
Purpose
This study aimed to identify the effects of psychological insulin resistance, diabetes distress, and diabetes self-efficacy of patients and their spouses on insulin therapy adherence of patients with type 2 diabetes.
Methods
A path analysis based on the actor-partner interdependence model, a couple analysis method, was used to identify the actor and partner effects of psychological insulin resistance, diabetes distress, diabetes self-efficacy on the insulin therapy adherence of patients with type 2 diabetes. Data were collected between February 25 and May 1, 2019, from 200 patients with type 2 diabetes and their spouses.
Results
The psychological insulin resistance of the patient had an actor effect on the diabetes self-efficacy of the patient and a partner effect on the diabetes self-efficacy of the spouse, and the patient’s diabetes distress had a partner effect on the diabetes self-efficacy of the spouse. The psychological insulin resistance of the spouse had an actor effect on the diabetes self-efficacy of the spouse, and the diabetes self-efficacy of the patient and spouse were found to affect the insulin therapy adherence of the patient directly.
Conclusion
This study provided basic data for the development of programs that can enhance insulin therapy adherence in patients with type 2 diabetes, focusing on the perspectives of both the patient and spouse.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
This study aimed to identify the effects of psychological insulin resistance, diabetes distress, and diabetes self-efficacy of patients and their spouses on insulin therapy adherence of patients with type 2 diabetes.
A path analysis based on the actor-partner interdependence model, a couple analysis method, was used to identify the actor and partner effects of psychological insulin resistance, diabetes distress, diabetes self-efficacy on the insulin therapy adherence of patients with type 2 diabetes. Data were collected between February 25 and May 1, 2019, from 200 patients with type 2 diabetes and their spouses.
The psychological insulin resistance of the patient had an actor effect on the diabetes self-efficacy of the patient and a partner effect on the diabetes self-efficacy of the spouse, and the patient's diabetes distress had a partner effect on the diabetes self-efficacy of the spouse. The psychological insulin resistance of the spouse had an actor effect on the diabetes self-efficacy of the spouse, and the diabetes self-efficacy of the patient and spouse were found to affect the insulin therapy adherence of the patient directly.
This study provided basic data for the development of programs that can enhance insulin therapy adherence in patients with type 2 diabetes, focusing on the perspectives of both the patient and spouse.
In Korea, the prevalence of diabetes increases sharply from 2.5% in those aged 30~39 years to 13.0% in those aged 50~59 years, and 26.5% in those aged ≥70 years, showing an increasing trend as age increases [1]. The diabetes-related mortality rate was 17.1% in 2018; the condition ranked sixth in the most common causes of death in adults that year [2], and by 2050, the prevalence of diabetes is expected to increase by more than twice the current level [3]. Type 2 diabetes is a progressive disease caused by an impaired function of pancreatic beta cells and decreased insulin secretion. Treatment for type 2 diabetes is chosen according to the degree of disease progression [4]. In particular, patients with type 2 diabetes have to improve their lifestyle habits (e.g., diet, exercise, and weight control) and also take oral hypoglycemic agents [5]. Many patients are prescribed insulin injections due to impaired insulin secretion after several years, with insulin therapy becoming stronger over time [6]. Moreover, because there is a tendency for insulin secretion to decrease to approximately 25% of the normal level at 6 years after diagnosis, early insulin therapy is recommended to protect beta cells, maintain an appropriate level of glycated hemoglobin, and prevent cardiovascular complications [5].
Insulin therapy adherence is an important factor in diabetes self-management that influences the maintenance of an appropriate level of blood sugar, and the risk of complications and mortality [7]. However, most patients with diabetes show low insulin therapy adherence, and the major causes associated with this have been identified as patient-related factors such as the fear of needles (for insulin injection), becoming hypoglycemic, weight gain, and complications associated with insulin administration; system-related factors such as inadequate follow-up and lack of a support system; and drug-related factors such as complicated insulin therapy and frequent changes in dosage [8]. Additionally, patients may have negative attitudes that interfere with their insulin therapy adherence. They may express anxiety about starting insulin therapy or refuse to administer insulin. This phenomenon has been termed “psychological insulin resistance” [9]. The major causes of psychological insulin resistance include patients having a misperception that insulin administration means failed diabetes management, pain associated with injection, anxiety about complications associated with insulin administration, absence of family members who can help with insulin administration, and being misinformed about insulin therapy [10]. From a long-term perspective, successful insulin therapy requires better understanding of psychological insulin resistance in patients and identification of the related factors [11].
In addition to psychological insulin resistance, patients with type 2 diabetes also experience lifestyle changes associated with diabetes management, changes in social activities, and high emotional stress concerning diabetes complications [12]. This experience is referred to as “diabetes distress.” Diabetes distress represents a negative emotional response from the patient to their own lives as individuals learning to live with diabetes [13]. Diabetes distress can have the physiological effect of elevating blood sugar by activating cortisol, growth hormones, and endorphin [12]. This distress is also known to have negative emotional effects. For example, it can hinder self-care and therapy adherence by lowering the will to manage diabetes [14]. Consequently, it is important to reduce diabetes patients' negative attitudes toward disease therapy and their own lives, in order to increase therapy adherence. Moreover, in many patients, the negative response toward insulin therapy is based on the belief that they will lose control over their own lives once insulin administration begins. Therefore, the confidence that they can prevent hyperglycemia and complications associated with diabetes and maintain their well-being can help increase insulin therapy adherence [9]. “Self-efficacy” refers to the ability of individuals to achieve their desired outcome or effect. Individuals with high self-efficacy not only think and behave in a manner that supports their aims but also tend to put more effort into problem-solving, which enables them to better overcome crises [15]. “Patient self-efficacy” refers to the ability of a patient to manage disease-related factors; when self-efficacy is high, the patient has positive thoughts about overcoming his or her disease and puts greater effort into adapting to treatment [16].
Berg and Upchurch's [17] model of couples coping with chronic illness suggests that the stress and disease awareness of patients interacts with the stress and disease awareness of their spouses. Such evaluative factors have a mutual effect on the process of patient and spouse coping and adapting to the disease. Because the couple's relationship is one of high interdependency, the psychological insulin resistance and diabetes distress of the patient with type 2 diabetes affects that of the spouse. The self-efficacy of the spouse refers to his or her level of confidence in providing physical and/or emotional care to the patient [18]. Thus, spouses with high self-efficacy have lower negative emotions while caring for patients, which allows them to provide better care and affects the self-efficacy of the patient, helping the patient to have a more positive attitude toward the therapy process [19]. Consequently, the diabetes self-efficacy of a patient with type 2 diabetes and his or her spouse can increase therapeutic effect by reducing negative emotions regarding therapy and increasing adherence to therapy. However, most Korean studies on insulin therapy adherence in patients with type 2 diabetes have only considered the patient's perspective, and studies on psychological insulin resistance have been limited to concept analyses and the development of measurement tools.
The present study applied the actor-partner interdependence model (APIM) [20] to its analysis of variables related to the insulin therapy adherence of patients with type 2 diabetes that apply to both the patient and his or her spouse. When dyadic data are treated as individual data, the dynamics between couples cannot be examined. Even if the data are collected from both members of a couple, analysis of such interdependent data as independent data would violate the major hypothesis of inferential statistics that the data are independent. Accordingly, the standard error would appear lower than it is, and type I error may occur. The APIM [20], a model for dyadic data analysis, can be used to analyze the data of interdependent dyads. Psychological insulin resistance, diabetes distress, diabetes self-efficacy, and insulin therapy adherence of patients with type 2 diabetes and their spouse must be analyzed by dyadic analysis. The purpose of this study was to identify the effects of psychological insulin resistance, diabetes distress, and the diabetes self-efficacy of patients and their spouses on insulin therapy adherence of patients with type 2 diabetes using APIM.
This study used path analysis based on a couple analysis method to identify the actor and partner effects of psychological insulin resistance, diabetes distress, and diabetes self-efficacy on insulin therapy adherence of patients with type 2 diabetes.
The study sample consisted of patients with type 2 diabetes at Gyeonggi Provincial Medical Center Pocheon Hospital and Hallym Hospital in Incheon City, and their spouses. The inclusion criteria were as follows: (1) adults aged 19 years or older, (2) patients who have been diagnosed with type 2 diabetes and are undergoing insulin therapy, (3) patients capable of communicating in Korean, (4) patients who understood the objective of the study and volunteered to participate in the study, and (5) the spouse of a patient (defined as the current common-law partner).
Since the appropriate sample size for the path analysis was ≥200, the study considered a drop-out rate of 10% and selected 220 patients with type 2 diabetes and their spouses. Of the 220 sets of questionnaires distributed, 200 (91.1%) were retrieved; accordingly, a total of 200 questionnaires were used in the final analysis.
Psychological insulin resistance was measured with the Korean version of the Psychological Insulin Resistance Measurement Tool developed by Song [3]. The tool was used with permission from its developer. The Psychological Insulin Resistance Measurement Tool consists of 18 items divided into two sub-domains: cognitive/psychological factors and support factors. Response for each item are based on a 5-point scale, with higher scores indicating a higher level of psychological insulin resistance. The reliability of the tool at the time of development was Cronbach's α=.75~.85. In this study, the reliability of the Korean version of the Psychological Insulin Resistance Measurement Tool was Cronbach's α=.81~.87 for the patients and Cronbach's α=.83~.87 for the spouses.
The Korean version of the Diabetes Distress Scale, originally developed by Polonsky et al. [13] and modified and translated into Korean by Choi [21], was used with permission from the developer and translator. The scale consists of 17 items: 5 items on emotional burden, 4 on physician distress, 5 on regimen distress, and 3 on interpersonal distress. Responses are based on a 5-point Likert scale. The frequency of feeling stress in the past month is scored on a 5-point scale (1=”not at all” to 5=”always”), with higher scores indicating a higher level of stress. The reliability of the Korean version of the Diabetes Distress Scale at the time of development was Cronbach's α=.87. In this study, the reliability was Cronbach's α=.88 for the patients and Cronbach's α=.91 for the spouses.
The Diabetes Self-Efficacy Scale developed by Rapley et al. [22] was used after modifying and supplementing some of the items according to the objective of the present study. This scale consisted of a total of 18 items in 5 subdomains (routine diabetes check-up, confidence in self-care, self-control, exercise management, and nutrition management). Each item was scored on a 5-point scale with higher scores indicating higher self-efficacy. Among these items, items 3, 4, 7, 8, and 11 were reversed according to developer's guideline [22]. The reliability of the scale at the time of development was Cronbach's α=.61~.76. In this study, the reliability was Cronbach's α=.78 for the patients and Cronbach's α=.76 for the spouses.
Permission to use the Morisky Medication Adherence Scale [23] was obtained from the original author, and the scale translated into Korean was obtained and modified according to this study's objective. The scale consists of four items with “Yes”(1) or “No”(0). The total score ranges from 0 to 4 points. The reliability of the scale at the time of development was Cronbach's α=.61. In this study, the reliability was Cronbach's α=.72.
Data were collected in the period between February 25 and May 1, 2019, from patients diagnosed with diabetes at Gyeonggi Provincial Medical Center Pocheon Hospital and Hallym Hospital in Incheon City, and the spouses of those patients.
This study was conducted after receiving approval from the Public Institutional Review Board of the Ministry of Health & Welfare (IRB No. P01-201902-22-004). Before the study, details about the study and recruitment of participants were explained through the relevant department, and permission was obtained. Prior written informed consent was obtained from each participant after they had been provided with an explanation of the objective and procedures of the study. The consent form contained information on the researchers, descriptions of the objectives and methods of the study, and explanation that personal information would not be released for any reason other than those related to the study's objective, that participation in the study was voluntary, and that participants were free to cease participation in the study at any time. We preserved their anonymity by encoding private information.
Data were analyzed using SPSS-WIN Version 20.0 and AMOS Version 20.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics of SPSS were used for descriptive statistics of the general characteristics of the participants and measured variables. For the data normality test, skewness and kurtosis of the measured variables were verified, and multivariate normality was verified using AMOS. Correlations between each variables and multicollinearity were verified by Pearson correlation coefficients. Cronbach's α was used to verify the reliability of each tool. To test the actor and partner effects of psychological insulin resistance, diabetes distress, and diabetes self-efficacy of patients with type 2 diabetes and their spouses on insulin therapy adherence, an analysis was performed using AMOS structural equation modeling. A measurement invariance test was performed to confirm that the participant data had homogeneous meaning within a single measurement tool. The maximum likelihood method was used to test the fitness of the study model, and a confirmatory factor analysis was performed to verify the validity of latent variables for model analysis. The fitness of the model was assessed by absolute fit indices: χ2, χ2/df, root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), goodness of fit index (GFI), adjusted goodness of fit index (AGFI), comparative fit index (CFI), normed-fit index (NFI) and the Tucker-Lewis index (TLI). The statistical significance of direct, indirect, and total effects was tested by bootstrapping.
The mean age of the patients and spouses was 60.75±13.22 (range: 29~84) and 53.76±12.69 (range: 24~89) years, respectively. For employment status, 104 patients (52.0%) and 126 spouses (63.0%) were employed. For previous insulin-related education, 130 patients (65.0%) and 96 spouses (48.0%) had previous experience participating in insulin-related education. For monthly household income, 3,000,000~4,999,999 won was the most common response with 73 households (36.5%).
Normal distribution was confirmed based on the absolute skewness not exceeding 2 (−0.45~0.12) and absolute kurtosis not exceeding 4 (−0.49~1.22). Each measured variable showed statistically significant correlation at a significance level of .05, and the absolute value of correlations between the variables did not exceed .80, indicating that there was no problem with multicollinearity (Table 1).
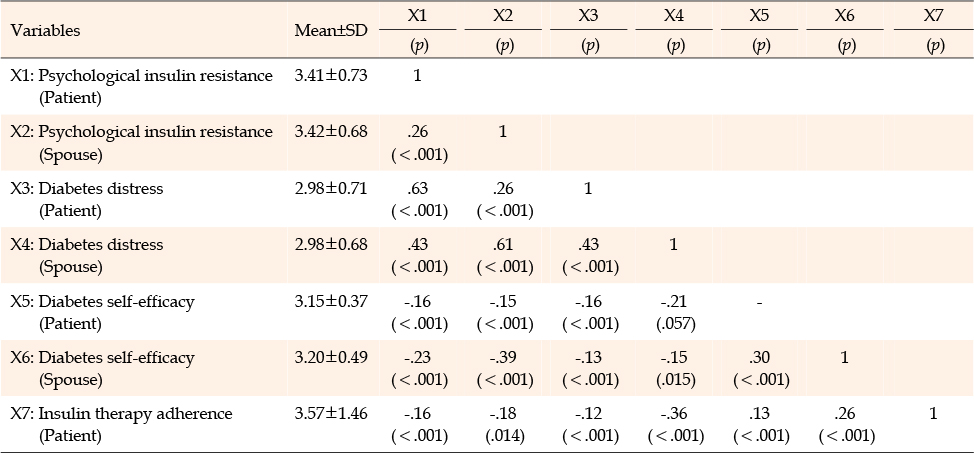
Table 1
Correlations of the Variables (Patients N=200; Spouses N=200)
To confirm that psychological insulin resistance, diabetes distress, and diabetes self-efficacy data of patients with type 2 diabetes and spouses have homogeneous meaning within a single measurement tool, a measurement invariance test was performed, and four competitive models were compared. The first model was the base model. The second was the model with factor coefficients constrained. The third was the model with error covariance constrained. The fourth was the model with factor coefficients and error covariance constrained. Comparison of fitness in the present study was based on TLI, CFI, and RMSEA, which are not sensitive to the number of cases and χ2; consequently, the measurement invariance was confirmed (Table 2).
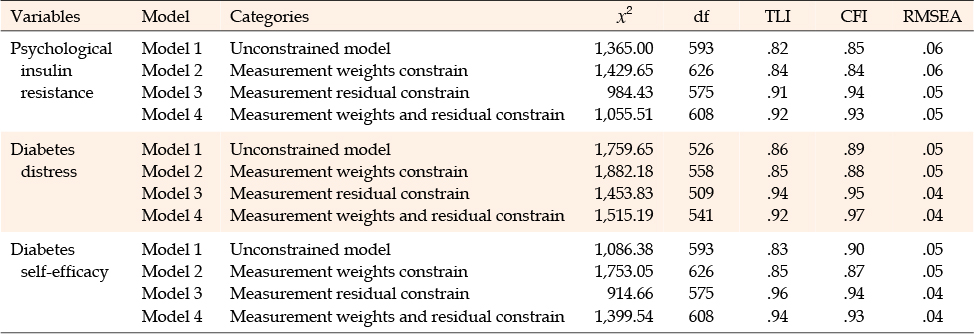
Table 2
Test of Measurement Equivalence
To test the effects of psychological insulin resistance, diabetes distress, and the diabetes self-efficacy of patients with type 2 diabetes and spouses on the insulin therapy adherence of patients, the normality of measured variables was tested. The univariate normality of each measured variable satisfied the conditions for normal distribution, with absolute skewness and kurtosis showing a range of value below 2, but multivariate normality was not satisfied at a significance probability level of .05 with multivariate skewness of 8.13 and critical ratio of 4.26. When multivariate normality is not satisfied, upward biasing of the threshold value may occur during parameter estimation. However, there have been reports indicating that, even if multivariate normality is not assumed, estimated parameters are reliable if the maximum likelihood method is used. Moreover, if the sample size is≥120, then the maximum likelihood method could be used for estimation by non-normal data. Based on these reports, the model was estimated without converting the data. The fitness of the hypothetical model was assessed by GFI, AGF, CFI, NFI, TLI, RMSEA, and SRMR. Goodness of fit index, AGFI, CFI, NFI, and TLI values ≥.90 was interpreted as showing good fitness of model, whereas RMSEA and SRMR values of <.05 was considered to indicate good fitness, with <.10 as average fitness and ≥.10 as poor fitness. When the maximum likelihood method was used to test the hypothetical model of the present study, the results showed χ2=13.47, df=6, RMSEA=.04, SRMR=.05, GFI=.97, AGFI=.95, CFI=.98, NFI=.96, and TLI=.90. Because these results showed that the fitness of the model was suitable, the model was confirmed. In the present study, 6 out of 10 hypotheses were selected (Table 3).
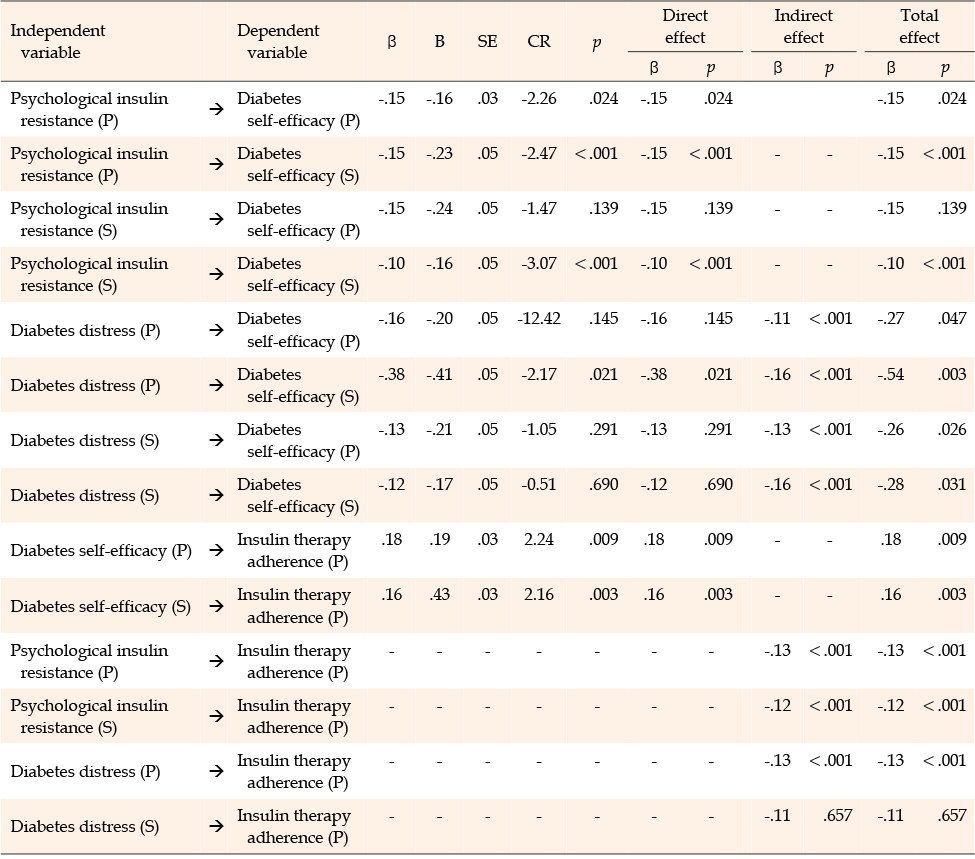
Table 3
Dyadic Effects of Hypothetical Model
Psychological insulin resistance of the patient had an actor effect (β=−.15, p=.024) on diabetes self-efficacy and partner effect (β=−.15, p<.001) on diabetes self-efficacy of the spouse. Stress of the patient had a partner effect (β=−.38, p=.021) on diabetes self-efficacy of the spouse. Psychological insulin resistance of the spouse had an actor effect (β=−.10, p<.001) on diabetes self-efficacy, while diabetes self-efficacy of the patient (β=.18, p=.009) and spouse (β=.16, p=.003) were found to have a direct effect on insulin therapy adherence of the patient. Moreover, psychological insulin resistance (β=−.13, p<.001) and diabetes distress (β=−.13, p<.001) of the patient and psychological insulin resistance (β=−.12, p<.001) of the spouse were found to have a diabetes self-efficacy mediated indirect effect on the insulin therapy adherence of the patient.
The purpose of this study was to identify the effects of psychological insulin resistance, diabetes distress, and diabetes self-efficacy of patients and their spouses on the insulin therapy adherence of patients with type 2 diabetes.
First, the psychological insulin resistance of patients with type 2 diabetes showed actor and partner effects on diabetes self-efficacy. This was consistent with the model proposed by Berg and Upchurch [17], who claimed that stress and disease awareness in patients interact with stress and disease awareness perceived by their spouse, while such evaluative factors mutually affect the process of patient and spouse coping and adapting to the disease. Because patients with type 2 diabetes need to personally administer insulin therapy, which is more complicated than therapies for other diseases [8], psychological insulin resistance, which is a negative emotion, is believed to affect the diabetes self-efficacy needed for efficient self-management of the disease. In particular, patients often need to rely on their spouse to help with insulin therapy; the psychological insulin resistance of the patient affects the diabetes self-efficacy of the spouse. Moreover, the psychological insulin resistance of the spouse also affects the diabetes self-efficacy of the spouse. Ultimately, the psychological insulin resistance of patients with type 2 diabetes is not only a problem for the patient, but it is a negative emotion that can also occur in the spouse. Considering that diabetes self-efficacy plays an important role in increasing the drug and insulin therapy adherence of the patient [9], medical professionals should provide interventions that target the psychological insulin resistance in both the patient with type 2 diabetes and the spouse.
Second, the stress of patients with type 2 diabetes was found to affect the diabetes self-efficacy of the spouse. The disease awareness and stress of the patient interact with the perceived disease awareness and stress of the spouse [17]; thus, the diabetes-related stress experienced by the patient is believed to affect the diabetes self-efficacy of the spouse. In particular, the spouse of a patient with type 2 diabetes performs various diabetes management activities, such as insulin administration, dietary management, and skin care, in daily life together with the patient. Thus, negative emotions of the patient that are related to the disease can lower the level of confidence the spouse has in providing physical and/or emotional care to the patient [18]. However, self-efficacy of the spouse can be a driving force for performing patient care work, which, consequently, can lead to the patient having a more positive attitude toward the therapy process [19]. Therefore, medical professionals should develop and implement stress management programs for patients with diabetes, to increase the diabetes self-efficacy of the spouse. Such programs are likely to have positive therapeutic effects for patients with type 2 diabetes.
Third, the diabetes self-efficacy of the patient and spouse were identified as factors that affect the insulin therapy adherence of the patient. This was consistent with a previous study on patients with diabetes [24] that reported that diabetes self-management education that included family members had a positive effect on diabetes management and maintenance by having a positive effect on the self-management behavior and self-efficacy of the patient. In particular, diabetes self-efficacy can directly strengthen self-management and improve the diabetes therapy adherence of the patient to have a long-term effect of lowering glycated hemoglobin levels [25]; thus, it is necessary for medical professionals to include the spouse in diabetes programs and education for the patient to improve the insulin therapy adherence of patients with type 2 diabetes.
Based on such findings, it is important to consider both the patient and spouse when addressing the insulin therapy adherence of patients with type 2 diabetes. In particular, the psychological insulin resistance of the patient and insulin resistance of the spouse can affect the diabetes self-efficacy of the patient and spouse concerning the therapy process, which ultimately affects the patient's therapy adherence. Therefore, it is necessary for medical professionals to develop interventions that can lower psychological insulin resistance and increase the diabetes self-efficacy of both the patient and spouse. However, it is necessary to conduct future longitudinal studies for an in-depth analysis of the effects of psychological insulin resistance, stress, and the diabetes self-efficacy of patients and their spouses on insulin therapy adherence. This study did not analyze the insulin therapy adherence of patients by age group. In future studies, it is necessary to grasp the degree of insulin therapy adherence perceived by patients and caregivers by age group and to determine factors affecting insulin therapy adherence.
The present study was conducted to identify the effects of psychological insulin resistance, diabetes distress, and the diabetes self-efficacy of patients with type 2 diabetes and their spouse on the insulin therapy adherence of patients. The findings provide basic data for the development of programs that can enhance the insulin therapy adherence of patients with type 2 diabetes from the perspectives of both the patient and spouse.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - HJW.
Data collection - KJS and PJH.
Analysis and interpretation of the data - HJW.
Drafting and critical revision of the manuscript - KJS, PJH, and HJW.
 E-SUBMISSION
E-SUBMISSION