
This study aimed to determine the effect of self-regulation and social support on post-stroke patients experiencing urinary incontinence.
This quasi-experimental study was conducted in Kota Kendari, Indonesia. Through consecutive sampling, 53 participants were selected: 26 in the experimental groups and 27 in the control group, studied over a period of four weeks. The self-regulation intervention included education about properly following recommended exercises to overcome urinary incontinence, focusing on goals, being optimistic, and having emotional control. The social support intervention included the provision of family and peer support during patient care. Differences in participants' quality of life was measured at three different stages during the study, using the Incontinence Quality of Life instrument. Data were analyzed using descriptive statistics, independent t-tests, and repeated measures ANOVA.
There was homogeneity of variance in both groups. Significant differences in quality of life were seen in the second and third measurements (p<.001). The interventions improved patients' quality of life by 6.43 times at 4 weeks, and 13 times at 8 weeks.
Self-regulation and social support played an important role in improving the quality of life of post-stroke urinary incontinence patients. Further studies with longer intervention periods are required to validate our results and contribute to better patient experiences.
Post-stroke Urinary Incontinence (UI) is common consequence following acute strokes, which affects more than a third of hospitalized stroke patients, with nearly a quarter of patients experiencing UI for up to a year [1]. In addition to increasing physical weakness [1], impaired motor, cognitive, and psychological functions are also risk factors for post-stroke UI [2]. Patients' difficulty in physically accessing their bathrooms to urinate is also related to the physical limitations and weaknesses they experience. The most common cognitive disorders experienced by stroke patients are memory disorders (e.g., forgetting where the bathroom is located) and communication disorders (aphasia) in which patients find it difficult to express their desire to urinate [1]. Further, anxiety can directly affect bladder function, causing changes in bladder pressure [3]. In addition to anxiety, post-stroke UI is also associated with depression. Depression has been reported to occur 2.4 times more frequently in UI patients [4]. Together, anxiety and depression can affect patients' ability to take action to cope with their illness. Moreover, patients who are affected by UI rarely talk about their condition because they feel embarrassed [2], even though they consider UI to hinder their social functioning and activities of daily living [4]. For instance, patients often choose not to leave their houses due to the fear and embarrassment of urinating in public, feeling wet, and smelling of urine [5].
Systematic reviews and meta-analyses have also corroborated that UI is associated with poorer quality of life [6], greater dependence in basic Activities of Daily Living (ADL), decreased participation in activities, and low life satisfaction [7]. To the best of our knowledge, there have not been any rigorous evaluations of interventions designed to manage UI after strokes in secondary care [8], or studies identifying efforts to maintain patient continence care in homes [9]. Behavioral treatments have been recommended as the first interventions for UI management [2, 10]. Based on recommendations from the Agency for Health Policy and Research Guidelines (APCHR) and the International Consultation on Incontinence that UI intervention is minimally invasive, behavioral treatments should be initiated early [11].
Behavioral and physical treatments have been found to improve patients' conditions. For instance, the results of our previous qualitative study found that patients who successfully coped with UI had done pelvic floor muscle training, strength training, and walking exercises, so that they were physically able to urinate in the bathroom [12]. They also trained themselves to think positively, enthusiastically, patiently; sought information related to treatments and medications for UI care; and needed family support in improving their ability to perform ADL [12]. Furthermore, self-regulation has been found to lead to improved self-management [13]. Self-regulation is generally defined as the “capacity” or “ability” for performing volitional activities, such as goal-setting, self-monitoring, activating and utilizing goals, implementing, self-evaluating, self-consequating, self-efficacious behavior, and meta-skills [14]. According to Bandura, the self-regulatory system is at the core of causal processes; not only does it mediate the effects of most external influences, but it also provides the very basis for purposeful action [14]. Self-regulation emphasizes the active roles that individuals can play to enhance their health, and prevent or alleviate the effects of illnesses [15].
Self-regulatory and motivational skills are required for self-management [16]. Self-regulation models vary in their specifics, but are rooted in three generic sub-functions, namely: self-monitoring of health-related behavior; social and cognitive conditions under which one engages in monitoring, and adopting goals toward the same; and self-reactive influences, including self-motivating and social support, to sustain healthful practices [16].
Previous studies have recommended the provision of social support interventions along with cognitive behavior treatment for UI patients [3, 17]. Peer support, when provided through sharing of experiences and health information, could help reduce feelings of isolation and fear [18]. Patients with histories of moderate or severe strokes, who received substantial social support, showed significantly improved functional status as compared to those who received less support [19].
In view of the scarcity of studies investigating interventions for UI, and the potential of behavioral and social interventions for reducing UI, the aim of this study was to determine the effects of self-regulation and social support on the quality of life of post-stroke UI patients.
This quasi-experimental study used a non-equivalent control group pretest-posttest design.
This study was conducted in four hospitals in Kota Kendari, Sulawesi Tenggara, Indonesia; namely: Regional Public Hospital Kota Kendari, Indonesian Army Hospital Dr. R. Ismoyo, Bhayangkara Hospital, and Aliyah I Hospital Kendari. The research period began in November 2020 and ended in March 2021.
The participants were post-stroke patients who had tested negative (non-reactive) for Coronavirus Disease-2019 (COVID-19) based on results from the Severe Acute Respiratory Syndrome Coronavirus-2 (SARS CoV-2) antibody serology test. Inclusion criteria were as follows: 1) stroke diagnosis by a doctor; 2) experience of post-stroke UI; 3) medically stable condition; 4) alert and conscious; 5) no known cognitive impairment (determined using the Indonesian version of the Montreal Cognitive Assessment (MoCa-Ina) with a value of ≥25); and 6) no experience of dysphagia.
Convenience sampling was used, and participants were divided into experimental and control groups using hospital matching. The experimental group comprised of patients from the Regional Public Hospital Kota Kendari and the Indonesian Army Hospital Dr. R. Ismoyo, while the control group comprised of patients from the Bhayangkara Hospital and Aliyah I Hospital Kendari.
The sample size was calculated using G*Power 3.1 software, with the assumption of α for a 5% interval, a test power of 80%, and obtained an effect size of 0.47 [20, 21]. The experimental group and control groups each required at least 26 participants. Considering the expected drop-out rate of 5~10%, 28 participants per group were included. Subsequently, two participants dropped out from the experimental group (one passed away and another did not respond); one participant from the control group also passed away. The final respondents were 53 patients: 26 in the experimental group and 27 in the control group.
This study was approved by the ethical committee of affiliated university (Faculty of Nursing Universitas Indonesia), with reference number: SK-242 / UN2.F12.D1.2.1 / ETIK.FIK.2019. All respondents signed an informed consent form, and received compensation in the form of stationery and educational information related to post-stroke UI.
Demographic data including gender, education, marital status, and age were collected. Clinical information included comorbidity, type of hemiparesis, type of stroke, type of UI, and the severity of UI. Quality of life was measured using the Incontinence Quality of Life (I-QOL) instrument, developed by The Scientific Advisory Committee Medical Outcomes Trust [21]. The I-QOL questionnaire was obtained from the owner of the questionnaire (via email) with permission to use it. The I-QOL contains 22 items across 3 subscales: avoidance and limiting behavior (8 items), psychosocial impacts (9 items), and social embarrassment (5 items). Each subscale uses a Likert scale ranging from ratings of 1 (very) to 5 (not at all) for each item. A higher I-QOL score indicates a better quality of life [22, 23]. The I-QOL score was calculated on a scale of 0~100 for easy interpretation [23]. The I-QOL also demonstrated reliability, with a Cronbach's α of .89, indicating its eligibility to be used for measurement. Each subscale also showed acceptable α values (.81 for behaviors, .79 for psychosocial impacts, and .68 for social embarrassment).
Before beginning the intervention procedure for the experimental group, the researchers and research assistants (nurses) assessed participants' urinary history data. The self-regulation component was implemented by educating patients about UI, and motivating them to be enthusiastic about performing recommended exercises such as bladder retraining, pelvic floor muscle training, Range of Motion (ROM), and walking. During the intervention, patients were encouraged to focus on their goals, be optimistic, and be able to control their emotions by practicing preferred distraction techniques such as counting down, listening to music, watching television, reading newspapers, performing dhikr, reading scriptures, and playing games. Dhikr was performed quite frequently, by praying or praising God. The social support component was implemented with the assistance of family and peers. Family members provided support in every activity such as helping patients meet their daily needs, transporting them for therapy sessions, contributing financially, etc. Peers provided encouragement and shared experiences of UI so that patients felt solidarity and confidence about overcoming UI.
The intervention period was four weeks. During the first week, the researchers and nurses provided 45~60 minute long educational sessions about post-stroke UI and coping skills training (bladder retraining, pelvic floor muscle training, and ROM) to patients and their families, first in the hospitals and then at patients' homes. Patients and families were encouraged to demonstrate the exercises that had been taught and were motivated to continue performing them. During the second week, researchers taught patients and families about the practice of distraction techniques, and motivated them to remain optimistic about and focused on treatment goals. Researchers also contracted time with patients and families for meetings with peers via telephone or video calls. Meetings with peers were held one each in the second and third weeks, with each call lasting for 30 minutes. Researchers facilitated the introductions and conversations of patients, families, and peers. During the fourth week, patients' physical abilities were monitored and evaluated through 2~3 home visits and telephone calls.
In contrast, participants from the control group only received exercises from rehabilitation clinics during the study; however, they did receive the aforementioned self-regulatory and social support intervention after the research period.
Researchers and nurses conducted data collection. Nurses, in their capacity as research assistants, first received training on how to fill the I-QOL questionnaire. Data collection was conducted thrice: before the intervention (week 0; pretest), after 4 weeks following week 0 (posttest 1), and after 8 weeks following week 0 (posttest 2). Researchers collected pretest data, while nurses collected posttest data.
SPSS version 24 was used for data analysis. Descriptive analysis was used to describe the participants' demographical as well as clinical information. The normality and homogeneity of the experimental and control groups data were tested, using the Shapiro-Wilk test and the Levene test, respectively. Following these analyses, bivariate analysis was conducted using independent t test and repeated measures ANOVA.
The majority of participants were women (58.5%). Most participants had acquired only a high school level of education (41.5%), were married (47.2%), had experienced non-hemorrhagic stroke (100.0%) with left-sided hemiparesis (56.6%), had hypertension comorbidity (39.6%), as well as mixed incontinence (functional+stress+urgency) (54.7%), and very severe incontinence (50.9%). The average age of participants in the experimental group was 56.54 years (Standard Deviation [SD]=12.58, range=31~75 years old) and in the control group was 54.93 years (SD=13.48, range =16~73 years old). The average elapsed time (in days) after stroke diagnoses in the experimental group was 5.04 days (SD=0.66, range=4~6 days) and in the control group was 5.00 (SD=0.62, range=4~6 days). There were no significant differences in age and in average time elapsed after acute stroke diagnoses, between the experimental and control groups (p=.935 for age distribution, p=.586 for average time elapsed after acute stroke diagnose) (Table 1). The average age of informal caregivers in the experimental group was 39.04 years (SD=11.38, range=21~58 years old) and in the control group was 44.89 years (SD=8.49, range=33~59 years old). Informal caregivers in both groups were participants' biological children, who had also only acquired high school education. There were no significant differences in caregivers' ages, relationships with participants, and education, between the experimental and control groups (p>.05).
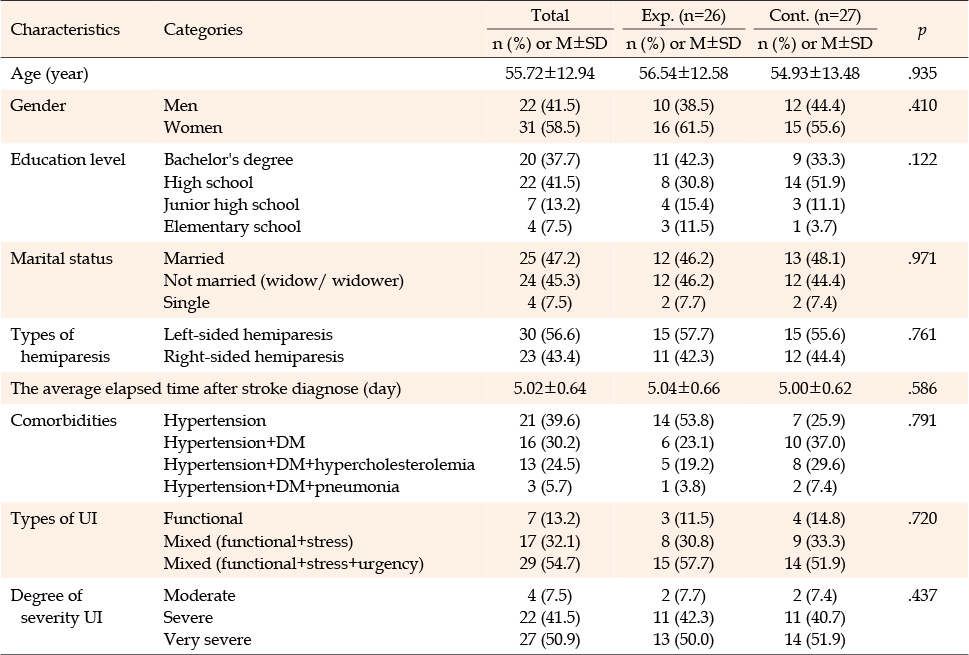
Table 1
Homogeneity Test of General Characteristics and Categories between the Two Groups (N=53)
Results from the normality test revealed similar distributions of quality of life in both groups, where both groups were normally distributed (p>.05 for each group). Results from the homogeneity test obtained p=.837, indicating that the two groups had the same variation of data, making the data eligible for parametric tests such as independent t-tests and repeated measures ANOVA.
Statistical analyses revealed that after the intervention, mean quality of life scores of participants from both groups increased between the first and third measurements. However, there were significant differences in the second measurement and third measurement (p<.001). The results of the repeated measures ANOVA (p<.001) indicated interactions between the first, second, and third measurements, and the experimental and control groups. The results of pairwise comparisons showed that the intervention was effective in improving the quality of life by 6.43 times at 4 weeks (second measurement) and 13.00 times at 8 weeks (third measurement) (Table 2).
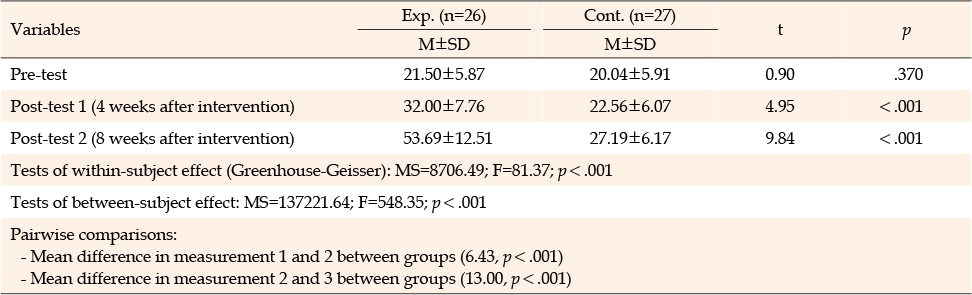
Table 2
Differences in Quality of Life between the Two Groups (N=53)
In the experimental group, scores for all quality of life items increased significantly after the intervention (p<.05) (Table 3). The items that increased the most in the third measurement were avoidance and limiting behavior.

Table 3
Differences in Quality of Life according to Three Variables between the Two Groups (N=53)
This study demonstrated that self-regulation and social support improve the quality of life of post-stroke UI patients. The experimental group, which received the intervention, showed higher and improved quality of life scores than the control group. Although quality of life was not maximized in 8 weeks, self-regulation made patients diligent toward exercising for overcoming UI. Self-regulation has been associated with many adaptive skills and desirable mental and physical outcomes across the life span [24], indicating that this behavioral change may continue improving patients' lives. The face-to-face, in-person education provided by researchers also contributed to improving patients' quality of life, given that the elderly ages of participants meant that tele-education may not have been the most optimal educational method [25].
Moreover, bladder retraining to encourage bladder emptying at regular time intervals has been demonstrated to be an effective method for treating incontinence [2]. In this study, it contributed to participants' bladder emptying times gradually increasing (10~15 minutes); participants were able to resist the urge to urinate immediately and attempted to urinate in the bathroom; and the average frequency of urination decreased, especially during night-time, from waking up 1~2 times each night to once a week. Bladder retraining also requires patients to be motivated to actively participate in treatment [26].
Actively performing ROM and walking exercises, and being involved in daily activities such as helping with housework, and meeting needs related to personal hygiene such as bathing, dressing, and walking to the bathroom when required, also contributed to improved quality of life. These findings corroborate those of other studies claiming that daily activity training can improve quality of life [27].
Participants of this study had experienced strokes accompanied by UI during the COVID-19 pandemic. Hence, family and peer support seemed to be particularly helpful for patients to cope with their conditions. Social support can serve as a protective buffer toward the perceptions of quality of life [28], and is a significant factor toward overcoming health-related problems [29]. Additionally, high levels of social support have been associated with better mental health [30].
Based on the analyses of three quality of life subscales, the results of this study aligned with previous findings demonstrating increased avoidance scores (p=.045) after 8 weeks of pelvic floor muscle training [31]. This could be attributed to participants' increased ability to manage their conditions related to UI, and these motor skills may be responsible for improving their continence [32].
There were some limitations of this study. There was a potential for selection bias in the participants in this study; differences in age characteristics in the two groups could have influenced our outcome variables. The limited sample size may also have influenced our analysis in identifying major changes in this study. Additionally, the relatively short study period was insufficient to demonstrate major changes in participants' quality of life which could have affected the results.
This study revealed that self-regulation and social support play an important role in improving the life quality of post-stroke UI patients. Further studies with longer intervention periods are required to validate our results and contribute to better patient life quality. Future studies may also compare the I-QOL with other similar instruments, such as those measuring health-related quality of life. Based on our findings, patient care programs can consider incorporating elements of self-regulation training and social support provision into their services for post-stroke UI patients, in order to improve patients' physical control and functioning.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design - HH, SR and ME.
Data collection - HH and NN.
Data analysis and interpretation - HH, SR, NN and ME.
Drafting of the article - HH, SR and NN.
Critical revision of the article - HH and ME.
This article is based on a part of the first author's doctoral dissertation from Universitas Indonesia.
This research was supported by PUTI Doktor 2020 funded by Direktorat Riset dan Pengembangan Universitas Indonesia.
 E-SUBMISSION
E-SUBMISSION