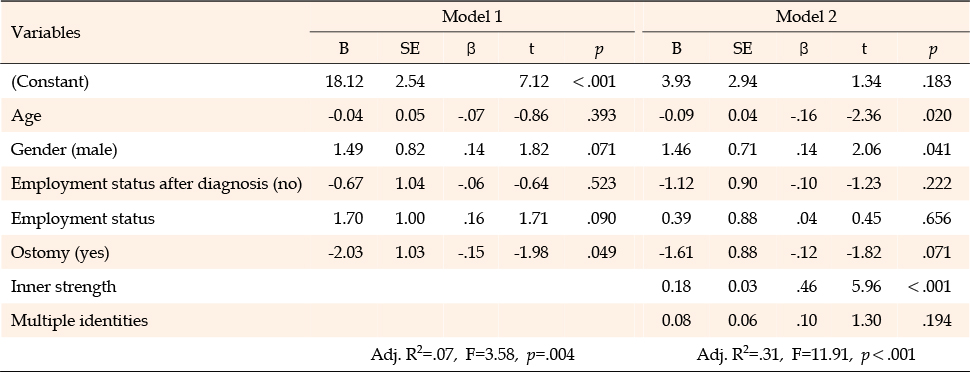
Table 4
Factors Influencing Quality of Life (N=170)
The first model was based on age, gender, employment status, and the presence of an ostomy. The presence of an ostomy was identified as a significant influencing factor (B=-2.03, p=.049), with people without an ostomy reporting a higher QOL than those with an ostomy. Model 1 was statistically significant (F=3.58, p=.004) and accounted for 7.1% of variance.
The second model involved the internal strength of CRC survivors. In this model, significant influencing factors were age (B=-0.09, p=.020), gender (B=1.46, p=.041), and inner strength (B=0.18, p<.001). QOL was higher in younger participants, d in those with higher levels of inner strength, and in men. Model 2 was statistically significant (F=11.91, p<.001) and accounted for 31.1% of variance.
This study investigated inner strength, multiple identities, and QOL in CRC survivors and identified factors affecting their QOL. Among the sub-categories of inner strength, connectedness exhibited lower scores in the ostomy group than in the non-ostomy group. Meanwhile, male participants had higher scores for anguish and searching, whereas female participants had higher scores for connectedness. A possible explanation for these findings may relate to the fact that physical problems, such as intestinal retention and sexual dysfunction, negatively affect QOL, especially among male CRC survivors [28]. In addition, CRC survivors with ostomies may have had a greater ability to deal with anguish and searching because they experience frequent ostomy-related difficulties causing them to focus on their physical symptoms.
Considering inner strength from the perspective of resilience [15], a previous study found that CRC patients with ostomies exhibited lower resilience than those without ostomies and that female patients had lower resilience than male participants [29]; these findings align with the present study’s overall outcomes. Among the four subcategories of inner strength, only anguish and searching had higher scores in the ostomy group than in the non-ostomy group, while connectedness was the only factor with higher scores among women than among men. It is necessary to further explore the specific experiences of CRC survivors' inner strength, despite the lack of significant differences in inner strength between genders and between those with or without ostomies.
Multiple identity scores were higher in the non-ostomy group and among male survivors compared to the ostomy group and female survivors, respectively. However, these differences were not statistically significant. Multiple identities should be explored to assess the degree of change in key groups before and after significant life events. This study, however, only investigated multiple identities at a single point in time, and this limitation should be taken into account when interpreting the results. Multiple identity pertains to the significance and extent of relationships. Multiple identities can manifest in various forms, and supportive relationships can develop through these connections [20]. Support systems, such as family or patient self-support groups, are crucial in aiding patients' adaptation to life post-diagnosis and treatment. CRC survivors often find comfort in sharing experiences with groups whose members have undergone similar experiences [21]. Therefore, in-depth interviews should be conducted to examine the support systems of CRC survivors.
In the present study, the QOL of patients with ostomies was found to be lower than that of patients without ostomies, aligning with the findings of Song and Han [30]. Additionally, a study by Yanez et al. [25], which utilized the same assessment tool (FACT-G7) as our study, reported that the QOL score of cancer-free individuals was 19.45 points, whereas it was 18.04 for cancer survivors of 11 types, including colon cancer. These scores are higher than those found in our study, where the overall QOL for the ostomy group was 15.29, and for the non-ostomy group, it was 17.44. These findings are consistent with those reported by Kim [31], who demonstrated that the QOL of CRC survivors was lower than that of other cancer survivors and the general population. It has been documented that CRC survivors experience a diminished QOL compared to other cancer survivors due to long-term bowel-related issues and bodily changes [9, 32]. However, understanding the impact of an ostomy on QOL over the mid- to long-term (5 years or more) is challenging, as the period following CRC diagnosis in this study was approximately 2 years.
The QOL of female CRC survivors was found to be lower than that of their male counterparts. This result is consistent with previous research indicating that women generally report a lower QOL than men [33]. Earlier studies have identified gender-based differences in the factors that affect the QOL of CRC survivors. Since this study did not explore aspects such as sexual activity, satisfaction, or the economic status of participants, it was not possible to determine any relationships or influencing factors between these characteristics and QOL. However, prior research has noted that women tend to face general social challenges and psychological issues stemming from changes in body image, whereas men primarily experience difficulties related to social factors and the effects of CRC itself.
The QOL of CRC survivors positively correlates with their inner strength and multiple identities. In this study, we found that higher levels of inner strength and multiple identities were associated with better QOL. These findings align with previous research on cancer survivors [16, 22]. Although prior studies have not specifically explored the inner strength of CRC survivors, Temprado Albalat et al. [34] demonstrated that the resilience of CRC survivors with ostomies positively correlated with their QOL. In essence, CRC survivors with higher levels of resilience experience less pain, which in turn positively influences their adaptation to new life circumstances. Future research should explore the variables associated with QOL across various physical, psychological, and social dimensions, focusing on inner strength and other factors that impact QOL.
In a hierarchical regression analysis examining factors that affect the QOL among CRC survivors, Model 1 accounted for 7.1% of the variance, while Model 2 accounted for 31.1%. The factors influencing QOL in CRC survivors are diverse, and the complexity and interplay of these factors make prediction difficult. The significant increase in explanatory power in Model 2 highlights the importance and necessity of this research, which provides essential insights for developing interventions to improve QOL in these individuals. In conclusion, although the explanatory power observed in this study is relatively low, it reflects the complex factors impacting QOL among CRC survivors. Given that various unseen elements could also affect QOL beyond the variables included in our study, future research should explore these factors more thoroughly and incorporate them into models to predict QOL outcomes more accurately.
In this study, gender, age, and inner strength influenced the QOL of CRC survivors. A higher QOL was associated with being younger, male, and having greater inner strength. Inner strength was the most significant factor affecting the QOL of CRC survivors. Roux et al. [14] identified inner strength as the most significant predictor of QOL among breast cancer survivors. This finding supports the hypothesis that enhancing inner strength can improve the QOL of cancer survivors.
According to Thong et al. [7], long-term CRC survivors generally exhibit similar QOL. However, issues such as loss of physical function, health deficiencies, symptoms, and financial problems predominantly affect younger CRC survivors. This finding contrasts with the results of the current study, which indicate that younger individuals tend to have higher QOL. This discrepancy may be due to the broad age range of the subjects in this study, which spans from 27 to 77 years, with a median age of 53.5, differing from previous research. Additionally, while age does impact QOL, the association between QOL and age primarily relates to variations in physical activity capability [35]. Therefore, future studies should include more detailed assessments of participants' physical abilities.
The limitations of this study are as follows. First, participants were recruited from online communities of CRC survivors, which may mean that the subjects were already relatively healthy. Additionally, caregivers were temporarily permitted to assist elderly participants, but it is unclear whether their opinions may have influenced the responses. Therefore, caution should be exercised when generalizing and interpreting the results of this study. Second, there was a significant disparity in the sample sizes between the ostomy and non-ostomy groups, as well as variations in the shape and type of ostomy; this limits the generalizability of the study findings to all CRC survivors. Third, this cross-sectional survey does not establish a causal relationship between the QOL of CRC survivors and related variables. Finally, the study did not measure anxiety and depression, psychological symptoms that can impact QOL, which limits the exploration of related factors.
Further studies are needed to explore and understand the factors that influence the inner strength and QOL of CRC survivors. These studies should aim to overcome the limitations of current research and expand our understanding of the differences among colon cancer survivors based on gender and intestinal health. Drury et al. [28] suggest that interventions aimed at supporting nursing staff, rather than focusing solely on primary care or specialist physicians, may be more effective in addressing the unmet QOL needs of CRC survivors. This study demonstrates that inner strength significantly enhances the QOL of CRC survivors, including men. It highlights differences in QOL based on gender and the presence of an ostomy, confirming that these factors significantly impact the well-being of CRC survivors. The research emphasizes the need to develop management protocols that are tailored to the specific characteristics of the subjects, showing that such protocols can improve their QOL. Furthermore, the study advocates for the integration of these protocols into mobile applications to improve ongoing care and accessibility for CRC survivors. This strategy is expected to contribute to the long-term improvement of survivors' QOL.
Although the concept of inner strength was initially researched among women with chronic illnesses, it has broad applicability, including to men and cancer patients. This study explored the relationship between inner strength, multiple identities, and QOL in CRC survivors. The findings revealed that inner strength had the most significant positive impact on participants' QOL. Additionally, there were notable gender differences in inner strength; women demonstrated higher levels of connectedness, whereas men experienced greater levels of anguish and searching. To enhance the inner strength of male CRC patients, interventions such as expressive writing programs could be beneficial. These programs help improve self-awareness, confirm identity, and develop problem-solving skills. For female patients, healthcare providers should highlight the importance of connectedness and consider strategies to nurture supportive relationships with themselves, family, friends, and spiritual sources in their individual care plans.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
All authors have contributed significantly, and all authors agree with the content of the manuscript.
Conception and design - YH and RE.
collection and assembly of data - YH.
data analysis and interpretation - all authors.
manuscript writing - all authors.
final approval of manuscript - all authors.
These results have not been previously published as a full article or in parts in any scientific journals.
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2021R1F1A1055687). This research was supported by the Chung-Ang University Research Scholarship Grants in 2022.
This article is based on part of the first author's master's thesis from Chung-Ang University The preprint version of this study is available on Research Square (www.researchsquare.com).
 E-SUBMISSION
E-SUBMISSION