Abstract
-
Purpose
This study aimed to develop and evaluate the effectiveness of a health management program using a mobile application for middle-aged men experiencing andropause.
-
Methods
A quasi-experimental design with a non-equivalent control group pretest-posttest structure was employed. The study took place from June 27 to August 30, 2024, with participant recruitment occurring from June 27 to July 10, 2024. In total, 61 participants (30 in the experimental group and 31 in the control group) participated from July 15 to August 20, 2024. The experimental group received an application-based health management program, while the control group did not.
-
Results
The experimental group showed significant improvements in subjective quality of life, health-promoting behaviors, and subjective health status compared to the control group (p<.001).
-
Conclusion
This study confirms that mobile applications can effectively manage health during andropause in middle-aged men. Further research with a larger sample size is recommended to validate these findings.
-
Key Words: Andropause; Health information management; Male; Mobile applications
INTRODUCTION
Andropause, derived from the Greek words
andras (man) and
pausē (cessation), refers to a clinical condition marked by a decline in masculinity due to age-related hormonal changes [
1]. It is a syndrome associated with androgen deficiency, primarily testosterone, leading to various physiological and psychological symptoms [
2]. Conditions such as androgen deficiency in the aging male, late-onset hypogonadism, and partial androgen deficiency in aging men are commonly observed in men undergoing andropause [
3].
In 1946, Werner published a seminal paper titled “The Male Climacteric” in the
Journal of the American Medical Association, outlining the clinical presentation of andropause [
4]. Since then, extensive research has examined the relationship between testosterone deficiency and associated symptoms, including diminished libido, reduced muscle mass and strength, impaired cognitive function, and overall decline in physical and mental well-being [
5].
The prevalence of andropause exceeds 60% among middle-aged men, significantly affecting their quality of life [
6]. If left unmanaged, andropause may contribute to chronic diseases such as metabolic syndrome, osteoporosis, and cardiovascular disorders [
7]. Thus, raising awareness and promoting proactive, evidence-based health management strategies are essential for mitigating the long-term impacts of andropause.
Middle age represents a peak period of social capability and a heightened need for recognition. However, it is also characterized by stress and instability due to experiences of andropause symptoms, aging-related physical and psychological changes, retirement, and shifting family dynamics [
8]. With a life expectancy of 83.3 years in Korea, advances in science and medical technology contribute to steadily increasing lifespans. Both men and women entering middle age at 40 years are expected to live an additional 40 years or more, prompting increased interest in quality-of-life enhancement during this extended period [
9]. Nonetheless, Korea’s 2022 Organization for Economic Co-operation and Development (OECD) life satisfaction score was 6.1 out of 10, below the OECD average of 7.4 [
10]. A previous study by Kim and Park [
11] identified factors such as andropause symptoms, depression, family bonding, physical activity, and monthly income as significant contributors to quality of life during early middle age. In later middle age, social support, subjective health status, job security, job stress, and smoking status were key influencing factors. Another study by Kim and Sung [
12] identified self-esteem, stress, andropause symptoms, and monthly income as significant factors impacting quality of life among middle-aged men.
With the increasing impact of andropause symptoms on quality of life in middle-aged men, there is an urgent need for effective prevention and management strategies [
12]. Educational programs emphasizing proper nutrition and physical activity, specifically tailored to middle-aged men, are essential for effectively managing andropause symptoms [
11]. Since mobile applications were introduced in Korea in November 2009, various applications have rapidly emerged. Currently, over 90% of Koreans use smartphones. This widespread smartphone usage has facilitated the introduction of health-related applications [
13], making them essential tools for self-management, patient education, and healthcare [
14]. Education through mobile applications enables tailored, individualized learning regardless of time and place. Leveraging smartphones, familiar to the general public, provides an accessible and cost-effective means of promoting health management and andropause prevention in men, maximizing benefits at minimal costs.
Despite the increasing use of mobile applications in healthcare, prior research on their effectiveness in health promotion, particularly for andropause management, remains insufficient [
12]. While existing studies have explored digital health interventions in chronic disease management, mental health, and physical activity promotion, research specifically addressing mobile application effectiveness in improving health outcomes for middle-aged men experiencing andropause is limited [
4]. This gap highlights the need for additional research into the potential benefits and limitations of mobile health applications within this population.
Furthermore, although previous research has explored digital health interventions, there is a lack of in-depth comparisons between different types of interventions implemented across diverse populations [
4,
5]. A more thorough discussion of mobile application-based health programs, covering their design, implementation, and long-term effectiveness, could strengthen the study’s context. Integrating findings from various mobile health interventions—such as diabetes management, cardiovascular disease prevention, and smoking cessation—would provide broader insights into the effectiveness of digital tools in managing andropause.
Most previous studies on middle-aged men have focused on specific aspects, such as relationships between andropause symptoms, stress, or quality of life [
12,
15], or have identified influencing factors without proposing comprehensive intervention strategies [
11]. In contrast, this study develops and implements a structured health management program specifically tailored for middle-aged men experiencing andropause. The program systematically aims to enhance health-promoting behaviors, subjective health status, and overall quality of life. By integrating nutritional, physical activity, and psychological education through an accessible mobile application, this study addresses existing research gaps and provides an innovative, practical solution for middle-aged men facing andropause-related challenges. Thus, this study aims to develop and evaluate the effectiveness of a mobile application-based health management program tailored for middle-aged men experiencing andropause.
METHODS
1. Study Design
This study used a quasi-experimental design featuring a non-equivalent control group pretest-posttest structure to develop and evaluate the effectiveness of a health management improvement education program for middle-aged men experiencing andropause. This study was reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials) guidelines.
2. Setting and Samples
The study was conducted from June 27 to August 30, 2024, targeting middle-aged men experiencing menopausal symptoms who visited urology departments at university hospitals in Seoul, Gyeonggi, and Gangwon provinces. Participants were recruited from June 27 to July 10, 2024, and data collection along with the intervention occurred from July 15 to August 20, 2024.
The inclusion criteria were as follows: participants were middle-aged men aware of their andropause (male menopause) symptoms who voluntarily consented to participate after fully understanding the study’s purpose. Participants had to communicate effectively and respond adequately to questionnaires. They could have common chronic conditions like prostate disorders, hypertension, hyperlipidemia, or diabetes, but they must not have been receiving specialized medical treatments, such as hormone therapy (e.g., testosterone replacement therapy). Additionally, their male hormone levels (e.g., total testosterone or free testosterone) should either not have been measured within the previous 6 months, or, if measured, results had to be at borderline levels without an established diagnosis or treatment plan.
The exclusion criteria were as follows: individuals requiring professional psychiatric treatment were excluded. Participants with physical disabilities hindering their use of mobile devices for the program were also excluded. Additionally, those already involved in other health management programs or clinical studies were not eligible to participate.
The sample size was calculated using G*Power 3.2 software [
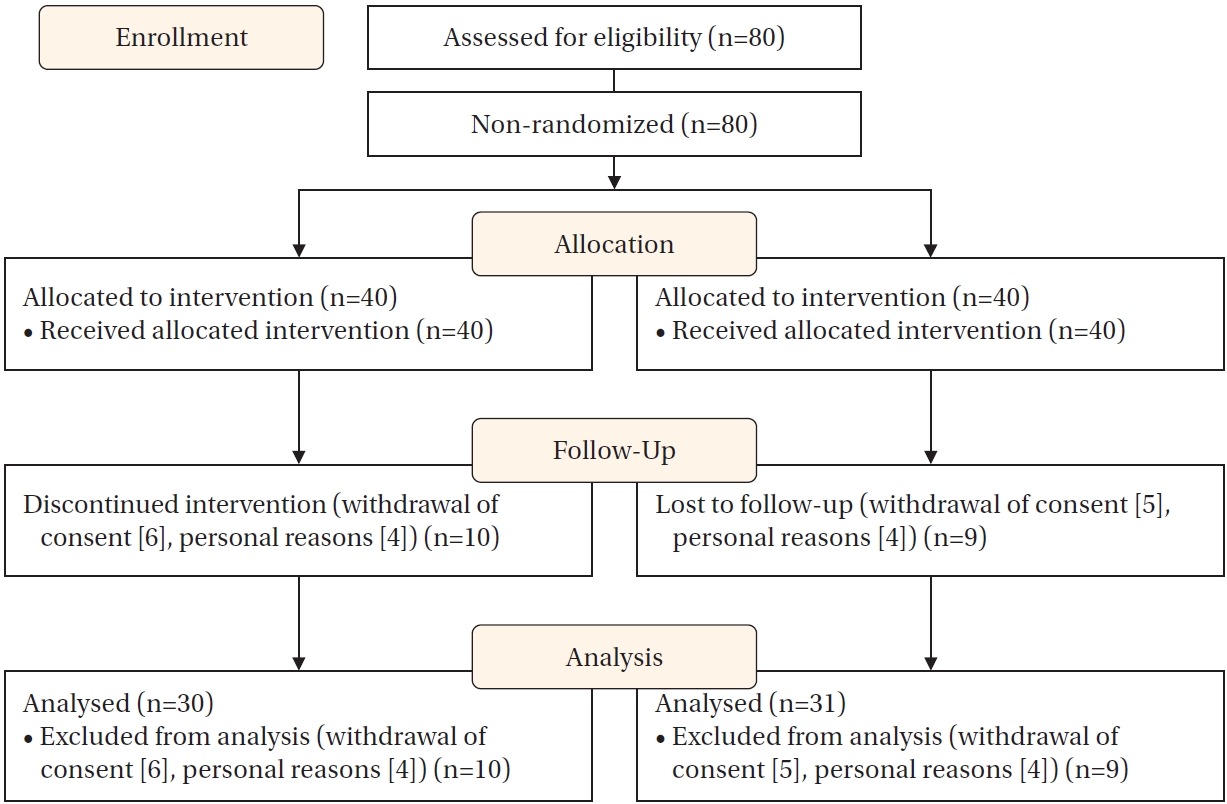
16], with a significance level of .05, statistical power of .80, and a medium effect size of .50. The required sample size per group was 27. Considering a potential dropout rate of 20%, 80 participants (40 per group) were recruited.
Participants were allocated to experimental and control groups through a non-randomized, convenience-based method. After verifying eligibility and obtaining consent, participants were sequentially assigned based on recruitment order and geographic accessibility. To minimize selection bias and enhance group equivalence, participants were matched by age and treatment history whenever possible. Although randomization was not implemented due to practical and ethical constraints in clinical settings, statistical tests confirmed homogeneity between groups before the intervention.
In the experimental group, 10 participants withdrew due to personal reasons (e.g., difficulty using the application or attending educational sessions). In the control group, nine participants withdrew due to relocation, business trips, or travel, preventing post-intervention data collection. Ultimately, data from 61 participants—30 in the experimental group and 31 in the control group—were included in the final analysis (
Figure 1).
Control group participants were selected via convenience sampling from the same hospitals and matched with the experimental group by age and treatment history.
3. Instruments
1) Subjective quality of life
In this study, subjective quality of life refers to an emotional evaluation that reflects a cognitive assessment of one’s overall life. The measurement tool used was the Subjective Quality of Life Scale, which was adapted and refined by Lee [
17] from Campbell’s Index of Wellbeing [
18]. This scale consists of eight items, each rated on a 5-point Likert scale, reflecting emotional evaluations based on recent experiences. Higher scores indicate greater satisfaction with life. Lee [
17] reported a reliability coefficient (Cronbach’s α) of .90; this study achieved a slightly higher reliability coefficient of .91.
2) Health-promoting behaviors
Health-promoting behaviors were measured using the Health Promotion Lifestyle Profile-II (HPLP-II), initially developed by Walker et al. [
19] and adapted for a Korean context by Seo and Hah [
20]. This instrument includes 50 items divided into six sub-factors: health responsibility (8 items), physical activity (8 items), nutrition (9 items), spiritual growth (9 items), interpersonal relationships (8 items), and stress management (8 items). Items are scored on a 4-point Likert scale, with higher scores indicating more frequent health-promoting behaviors. Cronbach’s α for reliability was .94 at original development, .92 in the adaptation by Seo and Hah [
20], and .94 in this study.
3) Subjective health status
Subjective health status was measured using the Health Self Rating Scale, originally developed by Northern Illinois University [
21] and later adapted and revised by Shin and Kim [
22]. This scale consists of three items rated on a 5-point Likert scale, with higher scores indicating better subjective health. Cronbach’s α for reliability was .70 in Shin and Kim’s study [
22] and .84 in the present study.
This study developed a mobile educational application designed to promote health management among middle-aged men experiencing andropause. The application development followed Keller’s ARCS (Attention, Relevance, Confidence, Satisfaction) motivational model [
23] and multimedia instructional design principles [
24]. The application aimed to enhance user motivation, improve health literacy, and encourage sustainable self-care behaviors (
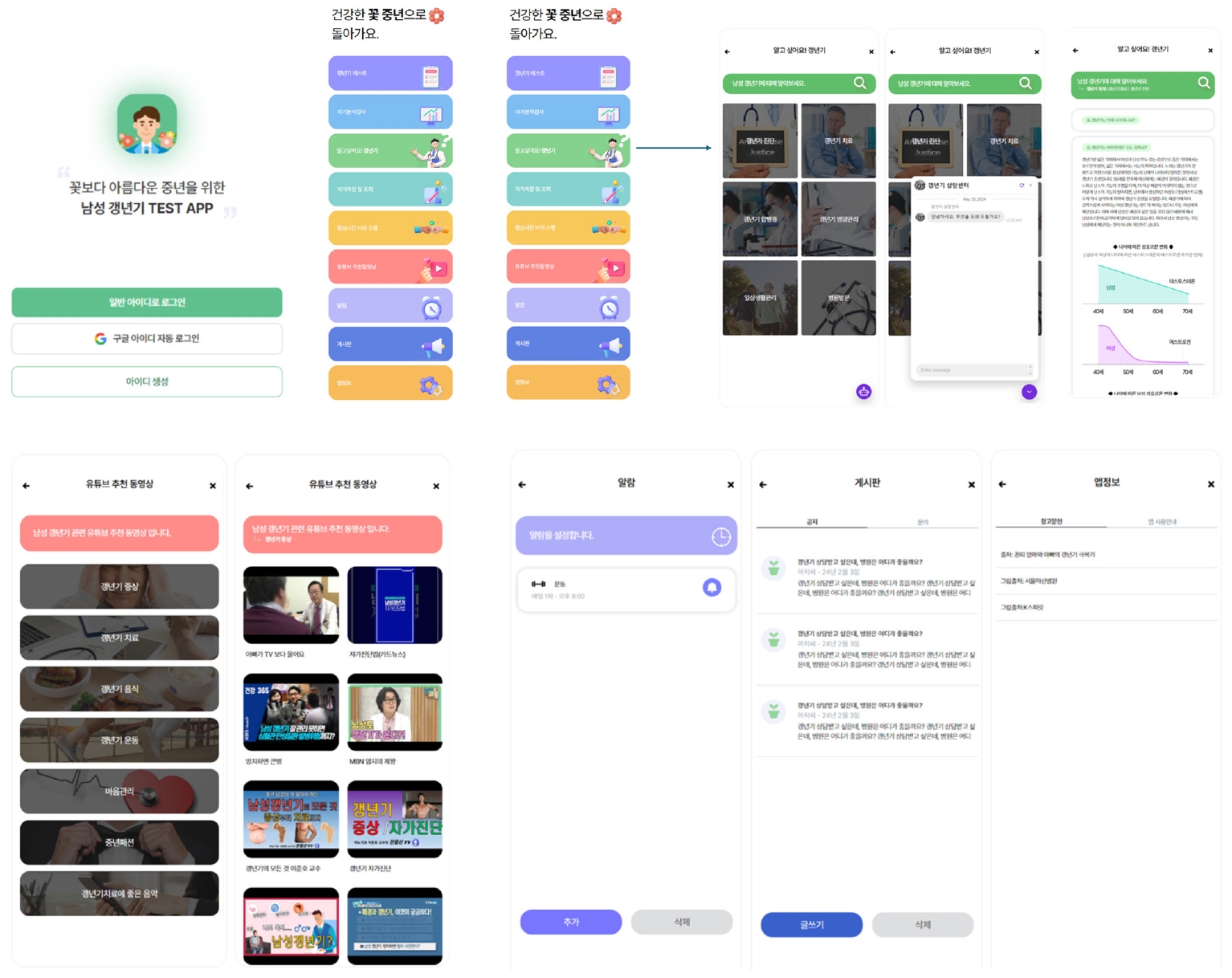
Appendix 1).
The mobile educational application used in this study was structured to support sustainable health behavior changes by increasing user engagement and self-efficacy. It included six key functions: educational content on andropause management, self-assessment checklists, symptom tracking, reminder alarms, peer support via a bulletin board, and application usage guidance. Additional features such as quizzes, educational videos, and an expert Q&A section were integrated based on user feedback to improve usability and satisfaction, as described in a previous study [
25].
Data collection was conducted from July 15 to August 20, 2024. With cooperation from the directors of participating hospitals, the research team carried out educational sessions and collected data at outpatient urology clinics. To ensure clear role distinctions between educators and data collectors, all research team members underwent training beforehand. Two primary educators delivered the intervention, while two assistant educators handled participant recruitment, administered the pre-test surveys, and guided participants through application installation.
The primary educators conducted face-to-face educational sessions and orientations, providing detailed instructions on both the content of the health management program and usage of the mobile application. Participants received individualized support, including additional guidance and feedback when encountering difficulties with the application. The structure of the mobile-based health management program, including its main menus and submenus, is presented in
Table 1 and
Appendix 2.
The assistant educators distributed and collected questionnaires, managed participant interactions, and conducted follow-up surveys. They also provided telephone consultations to ensure participants understood and effectively applied the educational content.
The intervention for the experimental group took place between July 15 and August 20, 2024. Participants engaged in a 14-day self-learning program via the application, accessing it at least once daily.
Before the intervention, a baseline survey was administered to assess participants’ health-promoting behaviors, subjective health status, and quality of life using standardized instruments. Participants received comprehensive explanations of the survey content and completion methods. Subsequently, during an application orientation session, two educators assisted participants with installing the application and provided detailed explanations about the program’s goals, participation methods, daily telephone consultation schedules, post-intervention survey procedures, and interview guidelines.
During the intervention period, participants performed daily self-directed learning through the application, complemented by daily telephone consultations with educators to reinforce content comprehension. After the intervention, assistant educators conducted a post-intervention survey to re-evaluate health-promoting behaviors, subjective health status, and quality of life. Additionally, participants completed individual interviews lasting 30–40 minutes to assess their satisfaction, application experiences, and overall impressions of the program.
For the control group, only pre- and post-intervention surveys were conducted, separated by a 14-day interval. In line with ethical considerations, after study completion, the mobile application was offered to control group participants. During the intervention period, the control group received a brief, one-time explanation emphasizing the importance of health management; however, no educational materials or interventions were provided.
6. Ethical Considerations
This study received approval from the Institutional Review Board of Sahmyook Seoul Hospital (IRB No: 116286-202403-HR-02). Before data collection, participants were informed of the study's purpose, confidentiality, absence of direct compensation or risk, and their rights to refuse or withdraw participation at any time. Written informed consent was obtained from all participants. All collected data were anonymized and accessible only to the research team. Regardless of group assignment, participants received a small token of appreciation for their voluntary participation.
7. Data Analysis
Data analysis was performed using the IBM SPSS/WIN version 24.0 software (IBM Corp., Armonk, NY, USA), applying the following statistical methods:
Descriptive statistics including frequency, percentage, mean, and standard deviation (SD) were used to analyze participants’ general characteristics, health-promoting behaviors, subjective health status, and quality of life. Normality of data distributions in both groups was assessed using the Kolmogorov-Smirnov and Shapiro-Wilk tests. Homogeneity between experimental and control groups prior to intervention was tested using parametric methods such as the independent t-test and chi-square test. Within-group differences before and after the intervention were examined using the paired t-test for parametric data and the Wilcoxon signed-rank test for non-parametric data, depending on data characteristics. Differences between groups post-intervention were analyzed using the independent t-test, the chi-square test, and the Mann-Whitney U test. p-values of less than 0.05 were considered significant. Lastly, the reliability of measurement instruments was confirmed by calculating Cronbach’s ⍺.
RESULTS
1. Homogeneity Test of Participants’ General Characteristics
To evaluate the development and effectiveness of the educational mobile application for health management among middle-aged men experiencing andropause, a homogeneity test on participants' general characteristics was conducted. The results confirmed no statistically significant differences between experimental and control groups at a significance level of 5%, ensuring homogeneity (
Table 1). Specifically, 36.7% of experimental participants and 38.7% of control participants resided in Seoul; this difference was not statistically significant (t=2.07,
p=.356). In Gangwon province, representation was 20.0% in the experimental group and 29.0% in the control group. Participants from Gyeonggi province accounted for 43.3% of the experimental group and 32.2% of the control group.
The mean age was 54.33 years (SD=5.66) in the experimental group and 53.77 years (SD=4.77) in the control group, with no significant difference (t=0.42, p=.678).
For the duration of andropause treatment, 50.0% of the experimental group and 74.2% of the control group had received treatment for less than 6 months; this difference was not statistically significant (t=4.18, p=.382). Treatment durations of 7 to 12 months were reported by 33.3% of experimental participants and 19.4% of controls, while durations of 13 to 18 months were reported by 10.0% and 6.4%, respectively. Only 3.3% of experimental participants had 19 to 24 months of treatment, compared to 0.0% in the control group. Treatment duration exceeding 24 months was reported by 3.3% of experimental participants and none in the control group.
Regarding marital status, 16.7% of experimental and 9.7% of control participants were single, with no significant difference (t=3.49, p=.175). Married participants constituted 83.3% of the experimental group and 80.6% of the control group. No experimental participants reported being divorced, whereas 9.7% of control participants were divorced.
In terms of living arrangements, 20.0% of experimental participants and 12.9% of control participants lived alone, with no significant difference (t=0.50, p=.973). Living with a spouse was reported by 23.3% of experimental participants and 25.8% of control participants. Living only with children was reported by 3.3% of the experimental group and 3.2% of the control group. Participants living with both spouse and children accounted for 46.7% of the experimental group and 51.6% of the control group, while other living arrangements were reported by 6.7% of the experimental group and 6.5% of the control group.
Educational attainment revealed no significant differences (t=5.10, p=.165), with 13.3% of experimental and 35.5% of control participants having a high school diploma or less. University-level education was reported by 30.0% of experimental and 22.6% of control participants. Bachelor’s degrees were held by 33.3% of experimental and 32.3% of control participants, while graduate-level education or higher was reported by 23.3% and 9.7%, respectively.
Regarding income levels (reported as annual income), no participants in the experimental group and 3.2% of participants in the control group reported earning between 10 and 20 million KRW per year, with no statistically significant difference between the groups (t=1.31, p=.715). Among the participants, 3.3% of the experimental group and 3.2% of the control group earned between 20 and 30 million KRW annually. An income between 30 and 40 million KRW was reported by 26.7% of participants in the experimental group and 19.4% in the control group. Lastly, a majority of participants in both groups earned over 50 million KRW annually 70.0% in the experimental group and 74.2% in the control group.
2. Homogeneity Test of Participants’ Subjective Quality of Life, Health-Promoting Behaviors, and Subjective Health Status
To evaluate the homogeneity of the experimental and control groups regarding subjective quality of life, health-promoting behaviors, and subjective health status prior to intervention, both parametric (independent t-test) and non-parametric (Mann–Whitney U test) analyses were conducted. The results confirmed no statistically significant differences at the 5% significance level, indicating homogeneity between groups in these variables prior to intervention (
Table 2).
Regarding subjective quality of life, the mean scores were 2.98 (SD=0.89) in the experimental group and 2.77 (SD=0.70) in the control group, showing no significant difference (t=1.005, p=.319). Similarly, the Mann-Whitney U test confirmed no significant difference (Z=–1.150, p=.250). The median scores were 3.06 (25th–75th percentiles=2.13–3.50) in the experimental group and 2.75 (25th–75th percentiles=2.25–3.00) in the control group.
With respect to health-promoting behaviors, the mean scores were 2.20 (SD=0.58) for the experimental group and 1.97 (SD=0.46) for the control group, with no significant difference (t=1.739, p=.087). The Mann–Whitney U test also showed no significant difference (Z=–1.428, p=.153). The median scores were 2.20 (25th–75th percentiles=1.79–2.60) for experimental participants and 1.86 (25th–75th percentiles=1.62–2.38) for controls, corresponding to a small difference.
For subjective health status, the mean scores were 2.86 (SD=0.82) in the experimental group and 3.08 (SD=0.64) in the control group, with no statistically significant difference (t=–1.163, p=.249). The Mann–Whitney U test similarly showed no significant difference (Z=–0.834, p=.404). The median scores were identical at 3.00, with interquartile ranges of 2.00–3.42 for the experimental group and 2.67–3.33 for the control group, confirming minimal variation between groups.
3. Pre-Post Comparison of Subjective Quality of Life, Health-Promoting Behaviors, and Subjective Health Status
The analysis of pretest and posttest measurements in the experimental group, conducted using both parametric (paired t-test) and non-parametric (Wilcoxon test) methods, revealed statistically significant improvements at the 5% significance level in subjective quality of life, health-promoting behaviors, and subjective health status. These results indicate that the health management improvement education program effectively enhanced these aspects for middle-aged men experiencing andropause. Conversely, the control group demonstrated no statistically significant differences between pre- and post-intervention measures. Moreover, the comparison between experimental and control groups after the intervention, analyzed using independent t-tests and Mann-Whitney U tests, showed statistically significant differences at the 5% significance level. Posttest results confirmed that the experimental group scored higher than the control group on subjective quality of life, health-promoting behaviors, and subjective health status (
Table 3).
For subjective quality of life, the experimental group’s mean score increased significantly from 2.26 (SD=0.86, median=2.19, 25th–75th percentiles=1.59–2.69) before the intervention, to 2.98 (SD=0.89, median=3.06, 25th–75th percentiles=2.13–3.50) after the intervention. In the control group, the mean score decreased from 2.75 (SD=0.69, median=2.75, 25th–75th percentiles=2.25–3.00) pre-intervention to 2.40 (SD=0.79, median=2.00, 25th–75th percentiles=1.88–2.81) post-intervention. The paired t-test showed that the experimental group significantly improved in subjective quality of life post-intervention (t=2.34, p=.028), and the Mann-Whitney U test confirmed this statistically significant difference (Z=2.33, p=.019).
Regarding health-promoting behaviors, the experimental group's mean score significantly increased from 2.20 (SD=0.58, median=2.20, 25th–75th percentiles=1.79–2.60) pre-intervention, to 2.57 (SD=0.64, median=2.63, 25th–75th percentiles=2.06–3.10) post-intervention. In the control group, the mean score rose from 1.97 (SD=0.46, median=1.86, 25th–75th percentiles=1.62–2.38) before the intervention, to 2.31 (SD=0.43, median=2.64, 25th–75th percentiles=2.22–2.82) after the intervention. The paired t-test indicated a statistically significant improvement for the experimental group in health-promoting behaviors (t=2.31, p=.021), further supported by the Mann-Whitney U test (Z=2.15, p=.032).
For subjective health status, the experimental group's mean score significantly increased from 2.86 (SD=0.82, median=3.00, 25th–75th percentiles=2.00–3.42) before the intervention to 3.40 (SD=0.66, median=3.67, 25th–75th percentiles=3.00–3.67) after the intervention. In the control group, the mean score rose from 3.08 (SD=0.64, median=3.00, 25th–75th percentiles=2.67–3.33) pre-intervention to 3.45 (SD=0.76, median=3.67, 25th–75th percentiles=3.00–4.00) post-intervention. The paired t-test showed that the experimental group’s improvement in subjective health status post-intervention was statistically significant (t=2.44, p=.019), and the Mann-Whitney U test also confirmed this significant difference (Z=2.02, p=.043).
DISCUSSION
In South Korea, public awareness and management strategies for male andropause remain relatively limited, and health promotion services offered by public health centers for this issue are also insufficient. Building upon prior research, this study developed a health promotion program aimed at improving symptom management for middle-aged men experiencing andropause [
4]. The findings confirmed that homogeneity was successfully established between the experimental and control groups, which is essential for verifying the research’s overall validity and strengthens the reliability of the program’s effectiveness evaluation. With established homogeneity, the experimental group demonstrated significant improvements in subjective quality of life, health-promoting behaviors, and perceived health status. These outcomes provide critical evidence supporting the educational program’s effectiveness for health management in middle-aged men.
In contrast, the control group showed no significant improvements in health-promoting behaviors, subjective health status, or quality of life compared to the experimental group. This lack of improvement may be attributed to the complex interplay of external factors such as voluntary participation in health management, insufficient educational support, low motivation, the short duration of the intervention, and environmental influences that could have impacted their health behaviors and quality of life.
To enhance the validity of future research, researchers should more rigorously control these external variables and refine the study design. Additionally, careful consideration of these external influences is necessary when comparing experimental and control groups to strengthen the reliability of findings.
This study’s intervention lasted approximately 2 weeks, making it challenging to evaluate its medium- to long-term effects. Particularly, further follow-up research is necessary to assess whether improvements in health-promoting behaviors and lifestyle changes persist over time. Future research should, therefore, evaluate the sustainability of these effects over longer periods, such as 6 months or one year.
This study demonstrated that mobile application-based health education positively influenced health promotion among middle-aged men. Further research is required to validate the effectiveness of this educational approach in greater depth and to develop additional strategies enhancing its practical applicability.
Andropause is characterized by substantial physical and psychological changes, making middle age a critical period for enhanced health management. Previous studies have confirmed that physical and emotional symptoms of andropause negatively affect subjective quality of life and health behaviors [
26]. Therefore, middle-aged men should emphasize proactive health management upon entering andropause. The health promotion program developed in this study significantly addresses these issues. According to the findings, the experimental group experienced meaningful improvements in subjective quality of life, health-promoting behaviors, and perceived health status following participation [
27].
The educational program used an integrated approach to comprehensively address the physical and emotional needs of men experiencing andropause, demonstrating a positive impact on their overall health. Specifically, the intervention provided education via a mobile application—covering essential knowledge, dietary recommendations, and exercise guidance—and included practice monitoring, which constituted targeted interventions specifically for middle-aged men with andropause. These elements were intentionally designed to address core health concerns related to andropause during the development process. By offering fundamental knowledge, the program increased participants' understanding of andropause; dietary and exercise guidance provided practical strategies for symptom management, and the application’s monitoring feature reinforced sustained participation and adherence, encouraging positive behavioral changes.
This study highlights that a targeted intervention effectively improved self-management among middle-aged men. By integrating various aspects of health management (knowledge provision, behavioral practices, and real-time monitoring), the program offered a holistic and systematic approach [
28]. This integrative method facilitated not only the management of physical symptoms but also promoted consistent engagement in health-promoting behaviors, enhancing overall well-being.
Therefore, ongoing data collection is essential for establishing structured and personalized programs as crucial tools in promoting health among men experiencing andropause. Such efforts will help alleviate andropause symptoms and expand opportunities to enhance overall quality of life.
The experimental group, which received the mobile educational intervention, exhibited significant improvements in health-promoting behaviors, subjective health status, and quality of life compared to the control group. These results align with previous research highlighting the effectiveness of mobile health interventions for enhancing physical, emotional, and overall well-being, especially in middle-aged men experiencing andropause.
The findings of this study are consistent with prior research demonstrating that mobile health interventions effectively improve health behaviors, subjective health status, and quality of life [
29,
30], reinforcing the potential of mobile health programs for managing health during andropause. The study supported all three hypotheses, confirming significant improvements through the mobile educational program. The program’s success can be attributed to its accessible and personalized approach. However, limitations include the short intervention period and reliance on self-reported data. Future research should include longer follow-up periods and objective outcome measures to further validate these findings.
However, this study has certain limitations. The use of convenience sampling limits the generalizability of the results. Additionally, participants were drawn from specific geographic regions (Seoul, Gyeonggi, and Gangwon provinces in Korea), further restricting the broader applicability of the findings. Future research should involve larger and more diverse samples to enhance the validity and applicability of the results.
CONCLUSION
This study evaluated the impact of an educational program designed to improve symptoms of andropause and promote health among middle-aged men. It specifically assessed the program's influence on subjective quality of life, health-promoting behaviors, and subjective health status. The experimental group demonstrated statistically significant improvements compared to the control group, underscoring the program’s effectiveness in enhancing health management among middle-aged men experiencing andropause.
Middle-aged men undergo significant physical and emotional changes during andropause, which, if inadequately managed, can lead to reduced quality of life and health deterioration. Consequently, structured and individualized health promotion programs are critically needed to effectively address these challenges. The program developed in this study utilized a mobile application-based educational approach, delivering accessible health management information free from constraints of time and location. This enabled participants to easily integrate health management practices into their daily routines, highlighting the program’s practical utility in facilitating consistent health behaviors.
The findings emphasize the necessity of systematic, regular educational programs to help middle-aged men manage the physical and emotional changes associated with andropause and to improve overall health. Mobile application-based health education is particularly promising as an essential tool within such programs. It is crucial to continue refining these methods so that more middle-aged men can effectively manage andropause symptoms and enhance their quality of life.
Based on the results of this study, the following recommendations are proposed: First, given the limited number of participants, further research involving continuous data collection with more diverse populations is necessary to develop effective health management programs tailored for men experiencing andropause. Second, due to the current lack of systematic support for andropause-related health promotion programs within public health services, increased efforts in awareness campaigns and educational initiatives are essential.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and design acquisition - SJP and YSL; data collection - SJP and YSL; analysis and interpretation of the data - SJP and YSL; discussion and conclusions -suggestions: SJP; english review - SJP and YSL; abstract and references and final submission - YSL; drafting and critical revision of the manuscript - SJP and YSL.
-
FUNDING
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. RS-2022-00166296).
-
ACKNOWLEDGEMENT
Application development was done by It's JLAB Co., Ltd.
-
DATA AVAILABILITY STATEMENT
The data can be obtained from the corresponding authors.
Figure 1.CONSORT 2010 flow diagram.
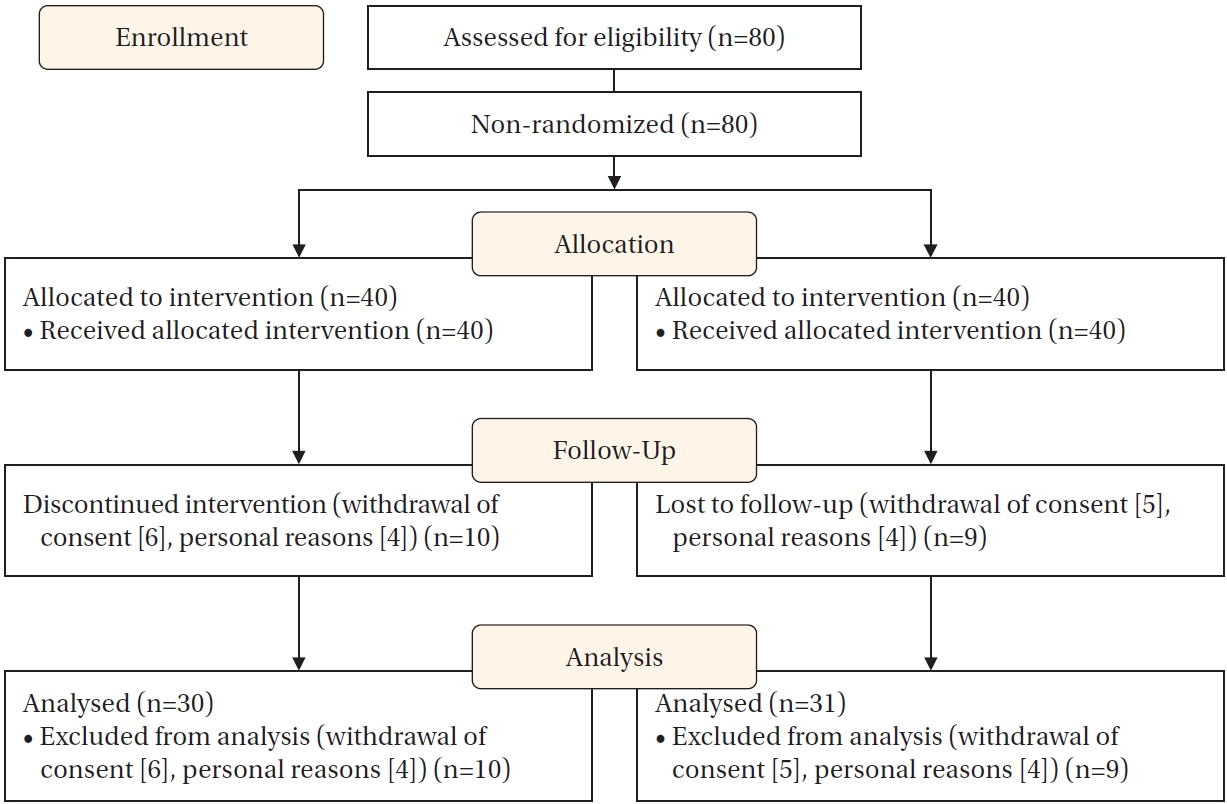
Table 1.Homogeneity Test of Participants’ General Characteristics
|
Variables |
Categories |
n (%) or M±SD |
χ2/t (p) |
|
Experimental group (n=30) |
Control group (n=31) |
|
Region |
Seoul |
11 (36.7) |
12 (38.7) |
2.07 (.356) |
|
Gangwon province |
6 (20.0) |
9 (29.0) |
|
|
Gyeonggi province |
13 (43.3) |
10 (32.3) |
|
|
Age (year) |
|
54.33±5.66 |
53.77±4.77 |
0.42 (.678) |
|
Andropause treatment duration |
≤6 months |
15 (50.0) |
23 (74.2) |
4.18 (.382) |
|
7–12 months |
10 (33.3) |
6 (19.4) |
|
|
13–18 months |
3 (10.0) |
2 (6.4) |
|
|
19–24 months |
1 (3.3) |
0 (0.0) |
|
|
>24 months |
1 (3.3) |
0 (0.0) |
|
|
Marital status |
Single |
5 (16.7) |
3 (9.7) |
3.49 (.175) |
|
Married |
25 (83.3) |
25 (80.6) |
|
|
Divorced |
0 (0.0) |
3 (9.7) |
|
|
Living with family |
Alone |
6 (20.0) |
4 (12.9) |
0.50 (.973) |
|
With spouse |
7 (23.3) |
8 (25.8) |
|
|
With children |
1 (3.3) |
1 (3.2) |
|
|
With spouse and children |
14 (46.7) |
16 (51.6) |
|
|
Other |
2 (6.7) |
2 (6.5) |
|
|
Education level |
≤High school graduate |
4 (13.3) |
11 (35.5) |
5.10 (.165) |
|
College graduate |
9 (30.0) |
7 (22.6) |
|
|
University graduate |
10 (33.3) |
10 (32.3) |
|
|
Graduate school or higher |
7 (23.3) |
3 (9.7) |
|
|
Annual income level (million KRW) |
10–20 |
0 (0.0) |
1 (3.2) |
1.31 (.715) |
|
21–30 |
1 (3.3) |
1 (3.2) |
|
|
31–40 |
8 (26.7) |
6 (19.4) |
|
|
≥41 |
21 (70.0) |
23 (74.2) |
|
Table 2.Homogeneity Test of Participants’ Subjective Quality of Life, Health-Promoting Behaviors, and Subjective Health Status
|
Variables |
Items |
Experimental group (n=30) |
Control group (n=31) |
Z (p) |
|
Subjective quality of life |
M±SD |
2.98±0.89 |
2.77±0.70 |
–1.150 (.250) |
|
Median (25th–75th percentiles) |
3.06 (2.13–3.50) |
2.75 (2.25–3.00) |
|
Health-promoting behaviors |
M±SD |
2.20±0.58 |
1.97±0.46 |
–1.428 (.153) |
|
Median (25th–75th percentiles) |
2.20 (1.79–2.60) |
1.86 (1.62–2.38) |
|
Subjective health status |
M±SD |
2.86±0.82 |
3.08±0.64 |
–0.834 (.404) |
|
Median (25th–75th percentiles) |
3.00 (2.00–3.42) |
3.00 (2.67–3.33) |
Table 3.Comparison of Subjective Quality of Life, Health-Promoting Behaviors, and Subjective Health Status
|
Variables |
Items |
Experimental group (n=30) |
Control group (n=31) |
t (p)/Z (p) |
|
Pre |
Post |
Pre |
Post |
|
Subjective quality of life |
Paired differences (M±SD) |
2.26±0.86 |
2.98±0.89 |
2.75±0.69 |
2.40±0.79 |
2.34 (.028)/2.33 (.019) |
|
Median (25th–75th percentiles) |
2.19 (1.59–2.69) |
3.06 (2.13–3.50) |
2.75 (2.25–3.00) |
2.00 (1.88–2.81) |
|
|
Health-promoting behaviors |
Paired differences (M±SD) |
2.20±0.58 |
2.57±0.64 |
1.97±0.46 |
2.31±0.43 |
2.31 (.021)/2.15 (.032) |
|
Median (25th–75th percentiles) |
2.20 (1.79–2.60) |
2.63 (2.06–3.10) |
1.86 (1.62–2.38) |
2.64 (2.22–2.82) |
|
|
Subjective health status |
Paired differences (M±SD) |
2.86±0.82 |
3.40±0.66 |
3.08±0.64 |
3.45±0.76 |
2.44 (.019)/2.02 (.043) |
|
Median (25th–75th percentiles) |
3.00 (2.00–3.42) |
3.67 (3.00–3.67) |
3.00 (2.67–3.33) |
3.67 (3.00–4.00) |
|
REFERENCES
- 1. Shibata M, Fojii M, Yamaguchi R. Pharmacological studies on bamboo grass. IV. Toxicological and pharmacological effects of the extract (FIII) obtained from Sasa albomarginata Makino et Shibata. Yakugaku Zasshi. 1979;99(6):663-8. https://doi.org/10.1248/yakushi1947.99.6_663
- 2. Kim EY, Jung EY, Lim HS, Heo YR. The effects of the Sasa borealis leaves extract on plasma adiponectin, resistin, C-reactive protein and homocysteine levels in high fat diet-induced obese C57/BL6J mice. J Nutr Health. 2014;40(4):303-11.
- 3. Park SJ, Lim YS. Challenges and experiences of men who have undergone andropause: insights from a focus group study. Korean J Adult Nurs. 2023;35(3):290-301. https://doi.org/10.7475/kjan.2023.35.3.290
- 4. Lim YS, Park SJ. Perceptions of andropausal experience types among middle-aged men: applying the Q methodology. J Mens Health. 2025;21(1):87-97. https://doi.org/10.22514/jomh.2025.009
- 5. Kwon MH, Oh JH. Subjective health status, job stress and andropause symptoms among middle-aged males who work. J Korea Soc Comput Inf. 2020;25(9):109-16. https://doi.org/10.9708/jksci.2020.25.09.109
- 6. Ding H, Zhao J, Liu H, Wang J, Lu W. BMAL1 knockdown promoted apoptosis and reduced testosterone secretion in TM3 Leydig cell line. Gene. 2020;747:144672. https://doi.org/10.1016/j.gene.2020.144672
- 7. Lee MW, Park H. A study on late-onset of hypogonadism, erectile dysfunction, depression, and quality of life among middle-aged male worker. Korean J Adult Nurs. 2013;25(5):483-93. https://doi.org/10.7475/kjan.2013.25.5.483
- 8. Jeon HW, Kim SA. A phenomenological convergence study on the experience of middle-aged menopause. J Korea Converg Soc. 2017;8(9):217-29. https://doi.org/10.15207/JKCS.2017.8.9.217
- 9. Statistics Korea. Life tables for Korea, 2021 [Internet]. Daejeon: Statistics Korea; 2021 [cited 2025 April 26]. Available from: https://kostat.go.kr/board.es?mid=a20108060000&bid=11746&act=view&list_no=422500
- 10. Organization for Economic Co-operation and Development (OECD). How’s life? 2020: measuring well-being [Internet]. Paris: OECD Publishing; 2020 [cited 2024 August 3]. Available from: https://doi.org/10.1787/9870c393-en
- 11. Kim HS, Park MH. A converged study on the influence on the quality of life for early and late middle-aged men. J Korea Converg Soc. 2018;9(6):133-45. https://doi.org/10.15207/JKCS.2018.9.6.133
- 12. Kim BR, Sung KM. Andropause symptoms, stress, self-esteem and quality of life among middle-aged men. J Digit Converg. 2018;16(12):467-75. https://doi.org/10.14400/JDC.2018.16.12.467
- 13. Brickwood KJ, Ahuja KD, Watson G, O'Brien JA, Williams AD. Effects of activity tracker use with health professional support or telephone counseling on maintenance of physical activity and health outcomes in older adults: randomized controlled trial. JMIR Mhealth Uhealth. 2021;9(1):e18686. https://doi.org/10.2196/18686
- 14. Byun H, Jeon SW, Yi ES. A study on the current situation and trend analysis of the elderly healthcare applications using big data analysis. J Korea Converg Soc. 2022;13(5):313-25. https://doi.org/10.15207/JKCS.2022.13.05.313
- 15. Olfson M, Wall M, Liu SM, Morin CM, Blanco C. Insomnia and impaired quality of life in the United States. J Clin Psychiatry. 2018;79(5):17m12020. https://doi.org/10.4088/JCP.17m12020
- 16. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149-60. https://doi.org/10.3758/brm.41.4.1149
- 17. Lee MS. Subjective quality of life of Korean workers and associated variables [dissertation]. Seoul: Yonsei University; 1998.
- 18. Campbell A. The sense of well-being in America: Recent patterns and trends. New York: McGraw-Hill; 1981. p. 23-45.
- 19. Walker SN, Sechrist KR, Pender NJ. The health-promoting lifestyle profile II. Omaha: College of Nursing, University of Nebraska Medical Center; 1995.
- 20. Seo HM, Hah YS. A study of factors influencing on health promoting lifestyle in the elderly: application of Pender's health promotion model. J Korean Acad Nurs. 2004;34(7):1288-97. https://doi.org/10.4040/jkan.2004.34.7.1288
- 21. McDowell I, Newell C. Measuring health: a guide to rating scales and questionnaires. New York: Oxford University Press; 1987.
- 22. Shin YS, Kim EH. A study on health behaviors, health status and anxiety about aging for the elderly: focused on the elderly in senior center. J Korean Acad Community Health Nurs. 2009;20(2):179-88.
- 23. Keller JM, Song SH. Charming instruction design. 1st ed. Seoul: Kyoyookbook; 2005.
- 24. Na IJ. Web-based education. 1st ed. Seoul: Kyoyookbook; 1999.
- 25. Korea Internet and Security Agency; Korea Communications Commission. Survey on the internet use 2012 [Internet]. Seoul: Korea Internet & Security Agency; 2023 [cited 2024 August 5]. Available from: https://www.nia.or.kr/site/nia_kor/ex/bbs/View.do?cbIdx=99870&bcIdx=26715
- 26. Mousavi M, Mahmoudi M, Golitaleb M, Khajehgoodari M, Hekmatpou D, Vakilian P. Exploratory study of andropause syndrome in 40-65 years in arak: a cross sectional study. J Fam Reprod Health. 2018;12(3):142-7.
- 27. Hess R, Thurston RC, Hays RD, Chang CC, Dillon SN, Ness RB, et al. The impact of menopause on health-related quality of life: results from the STRIDE longitudinal study. Qual Life Res. 2012;21(3):535-44. https://doi.org/10.1007/s11136-011-9959-7
- 28. Guerrero-Gonzalez C, Cueto-Urena C, Canton-Habas V, Ramirez-Exposito MJ, Martinez-Martos JM. Healthy aging in menopause: prevention of cognitive decline, depression and dementia through physical exercise. Physiologia. 2024;4(1):115-38. https://doi.org/10.3390/physiologia4010007
- 29. Lim YS, Park SJ. Development of a mobile-based health management application for men in andropause. J Mens Health. 2024;20(11):96-104. https://doi.org/10.22514/jomh.2024.189
- 30. Lee MS, Kim JM. The effects of health promotion program on health belief, health promoting behavior and quality of life for middle-aged women: based on health belief model. Int J Adv Cult Technol. 2019;7(3):25-34. https://doi.org/10.17703/IJACT.2019.7.3.25
Appendices
Appendix 1.
- Structure of the Mobile-Based Andropause Health Management Program
|
Day |
Education topic |
Educational method |
Remarks |
App feature |
|
1 |
App usage orientation and program introduction |
In-person education+app download instructions |
App usage instructions and installation support |
App information |
|
2 |
Understanding male menopause |
Watch app video+quiz |
Concept Understanding and Problem Check |
Education |
|
3 |
Exercise and physical activity |
Self-learning with app content |
Providing a Practice Checklist |
Education+self-assessment |
|
4 |
Nutritional management and healthy eating habits |
Self-study with app content |
Including sample diet plan |
Education+self-assessment |
|
5 |
Stress awareness and management techniques |
Self-study with app content |
Including deep breathing and meditation video |
Education |
|
6 |
Sleep hygiene education |
Self-study with app content |
Sleep diary instructions |
Self-assessment+inquiry |
|
7 |
Week 1 review and quiz |
App review content |
Providing phone feedback |
Learning module (quiz) |
|
8 |
Health behavior implementation strategies |
Self-Study with app content |
Encouraging lifestyle routine review |
Education |
|
9 |
Utilizing family and social support |
Self-study with app content |
Providing tips for family involvement |
Bulletin board |
|
10 |
Emotional management and self-motivation enhancement |
Self-study with app content |
Including examples of positive self-talk |
Education |
|
11 |
Setting personal health goals |
Self-study with app content |
Guidance for setting SMART goals |
Self-assessment |
|
12 |
Problem-solving strategies |
Self-study with app content |
Scenario-based learning |
Education |
|
13 |
Plan for maintaining healthy lifestyle habits |
Self-study with app content |
Providing a practice checklist |
Education+self-assessment |
|
14 |
Overall review+app usage satisfaction survey |
In-person interview (30–40 minutes) |
App usage feedback and satisfaction survey |
App information+Q&A |
|
Daily |
Daily phone consultation |
- |
Review and feedback |
Alarm+inquiry |
Appendix 2.
- Main menu and sub-menu interfaces of the health education application.


 E-SUBMISSION
E-SUBMISSION
