
Purpose
The purpose of this study was to develop and validate a tool to evaluate slow nursing performance for older adults in long-term care hospitals.
Methods
The search period was set from March 2013, when the term "slow nursing" was first used in the literature, to October 2021. A slow nursing tool was developed in two phases: development and verification. In the tool development phase, 29 items were developed through an extensive literature review and in-depth interviews with seven long-term care hospital nurses. Construct validity testing was performed by a 10-member expert panel, and a pilot survey was conducted on long-term care hospital nurses. In the tool validation phase, the construct validity, criterion validity, and reliability of the tool were tested by applying it to 181 nurses in long-term care hospitals .
Results
The final tool comprised five factors and 23 items, with an overall explanatory power of 56.8%. Construct validity was examined using confirmatory factor analysis, and the model fit was good. Known-group validity was established by the observation of a significant difference in the slow nursing score between intensive care unit and long-term care hospital nurses, and criterion validity was established by a significant correlation between the slow nursing and person-centered assessment scores. Internal consistency reliability was shown by a Cronbach's ⍺ coefficient of .781.
Conclusion
The concept of slow nursing has been clarified, improving the understanding and implementation of slow nursing care by nurses in long-term care hospitals. The Slow Nursing Tool for Long-term Care Hospital Nurses (SNT-LCHN) is expected to increase interest in and contribute to the effectiveness of slow nursing practices. It will serve as a valuable tool for improving nursing performance in these settings.
The purpose of this study was to develop and validate a tool to evaluate slow nursing performance for older adults in long-term care hospitals.
The search period was set from March 2013, when the term “slow nursing” was first used in the literature, to October 2021. A slow nursing tool was developed in two phases: development and verification. In the tool development phase, 29 items were developed through an extensive literature review and in-depth interviews with seven long-term care hospital nurses. Construct validity testing was performed by a 10-member expert panel, and a pilot survey was conducted on long-term care hospital nurses. In the tool validation phase, the construct validity, criterion validity, and reliability of the tool were tested by applying it to 181 nurses in long-term care hospitals.
The final tool comprised five factors and 23 items, with an overall explanatory power of 56.8%. Construct validity was examined using confirmatory factor analysis, and the model fit was good. Known-group validity was established by the observation of a significant difference in the slow nursing score between intensive care unit and long-term care hospital nurses, and criterion validity was established by a significant correlation between the slow nursing and person-centered assessment scores. Internal consistency reliability was shown by a Cronbach’s α coefficient of .781.
The concept of slow nursing has been clarified, improving the understanding and implementation of slow nursing care by nurses in long-term care hospitals. The Slow Nursing Tool for Long-term Care Hospital Nurses (SNT-LCHN) is expected to increase interest in and contribute to the effectiveness of slow nursing practices. It will serve as a valuable tool for improving nursing performance in these settings.
As of 2020, older adults account for 15.9% of the total population of Korea, and this proportion is projected to increase to 43.9% by 2060 [1]. This demographic shift is contributing to a higher prevalence of geriatric and chronic diseases, such as dementia and stroke, and is driving the demand for long-term health care services. This is reflected in the significant growth of long-term care hospitals in Korea, which have expanded since the early 2000s and reached a total of 1,468 by 2020, with an annual growth rate of 2.6% over the past five years [2]. Long-term care hospitals offer comprehensive medical services that include medical treatment, nursing, support for daily activities, and rehabilitation for chronically ill elderly patients [3]. However, many of these facilities lack a 24/7 presence of doctors, which places a heavier burden on nursing staff. This increased workload leads to a high turnover rate among nurses and challenges in recruiting new staff, ultimately compromising the quality of nursing care [4].
In particular, older adults, who constitute the majority of patients in long-term care hospitals, face numerous challenges including limited or absent mobility, a heightened risk of fractures and infections due to diminished physical function, frequent urination, incontinence, urinary retention, and decreased nerve conduction velocity. This reduction in nerve speed slows sensory response times as special sensory receptors age [5]. Therefore, it is crucial to approach care for older adults with slow and deliberate movements, particularly because they experience more pain when treated with the same speed as adult patients in general [6].
In addition, physical dysfunction in older adults adversely affects brain function, leading to cognitive decline [7] and impairing the central nervous system. This impairment can make it difficult for them to perform activities of daily living or lead to senile mental derangements. Consequently, this physical and cognitive decline can isolate older adults from society or reduce their social activities, potentially causing psychological issues such as depression and loneliness. Therefore, care for older patients should include interventions that enhance their social and psychological well-being and life satisfaction, as well as interaction-based mental health promotion programs designed to prevent cognitive decline [8, 9]. Particularly, since achieving self-integrity in the last stage of life involves reflecting on one’s past and contemplating the meaning of life, emotional support in nursing is crucial in care for older patients [9].
Older adults in long-term care hospitals often experience feelings of depression, decline, and loneliness due to provider-centered service decisions. Instead of being valued for their individuality, these patients are frequently seen merely as subjects needing life support treatment, lacking dignity, and essentially just awaiting death. In these settings, care is often administered without considering the pace of older adults, mirroring the disease-focused approach typical of acute care settings. Therefore, implementing measures to assess slow nursing performance in long-term care hospitals will not only aid nurses in understanding and adopting the slow nursing concept but also highlight its significance in delivering quality care to older patients. Moreover, through meaningful interactions with patients, nurses can provide care that allows patients to enjoy leisure and joy in life and engage actively in managing their own health. The recent rise in the older population has underscored the need for care for older patients that accommodates the physical, cognitive, psychological, and social changes in older adults, respects their individuality, and supports their sense of self-integrity. The concept of “slow nursing” exemplifies this approach by offering care paced to meet individual needs. Slow nursing focuses not merely on slowing down care but on providing comprehensive security tailored to each patient. This involves paying close attention to their well-being and observing their environment and social interactions without the constraints of time. Characteristically, slow nursing aids patients in self-care and fosters interactive care, enabling them to find comfort and pleasure in life [10].
As discussed earlier, slow nursing bears similarities to “respectful nursing” by prioritizing individual needs and upholding the patient’s human dignity [11, 12]. What sets slow nursing apart is its innovative approach of adjusting the pace of care to match the older patient’s physical, cognitive, and emotional slowdowns. This approach places significant emphasis on rebuilding self-confidence and enriching life by engaging patients in reflecting on life’s meaning. This concept is highly regarded within the field of nursing. Specifically, the reflection on life’s meaning, a key element of slow nursing, is an invaluable and essential aspect of care. It helps older patients find meaning in their lives, fostering feelings of joy and satisfaction in their current circumstances, and supports them in achieving self-integrity, a critical developmental goal in later life.
“Slow nursing” is a relatively new concept that has not been extensively studied. Previous research has shown that it has a positive impact on older patients with dementia by helping them maintain their daily routines, personal identities, sensory experiences, and providing them with a sense of belonging, joy, meaning in life, and emotional comfort [13, 14]. These findings suggest that slow nursing plays a crucial role in the care of older patients. Despite this, there is a notable lack of empirical research on the effects of slow nursing on this demographic, with existing studies primarily focusing on qualitative research or conceptual analysis. In particular, no studies have specifically explored the extent of slow nursing implementation among older patients who require such care, nor is there a tool available to measure the level of implementation. Therefore, developing a tool to assess the implementation level of slow nursing would provide valuable data for further research in this area. This study aimed to develop and validate a psychometric tool to assess the extent to which slow nursing is provided to older adults in long-term care hospitals.
This study employed a methodological design to develop a tool for assessing the level of slow nursing care provided to older patients in long-term care hospitals, and to verify its validity and reliability.
The process of developing and validating a slow nursing tool, designed to measure the extent of slow nursing care provided to older patients in long-term care hospitals was divided into two phases: tool development and validation, following the methodology proposed by DeVellis [15]. Initially, during the tool development phase, factors related to slow nursing performed by nurses in long-term care hospitals were identified through a literature review and in-depth interviews. Based on these factors, preliminary items were formulated, and the preliminary tool was refined after testing for content validity by an expert panel. Subsequently, in the tool validation phase, a main survey was administered to nurses in long-term care hospitals. Following the confirmation of the tool’s validity and reliability, the Slow Nursing Tool for Long-term Care Hospital Nurses (SNT-LCHN) was finalized and validated (Figure 1).
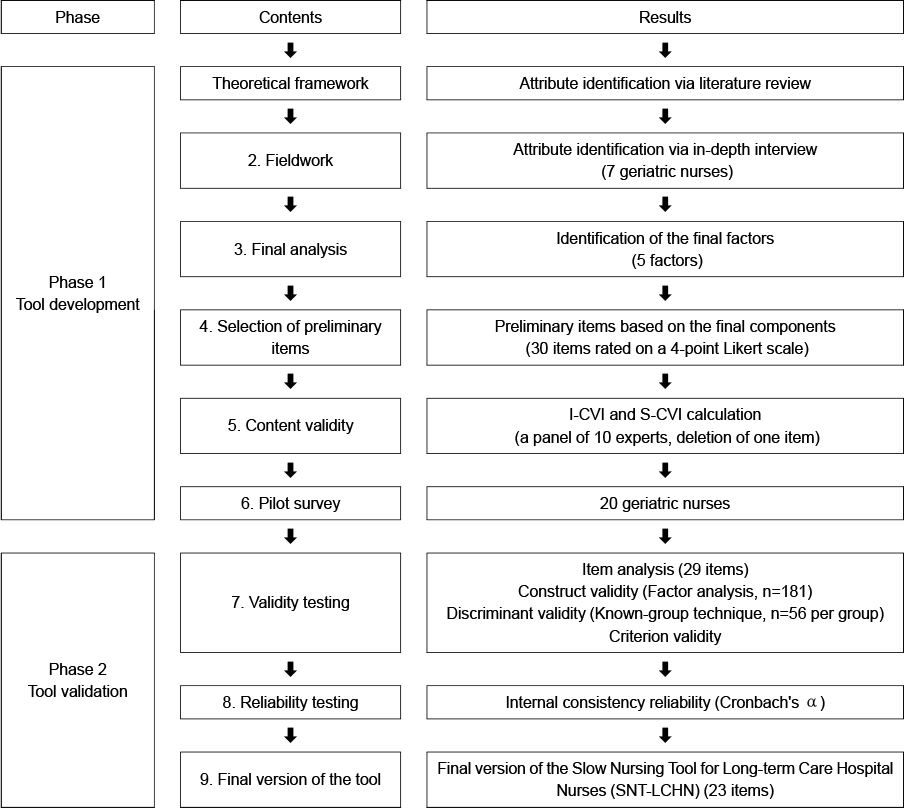
Figure 1
Tool development process flowchart.
To define the attributes of slow nursing provided to older patients in long-term care hospitals, a literature search was conducted across five databases: PubMed, DataBase Periodical Information Academic (DBPia), Google Scholar, National Digital Science Links (NDSL), and Research Information Sharing Service (RISS). The search utilized keywords such as “slow,” “slow nursing,” “slow medicine,” and “slow treatment.” The timeframe for the search spanned from March 2013, marking the initial mention of slow nursing, to October 2021. Out of the 17,953 articles and theses initially retrieved, 521 papers were selected for review after excluding 17,432 papers that lacked relevance in terms of slow nursing attributes, definitions, related concepts, similar terms, and antecedents. Following a quality evaluation of the literature, 91 papers were retained for further consideration. An additional 53 documents were subsequently removed for being irrelevant to slow nursing, leaving 38 papers for detailed review. From these, five attributes of slow nursing were identified [16].
The first attribute of slow nursing is “accommodating the patient’s pace” which involves not only adjusting the pace of nursing to suit the patient’s condition but also providing care in a calm, careful, and patient manner, while attentively observing the patient’s responses without the pressure of time constraints [12, 13, 14]. This attribute highlights the importance of the nurse’s demeanor; a nurse who appears rushed can cause patients to feel anxious and reluctant to communicate their needs, complicating the nurse’s ability to understand and address these needs effectively. Therefore, it is crucial to allocate ample time for patient care, matching the pace to the patient’s needs and prioritizing various needs to enhance care efficiency [17]. Specifically, slow nursing does not mean uniformly slow care but rather adjusting the pace based on the nature and urgency of the required care. This approach allows slow nursing to be more effective in alleviating patient issues by improving the efficiency of time allocation and priority setting [18].
The second attribute of slow nursing is “carefulness.” Patients in long-term care hospitals typically present with multiple, rather than singular, health issues, and their complex physical conditions can lead to anxiety and stress, which may exacerbate emotional health problems. Therefore, nurses in these settings must meticulously assess both the physical and emotional challenges faced by their patients. Considering that most patients in long-term care hospitals are receiving prolonged inpatient treatment, it is also crucial to evaluate and manage environmental factors to create a conducive recovery atmosphere [7, 19, 20]. This comprehensive approach requires close observation and accurate identification of all issues, embodying the principle of “carefulness” essential to slow nursing.
The third attribute of slow nursing is “comfort in the process,” which prioritizes the patient’s comfort throughout the care process to improve their physical well-being [18, 19]. This approach underscores nurses’ efforts to maximize patient comfort, involving attentive listening while administering care. Such attention can significantly motivate patients to engage more actively in their own healthcare and to place greater trust in their nurses.
The fourth attribute of slow nursing is “participation,” which emphasizes engaging the patient in the nursing process to enhance their self-care capabilities by utilizing the broadest possible range of physical activities. Similarly to how patients with dementia or stroke are encouraged to feed themselves using utensils despite limited dexterity, prompting long-term care hospital patients to engage in the nursing process is an effective method for helping them overcome or prevent the worsening of illness-related physical limitations in a self-directed manner [20].
The fifth attribute of slow nursing is “consideration of the meaning of life,” which involves an interactive approach that encourages patients to reflect on their life’s significance [13, 14]. Slow nursing emphasizes quality of life and strives to enhance patients’ quality of life by engaging with each individual and applying all relevant practical knowledge with dedication, creativity, and intuition [12]. Research has shown that slow nursing, through its interactive engagement between nurses and older patients, fosters joy and well-being by enabling patients to revisit and contemplate their life’s meaning [21]. Considering that “consideration of the meaning of life,” as the fifth attribute of slow nursing, is pivotal for achieving self-integrity-a significant developmental task in old age-it is deemed an essential aspect of nursing care for older patients in long-term care facilities.
This study reaffirmed the attributes of slow nursing through in-depth interviews with seven long-term care hospital nurses over a one-month period beginning April 7, 2021. Seven long-term care hospitals in Daegu and Gyeongsangbuk-do, recognized for their dignified care embodying the principle of humanitude, were selected for participation after completing necessary administrative procedures and obtaining approval. Following permission to proceed with the study, the heads of the nursing departments identified nurses who had positive experiences with slow nursing in practice to participate in the study. The number of nurses recommended and the number of those who declined participation were kept confidential from the participants. The demographic characteristics of the interviewees were as follows: the average age was 48 years; 85.7% were female; 42.8% held an associate degree, while 57.1% had obtained a bachelor’s degree or higher. The average clinical career spanned 14.28 years, with 6.28 years of experience specifically in long-term hospital care. The one-on-one in-depth interviews continued until saturation was reached, with no new information emerging. Each interview lasted between 50 and 70 minutes.
The main question posed during the in-depth interviews was, “What do you think slow nursing is?” This was supplemented by several sub-questions, including: “Tell me about your experience with slow nursing,” “What do you think is the most important factor in slow nursing?” “When do you think slow nursing is needed?” and “What may be obstacles to performing slow nursing?” among others. The interviews were recorded and promptly transcribed, and the key concepts and attributes were identified through a thorough comparison and analysis of the data, following the content analysis methodology proposed by Krippendorff (2004) [22].
In the in-depth field interviews, seven attributes were identified that demonstrate respect for the patient: accommodating the patient’s pace, sensitivity to changes in their condition, involving the patient in treatments or activities, prioritizing the patient’s well-being during nursing care, understanding the patient’s emotions, engaging in listening and light physical contact, and reminiscing about the patient’s life.
An analysis of the in-depth interviews confirmed that all attributes identified in the literature review were reflected in the interviewees’ statements. These included “respect for the speed of the subject,” emphasizing adaptation to each patient’s pace; “carefulness,” which involves observing not only the physical but also the emotional and environmental conditions of patients; “comfort in the process,” prioritizing patient comfort throughout the care process; “participation,” encouraging active patient involvement in the nursing process to boost their self-care capabilities; and “consideration of the meaning of life,” offering patients a chance to reflect on their lives through interaction. The attributes of slow nursing also mentioned in in-depth interviews were as follows: patients’ emotional comfort and nurses’ language, gestures, and facial expressions that make the patients feel respected, such as “making eye contact when talking to a patient,” “carrying on a conversation with respect using honorifics,” “listening to the same story with attention and responding as if hearing it for the first time,” “explaining nursing activities to patients before performing them”, and “giving praise.”
In the stage of preliminary question construction, we integrated the results from a literature review and in-depth interviews to identify five key attributes: respecting the subject’s speed, carefulness, comfort in the process, participation, and consideration of the meaning of life. In the final stage of confirmatory factor analysis, the attributes of slow nursing identified among long-term hospital nurses included accommodating the patient’s pace, encouraging observation and participation, promoting comfort, respect, and reminiscing about the patient’s life. These five attributes, including respect, were derived.
Five factors contributing to slow nursing were identified through a literature review and in-depth interviews. These include “adapting to the patient’s pace,” “encouraging observation and participation,” “providing comfort,” “showing respect,” and “bestowing value on life.”
The first factor, “adapting to the patient’s pace,” was derived from the attribute “respect for the speed of the subject,” which emerged from both the literature review and in-depth interviews. The second factor, “encouraging observation and participation,” combines attributes from various sources. “Carefulness” and “sensitivity to the patient’s changing condition,” identified through concept analysis and in-depth interviews respectively, emphasize the importance of attentively monitoring the patient’s condition. Additionally, “participation” and “inducing patients to participate in treatments or activities,” also from concept analysis and interviews, highlight the need to encourage patients to actively engage in treatments and activities by assessing their capabilities through therapeutic communication and motivating them to utilize their remaining abilities to the fullest extent. The third factor, “providing comfort,” was formulated from the attribute “comfort in the process,” identified in the concept analysis. The fourth factor, “showing respect,” encompasses attributes identified solely in in-depth interviews (not extracted from the literature review) and reflects considerations and respect for long-term care hospital patients. This includes behaviors such as “carrying on a conversation with respect using honorifics” and “listening to the same story with attention and responding as if hearing it for the first time.” The fifth factor, “bestowing value on life,” was developed by combining the attributes “consideration of the meaning of life” and “looking back on life,” which were derived from both concept analysis and in-depth interviews.
From an initial set of 67 items derived from a literature review and in-depth interviews, 30 items were ultimately selected. This selection involved removing, correcting, or supplementing items with unclear content, with the assistance of two experts who each have over 25 years of experience in tool development, and a professor of geriatric nursing. Each of the five factors was represented by six items.
To prevent centralization of respondents’ answers and a decrease in reliability due to fatigue, each response was rated using a 4-point scale proposed by Lynn [23]. The scale ranges from 1 (not relevant) to 4 (very relevant), with higher total scores indicating a greater degree of implementation of slow nursing.
A 10-member expert panel was established to assess the content validity of a preliminary tool. This panel included two geriatric doctors, two geriatric nursing professors, three geriatric nurses from long-term care hospitals, and three general nurses with at least 10 years of experience in long-term care hospitals. The panel members were given a questionnaire to rate the content validity of 30 preliminary items. According to the evaluation criterion requiring an overall item-level content validity index (I-CVI) of .78 or higher [22], 29 final preliminary items were selected after the removal of one item, “I perform one nursing care task at a time” (I-CVI=.70). The concept of performing “one task at a time” was intended to emphasize the need for a 1:1 nurse-to-patient ratio in monitoring and interacting with patients [12]. However, the experts determined that this did not accurately reflect the realities faced by nurses in Korean long-term care hospitals.
The initial version of the tool was linguistically improved by a PhD in Korean literature, who was consulted to improve sentence flow and term accuracy, and to correct ambiguous expressions and distortions in meaning.
Prior to the main survey, a pilot survey was conducted using the preliminary tool to assess the comprehensibility of the items and the time required to complete the questionnaire. In line with DeVellis’s recommendation that a suitable sample size for a pilot survey ranges from 20 to 40 [24], the pilot survey was administered to 20 nurses, each with at least one year of direct work experience in long-term care hospitals. The feedback from this pilot survey was used to evaluate and adjust the appropriateness of the items. Although no items were requested to be removed during the preliminary survey, additional explanations were provided for questions that necessitated a more detailed understanding of the content, using examples from potential scenarios in a nursing hospital setting. The time to complete the questionnaire varied from 3 to 12 minutes.
The validity and reliability of this tool were established through various methods. Item analysis, exploratory factor analysis, and confirmatory factor analysis were performed to assess construct validity, convergent and discriminant validity, known-group validity, and criterion validity. Additionally, reliability tests were conducted.
The inclusion criteria for this study were nurses who had at least one year of direct experience caring for older adults in long-term care hospitals and who understood the study’s purpose and provided informed consent after receiving explanations about the study. Nurses responsible for management and administration, who did not directly perform patient care, were excluded from this study.
A total of 195 nurses from eight long-term care hospitals participated in the main survey. The participant count was determined based on the recommendation that the minimum sample size for stable tool reliability and validity testing should be five times the number of items [25], considering a potential dropout rate of 10%. After excluding 14 questionnaires due to insufficient responses, 181 respondents were included in the analysis.
The convergent validity of the tool was estimated using standardized factor loadings, Critical Ratio (CR.), Average Variance Extracted (AVE), and Construct Reliability (CR). Discriminant validity was assessed by calculating the difference between the square root of the AVE value and the correlation coefficient. To employ the known-group technique, two distinct groups of nurses were chosen: nurses from long-term care hospitals experienced in slow nursing, and Intensive Care Unit (ICU) nurses from tertiary hospitals, who manage critically ill patients with acute diseases where slow nursing is impractical. The minimum required sample size for each group was determined to be 51, calculated using G*Power 3.197 for the t-test. This calculation was based on an effect size of 0.5 (moderate magnitude), a significance level of 0.05, and a power of 0.80. Considering a potential dropout rate of 10.0%, 56 nurses from long-term care hospitals (randomly selected from 181 who participated in a survey for reliability and validity) and 56 nurses with at least one year of direct ICU patient care experience from two tertiary hospitals were selected, making a total of 112 nurses.
The criterion validity of the preliminary tool was evaluated by determining its correlation with the Korean version of the Person-centered Care Assessment Tool (P-CAT), which was developed by Edvardsson, Sandman, and Rasmussen [26] and adapted for long-term aged care facilities as the K-P-CAT [27]. This self-report tool comprises 23 items, organized into five domains, each rated on a 5-point Likert scale. Permission for its use was secured from the original authors. In the study conducted by Tak et al., Cronbach’s α was reported as .86 [27].
This study received approval from the Keimyung University Institutional Review Board (approval number: 40525-202101-HR-089-02). Due to COVID-19 restrictions, external access to nursing hospitals was prohibited. Consequently, one data collector from each nursing hospital was selected, and each was thoroughly briefed on data collection methods, personal information protection, potential risks of information exposure during the data collection process, and the importance of voluntary participation and informed consent. Researchers visited long-term care hospital nurses at their workplaces to recruit participants who met the selection criteria. Nurses who agreed to participate signed consent forms after being informed about the research purposes and methods. The survey was conducted in a private space within the hospital, such as the nurse’s personal area, to maintain confidentiality and protect the personal information of the research subjects. To further ensure confidentiality, the data collector provided the consent forms and questionnaires separately, allowing the subjects to manage these documents themselves. Participants were instructed to complete the questionnaire, seal it in an envelope, and return it to the data collector. As a gesture of appreciation, all participants received a small gift immediately after completing the survey. Each questionnaire was distributed in a sealed envelope and remained sealed after collection. Data collection occurred from July to August 2021.
The collected data were analyzed using the SPSS version 26 program. Participants’ general characteristics were examined through descriptive statistics. The construct validity of the developed tool was evaluated by an expert panel and determined by the resultant I-CVI scores. Additionally, the construct validity was assessed through item analysis, factor analysis, convergent validity, and discriminant validity. Item analysis included examining the normality of distribution through standard deviation, mean, skewness, kurtosis, response distribution by item, and item-total correlation. In the item-total correlation analysis, items with a value of 0.30 or less were reviewed. Construct validity was further assessed by performing exploratory factor analysis, with the suitability of this analysis determined by the Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s sphericity test. Factors were extracted using principal component analysis with varimax rotation, which is advantageous for extracting appropriate factors while maintaining independent correlations. The number of factors was determined based on a minimum eigenvalue of 1.0, and factors and items were finalized through confirmatory factor analysis. To assess known-group validity, an independent samples t-test was conducted, and the correlation between the total score of the tool and the extracted items was analyzed. Criterion validity was evaluated using the correlation coefficients between the SNT-LCHN developed in this study and the K-P-CAT. The internal consistency reliability of the tool was assessed by calculating the Cronbach’s α value.
The mean age of the participants was 49.99 years, with those aged 50 and over accounting for 42.5%. Most of the participants were women (91.2%), and 50.3% were not religious. Those with an associate degree slightly outnumbered those with a bachelor’s degree or higher (54.1% vs. 45.9%). General nurses far outnumbered charge or head nurses (71.8% vs. 28.2%). The mean clinical experience was 18 years, and participants with 20 years or more of experience accounted for the highest proportion (38.7%). Those with less than 5 years of long-term care hospital work experience accounted for 42.5% of the participants, followed by those with 10 years or more of experience (33.7%) (Table 1).
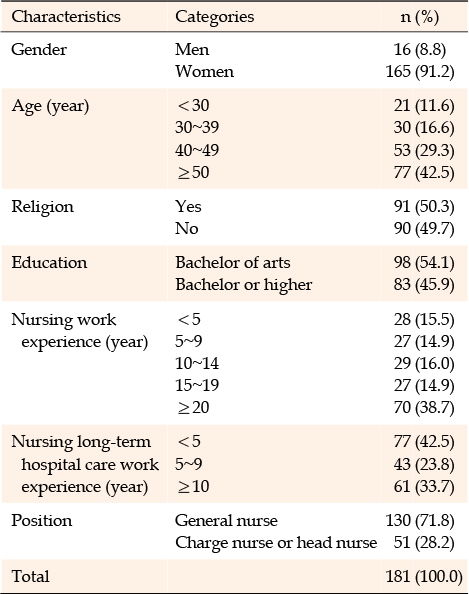
Table 1
Participants’ Demographics (N=181)
An analysis of the 29 items in the tool revealed mean item scores ranging from 2.42 to 3.42 and standard deviations from 0.56 to 0.82. The absolute values of each item’s skewness and kurtosis ranged from −0.66 to 0.31 and from −0.68 to 0.61, respectively, all below the threshold of 2, confirming normality. The correlation coefficient between individual items and the total score varied from 0.35 to 0.71, satisfying the minimum required absolute value of 0.30 (Table 2). The tool’s appropriateness and comprehensiveness were further supported by the observation that the floor/ceiling effects for all items were below 30.0%, as determined by analyzing the frequency (%) of items scoring at the minimum and maximum levels.
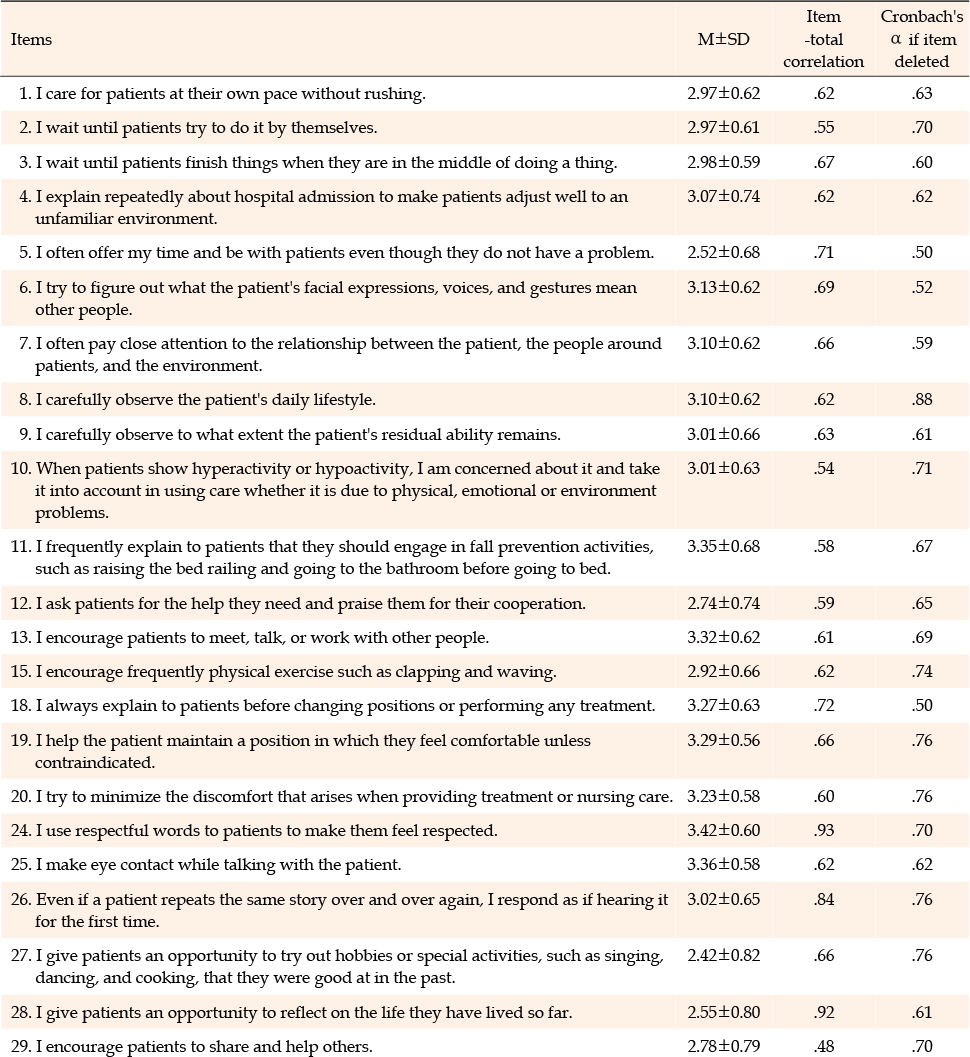
Table 2
Item Analysis
In Exploratory Factor Analysis (EFA), the criteria for determining the number of factors included an eigenvalue of at least 1.0, a commonality of 0.40 or higher, and a factor loading of 0.50 or more [25]. Six items-numbers 14, 16, 17, 21, 22, and 23-that loaded on two factors were removed. The ranges for commonality and factor loading were 0.46 to 0.74 and 0.51 to 0.89, respectively. Item 1, which initially showed a factor loading below 0.5 in the first factor analysis, was reanalyzed and subsequently reincluded because it embodies the core attribute of “slow nursing,” despite its factor loading of 0.417 falling below the threshold of 0.5. As a result, the final version of the SNT-LCHN comprises a total of 23 items (Appendix 1).
In the KMO and Bartlett’s sphericity test, conducted to assess the suitability of the items for factor analysis, a KMO value of 0.82 was achieved, and the results of Bartlett’s sphericity test were also significant (χ2=1,472.09, p<.001). These results confirm that the items are appropriate for factor analysis. The factor analysis identified five factors that together explained 56.8% of the total variance: factor 1 “adapting to the patient’s pace” (7 items, explanatory power=10.9%); factor 2 “encouraging observation and participation” (7 items, explanatory power=26.2%); factor 3 “providing comfort” (3 items, explanatory power=6.9%); factor 4 “showing respect” (3 items, explanatory power=6.6%); factor 5 “bestowing value on life” (3 items, explanatory power=6.0%%) (Table 3).
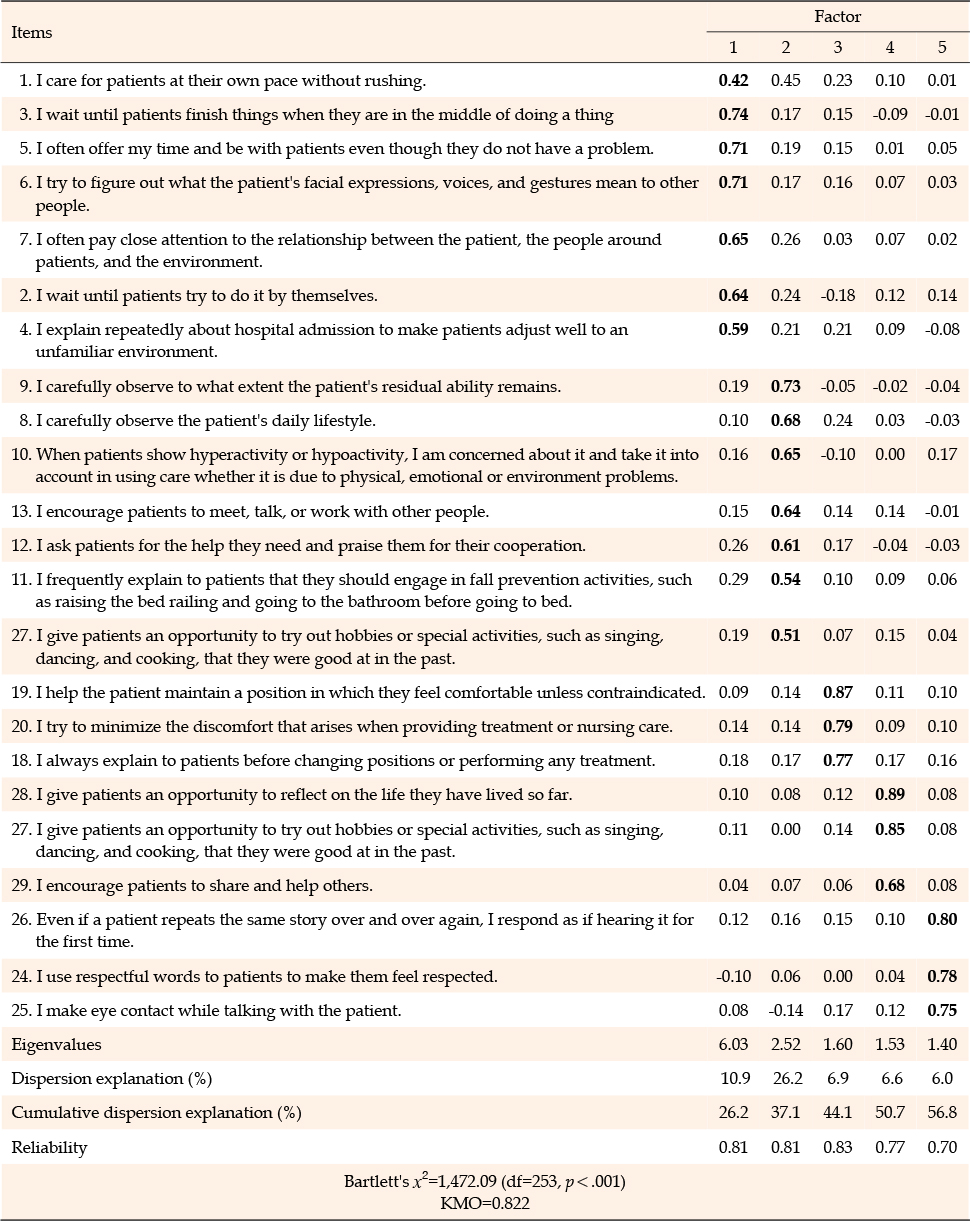
Table 3
Exploratory Factor Analysis of Slow Nursing Measures of Long-term Hospital Care Nurses
Confirmatory Factor Analysis (CFA) was conducted on the items of the initial hypothetical model derived from EFA. The results showed that the representative model fit indices met the required standards. Absolute fit measures were calculated at 1.29, significantly meeting the cut-off value of <3 at the p<.001 level, thus confirming the model fit at the p<.05 level [28]. The model demonstrated an appropriate fit, as indicated by the following indices: root mean square error of approximation=.039, root mean square residual=.06, Tucker Lewis index=.97, comparative fit index=.98, incremental fit index=.98, normed fit index=. 90, goodness of fit index=.88, and adjusted goodness of fit index=.85. Overall, the fit of the measurement model, which includes both latent variables (factors) and observed variables (measurement items), was deemed appropriate.
The construct validity of the tool was established by assessing the convergent and discriminant validities of the items (Table 4). The assessment of convergent validity showed that the standardized factor loadings (λ) for all items, except item 26 (.37), exceeded the recommended threshold of .50, and the C.R. for each item surpassed the cut-off value of 1.97. The relatively low standardized factor loading for Item 26, “Even if a patient repeats the same story over and over again, I respond as if hearing it for the first time,” may be attributed to its less frequent implementation in clinical settings compared to simply listening, as it involves attentively listening to a patient’s repeatedly told story and explaining the situation in easy-to-understand terms. Given that this item is specifically relevant to the care of long-term care hospital patients with dementia and received a high CVI score of .85, it was included in the factor “showing respect.” With the reliability of all items except item 26 exceeding the cut-off value of .70, the convergent validity of the 23 items of SNT-LCHN was confirmed. Similarly, the discriminant validity analysis, aimed at confirming the low correlations and independence between latent variables, demonstrated that the square of the correlation coefficient between all latent variables was smaller than the AVE value, thereby establishing the discriminant validity of the tool.
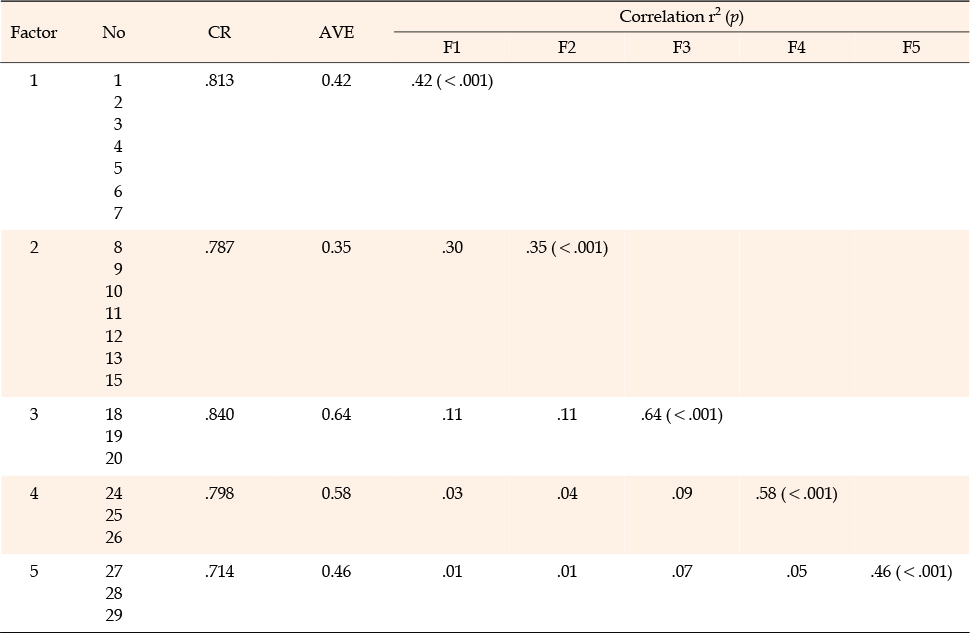
Table 4
Convergent and Discriminant Validity
The known-group validity of the tool was assessed by evaluating its ability to discriminate between different groups. In a comparison of slow nursing implementation, nurses from long-term care hospitals scored higher on average than their counterparts in tertiary hospital ICUs, with statistically significant results: 3.13 (0.33) vs. 2.50 (0.36) (t=9.75, p<.001). When broken down by factor, the long-term care hospital nurses significantly outscored the ICU nurses in all domains as follows: “adapting to the patient’s pace” (3.01 [0.41] vs. 2.42 [0.45]; t=7.19, p<.001), “encouraging observation and participation” (3.17 [0.39] vs. 2.49 [0.47]; t=8.39, p<.001), “providing comfort” (3.38 [0.44] vs. 3.01 [0.41]; t=4.66, p<.001), “showing respect” (3.44 [0.44] vs. 2.65 [0.60]; t=7.93, p<.001), and “bestowing value on life” (2.73 [0.66] vs. 2.00 [0.59]; t=6.12, p<.001). These findings confirm the known-group validity of the SNT-LCHN, as the statistically significant differences in slow nursing scores between the long-term care hospital and ICU nurse groups align with the theoretical expectations of varying degrees of implementation of slow nursing.
Given the particular importance of slow nursing for older patients, the criterion validity of the SNT-LCHN was evaluated by examining its correlation with the K-P-CAT, which was validated by Tak et al. (2015) for workers in long-term aged care facilities. The analysis revealed a statistically significant positive correlation between the SNT-LCHN and the K-P-CAT (r=0.43, p<.001), thereby confirming the criterion validity of the SNT-LCHN.
In the reliability testing based on internal consistency, Cronbach’s α for the tool (23 items) was 0.78. The values for each factor were as follows: 0.81 for “adapting to the patient’s pace,” 0.79 for “encouraging observation and participation,” 0.83 for “providing comfort,” 0.77 for “showing respect,” and 0.70 for “bestowing value of life.” Since the Cronbach’s α values for all five factors and the entire tool exceed 0.70, which is considered an acceptable level of reliability for a new tool [25], the reliability of SNT-LCHN was established.
To test the stability of the instrument over time, test-retest reliability was evaluated among 181 nurses from nursing hospitals who participated in the questionnaire for instrument development. The retest occurred three weeks after the initial test, based on the recommendation that an interval of 2 to 4 weeks is suitable, as it typically diminishes the memory of the first test [28]. The test-retest reliability of the SNT-LCHN was confirmed with a high Cronbach’s α value of .829.
This study derived attributes of slow nursing through a literature review and in-depth interviews. Based on these attributes, it developed a tool for measuring slow nursing care among long-term hospital nurses. The conceptual attributes of slow nursing identified from the literature analysis included five key elements: respect for the subject’s speed, carefulness, comfort, participation, and contemplation of the meaning of life. In the in-depth field interviews, seven attributes were derived: accommodating the patient’s pace, sensitivity to changes in their condition, involving the patient in treatments or activities, prioritizing the patient’s well-being during nursing care, understanding the patient’s emotions, engaging in listening and light physical contact, and reminiscing about the patient’s life.
In the phase of preliminary item construction, we integrated the results of a literature review and in-depth interviews to identify five key attributes: respecting the subject’s speed, carefulness, comfort in the process, participation, and consideration of the meaning of life. This study identified attributes of slow nursing through a literature review and in-depth interviews. These attributes were then used to develop a tool for measuring slow nursing care among nurses in long-term care hospitals. The resulting tool comprises five factors and 23 items designed to assess the level of slow nursing care provided to older patients in long-term care hospitals. The tool’s reliability and validity were confirmed by calculating Cronbach’s α (.781) and evaluating both construct and criterion validity. This validation supports the tool’s effectiveness, designated as SNT-LCHN, in measuring slow nursing implementation by long-term care hospital nurses.
The most important element in tool development is testing the tool’s validity and reliability through theoretically and methodologically sound processes. In this study, preliminary tool items were developed based on a literature review and in-depth interviews focused on slow nursing. The content validity of these items was then evaluated by a 10-member expert panel. After receiving detailed explanations of the slow nursing concept and the study’s objectives, the panel members rated the suitability of each item.
The construct validity of SNT-LCHN was established by performing EFA and CFA. The EFA of the 23 items identified five factors: “adapting to the patient’s pace,” “encouraging observation and participation,” “providing comfort,” “showing respect,” and “bestowing value on life.” The model’s fit was confirmed by calculating representative model fit indices, which met the recommended levels. Additionally, the CFA was conducted to assess the convergent and discriminant validity of SNT-LCHN. Here, construct validity was supported by high correlations between items within each factor and clear independence among the factors. The five factors identified by the EFA account for 56.82% of the total variance: Factor 1 “adapting to the patient’s pace”; Factor 2 “encouraging observation and participation”; Factor 3 “providing comfort”; Factor 4 “showing respect”; Factor 5 “bestowing value on life” (Table 3). Each factor and its corresponding items are detailed below.
Factor 1: These results align with Bachmann’s study [18], which emphasized that slow nursing enhances patient care by balancing speed. Lillikroken [10] identified three attributes of slow nursing for dementia patients: “this moment,” “one thing at a time,” and “creating joy and meaning.” The practice of adjusting to the patient’s pace falls under “one thing at a time,” encompassing actions such as slowing down, not rushing, allowing patients the time they need, and avoiding unneeded work, stress, and noise. This study’s inclusion of questions about slowing down and not rushing suggests a strong alignment with the core principles of slow nursing. Elst, Casterle, and Gastmans [30] noted that although nursing tasks in hospitals are diverse and numerous, spending time with patients is paramount. The most effective approach is to provide care at the patient’s pace without rushing.
Factor 2: Carlson and Bengtsson [31] observed that changes in a patient’s condition should encompass not only physical alterations and shifts in daily habits but also changes in their relationships with other patients and medical staff, which require meticulous observation. Bedin et al. [32] highlighted that a nurse’s role in a nursing home involves understanding patient emotions, making clinical judgments from various data, and observing behaviors like elopement, abuse, and refusal to bathe, to implement individualized care. This approach aligns with the “encouragement of observation and participation” factor identified in this study. Lillikroken [29] argued for the importance of stimulating the imagination and engaging patients in meaningful, creative activities, reflecting the slow nursing characteristics identified in this study.
Factor 3: Lillikroken’s [10] study on slow nursing in dementia patients identified attributes such as “this moment,” “one thing at a time,” and “creating joy and meaning.” The practice of focusing on “this moment” helps patients become aware of their current reality, alleviating dangers, social isolation, or discomfort. Given that many patients in nursing hospitals have diminished cognitive functions, explaining details like the current season, time, personal information, treatment, and purpose of activities in advance is crucial to prevent strong adverse reactions. Attention must also be given to “promoting comfort” [33], as many patients struggle with physical activities.
Factor 4: Among the three attributes derived from research on the meaning of slow care for dementia patients [10, 21, 29], this factor can be seen as belonging to the “creating joy and meaning” attribute. Allowing patients to participate in pleasant and meaningful activities helps them not only to achieve physical well-being, but also to develop a strong sense of self and solid identity, as well as a sense of coherence. In particular, these actions are characterized by expandability in the sense that they are performed not just for one’s own sake, but also to find ways to help others or those who are currently weak. Lillikroken’s [29] study of dementia patients found that consistent meaningfulness occurs when people think that what is required of them is reasonable for their time and energy; thus, it is possible to provide nursing care that allows dementia patients to recall past times and give meaning to them. Korean older adults find meaning in life through interpersonal relationships and daily life, and in the process of contemplating the meaning of life, they regain confidence and evaluate their own value positively [34]. Many older adults exhibit reduced cognitive ability, and it is important to maintain daily life well nonetheless. Therefore, by creating and applying programs that allow patients to participate in all treatment activities, the patient’s self-integration can be improved. This approach can increase awareness and improve treatment effectiveness [9]. Of note, providing the opportunity for patients to try activities they used to like and were good at, such as knitting, cooking, calligraphy, tending flowers, and listening to music, can help them regain confidence, reminisce about life, and ponder the meaning of life. Engaging dementia patients in meaningful activities, such as work or cultural activities related to household activities, also helps patients feel comfortable. The nurse’s creativity and intuitive sense of what makes patients feel comfortable and what resources can be utilized to create meaning are essential [35]. This allows one to recall past positive life experiences through meaningful activities, ponder the meaning of life, and give value to life.
Factor 5: Dignity care is crucial for nursing home residents because disrespectful or even violent service providers in nursing homes can pose physical threats to dependent patients who do not live with their families [36]. Since personality is maintained through relationships with others, it is absolutely necessary to provide good nursing care with respectful interactions between nurses and patients with dementia [13]. All human beings possess dignity, and this absolute dignity should never be harmed or destroyed; therefore, the dignity of dependent patients hospitalized for long periods of time in nursing hospitals should be actively protected not only by service providers but also by society as a whole Edlund [37].
In this study, the mean slow nursing score for nurses in long-term care hospitals was 3.13 on a 4-point scale, with charge nurses and head nurses scoring higher than general nurses. This indicates that factors like clinical career and expertise positively influence the implementation of slow nursing. Consequently, further research is needed to explore how different personal and professional characteristics of long-term care hospital nurses affect the implementation levels of slow nursing.
While several suggestions have been made and qualitative studies on slow nursing have been conducted in recent years [12, 13, 14], and its importance is increasingly recognized [21], there remains no tool to measure the extent of its implementation. This study is significant because it developed the SNT-LCHN, a tool designed to measure the implementation level of slow nursing among nurses in long-term care hospitals, which is especially crucial for those caring for older inpatients. The findings of this study not only enhance the assessment of slow nursing implementation for older patients in long-term care hospitals but also facilitate the measurement and evaluation of slow nursing performance in community settings where older patients reside or receive care. Notably, the slow nursing tool developed here is particularly significant as it accounts for the unique characteristics of older patients, including impaired physical, emotional, and cognitive functions, as well as developmental stage tasks associated with old age. However, this study has limitations, notably that data collection was confined to nurses working in eight long-term care hospitals in the Daegu and Gyeongsangbuk-do area, recruited through convenience sampling. This methodological choice necessitates caution when generalizing the study’s results.
In this study, we developed SNT-LCHN, a tool designed to measure the level of slow nursing implementation among nurses in long-term care hospitals, specifically tailored to the unique environment and needs of older patients. We also tested its reliability and validity. The SNT-LCHN comprises 23 items divided into five categories: “adapting to the patient’s pace,” “encouraging observation and participation,” “providing comfort,” “showing respect,” and “bestowing value on life.” Each item is evaluated using a 4-point Likert scale, where a higher total score indicates a greater extent of slow nursing care provided to older patients in long-term care hospitals. Completing the tool typically requires between 5 to 10 minutes. The SNT-LCHN is expected to lead to a deeper understanding of slow care practices for older patients in long-term care settings and to serve as a valuable resource for measuring and evaluating the slow nursing care provided by nurses. Given that its theoretical components have been implemented in actual nursing practices, the tool is anticipated to aid in the development of Korea-specific slow nursing models and related theoretical frameworks. Furthermore, the SNT-LCHN could be beneficial for researchers who are developing interventional or educational programs aimed at promoting slow nursing in long-term care settings for the older, as well as for evaluating the effectiveness of these programs. Additionally, we propose conducting follow-up studies to further explore and validate the utility and applicability of this tool by applying it to nurses in long-term care hospitals of varying sizes and across different regions, and to identify factors influencing the level of slow nursing care.
CONFLICTS OF INTEREST:The author declArabes that there is no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - WHM.
analysis - WHM.
interpretation of the data - WHM.
drafting or critical revision of the manuscript for important intellectual content - WHM.
1=not relevant; 2=somewhat relevant; 3=quite relevant; 4=very relevant.

 E-SUBMISSION
E-SUBMISSION