
Purpose
Patients with heart failure report low levels of physical activity and quality of life, both of which are important predictors of patient prognosis. This study aimed to investigate the effects of nurse-led motivational interviewing on self-efficacy for exercise, engagement in regular exercise, exercise capacity, and quality of life among patients with heart failure.
Methods
A randomized controlled trial design was used, and 66 Korean participants (i.e., 38 in a control group and 28 in an intervention group) aged 40~80 years who were diagnosed with heart failure were recruited between May 2012 and September 2013. The intervention group received telephone-based motivational interviews twice a week for one month. All participants were assessed for exercise regularity, levels of exercise, exercise capacity, and quality of life at baseline, one month, and three months. The data were analyzed using independent t-tests, repeated measures ANOVA, and nonparametric tests.
Results
At one month, there were significant group differences in exercise regularity (x2 =6.10, p=.013) and levels of exercise (Z=-2.56, p=.024). There was a significant group-by-time effect on the quality of life (F=3.76, p=.044).
Conclusion
Nurse-led motivational interviewing was effective in increasing exercise levels and quality of life in patients with heart failure. In the future, we propose a study with a larger number of participants and a long-term follow-up study with additional contact to maintain the intervention effect.
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-
Patients with heart failure report low levels of physical activity and quality of life, both of which are important predictors of patient prognosis. This study aimed to investigate the effects of nurse-led motivational interviewing on self-efficacy for exercise, engagement in regular exercise, exercise capacity, and quality of life among patients with heart failure.
A randomized controlled trial design was used, and 66 Korean participants (i.e., 38 in a control group and 28 in an intervention group) aged 40~80 years who were diagnosed with heart failure were recruited between May 2012 and September 2013. The intervention group received telephone-based motivational interviews twice a week for one month. All participants were assessed for exercise regularity, levels of exercise, exercise capacity, and quality of life at baseline, one month, and three months. The data were analyzed using independent t-tests, repeated measures ANOVA, and nonparametric tests.
At one month, there were significant group differences in exercise regularity (χ2=6.10, p=.013) and levels of exercise (Z=-2.56, p=.024). There was a significant group-by-time effect on the quality of life (F=3.76, p=.044).
Nurse-led motivational interviewing was effective in increasing exercise levels and quality of life in patients with heart failure. In the future, we propose a study with a larger number of participants and a long-term follow-up study with additional contact to maintain the intervention effect.
An estimated 64.3 million people live with heart failure worldwide [1]. In 2019, the hospitalization rate of heart failure patients in Korea was 88.4 per 100,000 patients, which was higher than that of patients with asthma [2]. The number of medical treatments such as coronary angioplasty, cardiac catheterization, or coronary artery bypass surgery due to the worsening of heart failure was 1,181 and medical costs increased to 15.7 billion won [3]. Patients with heart failure tend to report a reduction in Quality of Life (QOL) [4]. Low levels of QOL were associated with depressive and physical symptoms [5], and the longitudinal trajectories in QOL demonstrated that QOL differed significantly among patients with heart failure between survivors and non-survivors over a 12-month period [6]. Among those with heart failure, decreased physical function was one of the most common complaints [7], and notably, physical function was a strong predictor of mortality [6]. Low levels of QOL and poor physical function can be substantially improved by promoting healthy behaviors in patients with heart failure [8]. Exercise is a class I recommendation by the American College of Cardiology Foundation/American Heart Association Guideline for the Management of heart failure [9]. Exercise increases peak cardiac output, improves vascular reactivity, utilizes oxygen better through metabolic changes in the skeletal muscle, and facilitates more efficient ventilation [8]. In a previous study, heart failure patients with higher activity levels showed greater exercise capacity as measured by the 6-Minute Walk Test (6 MWT) [10]. A physically inactive lifestyle was found to correlate negatively with QOL and was identified as a significant predictor of QOL [7]. In addition, exercise training was associated with a 25.0% lower risk of all-cause hospitalization compared to usual care [8].
However, patients with heart failure engage in very limited amounts of exercise. According to a previous study [11], 42.0% of patients reported engaging in less than 60 minutes of exercise per week, and approximately two-thirds of patients had a low level of exercise [10], which corresponded to a total Physical Activity (PA) of <600 Metabolic Equivalent of Task (MET)-minutes/week according to the International Physical Activity Questionnaire (IPAQ). These results suggest that much of this population was relatively sedentary. According to a recent report [12], the rate of adherence to exercise guidelines was lower among Asians than among Caucasians. The reasons for decreased exercise among patients with heart failure included shortness of breath, exercise intolerance, and fatigue [9]. Among older adults with heart failure, poor adherence to exercise was strongly related to a lack of motivation for exercise, and the motivation and Self-Efficacy for Exercise (SEE) were significantly correlated [11]. SEE could be a mediator in the relationship between motivation and adherence to exercise [11], which implies that motivation could result in a change in SEE, which in turn could result in increased adherence to exercise. Therefore, strategies that aim to increase engagement in exercise among older adults with heart failure should address their SEE and motivation to exercise.
Motivational Interviewing (MI) is a collaborative convertsation that elicits change talk during counseling, evokes motivation, and strengthens patient commitment to the implementation of positive behavior changes [13]. Since older adults aged 60 and above value collaborative communication, MI can increase their motivation for change and enhance their responsibility for active participation and long-term adherence to an exercise program [4]. Riegel et al. conducted a study using a mixed method design and identified that MI techniques such as reflection and reframing, empathy, affirmation, and humor, and individualized problem solving contributed to improvement in self-efficacy and self-care among patients with heart failure [14]. Patients with heart failure showed an increase in PA and peak VO2 after receiving monthly MI intervention for six months [4]. In a systematic review of the literature on the effects of MI on patients with heart failure, MI demonstrated a positive effect on self-care behaviors, including exercise, QOL, and hospital readmission [15, 16]. Significant differences in self-care management have been observed among patients with heart failure at the three-month and six-month follow-up, after one face-to-face session and three telephone contacts provided by nurses over a two-month period [17].
While there are numerous benefits of MI, it has been applied narrowly to change behaviors in patients with heart failure. In a systematic review on the effects of MI on self-care behaviors, QOL, and hospital readmission in patients with heart failure, Poudel et al. [15] researched literature published from 1990 to 2019, and only nine articles were retained at the conclusion. While nurses provided MI in five out of nine articles [15], there were few studies that conducted MI in Korean patients with heart failure. Therefore, it is necessary to establish evidence for the effects of MI by conducting a study using a strictly controlled method, such as a Randomized Controlled Trial (RCT) for heart failure patients in Korea.
Nurse-led MI may improve patient outcomes in diverse areas such as medical-surgical units, intensive care units, oncology units, and home healthcare when used effectively [18]. We predicted that MI would play an important role in promoting engagement in exercise and maintaining exercise involvement among patients with heart failure by improving their SEE. Given this evidence, MI could be a promising target for regular exercise and exercise capacity alongside QOL in patients with heart failure in Korea. Furthermore, according to Katherine Letourneau, an Adult-Gerontology Nurse Practitioner, and Janice H. Goodman, a psychiatric and mental health clinical nurse specialist, MI alleviates the burden of healthcare providers who persuade patients to change their behaviors [19]. The purpose of this study was to examine the effects of nurse-led MI on SEE, regular exercise, exercise capacity, and QOL, and the sustainability of the effects over three months.
This study was an RCT with a repeated measures design that investigated the effects of MI on patients with heart failure over three months. Part of the one-month immediate effect of nurse-led MI was reported elsewhere as a result of a pilot study [20]. This trial was registered by the Clinical Research Information Service (CRIS) (No. KCT 0005300).
Individuals with a documented diagnosis of heart failure, who understood the purpose of the study and provided written informed consent, were eligible for participation. Participants were recruited from the outpatient clinics of three university-affiliated hospitals and one general hospital in South Korea. The inclusion and exclusion criteria are presented in Table 1. The sample size was calculated using G*Power version 3.1 program for repeated measures analysis of variance (ANOVA). A sample of 19 participants was required for each group to reach a power of β=.80, with an α-error probability of <.05, based on a middle effect size f=0.25. Based on previous studies in this population, the estimated attrition rate was 55.0% [20]; therefore, the target recruitment size was 88 participants. We approached 374 patients, however 286 patients were excluded because of a decline in participation, engagement in regular exercise, physical problems, or other reasons (Figure 1). A total of 88 eligible participants who provided informed consent were randomly assigned to an intervention or control group based on computer-generated numbers each week. Considering the high dropout rate of the intervention group [20], the randomization ratio between intervention group and control group was 6:4.
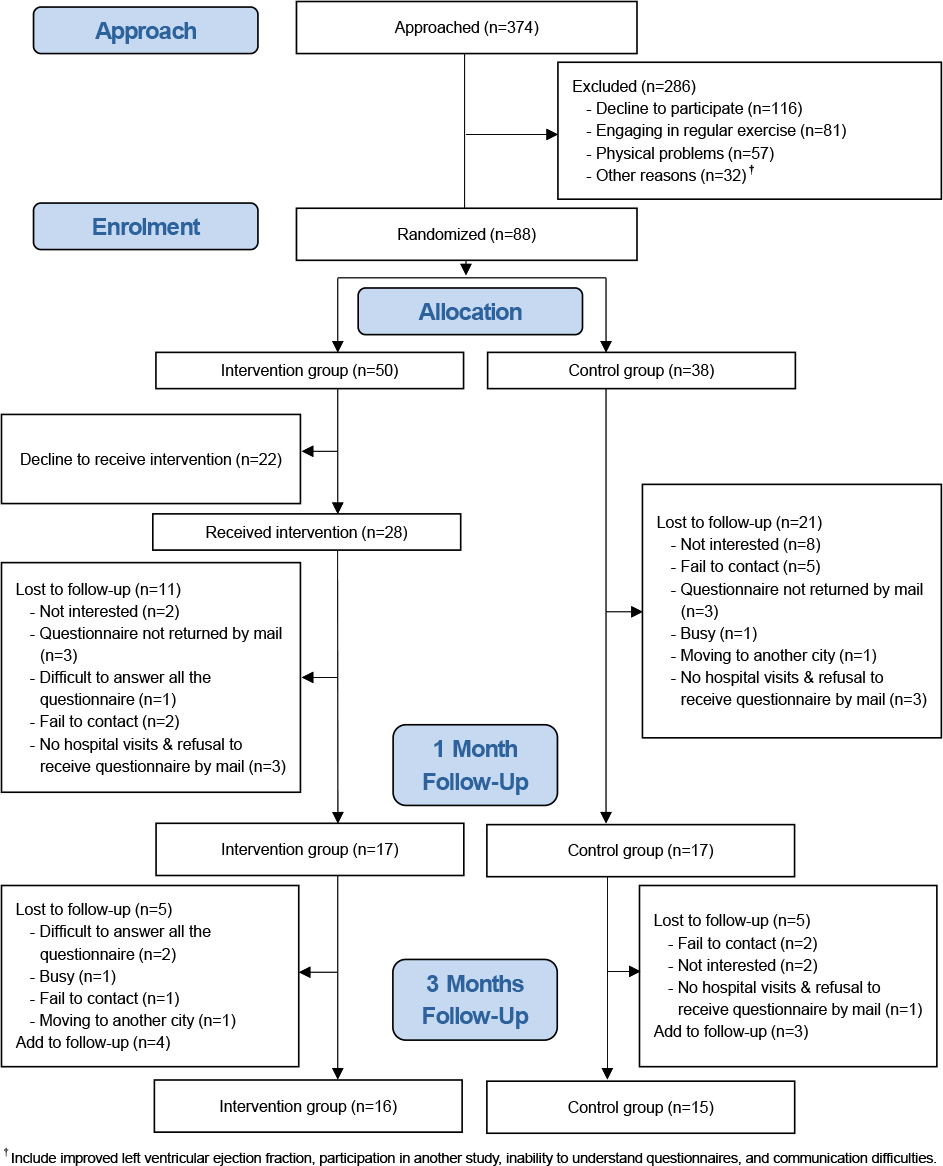
Figure 1
Flow diagram of the study.
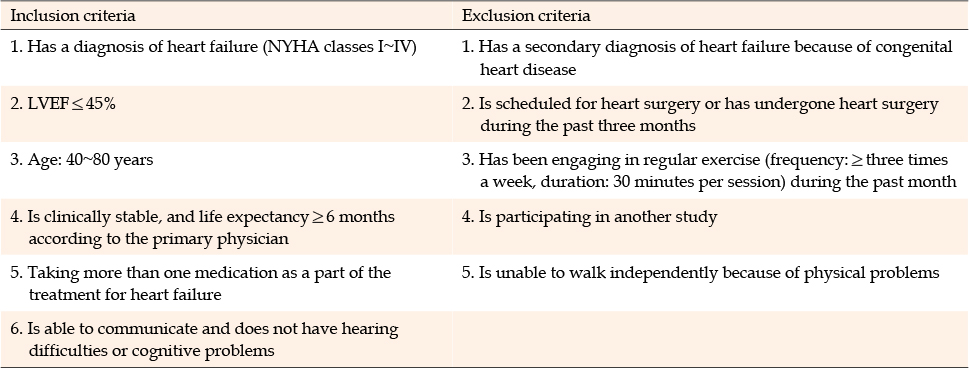
Table 1
Eligibility Criteria
At the one-month follow-up, 17 of 50 participants remained in the intervention group (dropout rate: 66.0%) and 17 of 38 participants remained in the control group (dropout rate: 55.3%). At the three-month follow-up, 16 of 17 participants remained in the intervention group (dropout rate: 5.9%) and 15 of 17 participants remained in the control group (dropout rate of 11.8%). Dropout analysis revealed that the baseline characteristics of dropout patients (n=57) and patients remaining until the end of the study (n=31) were not significantly different except for the comorbidities. Higher numbers of dropout patients tend to have comorbid conditions than those who remained until the end of the study (χ2=5.14, p=.023).
Baseline Characteristics The following baseline sociodemographic characteristics were measured: age, gender, marital status, educational level, total monthly family income, smoking habits, and alcohol consumption. The following baseline clinical characteristics were also measured: duration of heart failure, Left Ventricular Ejection Fraction (LVEF), New York Heart Association (NYHA) class for heart failure, comorbidities, Activities of Daily Living (ADL), and functional status assessed using the KASI. Data were collected using questionnaires and retrieved from medical records. The severity of heart failure was classified according to the NYHA criteria. ADL was measured using the Korean version of the ADL instrument (K-ADL). The original instrument was developed by Katz et al. [21], and Korean adaptation was developed by Won et al. [22]. Responses were recorded on a 3-point Likert scale. The total score ranged from 3 to 21. Higher scores were indicative of lower levels of engagement in ADL. The KASI consisted of 15 items that assess engagement in daily life and leisure activities (e.g., sports, housework, and sexual activity) [23]. Total scores ranged from 0 to 77, and higher scores were indicative of a better functional status. In the original validation study, the Spearman’s rank-order correlation coefficient that emerged for the relationship between scores on the KASI and time spent exercising on the treadmill was .62 (p<.001) [23].
SEE SEE was measured using the Self-Efficacy for Exercise scale developed by Resnick and Jenkins [24]. The SEE scale measures self-efficacy beliefs about one’s ability to continue exercising when faced with barriers, which measured the participants’ ability to regularly engage in 20 minutes of exercise three times per week. After obtaining approval from the developers to use the instrument, forward translation from English into Korean was performed independently by two researchers in the research team who were fluent in both English and Korean. Back translation was performed by two bilingual experts who were unfamiliar with the SEE. The back-translated SEE was reviewed by the researchers by comparing it to the original text and the concept of SEE. The researchers confirmed that most questions were similar to the original version and recommended a few minor changes in wording. Next, a preliminary test of the final translated questionnaire was conducted on Korean patients with heart failure. After completing the questionnaire, all respondents reported that they understood the content of the items, and we concluded that the translated questionnaire was acceptable. The scale consisted of nine items, and responses were recorded on a scale ranging from 0 (no confidence) to 10 (very confident). To obtain a total score, each response was added and divided by the number of items and multiplied by 10. The total scores ranged from 0 to 100, and higher scores were indicative of a higher level of SEE. In Resnick and Jenkins’s study [24], the internal consistency of the SEE scale was represented by Cronbach's α coefficient of .92, and the squared multiple correlation coefficients ranged from 0.38 to 0.76. In this study, the Cronbach's α coefficient was .93.
Levels of Regular Exercise The amount of regular exercise was computed using METs and the following formula: MET scores for the type of exercise × weekly frequency of exercise × duration of each session of exercise (minutes). MET-minutes/week was the unit for the level of exercise, and the MET scores for each type of exercise were derived from the study by Ainsworth et al. [25]. Generally, scores for walking, moderate PA, and vigorous PA represented 3.3, 3~6, and >6 MET scores, respectively [25]. Participants were asked to indicate whether they had exercised regularly during the past month, the frequency with which they exercised each week, and the duration for which they exercised at a given time.
Exercise Capacity Exercise capacity was assessed using the 6 MWT [26]. The 6 MWT is often used as an objective measure of exercise capacity in patients with heart failure [26]. Participants walked back and forth within a designated area of 60 meters in the hospital for 6 minutes. The distance walked in 6 minutes was recorded as the number of rotations, and this figure was converted into meters.
QOL QOL was assessed using the Kansas City Cardiomyopathy Questionnaire (KCCQ) developed by Green et al. [27]. The developers permitted us to use this instrument, and the publisher provided us with the Korean version of the KCCQ. The KCCQ is a disease-specific instrument. It assesses a higher number of clinically relevant domains than generic QOL instruments and is more sensitive to clinical changes. Responses are recorded on either a 5-, 6-, or 7-point Likert scale. The KCCQ consisted of 23 items and the following seven domains: physical limitation, symptom frequency, symptom burden, symptom stability, self-efficacy for coping with symptom aggravation, social limitation, and emotional QOL. The total scores ranged from 0 to 100, and higher scores were indicative of a better QOL. The Cronbach’s α coefficient for the subscale of self-efficacy for coping with symptom aggravation was .62 and the Cronbach’s α coefficient for the other subscales ranged from .78 to .95 [27]. In this study, the Cronbach’s α coefficient for the total scale was .94.
Figure 2 presents the conceptual framework of the study. In this study, MI was conducted by discussing participants’ perceived importance of behavior changes, severity of unhealthy behaviors, barriers to and benefits of healthy behaviors, and self-efficacy, which are the key variables embedded within the health behavior theory [13]. The four core counseling principles of MI included: expressing empathy, developing discrepancy, rolling with resistance, and supporting self-efficacy [13].
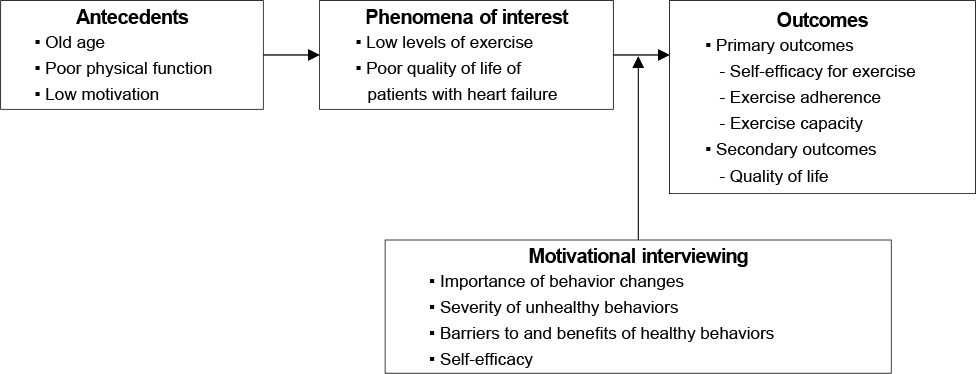
Figure 2
Conceptual framework of the study.
The research team consisted of one professor, one doctoral student, two master’s students in nursing, and two cardiologists. Three nursing graduate students had more than three years of nursing experience as registered nurses. Two graduate nurses (one doctoral student and one master’s student) provided MI as an interventionist. Interventionists studied the theoretical basis of MI in a graduate program in nursing, practiced MI through role play, and received advice from a researcher who had experience conducting and researching MI with schizophrenic patients in the United States [18]. In accordance with the principles of MI, interventionists counseled the participants and nurtured their intrinsic motivation to implement behavioral changes. Telephone-based, nurse-led MI was provided to the participants twice a week for four weeks. Each session lasted 10~20 minutes. The interviews were audio-recorded during the intervention implementation and periodically shared with the research team to ensure consistency in implementation. The research team regularly convened debriefing meetings and rated a random sample of 10.0% of the intervention recordings to ensure treatment fidelity.
In the first session, participants were provided with an introduction to the program, a schedule was established, and the behaviors that they wished to change the most to improve their health status were identified. To elicit participants’ motivation, the interventionists asked them how important the change was, as well as what would happen if participants were to make the change or if things were to continue as they were. Next, participants were provided with adequate time to identify factors that may influence their ability to implement behavioral changes and establish their goals. In the second session, participants were encouraged to analyze how they would achieve their goals, identify the barriers to and facilitators of change, and reset their goals. Subsequently, interventionists helped patients to elicit new change talk, and these practices were repeated through the seventh session. In the eighth session, interventionists encouraged participants to maintain their changed behaviors and supported participants’ goal setting efforts, after which the session was terminated.
Data were collected using a questionnaire administered between May 2012 and September 2013. The measurements of both the intervention and control groups were taken according to the same schedule (i.e., at baseline, one month, and three months after the baseline data collection). All data collectors underwent a 2-hour role-play training to familiarize themselves with the questionnaire and ensure consistency in data collection. Trained data collectors conducted a 30-minute survey when potential participants visited outpatient clinics. All eligible participants were informed about the purpose and procedures of the study and were assured about the privacy of their data. Those who were willing to participate in the study signed an informed consent form; subsequently, their data were collected. While some participants independently completed the questionnaires, others needed help and were assisted by data collectors. After baseline measurements were taken, participants were randomly assigned to either the intervention or control group based on computer-generated numbers. Telephone-based, nurse-led MI was conducted within one week after random assignment. Participants in the control group received usual care from a physician at an outpatient clinic.
Prior to data collection, ethical approval was obtained from the Institutional Review Boards (IRBs) of the three university-affiliated hospitals [20]. The IRB approval numbers were as follows: 05-2012-014 (P National University Y Hospital), D-1205003-001 (P National University Hospital), and 2013-04-018-001 (K National University Hospital). One general hospital did not have an IRB. However, the ethical approval of the IRBs in the three university-affiliated hospitals compensated for this limitation.
SPSS version 25.0 (IBM Corp., Armonk, NY) was used to conduct all statistical analyses. All assumptions were examined (e.g., normality, sphericity, and others), and remedial measures were used (e.g., use of Greenhouse-Geisser) when appropriate. Statistical significance set at p<.05 were considered statistically significant. Descriptive statistics were used to describe the baseline sociodemographic characteristics, clinical characteristics, and dependent variables of participants. The chi-squared (χ2) test, Fisher’s exact test, independent-samples t-test, and Mann-Whitney U test were used to examine group homogeneity.
The repeated measures ANOVA was used to evaluate group differences over the three time points in SEE and QOL. If there was a significant group by time interaction, a post-hoc test was performed using the independent t-test or Mann-Whitney U test. The Friedman test was conducted in exercise capacity because assumptions for repeated measures ANOVA were not met. The chi-squared (χ2) test or Fisher’s exact test and the Mann-Whitney U test were used to test group differences in the proportion of participants who exercised regularly and in the levels of regular exercise at one month and three months.
Patients who participated in at least five sessions were included in the final analysis. The baseline characteristics of participants and the results of the group homogeneity tests are presented in Table 2. The mean age of all participants was 61.79 years of age. Furthermore, 81.8% of participants were men, 18.2% were women, and 97.0% were married. With regards to education level, 34.8% of participants had graduated from high school and 24.2% had received elementary education or less. The monthly income of 45.5% of participants was less than one million won. Moreover, 24.2% were current smokers, while 43.9% consumed alcohol. The heart failure duration of most participants (63.6%) was <five years, and their mean LVEF was 34.0%. Most participants (63.6%) were classified as NYHA class I, and 1.5% were classified as NYHA class IV. Participants with comorbid conditions accounted for 77.3% of the total participants, and there were significantly higher numbers of participants with comorbid conditions in the intervention group (χ2=4.00, p=.046). Their average scores on the K-ADL and KASI were 7.06 and 46.35, respectively. The average SEE scores of participants in the control and intervention group were 33.76 and 45.82, respectively, and those of participants in the intervention group were significantly higher (Z=-1.98, p=.048). The average scores on the exercise capacity (meter) and QOL were 352.29 and 79.38, respectively. Group differences in baseline characteristics, other than the frequency of comorbid conditions and the average SEE scores, were not significant (p>.05).
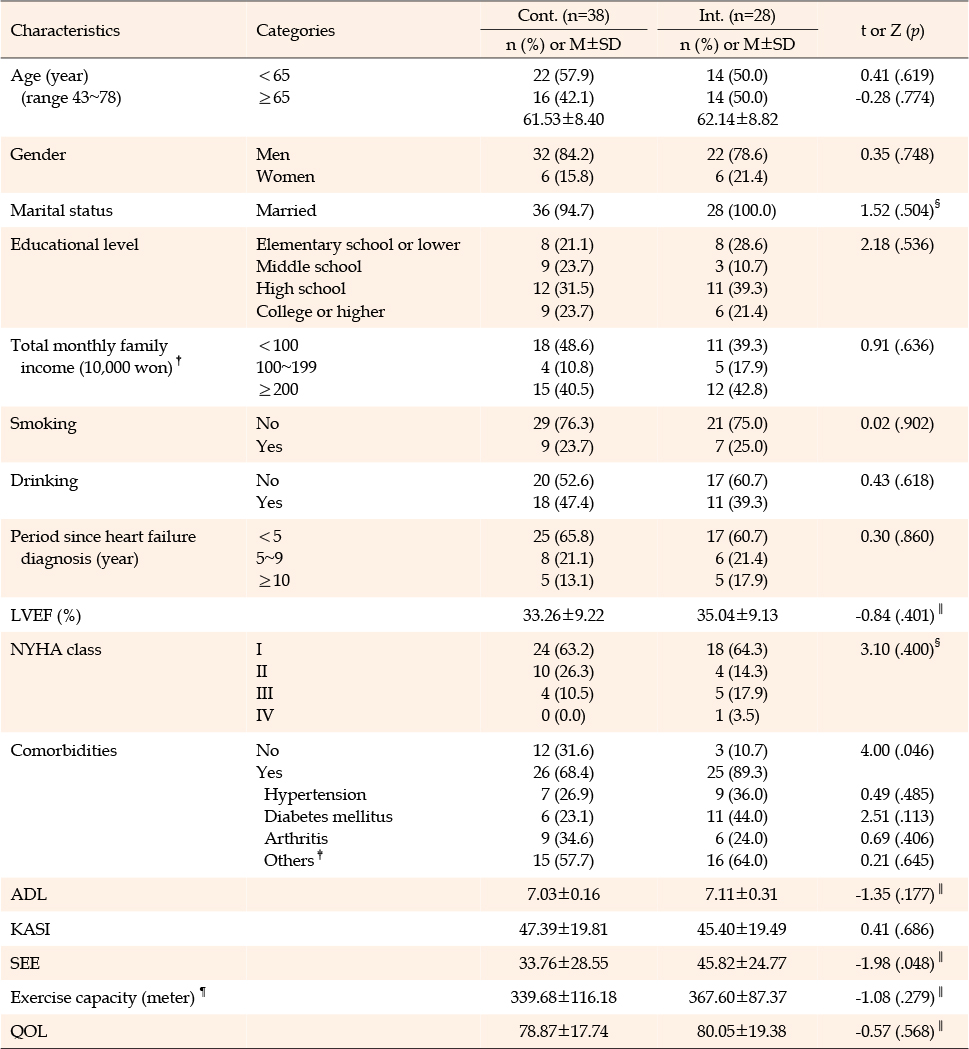
Table 2
Baseline Characteristics and Results of Tests of Group Homogeneity (N=66)
The effects of MI on SEE, exercise (i.e., levels of regular exercise and exercise regularity), exercise capacity, and QOL are shown in Table 3. Before analyzing the effects of the intervention on exercise outcomes, we explored the influence of age on exercise outcomes. There was no significant difference between the group under 65 years of age and the group over 65 years of age in levels of regular exercise (T2: Z=-1.28, p=.271, T3: Z=-1.40, p=.258), exercise regularity (T2: χ2=2.59, p=.107, T3: χ2=1.98, p=.247), and exercise capacity (T2: Z=-0.80, p=.485, T3: Z=-1.85, p=.065).

Table 3
Effects of Nurse-led Motivational Interviewing on Outcome Variables
A total of 24 participants were included in the SEE analysis. There was no significant group-by-time effect on SEE (F=0.37, p=.692). There was a significant difference in the levels of regular exercise immediately after the intervention (Z=-2.56, p=.024). The mean levels of exercise were 399.79±461.21 MET-minutes/week and 99.65±282.73 MET-minutes/week among the intervention and control group participants, respectively. At three months after baseline, no significant group difference was found (Z=-1.24, p=.318). Similarly, there were no significant group differences in the mean changes in exercise levels between the first and third months (Z=-1.13, p=.319). At baseline, participants in both groups reported that they had not engaged in regular exercise. Immediately after the one-month intervention, there was a significant group difference in exercise regularity (χ2=6.10, p=.013). More than half (58.8%) of the intervention group participants reported engaging in regular exercise more than 297 MET-minutes/week, whereas 17.6% of the control group participants reported engaging in regular exercise. At three months after baseline, no significant group difference was found (χ2=2.00, p=.252). Between the first and third months, the percentage of participants who engaged in regular exercise decreased by 15.0% in the intervention group and increased by 2.4% in the control group. There was no significant difference in exercise capacity measured by the 6 MWT over time either in the intervention group (χ2=0.29, p=.867) or control group (χ2=1.20, p=.549). A total of 24 participants were included in the QOL analysis. There was a significant group-by-time effect on QOL (F=3.76, p=.044). Post-hoc analysis showed that group differences in mean changes in QOL between the first and third months were significant (t=-3.38, p=.003).
In this study, we used MI to evoke participants’ intrinsic motivation to make positive behavioral changes [13]. Specifically, patients with heart failure were encouraged to motivate themselves to engage in health-related behaviors. The present study revealed that the intervention was effective in increasing engagement in regular exercise and QOL. This observation is consistent with previously reported effects of similar interventions that have been provided to patients with heart failure [4, 16] and other patient populations, such as those with physical disabilities [28] and older patients who underwent coronary artery bypass surgery [29].
Our study showed no significant improvements in SEE after nurse-led MI in patients with heart failure. This finding is inconsistent with the results of Vellone et al.’s study, which found a beneficial and significant effect of MI on self-care self-efficacy in patients with heart failure at six- and nine-month follow-ups [17]. Our findings may be explained by the significant group differences at baseline and the small sample size due to the high dropout rate. Baseline SEE scores were significantly higher in the intervention group, and because of the high dropout rate, only 24 of 66 patients were included in the repeated measures ANOVA for the SEE analysis. If the sample size was larger and MI techniques were further strengthened self-efficacy by emphasizing reflection, empathy, affirmation, and humor [14], the improvement in SEE would have been verified.
In the study by Audsley et al. [30], interventions delivered on a monthly or quarterly basis over six months to two years consistently showed significant effects on exercise maintenance. Intervention time periods and contact frequency appeared to influence intervention effectiveness. Therefore, it may be necessary to implement a long-term intervention or include additional contact, such as a booster session or follow-up prompts, in future research. Moreover, in this study, participants kept an exercise diary during the intervention period to increase compliance for intervention and elicit their motivation to exercise. However, they did not monitor their exercise for two months after the first month of intervention. We suggest a varying additional approach to eliciting the motivation of heart failure patients to exercise. Specifically, utilizing an activity diary for a longer time may be helpful in motivating participants to exercise [4, 31]. Alternatively, increased family engagement may play a crucial role in patients with an Asian cultural background [29].
In Arkkukangas et al.’s study, participants in the intervention group showed intervention adherence of 55.0% and adherence of an adequate amount of exercise (22.0%) among all participants [32]. Intervention adherence of older adults was influenced by weather conditions and life events such as death among close family members, in addition to behavioral and cognitive factors such as activity level, self-efficacy, and motivation [32]. Since there was no significant improvement in SEE in this study, it is thought that the increased exercise was not maintained until three months. Considering the older age of the participants in this study, recurring life events and coping strategies for these life events could have played a critical role in the compliance of healthy behaviors. Therefore, guiding participants through MI intervention across various topics can be an essential approach for older adults with chronic health problems to improve healthy behaviors.
Our study showed no significant improvement in exercise capacity. Similarly, Schertz et al. found no significant change in performance on the 6 MWT between baseline and the six-month follow-up in either intervention or control group participants [4]. Patients with heart failure in Korea should be motivated to consistently increase their level of exercise to improve their exercise to a greater extent, particularly as patients with heart failure in other countries reported a higher walking distance [4, 12] than the value that emerged in this study. There were many missing values of the 6 MWT because data collection was conducted by mail to participants who were unable to visit the hospital on the follow-up day. Moreover, some participants refused to participate in the 6 MWT after answering the questionnaire. Nevertheless, the 6 MWT is an easy-to-use, low-cost test that objectively evaluates the degree of functional limitation and prognosis of heart failure [26], and it is recommended that the 6 MWT be measured on a patient’s regular hospital visit.
A significant group-by-time effect on QOL was observed following nurse-led MI in patients with heart failure. Similarly, other published studies reported positive results regarding the impact of MI on QOL at 3~4 months among patients with heart failure [15]. The QOL of patients with heart failure may decrease over a three-month period due to the deterioration of the disease. However, the QOL of participants in the intervention group in this study remained almost the same throughout the study period, and the QOL of the control group decreased over time. This is thought to be the result of increased exercise in the intervention group at one month.
In this study, it was very difficult to induce participation in the study because many participants were elderly and in debilitating health conditions. Among the participants assigned to the intervention group, 22 participants (44.0%) declined to participate even before the intervention started, and 12 of 28 members of the intervention group (42.9%) and 23 of 38 members of the control group (60.5%) dropped out at the three-month follow-up. Among the reasons for dropout of the intervention group, "difficult to answer all the questionnaire" was the most common response for three cases, and "not interested", "questionnaire not returned by mail", and "failed to contact" were given as reasons in two cases each. Therefore, it is crucial to develop a data collection strategy to induce heart failure patients to participate in future studies.
There were many cases of not answering or refusing phone calls and feeling burdened by inducing behavioral changes during the intervention period. Participants were asked questions according to the prepared protocol, but a very limited number of participants responded adequately. When answering a call on a cellular phone, there was a tendency for people to be disturbed or to lose concentration on the content of the conversation because they answered the call wherever they were. It was thought that these participants would have had difficulty obtaining sufficient MI effects. In the case of participants who were reluctant to change, a differentiated approach and intervention with sufficient time, frequency, and interval adjustment to induce behavioral change are required according to their readiness for behavior change. In the case of the participants of this study, in order to minimize the inconvenience of additional visits to medical institutions, MI was provided by phone. Since MI depends on collaboration and elicits active thinking about health behaviors in patients, it may be delivered less effectively [16, 33] and may increase dropout rates when offered primarily over the telephone as opposed to face-to-face sessions. Methods such as face-to-face interviews or video calls are thought to further enhance the effectiveness of the interview, by eliciting an appropriate response from the participant to questions and inducing smooth communication, which should be considered in future research.
In the control group, "not interested" was the most common reason given for dropout with ten cases, and "failed to contact" followed with six cases (Figure 1). Heart failure patients in Korea had a prejudice against participation in the study, making it very difficult to invite patients with heart failure to take part in the study. Several patients who wanted to receive the intervention dropped out after being randomly assigned to the control group. High dropout rates have been observed in lifestyle modification interventions [20]. Patients with heart failure in Korea seem to rely on medication rather than lifestyle changes to manage their disease. It needs to be strongly emphasized that study participation could improve health by establishing a lifestyle that reduces symptoms of exacerbations in patients with heart failure. In addition, increasing rewards for participating in research may be a solution to reduce dropout rates. Recently, Wade et al. explored predictors of dropout within an exercise program using MI [34]. It found that people who were categorized as engaging in health-enhancing PA were less likely to drop out [34]. Therefore, special attention is needed to ensure that those engaging in low exercise do not drop out.
This study had several strengths. First, the study investigated the effects of MI on SEE, exercise, exercise capacity, and QOL in patients with heart failure and the sustainability of the effects after the intervention was terminated (i.e., at the three-month follow-up). Second, exercise capacity was measured using an objective test rather than a self-report measure. Third, to improve the quality of the study, an RCT was conducted. However, this study also had some limitations that must be considered when interpreting the results. A large percentage of participants were men (81.8%) and had NYHA class I heart failure (63.6%). This limits the generalizability of our findings to a larger population of patients with heart failure in Korea. Future studies should aim to recruit a larger and more diverse sample. Second, a high dropout rate can reduce the statistical power. Furthermore, since higher numbers of dropout patients had comorbidities than those who remained until the end of the study, this may have impacted the results favorably toward intervention groups with regard to outcomes measured. Third, data on all medications used were not investigated in this study. Medication use may be a covariate affecting outcome variables and should be thoroughly investigated in future studies. Finally, these results may differ from the current clinical environment because the data was collected between 2012 and 2013.
Despite these limitations, MI is a clinical communication skill that nurses can develop to elicit patients’ personal motivations for changing behavior to promote health that has been utilized in the past and at present [17, 18]. As nurses are health care providers who interact most closely with patients, nurse-led MI needs to be widely applied. With MI, nurses can explore patients’ understanding, motivation, confidence, and barriers to change by asking evocative questions, acknowledging patient autonomy and personal responsibility, and reserving judgment. The current study demonstrated that MI can achieve significant effects on exercise and QOL in heart failure patients with comorbid conditions. Using a repeated measures approach, we found that the positive effects of the exercise did not last for three months. This methodology highlights the value of multiple measurements of patient outcomes over time when developing strategies to promote health behaviors.
This study has shown that nurse-led MI has beneficial effects in patients with heart failure. Patients in the intervention group demonstrated greater improvements in their engagement in exercise and QOL than those in the control group. Furthermore, MI generally requires less contact time than other behavior change strategies, and is delivered effectively in this study. The results of this study provide an empirical basis for future efforts to develop effective strategies to improve exercise participation and QOL in patients with heart failure in Korea. Future studies should recruit patients with heart failure from other regions to increase the generalizability and establish the validity of the current results. In the future, we propose a study to analyze the differences in the effectiveness or compliance of interventions according to the type and number of comorbidities.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - LH and JH.
Data collection - JH, CKJ, and KJH.
Analysis and interpretation of the data - LH, PG, and JH.
Drafting of the manuscript - LH, PG and JH.
Critical revision of the manuscript - LH and PG.
Final approval - LH, PG, JH, CKJ, and KJH.
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology [NRF-2012R1A1A2041893].
 E-SUBMISSION
E-SUBMISSION