
Purpose
Contrast therapy, which includes alternately applying cold and heat therapy, is an effective intervention to increase muscle elasticity and reduce musculoskeletal edema and pain. This study aimed to confirm the effects of contrast therapy by using flexible Thermoelectric Devices (TEDs) — that not only maintain a constant temperature but can also change the temperature in a short time — on lower extremity edema, pain, muscle fatigue, and stress among nursing home workers.
Methods
This randomized controlled pre-post experimental study used a flexible thermoelectric element to administer contrast therapy in nursing home workers to compare its impact on lower extremity swelling, pain, muscle fatigue, and stress. As an intervention method, 4 minutes of heat therapy and 1 minute of cold therapy were repeated for a total of 30 minutes.
Results
The experimental group displayed a significant difference of -2.53 points, and the control group displayed a significant difference of -0.94 points (t=2.65, p<.050) as a result of an analysis comparing the two groups’ pain levels before and after the experimental treatment. The experimental group also displayed a statistically significant reduction in the degree of lower extremity edema (t=3.91, p=.001). Furthermore, the experimental group’s lower extremity stress index decreased significantly (t=2.87, p=.049).
Conclusion
The findings of this study indicated that contrast therapy by using flexible TEDs alleviated stress, leg pain, and swelling in nursing home workers and could be used as an intervention to alleviate musculoskeletal problems in healthcare workers.
Contrast therapy, which includes alternately applying cold and heat therapy, is an effective intervention to increase muscle elasticity and reduce musculoskeletal edema and pain. This study aimed to confirm the effects of contrast therapy by using flexible Thermoelectric Devices (TEDs)—that not only maintain a constant temperature but can also change the temperature in a short time—on lower extremity edema, pain, muscle fatigue, and stress among nursing home workers.
This randomized controlled pre-post experimental study used a flexible thermoelectric element to administer contrast therapy in nursing home workers to compare its impact on lower extremity swelling, pain, muscle fatigue, and stress. As an intervention method, 4 minutes of heat therapy and 1 minute of cold therapy were repeated for a total of 30 minutes.
The experimental group displayed a significant difference of -2.53 points, and the control group displayed a significant difference of -0.94 points (t=2.65, p<.050) as a result of an analysis comparing the two groups’ pain levels before and after the experimental treatment. The experimental group also displayed a statistically significant reduction in the degree of lower extremity edema (t=3.91, p=.001). Furthermore, the experimental group’s lower extremity stress index decreased significantly (t=2.87, p=.049).
The findings of this study indicated that contrast therapy by using flexible TEDs alleviated stress, leg pain, and swelling in nursing home workers and could be used as an intervention to alleviate musculoskeletal problems in healthcare workers.
According to the age-specific demographic data released by the National Statistical Office in South Korea, the proportion of older adults aged 65 or older accounted for 14.3% of the total population by 2018; this proportion is projected to increase every year, with an estimate of reaching 15.7% in 2020, 25.0% by 2030, and 34.4% by 2040 [1]. Additionally, it was reported that most older adults have chronic diseases, 43.3% of them have limitations in activities of daily living, and at least 8% of older adults are currently in need of nursing care owing to dementia [2]. In modern society, there is an increasing demand for facilities and nursing care services to support older adults with chronic diseases and their families, because family functions for supporting older adults are weakened owing to a decrease in the number of family members and women’s active entry into society [3]. As compared to before the implementation of the long-term care insurance system, the number of long-term care service institutions and care workers has increased two to three times recently, and is expected to continue to increase [4]. Nursing homes are emerging as increasingly important palliative care providers and employers in modern society.
Nursing home workers usually consume a significant amount of energy because of repetitive and fast tasks, such as taking care of patients’ eating, dressing, bathing and toilet and moving them from bed to chair [5]. In particular, since patients in nursing homes rely heavily on nursing care for almost all their activities of daily living, workers caring for nursing home patients may particularly be at risk of developing musculoskeletal disorders owing to the nature of their job [6, 7]. As a result, workers in nursing homes complain of musculoskeletal symptoms and fatigue, which negatively affect job stress [8]. Some studies have reported that home care and nursing home workers had more work-related injuries due to tasks than other occupations, and higher levels of care dependency in patients were associated with a higher incidence of musculoskeletal disorders in caregiving workers [9, 10]. A study involving hospital workers reported that the prevalence of musculoskeletal symptoms, back pain, neck and shoulder pain, and knee pain among nurses and patient care assistants in the last three months was 74%, 53%, 42%, and 37%, respectively [11]. In a previous study on musculoskeletal symptoms of caregivers, 31.8% of caregivers showed musculoskeletal symptoms, of which 45.2% reported lower extremity pain [8]. Physical exposure causing musculoskeletal pain includes patient transport work requiring patient handling out of bed and tasks using strong physical force [11, 12].
Interventions such as stretching, exercise, cold and heat therapy, and massage for muscle atrophy and weakness are effective in relieving pain and increasing flexibility [13, 14, 15]. Among them, contrast therapy, which includes alternating heat and cold therapy, is effective in reducing musculoskeletal edema and pain and is an effective intervention to increase muscle elasticity [16]. In general, local cold therapy (or cryotherapy) is used as an intervention to reduce skin and tissue temperature to induce vasoconstriction, reduce blood flow, and prevent tissue fluid movement, thereby reducing edema and slowing nerve transmission speed, and finally controlling pain [17]. Heat therapy is used as an effective intervention to relieve joint stiffness by increasing connective tissue elasticity and promoting inflammatory processes and wound healing [18]. Previous studies reported that pain and related symptoms were significantly reduced by the contrast applications of cold and warm therapy as compared to the single application of cold or warm therapy in osteoarthritis patients [19]; additionally, muscle soreness and fatigue significantly reduced as compared to the control group when athletes were subjected to contrast therapy using water after training [20]. However, contrast bath therapy, which is often used as a contrast therapy, has limitations in its application because it requires a large amount of water, mobility and usable locations, and maintenance of a constant temperature.
Therefore, this study aimed to investigate the effects of contrast therapy using a flexible Thermoelectric Device (TED)—that can maintain a constant temperature and change the temperature within a short period of time—on lower extremity edema, pain, muscle fatigue, and stress in nursing home workers.
This randomized controlled pretest-posttest experimental study aimed to investigate the effects of contrast therapy using flexible TED on lower-extremity edema, pain, muscle fatigue, and stress in nursing home workers (Figure 1).
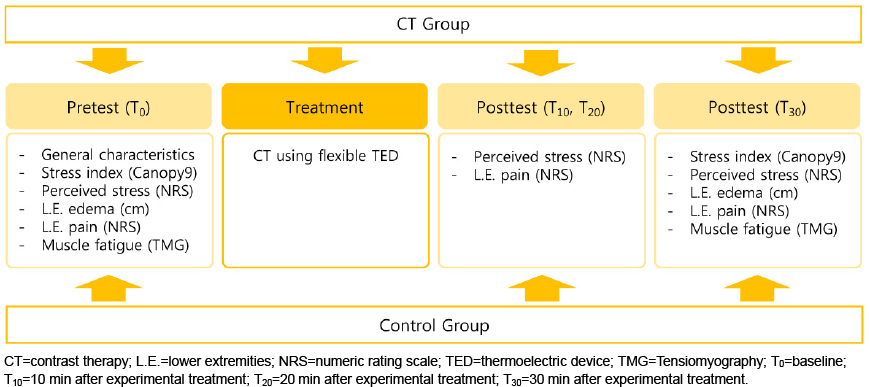
Figure 1
Study design.
The participants were nursing home workers at S nursing home located in D City, South Korea, who agreed to participate in this study. The selection and exclusion criteria for this study were as follows: 1) those who understood the purpose of this study and voluntarily agreed to participate in this study; 2) were able to communicate; and 3) currently did not have fractures, disabilities, or diseases in the lower extremities. The exclusion criteria were as follows: 1) those who were currently being treated for a mental illness, 2) had open wounds or inflammation in the lower extremities, 3) had skin diseases or allergies, 4) had a cardiovascular disease, and 5) currently were musculoskeletal medication users (e.g., pain control, NSAIDs).
To determine the number of participants required for this study, we used an effect size (Cohen's d) of 0.29 as calculated based on a previous study [20] in which contrast therapy was provided to healthy adults. When the required number of participants was calculated based on an effect size (f) of 0.29, significance level (α) of .05, power (1-β) of .80, number of groups of two, and number of repeated measurements of three using the F-test, the appropriate sample size obtained was 34. Considering a dropout rate of 20%, 40 participants were included in the study. Of them, 7 dropped out, indicating a dropout rate of 17.5%. For one participant, data collection was not possible owing to personal reasons at the time of data collection; two participants refused to participate in this study. Four participants with insufficient pre- and post-test data (general characteristics, perceived stress, lower extremities pain) were excluded from the Contrast Therapy Group (CTG) and the Controlled Group (CG) two participants from each group. Therefore, 33 participants, consisting of 15 in the CTG and 18 in the CG, were included in the analysis (Figure 2).
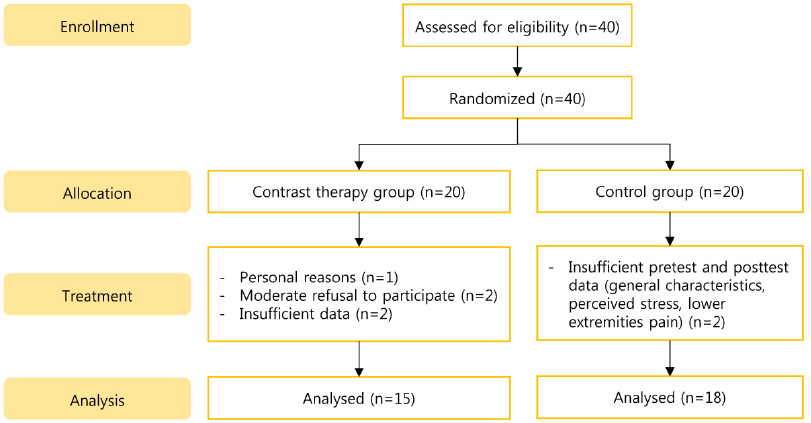
Figure 2
Flow diagram of the study.
To comply with research ethics and protect participants, this study was conducted after receiving approval from the institutional review board of K University (KYU-2021-021-01). For data collection, the researcher explained the purpose and method of the study to each subject to seek consent and cooperation in data collection and explained that consent could be withdrawn at any time during the study. The experimental treatment was conducted in compliance with safety management regulations, and data collected for personal protection were coded and anonymized.
This was a randomized controlled pretest-posttest experimental study. The researchers divided the participants into experimental and control groups using the random number generation feature on Microsoft Excel program Version 2016 for each group task. Twenty participants in the CTG received contrast therapy using a flexible TED and 20 participants in the CG did not receive any therapy.
The intervention for the participants was conducted by the researcher. The data were collected by three research assistants who received eight hours of training from the principal researcher, through which they became familiar with the contents of the training, including a practical course in which they learned about explanation and simulation. And the researcher did not share information about randomization with the research assistants and did not provide participants with information about their own group after randomization. To prevent the spread risk of experimental results, data collection from CTG was conducted after data collection from CG. After all interventions were completed, contrast therapy was administered to the participants in the control group who wanted to do so.
The laboratory temperature was set at 25℃, which was optimal for measuring muscle fatigue and stress in the participants, and the laboratory was well ventilated. In addition, tables, chairs, and beds for measurement were installed in the laboratory to provide a comfortable environment for the participants, and a monitoring device was installed to measure muscle fatigue and stress.
In this study, contrast therapy using a wearable intervention device with four temperature conduction plates was performed and flexible thermoelectric devices were used as the experimental treatment. Flexible TED is a new material developed by TEG way that can maintain a constant temperature continuously using electricity, and can change the temperature between low and high temperatures within 3 seconds, and is thus appropriate for contrast therapy [21]. A study by Kim et al., [16] revealed that when an intervention using heat therapy for 4 minutes and cold therapy for 1 minute was repeated, it was effective in reducing muscle stiffness and relieving muscle pain. Based on these results, one treatment session involving 40℃ heat therapy for 4 minutes and 12℃ cold therapy for 1 minute was repeated six times for a total of 30 minutes on the right lower extremity.
To measure lower extremity edema, each participant’s calf circumference (cm) was measured using a surface measurement method with tape measurement (PIE, BagelLabs Co., Ltd., Korea). Calf circumference was measured to one decimal place from the thickest part of the calf to the front part of the tibia, while each participant sat with the knees up. For an accurate measurement, two measurements were made, and the average value was used.
Lower extremity pain was measured using the Numeric Rating Scale (NRS). The participants were asked to indicate their pain level in the lower extremities on a 10 cm horizontal line marked with 0 (no pain at all) on the left end of the tool and 10 points (very painful) on the right end. A higher score indicated higher perceived lower extremity pain.
Muscle fatigue was measured using Tensiomygoraphy (TMG), a muscle function evaluation tool manufactured by the TMG-BMC Ltd. TMG is a non-invasive neuromuscular evaluation method that can selectively examine specific muscles and is relatively easy and simple to measure muscle function, and it is thus widely used in sports. As for its measurement method, it was reported that the degree of muscle stiffness, muscle tone, and muscle fatigue can be determined by evaluating the contractile properties of the concerned muscle when a single electrical stimulation is applied to muscle to be measured [22]. A variable that has a high correlation with muscle tone and fatigue in the TMG is the displacement maximum (Dm), which refers to the maximum displacement distance traveled by muscle contraction caused by electrical stimulation [22]. A shorter Dm indicates greater muscle fatigue.
The stress index was used to objectively measure the stress. It refers to the autonomic nervous system index values measured using Canopy 9 RSA (respiratory sinus arrhythmia)( IEMBIO, USA) with a finger sensor, an autonomic nervous system measuring device. With this tool, the finger sensor is supposed to be placed on the index finger of the left hand, and to continuously measure for 2 minutes and 30 seconds, and then quantify the ratio of sympathetic nerve and parasympathetic nerve activity values based on Heart Rate Variability (HRV) through the standard induction method to yield autonomic nervous system index values. The stress index ranges from 1 to 10, with higher values indicating exposure to stressful situations.
Subjective stress is measured using a NRS. Each participant was asked to indicate the degree of lower extremity pain felt on a 10 cm long horizontal line marked with 0 (do not feel stressed at all) on its left end and 10 (feel very stressed) on its right end. A higher score indicates a higher level of perceived stress.
The data were collected from July 15, 2021, to August 3, 2021, in a laboratory at S nursing home located in D City, South Korea. Data collection and intervention of study participants were conducted during breaks at work. A questionnaire was distributed to the participants after entering the laboratory, and they were asked to fill out their general characteristics, current lower extremity pain and discomfort, and subjective stress. Lower extremity edema, muscle fatigue, and stress index were measured. The participants in the experimental group were provided with contrast therapy using flexible TED while lying in bed for 30 minutes, and the participants in the control group rested for 30 minutes. To determine the subjective stress reduction time of the experimental group, while the intervention for 30 minutes was provided to the experimental group, perceived stress and lower extremity pain levels were measured three times at 10-minute intervals. To minimize extraneous variables, the stress index, lower extremity edema, and muscle fatigue were measured after 30 minutes of intervention. After data collection, a token of appreciation was given to the participants, and all collected data were recorded anonymously and input to an Microsoft Excel program Version 2016 for analysis.
The collected data were analyzed using IBM SPSS Statistics 24.0. The skewness and kurtosis values were tested to determine the normality of the data, and the results indicate skewness values of -0.10~0.39, and kurtosis values of -1.28~0.08. They were normally distributed in the range of skewness absolute value 2 and kurtosis absolute value 4 [23]. The general characteristics of the participants were analyzed using frequency, real number, and percentage. The pre-homogeneity test for the dependent variables in the experimental and control groups was performed using the χ2 test and t-test. The effects of the intervention on stress, lower extremity pain, edema, and muscle fatigue were analyzed using independent t-tests and repeated-measures Analysis of Variance (ANOVA), and the mean difference test was analyzed as an independent t-test.
The results of analyzing the general characteristics and dependent variables of the participants in the experimental and control groups are presented in Table 1. The results of the homogeneity test of the general characteristics between the two groups showed no significant differences in age, height, weight, drinking status, smoking status, and exercise between the two groups. The initial stress index scores of the participants were 7.13±2.30 points and 6.83±2.15 points in the experimental group and the control group respectively. The perceived stress scores were 4.60±1.81 points, and 5.06±2.10 points, in the experimental group and the control group respectively. This indicates that there was no significant difference between the two groups, thus confirming the homogeneity between the two groups. The lower extremity pain scores in the experimental and the control groups were 4.87±2.56 points, and 4.28±2.32 points, respectively; the degrees of edema in the experimental and the control groups was 35.42±2.92 cm, and 34.92±2.67 cm, respectively; the muscle fatigue scores in the experimental and the control groups were 3.01±0.80 points, and 2.90±1.39 points, respectively, indicating that there was no significant difference between the two groups.
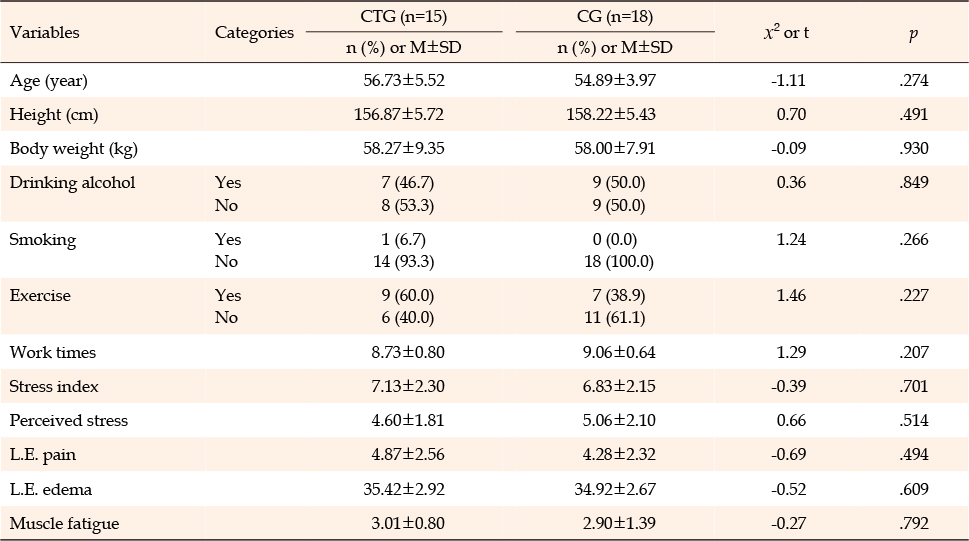
Table 1
Characteristics of the Experimental and Control Groups (N=33)
After the experimental treatment, the degree of lower extremity edema was 34.41±3.19 cm in the experimental group, and 34.89±2.60 cm in the control group, indicating no significant difference. However, the results of analyzing the difference in lower extremity edema between the two groups before and after the experimental treatment found that the degree of lower extremity edema was -1.01±0.96 cm in the experimental group, and -0.03±0.20 cm in the control group, indicating a significant difference (t=3.91, p=.001)(Table 2).
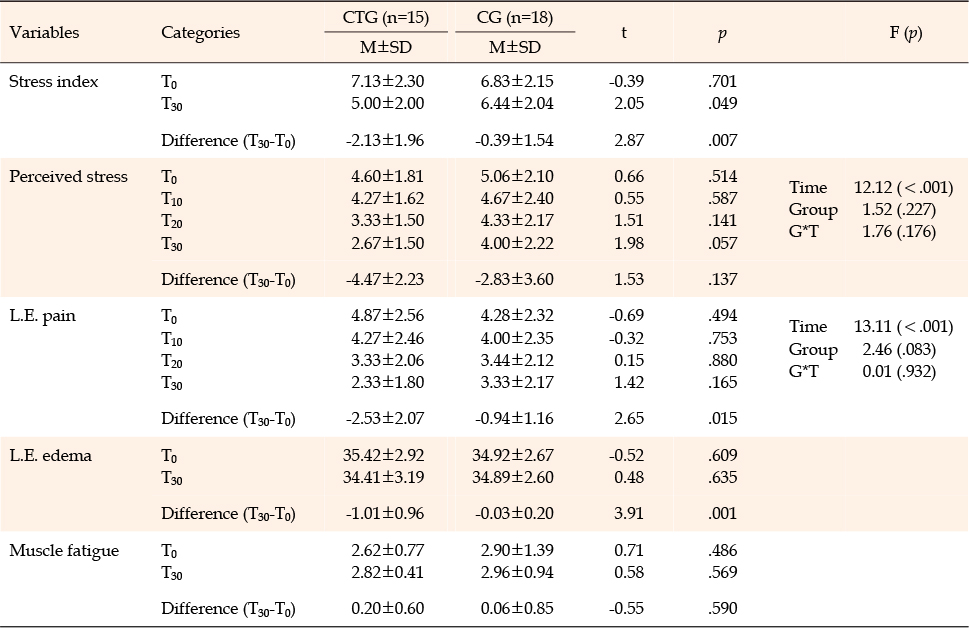
Table 2
Comparison of Stress Index, Perceived Stress, L.E. Pain, L.E. Edema, Muscle Fatigue between the Experimental and Control Groups (N=33)
Lower extremity pain scores were measured four times in total: before experimental treatment, at 10 minutes (T10), 20 minutes (T20), and 30 minutes (T30) after the experimental treatment. The results revealed that there was a significant difference over time (F=13.11, p<.001), but there was no significant difference in group-by-time interaction, and there was also no significant difference in repeatedly measured stress score results between the groups. The results of analyzing the difference between the two groups before and after the experimental treatment using difference verification revealed that the difference before and after the experimental treatment was -2.53±2.07 points in the experimental group, and -0.94±1.16 points in the control group, indicating a significant difference between the groups (t=2.65, p<.050) (Table 2).
The difference in muscle fatigue before and after the experimental treatment was 0.20±0.60 points in the experimental group, and 0.06±0.85 points in the control group, showing no significant difference (Table 2).
The objective stress score measured after the experimental treatment using the stress index was 5.00±2.00 points in the experimental group, and 6.44±2.04 points in the control group, indicating that there was a statistically significant difference (t=2.05, p=.049). The difference in the stress index before and after the experimental treatment was -2.13±1.96 points in the experimental group, and -0.39±1.54 points in the control group, indicating that the stress index score in the experimental group had significantly decreased (t=2.87, p=.007) (Table 2).
The subjective stress scores perceived by the participants were measured four times in total: before the experimental treatment, at 10 minutes (T10), 20 minutes (T20), and 30 minutes (T30) after the experimental treatment. The results revealed that there was a significant difference over time (F=12.12, p<.001), but there was no significant difference in group-by-time interaction, and there was also no significant difference in stress scores measured repeatedly between the groups. The results of analyzing the difference before and after the experimental treatment between the two groups by using difference verification revealed that the difference in perceived stress was –4.47±2.23 points in the experimental group, and -2.83±3.60 points in the control group, indicating that there was no significant difference (Table 2).
This study aimed to investigate the effects of contrast therapy using flexible TED, which is capable of heat/cold temperature control, on lower extremity pain, edema, muscle fatigue, and stress in care workers who belong to an occupational group with a high musculoskeletal burden. The results showed that contrast therapy using flexible TED had positive effects on care workers and that there was a statistically significant difference in lower extremity pain, edema, and stress index between the groups. The results of this study are as follows:
Although the mechanism by which alternating the use of heat and cold treatments affects the recovery of damaged muscle has not yet been clearly identified, the following three points can be considered. First, heat therapy, which forms an important part of contrast therapy, might enhance vasodilation to increase oxygenation and metabolite excretion [24]. This study indicated that such a phenomenon occurred to some extent because the contrast therapy using a 40℃ TED was applied six times for 4 minutes per treatment session for a total of 24 minutes. In addition, heat therapy might increase the immune response to muscle damage, similar to symptoms occurring during fever, and this response might accelerate muscle recovery [25]. In fact, Viitasalo et al. reported that when applying 37℃ underwater water jet massage to athletes after training, muscle function maintenance was improved, and Creatine Kinase (CK) and myoglobin levels were increased in those receiving warm water therapy compared to the control group [26]. The authors suggested that warm water therapy might increase the release of proteins from the muscle into the blood, and that the increased protein release might reduce the percentage of muscle components degraded in the extracellular matrix [27]. Second, cold therapy with contrast may reduce nerve conduction velocity and decrease nerve transmission [28]. In addition, Gregson suggested that blood flow to muscles may be lowered after 8~20℃ cold pack application, and stated that this may be because the activation of heat receptors may result in changes in sympathetic activity, thereby decreasing arterial flow [29]. Therefore, the physiological effects of cold therapy may be partially mediated through a decrease in microvascular blood flow around the injured site, which in turn can reduce edema and inflammation induction. Finally, the alternating use of cold and heat therapy can result in drastic changes in muscle perfusion owing to a combination of cold / heat effects, which is called the pumping effect [30]. It has been reported that the pumping effect might cause changes in muscle perfusion through vasodilation and vasoconstriction, thereby weakening the immune response and reducing muscle cell damage. In this study, no vasodilation or constriction was observed; however, muscle pain and edema were significantly reduced after contrast therapy. Vaile et al. reported in a study examining 15℃ / 38℃ contrast bath therapy (15℃ cold water therapy, and 38℃ warm water therapy) that the 15℃ cold water therapy was effective in reducing physiological and functional deficits related to muscle pain, including muscle recovery and edema reduction, and 38℃ warm water therapy was effective for muscle recovery, but had no effect on other recovery as compared to the control group [31]. It can be concluded that contrast therapy is effective in helping muscle recovery and reducing pain, and edema. Comparative studies with cold therapy that show similar results are needed to further clarify the effects of contrast therapy.
Stress refers to a state of physical, physiological, and psychological tension that an individual experiences in difficult situations [32]. Excessive stress can have negative effects on mental and physical health, cause deterioration of work quality, and should be properly relieved [32]. This study found a significant difference in the stress index, which measured the autonomic nervous system index based on heart rate variability, before and after the experiment, between the two groups. In addition, perceived stress showed no statistically significant difference but decreased by 4.47 points in the experimental group and 2.83 points in the control group, showing more reduction effects in the experimental group. As studies regarding the effects of contrast therapy on stress could not be identified, a direct comparison between this study and other studies was not feasible. However, it was reported that the use of 40℃ foot bath therapy 4 days per week for 3 weeks in operating room nurses was helpful in relieving stress [33], and stress has been reported to have a significantly positive correlation with musculoskeletal disorders such as back pain [34]. Hence, it is thought that the contrast therapy used in this study might alleviate lower extremity discomfort and thus reducing stress.
Taken together, the results of this study are significant in confirming that contrast therapy using a flexible TED has similar effects to contrast bath therapy using water temperature. In addition, a study by Kim reported that both contrast bath therapy using 38~40℃ hot water and 12~14℃ cold water, and contrast therapy using a 38~40℃ infrared heating device and a 12~14℃ refrigeration device was effective in enhancing muscle recovery, confirming that both wet heat therapy using immersion bath and dry heat therapy using infrared rays and a refrigeration device can help muscle recovery [16]. Therefore, since contrast therapy using flexible TED can minimize individuals’ movement without moving themselves while alternating cold/heat therapy and maintain a constant temperature, it is considered an effective intervention method.
This study was conducted using a randomized controlled pretest-posttest experimental design to understand the effect of contrast therapy using flexible TED on the musculoskeletal system and stress of workers in nursing institutions. In order to confirm the effectiveness of contrast therapy using flexible TED, 40℃ heat therapy and 12℃ cold therapy were applied to the study participants six times for 4 minutes and 1 minute, respectively. The results showed that contrast therapy using flexible TED had a positive effect on leg edema, pain, muscle fatigue, and stress. Therefore, we believe that the results of this study provide positive scientific evidence for the application of contrast therapy using flexible TED and that contrast therapy using flexible TED can be used as an intervention to alleviate musculoskeletal problems in healthcare workers. However, this study has a risk of performance bias because the researcher was not blinded by random sequence generation and intervention, and there is a limit to generalization as a study was conducted at a single nursing institution.
Based on the results of this study, I suggest the following. First, this study was conducted at a nursing institution in one location, and there are limitations in generalization; therefore, further studies are needed. Second, in this study, the effect before and after therapy was verified by applying six on-therapy sessions for 4 minutes and cold therapy for 1 minute; however, for future studies, I recommend comparing and verifying the effect on time flow. Third, because the effects of contrast therapy, heat therapy, and cold therapy may vary depending on the use of flexible TED, a comparative study of these effects is suggested.
CONFLICTS OF INTEREST:The author declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition-SJ-A.
Analysis and interpretation of the data-SJ-A.
Drafting and critical revision of the manuscript-SJ-A.
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean Government (No. 2019R1G1A1002538).
 E-SUBMISSION
E-SUBMISSION