
Purpose
This study was performed to identify factors associated with nursing performance, classify potential profiles of nursing performance-related variables, and explain their effects on nursing performance.
Methods
The study involved 245 nurses at a University Hospital in South Korea from September 1 to 14, 2021. The participants were nurses in a ward who operated within a team and had at least 6 months of clinical experience. Structured questionnaires were used to measure variables, and data were collected online using Google Forms. Using latent profile analysis, the participants were classified into four human resource and job attitude profiles. Linear regression was used to identify relevant factors, and one-way analysis of variance was employed to examine the differences in nursing performance between the four profiles.
Results
Shared leadership (β=.30, p<.001) was most strongly associated with nursing performance, followed by authentic leadership (β=.16, p=.009), and education level (β=.15, p=.006).
Significant differences in nursing performance (F=22.48, p<.001) were observed across profiles, with the groups deemed "excellent" and "best" scoring higher in nursing performance and authentic leadership compared to the "fair" and "worst" groups. However, no significant difference in education level was found across the latent profiles (p=.212).
Conclusion
This research examined the impact on nursing performance through variable-centered analysis and a person-centered approach. Accordingly, this study provides valuable insights for interpreting the results of linear regression analysis, highlighting the need to consider individual heterogeneity.
This study was performed to identify factors associated with nursing performance, classify potential profiles of nursing performance-related variables, and explain their effects on nursing performance.
The study involved 245 nurses at a University Hospital in South Korea from September 1 to 14, 2021. The participants were nurses in a ward who operated within a team and had at least 6 months of clinical experience. Structured questionnaires were used to measure variables, and data were collected online using Google Forms. Using latent profile analysis, the participants were classified into four human resource and job attitude profiles. Linear regression was used to identify relevant factors, and one-way analysis of variance was employed to examine the differences in nursing performance between the four profiles.
Shared leadership (β=.30, p<.001) was most strongly associated with nursing performance, followed by authentic leadership (β=.16, p=.009), and education level (β=.15, p=.006). Significant differences in nursing performance (F=22.48, p<.001) were observed across profiles, with the groups deemed "excellent" and "best" scoring higher in nursing performance and authentic leadership compared to the "fair" and "worst" groups. However, no significant difference in education level was found across the latent profiles (p=.212).
This research examined the impact on nursing performance through variable-centered analysis and a person-centered approach. Accordingly, this study provides valuable insights for interpreting the results of linear regression analysis, highlighting the need to consider individual heterogeneity.
Healthcare institutions are increasingly tasked with improving their staff's work ability to meet the rising expectations of consumers for services [1]. Nursing performance, which includes the work process, attitude, and outcomes of individual nurses within a unit, is the cornerstone of productivity in hospitals due to the high presence of nursing staff [2]. Human factors play a key role in the performance of individual nurses, as nursing care is inherently team-based [3]. The Nursing Care Performance Framework was developed through a systematic review that identified support from managers and co-workers as critical human resources, along with professional attitude [4]. Consequently, leadership and job attitude exemplify factors that may influence the improvement of nursing performance.
Regarding support from key human resources, both authentic and shared leadership foster an empowering environment that delegates authority to nurses [5]. When nurse managers employ authentic leadership, they cultivate a high-quality work environment. This style of leadership demonstrably improves the work atmosphere, raising nursing performance levels and supporting psychological well-being in the workplace [6, 7]. At the same time, shared leadership has gained recognition as a contemporary leadership model. Shared leadership is characterized by voluntary cooperation and interaction among team members, who contribute based on their individual competencies and responsibilities [8]. This model of leadership improves staff engagement, satisfaction, and team performance, which are vital in the collaborative field of nursing [8].
Moreover, nursing performance is shaped by the interplay between individual nurses' abilities and attitudes [9]. Professional attitudes related to nursing performance, such as organizational commitment and job engagement, positively impact performance [10]. Organizational commitment in nursing significantly influences the quality of care provided, reflecting attitudes regarding job performance. Notably, individual abilities can vary, regardless of the organizational context [11]. Job engagement, another key professional attitude, also impacts nursing performance. Research on job engagement in nursing has highlighted four key attributes: vigor, dedication, absorption, and zest [12]. Thus, the role of management in fostering job engagement is vital, as it is directly correlated with organizational performance [13].
Consequently, this study aimed to explore the association of nursing performance with authentic and shared leadership styles (representing leadership characteristics) and organizational commitment and job engagement (reflecting the job attitudes of individual nurses). A variable-centered approach, specifically regression analysis, was employed to evaluate the links between these four factors and nursing performance. Such an approach is typically employed to understand the structure of variables that are consistent across individuals or to determine the relationships between variables as perceived by an average person [14]. However, this study shifts the focus from personal leadership to external leadership influences while still examining personal job attitudes. It also acknowledges the need to identify latent subgroups to achieve optimal nursing performance, as linear regression analysis primarily reveals linear relationships that correspond to changes in variables. To address this, Latent Profile Analysis (LPA) can be applied as a person-centered analytical tool. As such, this study was conducted to identify any differences in nursing performance among subgroups classified according to the four variables under investigation. This methodology was crucial, since person-centered analyses can reveal individual heterogeneity [15].
In short, the present study aimed to identify factors associated with nursing performance and to categorize latent profiles using four variables related to leadership and job attitude. We explored whether LPA can offer further insights into nursing performance-related factors that are not captured by linear regression analysis.
This study aimed to identify factors associated with nursing performance, classify potential profiles based on variables related to nursing performance, and explain the differing effects of these variables on nursing performance.
This cross-sectional correlational study aimed to identify factors associated with nursing performance.
Participants were recruited from the nursing staff at C University Hospital, located in G Metropolitan City, in southwestern Korea. The inclusion criteria were as follows: nurses who 1) worked in a ward functioning as a team and 2) possessed a minimum of 6 months of clinical experience. This minimum experience requirement aligns with the criteria used in prior research on nursing performance [16, 17]. Head nurses or unit managers were not eligible for the study. Of the 700 nurses working in wards where care is provided by a team, 520 met the inclusion criteria.
G*Power 3.1.9.7 (University of Dusseldorf, Dusseldorf, Germany) was used to determine the necessary sample size. Prior research suggested an effect size between 0.03 and 0.23 for factors influencing nursing performance [6, 11, 13, 18]. Using an average effect size of 0.15, a significance level of .05, a power of .90, and considering 14 factors-including the four study variables, age, gender, education level, marital status, position, and clinical experience, as supported by previous studies [6, 11, 13, 18]-the minimum sample size was calculated to be 194. To compensate for a potential 20% dropout rate, the recruitment target was set at 239 nurses. Ultimately, 245 of the 520 nurses consented to participate, and the data from these 245 participants were included in the analysis, although research has indicated that a minimum of 500 participants is required for sufficient accuracy of LPA [19]. The survey was conducted online at a specific time with multiple simultaneous responses, resulting in an actual participant number that exceeded the planned sample size.
The Authentic Leadership Questionnaire, originally developed by Walumbwa et al. [20] and subsequently translated by Kim, Ko, and Lee [21], was employed to assess participants' perceptions of authentic leadership by their unit managers. This questionnaire consists of 16 items divided into four domains: self-awareness (4 items), internalized moral perspective (4 items), balanced processing (3 items), and relational transparency (5 items). Participants responded using a 5-point Likert scale, with total possible scores of 16 to 80. Higher scores indicate a greater degree of authentic leadership. Cronbach's α for this instrument was .79 as reported by Walumbwa et al. [20] and was found to be .95 in the present study.
The Typology of Leadership Styles (TLS), developed by Pearce and Sims [22] and subsequently translated by Lee [23], was used to evaluate participants' perceptions of shared leadership among their nursing peers. This instrument comprises 13 items, divided into four substyles: directive leadership (3 items), transactional leadership (2 items), transformational leadership (4 items), and empowering leadership (4 items). Respondents rate each item using a five-point Likert scale, resulting in a total score that can range from 13 to 65. Higher scores indicate a higher level of shared leadership. Cronbach's α for the TLS was reported as .75 in the original study [22] and was found to be .92 in the current study.
The Organizational Commitment Questionnaire, developed by Mowday, Steers, and Porter [24] and translated by Chung [25], was applied to assess levels of organizational commitment. This questionnaire consists of 12 items, with each item rated on a five-point Likert scale. Scores can vary from 12 to 60, with higher scores denoting stronger organizational commitment. The Cronbach's α coefficient was .90 in the original study by Mowday et al. [24] and .89 in the present study.
Job engagement was assessed using the Job Involvement Scale developed by Kanungo [26] and translated by Kim [27]. This scale consists of 7 items, each rated on a five-point Likert scale. Items that carry negative connotations are reverse-scored. The total score ranges from 7 to 35, with higher scores indicating greater job engagement. Cronbach's α for the scale was .87 in the research by Kanungo [26] and .70 in the present study.
The Performance Measurement Scale for Hospital Nurses, developed by Ko, Lee, and Lim [28], comprises 17 questions rated on a five-point Likert scale. These questions are categorized into four domains: 7 questions assess nursing performance ability, 4 evaluate attitude, 3 measure willingness to improve, and 3 gauge the application of the nursing process. The total score ranges from 17 to 85, with higher scores reflecting superior nursing work performance. Cronbach's α for the scale was reported as .92 in the study by Ko et al. [28] and was also .92 in the current study.
Data were collected using Google Forms from September 7 to September 14, 2021. The online survey tool featured a mandatory response function, ensuring that all questions were answered before submission; thus, no data were missing. A researcher extended an email invitation to nurses who met the study criteria via the research hospital's intranet. Interested participants provided voluntary consent along with their cell phone numbers. Subsequently, a link to the survey was shared, and the participants completed the structured questionnaires.
Data analysis was performed using R (R Foundation for Statistical Computing, Vienna, Austria) with the median package (version 4.5.0), as well as Mplus (version 8.8; Muthen & Muthen, Los Angeles, CA, USA). Linear regression analysis was applied to investigate factors that affect nursing performance. Additionally, to identify differences in nursing performance among various groups, LPA was employed. This analysis incorporated information criteria as described in a previous study [29]. The optimal number of profiles was ascertained using the Lo-Mendell-Rubin likelihood ratio test and the bootstrap likelihood ratio test. Decreased values of the Akaike information criterion, Bayesian information criterion, and sample size-adjusted Bayesian information criterion indicated statistical significance. Furthermore, to ensure reliable profile estimation, each estimated subgroup was required to contain a minimum of 5% of the total sample size [30]. Descriptive statistics, independent t-tests, analysis of variance with Scheffe test, and Pearson correlation tests were also performed, with a p-value of less than .05 considered to indicate statistical significance.
This study received approval (CNUH-2021-275) from the Institutional Review Committee of Chonnam University Hospital in Gwangju Metropolitan City. To show appreciation for their participation, study participants were given a gift valued at approximately 3 dollars.
The average scores for authentic leadership, shared leadership, organizational commitment, job engagement, and nursing performance were 55.35±12.75, 41.79±7.14, 37.46±7.78, 21.64±3.35, and 64.40±7.64, respectively.
The general and work-related characteristics of the study are detailed in Table 1. The mean age of the participants was 29.97±5.06 years, with 225 (91.8%) being female. Regarding educational attainment, 217 (88.6%) had earned a four-year university degree. The surgical ward was the largest departmental group, representing 20.0% (n=49) of the participants. Significant differences in nursing performance were observed based on educational level (t=4.97, p=.008). Post-hoc analysis indicated that individuals with a master's degree or higher demonstrated better nursing performance compared to those with a bachelor's or professional bachelor's degree.
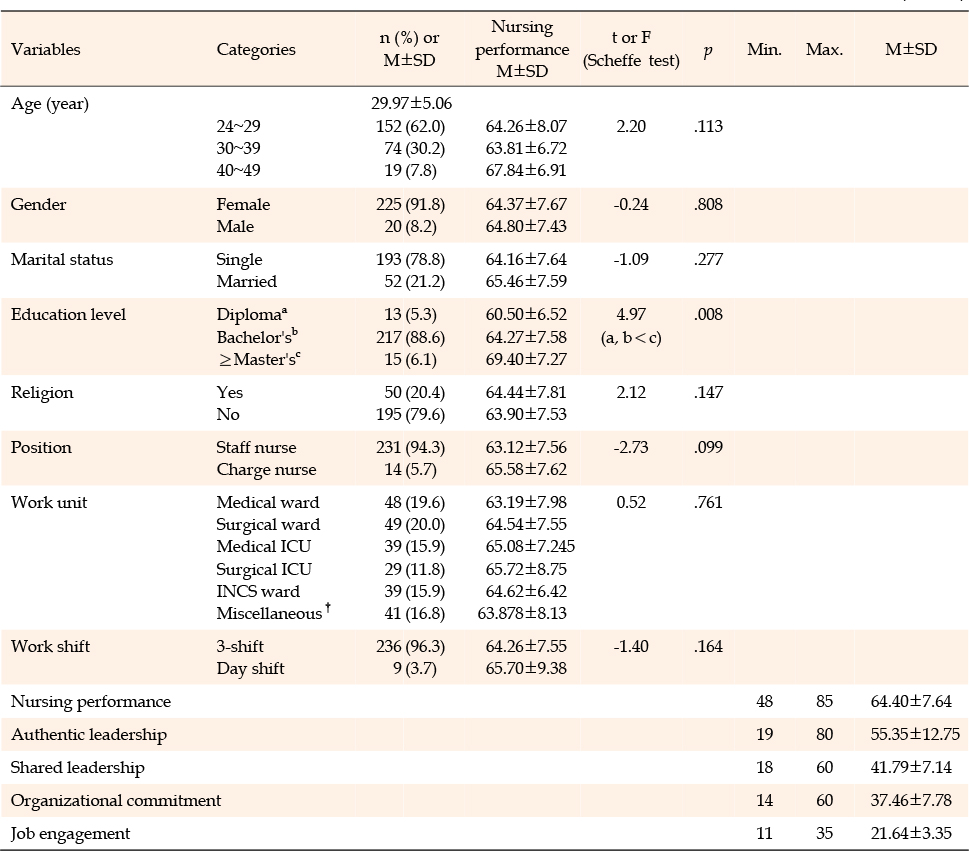
Table 1
Nursing Performance Level According to General and Job-related Characteristics and Levels of Research Varaibles (N=245)
Table 2 presents the correlations between nursing performance and various study variables. Positive correlations were observed between nursing performance and authentic leadership (r=.31, p<.001), shared leadership (r=.42, p<.001), organizational commitment (r=.37, p<.001), and job engagement (r=.25, p<.001).
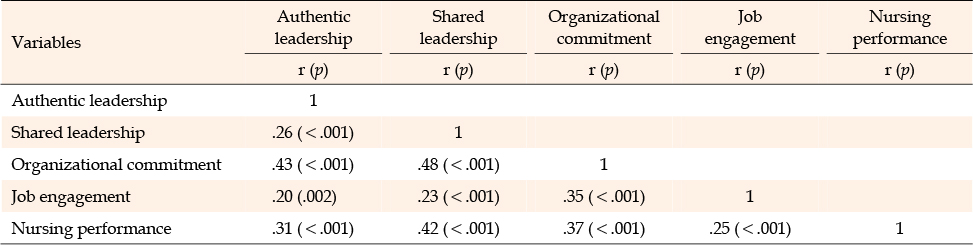
Table 2
Correlations among Main Variables (N=245)
The regression model was found to be robust (F=19.52, p<.001). Upon examining the basic assumption of multiple regression analysis, we found that the correlation coefficients among independent variables ranged from .20 to .48, with none exceeding .70. This confirmed the independence of the study variables. Tolerance limits ranged from .63 to .99, all above the threshold of 0.1. The variance inflation factor values were between 1.01 and 1.59, all below the critical value of 10, indicating no issues with multicollinearity among the independent variables. Furthermore, the Durbin-Watson test, used to assess the autocorrelation of residuals in a linear regression model, yielded a value of 2.03. This value, being close to 2, verified the absence of autocorrelation.
Shared leadership (β=.30, p<.001, 95% CI=0.21~0.51) was the most significant factor influencing nursing performance, followed by authentic leadership (β=.16, p=.009, CI=0.03~0.19) and education level (β=.15, p=.006, CI=1.55~9.25). Collectively, these variables explained 25.0% of the variance in nursing performance. However, organizational commitment (β=.12, p=.095, CI=−0.02~0.28) and job engagement (β=.10, p=.096, CI=−0.05~0.55) did not significantly impact nursing performance (Table 3).
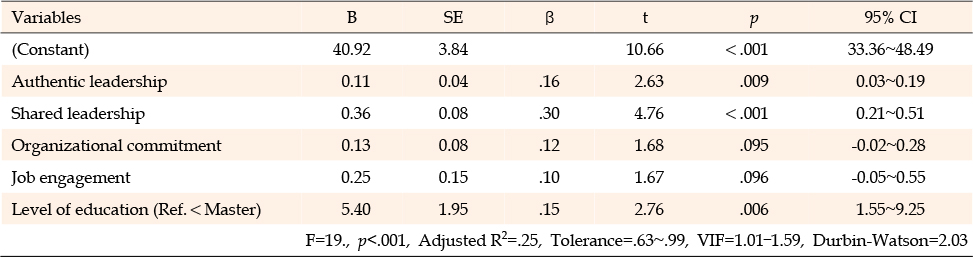
Table 3
Factors Influencing Nursing Performance Using Multiple Regression Analyses (N=245)
The analysis identified four as the optimal number of profiles, or subgroups (Table 4). Based on human resource-related and job attitude factors, these groups were designated as follows: class 1, the "best" group (n=13, 5.3%), class 2, "excellent" (n=78, 31.8%), class 3, "fair" (n=140, 57.4%) and class 4, the "worst" group (n=14, 5.7%).
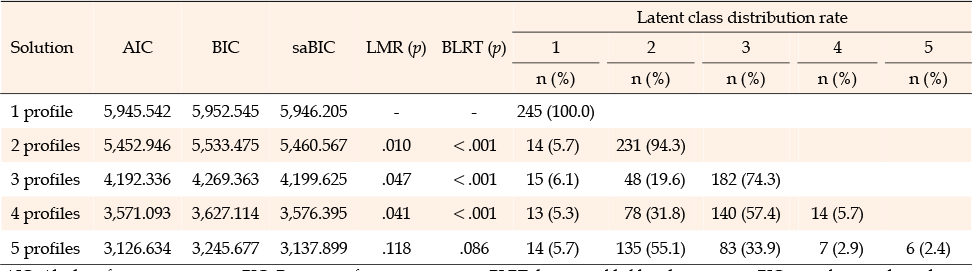
Table 4
Fit Indices, Entropy, and Model Comparisons for Five Estimated Profiles (N=245)
Across profiles, significant variations were observed in nursing performance (F=22.48, p<.001), along with differences in authentic leadership (F=39.43, p<.001), shared leadership (F=33.47, p<.001), organizational commitment (F=57.53, p<.001), and job commitment (F=27.00, p<.001). Post-hoc analysis revealed that the "excellent" and "best" groups had significantly higher scores in nursing performance and authentic leadership compared to the "fair" and "worst" groups. Regarding shared leadership and organizational commitment, the best group scored highest, followed by the excellent group, the fair group, and the worst group. Job engagement followed a similar trend, with the excellent group scoring higher than the fair and worst groups, and the best group scoring higher than the excellent group. However, no significant difference was found in education level across the latent profiles (p=.212) (Table 5).
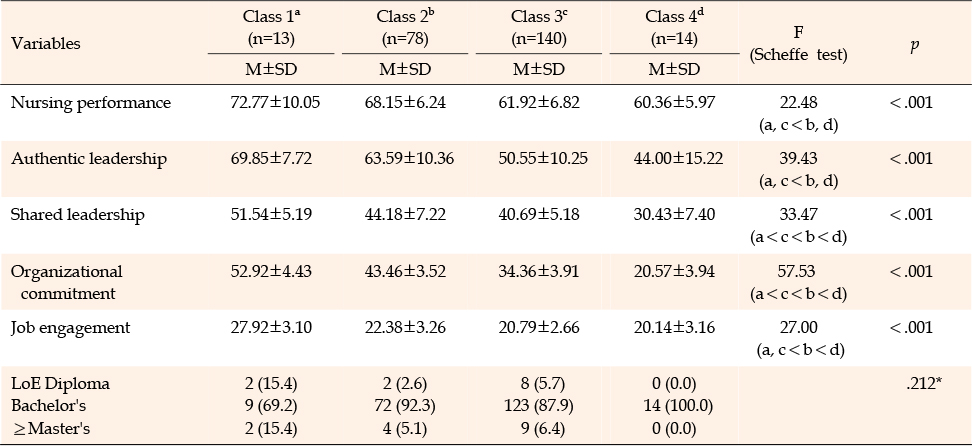
Table 5
Nursing Performance According to Profile (N=245)
In this study, we aimed to identify factors associated with nursing performance and to classify potential profiles within the context of authentic leadership by nursing unit managers, shared leadership among peer nurses, organizational commitment, and job engagement. The impact on nursing performance was examined through both variable-centered analysis and a person-centered approach, revealing minor differences between the two methodologies. LPA indicated that, among the four profiles, the groups identified as "best" and "excellent" exhibited higher nursing performance compared to the "worst" and "fair" groups, particularly regarding human resources and job attitude. Additionally, linear regression analysis demonstrated direct relationships between nursing performance and both authentic and shared leadership. For authentic leadership alone, the LPA results were consistent with the nursing performance outcomes. Education level also influenced nursing performance in the linear regression analysis, although the representation of nurses with a master's degree or higher was limited. Interestingly, no significant difference in education level was observed across profiles. This necessitates cautious interpretation, especially when considering subgroups within linear correlations and with a small sample size. The study also suggests that achieving optimal levels of human resource-related factors and job attitudes might be more efficient for improving nursing performance than merely increasing these factors. This implies a need for further exploration and discussion about the ideal levels of leadership and job attitudes required to improve nursing performance. An integrated analysis of both variable-centered and person-centered approaches could provide deeper insight into this phenomenon.
Linear regression analysis revealed that both authentic and shared leadership styles significantly impact nursing performance. The study indicates that the leadership displayed by influential figures had a greater influence on nursing performance than the participants' job attitudes. LPA indicated a similar trend regarding nursing performance, as evidenced by the authentic leadership demonstrated by the unit manager. In both variable-centered and person-centered approaches, the level of authentic leadership of the unit manager, as perceived by the nurses, was strongly correlated with nursing performance. While both previous research [6, 7] and the present study have focused on nurses' perceptions of authentic leadership by their nursing unit managers, these perceptions may differ from the nursing unit managers' subjective experiences of their leadership. Given the significant impact of authentic leadership on nursing performance [6, 7], reducing the gap between the objective and subjective experiences of authentic leadership by nursing unit managers could facilitate improvement.
The linear regression analysis conducted in this study revealed that shared leadership among peer nurses was a critical factor influencing nursing performance. However, a notable distinction was observed: while shared leadership varied across all four subgroups, significant differences in nursing performance were only evident in the two higher and two lower groups as determined by LPA. Consequently, the relationship between shared leadership among peer nurses and nursing performance was not as pronounced as the latent profiles suggested. Research on the effects of shared leadership among peer nurses on nursing performance is currently limited, with inconsistent findings. In particular, the lack of studies focusing on the performance of individual nurses highlights the need for further research in this domain. Future research should emphasize the assessment of individual nursing performance, rather than team performance [31].
In this study, organizational commitment did not emerge as a significant factor influencing nursing performance in linear regression analysis, nor did it account for the variability in nursing performance across profiles. Although previous research has identified organizational commitment as a key determinant of work performance in various settings [32], this relationship appears to be inconsistent when applied to nursing performance. This inconsistency may stem from the distinctive aspects of nursing work, which is often high-intensity, involves shift work, and is carried out by a workforce that is predominantly female and specialized in the field of nursing [33]. The variation in findings could also result from the different variables considered to influence nursing performance in various studies. Future research should prioritize the selection of predictive variables based on comprehensive literature reviews or well-established theoretical frameworks.
The linear regression analysis conducted in this study did not indicate a significant impact of job engagement on nursing performance. In contrast, LPA revealed a somewhat consistent relationship between nursing performance and job engagement. Specifically, this pattern was evident in the lower performance groups, designated as "fair" and "worst." In contrast, a different pattern was observed in the "best" and "excellent" groups, especially regarding human resource-related factors and job attitudes. In a study that employed structural modeling to examine performance among nurses in general hospitals, job engagement was found to exert no direct influence. However, a significant indirect effect was observed through organizational citizenship behavior [34]. In contrast, a direct impact of job engagement on nursing performance was confirmed in a study of nurses with more than a year of experience in operating rooms [35]. Previous research has largely indicated a direct effect of job engagement on nursing performance, particularly in situations involving elevated role burden, such as specialized duties in operating rooms and public healthcare settings. These results highlight the importance of continuing to assess the role of job engagement in nursing performance.
While this study provides valuable insights, its generalizability is limited. A serious limitation stems from the use of a smaller sample size than typically recommended for LPA. The potential for overestimation or underestimation of the relevance of certain factors is also a concern, given that the data originated from a single country and center. Comprehensive follow-up research is necessary to further explore the factors associated with nursing performance in larger and more diverse samples.
Our study revealed a strong association between the authentic leadership of nursing unit managers and nursing performance, as evidenced by linear regression analysis and LPA. These findings highlight the importance of acknowledging individual heterogeneity rather than relying on average interpretations in linear regression analysis. Future research on the determinants of nursing performance should emphasize the careful selection of variables, with a focus on theoretical grounding. Furthermore, given the observed differences in nursing performance across latent profiles characterized by human resources and job attitudes, a pressing need exists for exploratory studies to quantify the optimal levels of human resource development and job attitude improvement, rather than employing vague approaches to human resource and attitude management.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - CEJ and CJY.
analysis - CJY.
interpretation of the data - CEJ and CJY.
drafting or critical revision of the manuscript for important intellectual content - CEJ and CJY.
This article is a revision of the first author's master's thesis from Chonnam University.
 E-SUBMISSION
E-SUBMISSION