
Purpose
This study aimed to evaluate the validity and reliability of the revised Korean version of the Nurses' Ethical Behaviors for Protecting Patient's Rights Scale (NEBPPRS-K25).
Methods
The participants in this study consisted of 311 nurses employed at university hospitals located in D, S, or U cities. Data were collected from July 1 to August 31, 2022. The collected data were analyzed utilizing SPSS and AMOS version 28.0.
Results
The statistical analysis led to the exclusion of three items from the original version, resulting in five subscales encompassing a total of 25 items. Confirmatory factor analysis demonstrated satisfactory model fit indices (normed χ2 =2.56, p<.001, RMR=.05, RMSEA=.07, GFI=.84, CFI=.86, TLI=.85, IFI=.87). The items' convergent and discriminant validity were verified using confirmed through the extracted mean variance (.54~.65) and composite reliability (.78~.90). The Cronbach's ⍺ value for the overall NEBPPRS-K instrument was .89, while the Cronbach's ⍺ value for each individual subscale ranged from .66 to .85.
Conclusion
The NEBPPRS-K25 is a valid and reliable scale, making it suitable for widespread use in measuring nurses' ethical behaviors to safeguard patient rights.
This study aimed to evaluate the validity and reliability of the revised Korean version of the Nurses' Ethical Behaviors for Protecting Patient's Rights Scale (NEBPPRS-K25).
The participants in this study consisted of 311 nurses employed at university hospitals located in D, S, or U cities. Data were collected from July 1 to August 31, 2022. The collected data were analyzed utilizing SPSS and AMOS version 28.0.
The statistical analysis led to the exclusion of three items from the original version, resulting in five subscales encompassing a total of 25 items. Confirmatory factor analysis demonstrated satisfactory model fit indices (normed χ2=2.56, p<.001, RMR=.05, RMSEA=.07, GFI=.84, CFI=.86, TLI=.85, IFI=.87). The items' convergent and discriminant validity were verified using confirmed through the extracted mean variance (.54~.65) and composite reliability (.78~.90). The Cronbach's α value for the overall NEBPPRS-K instrument was .89, while the Cronbach's α value for each individual subscale ranged from .66 to .85.
The NEBPPRS-K25 is a valid and reliable scale, making it suitable for widespread use in measuring nurses' ethical behaviors to safeguard patient rights.
Protecting patient rights is one of the paramount duties of medical professionals and other healthcare personnel. A particular emphasis is given to the protection of patient rights in nursing roles, and the majority of hospitals overtly present a Patient's Bill of Rights as a means of promoting patient rights and delivering optimal medical care [1]. Recognizing the vulnerability of patients, they must be shielded from potential ethical violations that could infringe upon their rights [2]. Consequently, nurses and other medical team members must strive diligently establish to cultivate their ethical values, which underpin ethical decision-making and conduct behavior [3]. Ethical behavior is defined as adherence to societal or cultural norms of right and wrong [4], and ethical practice is an essential attribute for nurses dealing with ethical dilemmas [5].
The conceptual foundation of a nurse's ethical behavior can be traced to the four bioethical principles laid out by Beauchamp and Childress [6]. These principles-namely, respect for autonomy, nonmaleficence, beneficence, and justice-must be adhered to in nursing practice. However, individuals often face situations where medical services are distributed unevenly based on not just race, gender, and age, but also factors such as sexual orientation, socioeconomic status, political affiliations, and personal relationships [7]. There are instances where patients' rights to protection from harm are violated, such as in the case of medication errors [8]. Moreover, patients can be susceptible to infringements on their autonomy due to their trust and reliance on nurses as professionals who make decisions during the caregiving process, underscoring the need for protection of patients' rights [9].
Patients' rights to their values and preferences must be respected. For instance, religious or cultural values, such as seeking alternatives to blood transfusions [10] or setting aside time for prayer, should be honored. However, these rights are not always guaranteed. Patients also possess a right to privacy [11]; hence, nurses are obligated to maintain the confidentiality of all patient information, including medical records and any personal information obtained in their professional role [12, 13]. However, this obligation is not always upheld.
Nurses frequently confront ethical dilemmas and may find it challenging to uphold ethical nursing practices for the protection of patient rights due to the lack of supportive resources within hospitals, such as ethical consultations, education, and problem-solving systems [14]. In this context, forming a clear definition and content for patient rights can lead to standardized treatment across the medical field, offering patients consistent expectations during their care [15]. Hence, nurses need to enhance their ethical nursing competencies to safeguard patient rights. A vital step towards this improvement involves evaluating their current ethical nursing performance and developing a valid and reliable tool for measurement.
Several tools exist for measuring nurses' ethical behavior, such as the Nurses' Wrongdoing Scale [16], Nurses' Ethical Behaviors Scale [17], and the Ethical Nursing Competence Self-Rating Scale [18]. However, these tools either fail to focus on measuring patient rights or fail to provide a comprehensive conceptual framework for the "ethical behavior" expected of nurses. For instance, the Wrongdoing Scale item "drug abuse by nurses" appears somewhat distant from Korean culture. Furthermore, it was only employed as a questionnaire in a single study without systematic tool development or validation, leaving its validity and reliability unconfirmed. The Ethical Behavior Scale only evaluates three dimensions: autonomy, justice, and non-maleficence/beneficence. In contrast, the Ethical Nursing Competence Self-Rating Scale assesses five dimensions: ethical sensitivity, ethical knowledge, ethical reflection, ethical decision-making and action, and ethical behavior. Despite its comprehensiveness, the inclusion of personal reflection and attitude makes it less focused on protecting patient rights.
Alternatively, Gulcan developed the Nurses' Ethical Behaviors for Protecting Patient's Rights Scale (NEBPPRS) [19], an ethical behavior measurement tool for nurses. This tool, based on the ICN Code of Ethics for Nurses, patient rights protection, and the biomedical ethics principles of Beauchamp and Childress [6], focuses on the protection of nurses' patient rights. It measures "respect for right to information and decision making", "providing fair care", "providing benefit-not harming", "respect for patient values and choices", and "attention to privacy", setting it apart from other tools. The advantages of this tool are its proven reliability and validity, achieved through proper procedures, a manageable number of items for ease of use, and its utility in protecting patient rights in clinical settings that require patient-centered nursing. Furthermore, each item evaluates various aspects of patient rights from an ethical perspective, allowing for a comprehensive assessment. This study aimed to establish the cultural validity and reliability of the Korean version of the NEBPPRS for measuring the ethical behavior of Korean nurses in protecting patient rights.
The purpose of this study was to assess the validity and reliability of the Korean translated version of the NEBPPRS among Korean nurses.
This methodological study aimed to assess the validity and reliability of the Korean translated version of the NEBPPRS among Korean nurses.
The participants consisted of nurses employed at university hospitals in D, S, or U cities. Over 300 samples are considered excellent for Confirmatory Factor Analysis (CFA) for validity verification [20]. Accounting for a potential 10% dropout rate, a sample size of 330 was initially recruited. After excluding 18 questionnaires with incomplete or missing responses, a total of 311 questionnaires were analyzed.
The NEBPPRS [19] was originally developed and validated in Turkey with 450 university hospital nurses. This tool comprises 28 items categorized into five sections: 9 items for "respect for right to information and decision making", 6 items for "providing fair care", 5 items for "providing benefit-not harming", 4 items for "respect for patient values and choices", and 4 items for "attention to privacy". It utilizes a Likert scale, with 1 point for "never" and 5 points for "always". Higher total scores suggest higher levels of ethical behavior. The Cronbach's α coefficient for the NEBPPRS was .84, and it ranged from .59 to .81 for each of the factors.
The NEBPPRS questionnaires were translated into Korean, following the procedures and methods recommended by the World Health Organization [21]. The translation was carried out by a bilingual nursing professor fluent in both Korean and English, who holds a doctorate from an English-speaking country. The researcher and translator ensured that the sentiment, flow of context, and grammar of the Korean language were appropriate, while comparing and reviewing the Korean translated version with the original version. An English linguistics professor, who had not seen the original version, back-translated the Korean translation to confirm there were no discrepancies in phrasing and content. The back-translated English version was then sent to the original author for approval, and any detected errors were retranslated and corrected.
An expert panel was assembled to determine content validity, adhering to Lynn's [22] recommendation that such a panel should consist of between three and 10 experts. This panel included a nursing professor, a nursing Ph.D. with tool development experience, and four nurses with more than a decade of clinical experience. The panel of six experts was briefed on the study's purpose and the development of the NEBPPRS. They were asked to help validate the content, and the Korean translation was either handed directly to the experts or sent via email. Preliminary surveys were conducted to assess the clarity of items, the ease of understanding words and phrases, and the appropriateness of item length. Feedback was collected in person or via email for items that needed revision. After evaluating the validity of each item using a 4-point Likert scale ranging from "very appropriate" (4 points) to "not appropriate at all" (1 point), the Content Validity Index (CVI) was calculated.
Known-group validity assesses whether a measurement tool accurately predicts differences in concept attributes between groups that are expected to differ due to known characteristics. Based on the hypothesis that nursing ethics education fosters ethical behavior [18], this study assessed known-group validity by using the t-test to determine if there was a significant difference in nurses' ethical behavior based on their exposure to nursing ethics education.
Before initiating this research, the investigators secured permission to use the original NEBPPRS from the developer, and approval (IRB No. EU22-23) for this research was obtained from the institutional review board of Eulji University in D city. Subsequently, the researchers reached out to and visited the target hospitals to explain the research's purpose to the head of the nursing department and secure permission. Participants were informed about the research purpose, data collection procedures, and methods, and written consent was obtained from those who voluntarily agreed to participate. All participants were given a small gift as a token of appreciation. Participants were also notified that their data would be securely stored in a locked cabinet for three years before being discarded.
The collected data were analyzed using SPSS 28.0 and AMOS 28.0 software, and the general characteristics of the participants were evaluated. Content validity was assessed using the CVI. Item analysis was conducted to check the normality and homogeneity of the items, and it included the mean, standard deviation, skewness, kurtosis, ceiling effect, floor effect, and corrected item-total correlation.
In order to verify the construct validity of the translated tool, CFA was used to confirm whether the factor fit indices met the criteria of normed x2 (CMIN/DF) less than 3.00, Root Mean Residual (RMR) equal to or less than .05, Root Mean Square Error of Approximation (RMSEA) within the range of .05 to .08 [23], Goodness of Fit Index (GFI) greater than or equal to .80, Comparative Fit Index (CFI) greater than or equal to .80, Tucker-Lewis index (TLI) greater than or equal to .80, and Incremental Fit Index (IFI) greater than or equal to .80 [24]. The convergent and discriminant validity of the items were evaluated using standardized coefficients (λ), Average Variance Extracted (AVE), Construct Reliability (CR), correlation coefficient, and standard errors. Known-group validity was assessed using the independent t-test, and the internal consistency reliability was evaluated using Cronbach's α.
Among the 311 participants, the average age was 29.37±6.37 years. Women comprised a substantial majority (87.1%), and 81.4% were single. The sample was predominantly non-religious (66.9%). A significant portion, 81%, held bachelor's degrees. The largest group, 27.3%, reported 2~4 years of Clinical experience, and 48.2% were employed in general wards. Notably, 74.6% had previously undergone ethics education (Table 1).
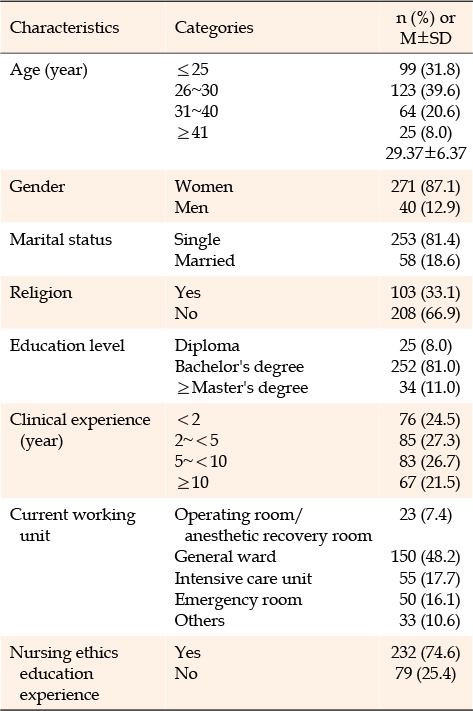
Table 1
General Characteristics of Participants (N=311)
Content validity was confirmed, with a Scale-level Content Validity Index (S-CVI) of .98 and an Item-level Content Validity Index (I-CVI) ranging from .83 to 1.00, thereby satisfying the criteria of S-CVI ≥.90 and I-CVI ≥.80 [25].
Skewness ranged from -1.21 to -0.09, while kurtosis ranged from -0.82 to 4.34 (Table 2).
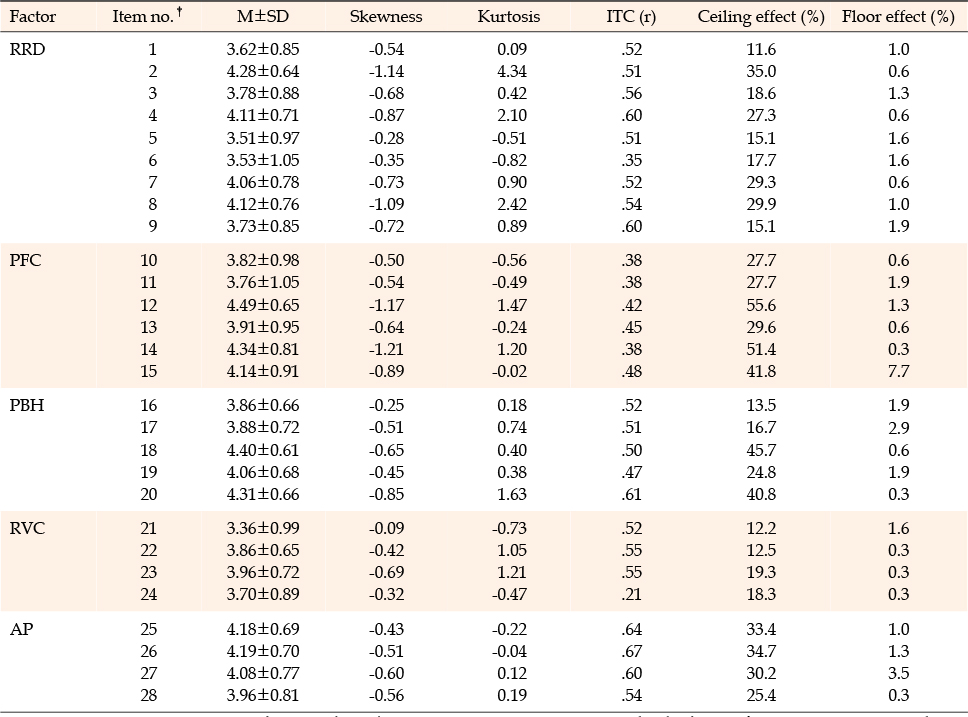
Table 2
Ceiling and Floor Effects of the Korean Version of the NEBPPRS (N=311)
The ceiling effect spanned from 11.6% to 55.6%, and the floor effect was between 0.3% and 7.7%. A total of 9 items exhibited a ceiling effect of 30.0% or more (items 2,12,14,15,18,20,25,26,27), but no items presented a floor effect of 30.0% or more (Table 2).
The corrected item-total correlation ranged from .21 to.67. Item 26, "I refrain from sharing patient information with the people who are not involved in the care and treatment process", had the highest correlation coefficient (r=.67), while item 24, "I refrain from performing professional practices refused by the patient", had the lowest correlation coefficient (r=.21). Five items had correlation coefficient (r) values less than .40 (Table 2).
Throughout the research process, permission to modify and delete items based on statistical analysis results and cultural characteristics was granted by the developer of the NEBPPRS via email. The researchers noted 5 items (6,10,11,14,24) with correlation coefficients (r) less than .40 between the items and the total score, suggesting minimal contributions to the scale [26]. After expert consultation, discussions with the developer, and careful consideration, 3 items (6,14,24) were removed. The final Korean version of the NEBPPRS, now known as NEBPPRS-K25, consists of 5 factors and 25 items.
The model fit values in this study were as follows: normed χ2 (CMIN/DF) value of 2.56, p<.001, RMR=.05, RMSEA=.07, GFI=.84, CFI=.86, TLI=.85, IFI=.87 (Table 3). The analysis of item convergent and discriminant validity revealed that the standardized coefficients (λ) for the 25 items ranged between .50 and .84. The AVE values for the 5 sub-factors spanned from .54 to .65, and the CR values ranged from .78 to .90. Regarding discriminant validity, no factors included 1 within the range of twice the standard error of the correlation coefficients (Table 4). The measurement model of the nursing ethical behavior assessment tool is illustrated in Figure 1.
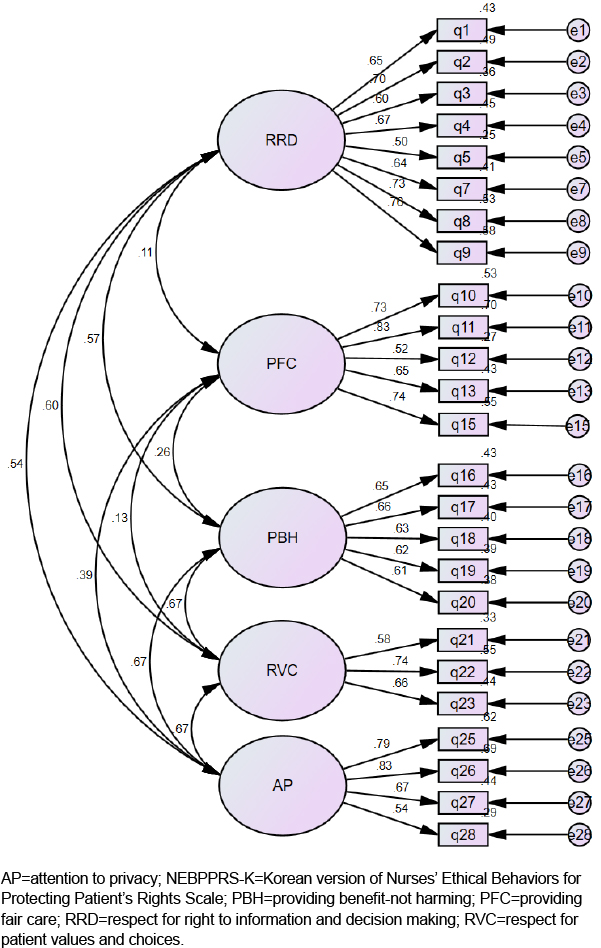
Figure 1
Measurement model of the NEBPPRS-K25.

Table 3
Summary of Indices from Confirmatory Factor Analysis for the NEBPPRS-K25 (N=311)
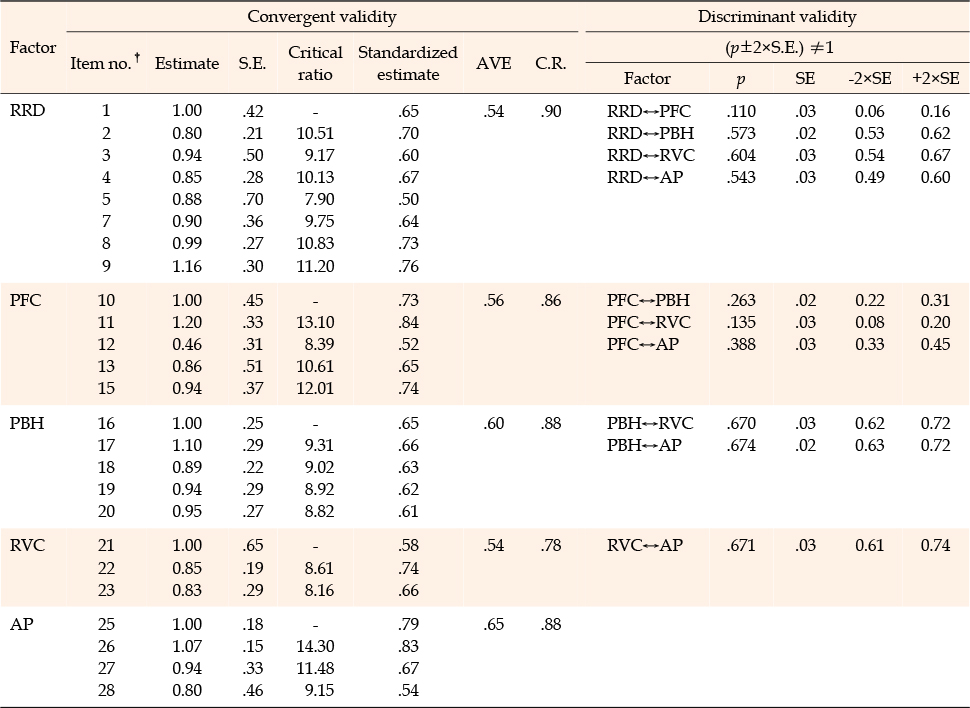
Table 4
Convergent and Discriminant Validity (N=311)
The analysis of average ethical behavior scores based on the experience of nursing ethics education showed that nurses who had experienced nursing ethics education scored 100.35±10.49, which was statistically significantly higher than the score of nurses with no such experience (96.59±9.40; t=2.82 and p=.005).
The internal consistency analysis showed a Cronbach's α value of .89 for the overall reliability of the tool. The reliability of each sub-factor was shown by Cronbach's α values ranging from .66 to .85. "Respect for right to information and decision making" had a Cronbach's α of .85, "providing fair care" had a Cronbach's α of .83, "providing benefit-not harming" had a Cronbach's α of .77, "respect for patient values and choices" had a Cronbach's α of .66, and "attention to privacy" had a Cronbach's α of.79. There were no items whose removal would have resulted in a higher Cronbach's α value than the overall .89.
To respect and protect patients' rights, nurses, along with other healthcare professionals, need to uphold the highest ethical standards when making decisions and taking actions. Yet, nurses frequently encounter numerous ethical dilemmas and may find it challenging to exercise ethical nursing for the protection of patient rights due to the absence of systematic support within hospitals, such as ethical consultations, education, and systems for resolving problems [14]. Regardless of the ethical conflicts they face in clinical settings, it's imperative for nurses to establish and adhere to their values related to nursing ethics [19]. Consequently, this study evaluated the cultural validity and reliability of the Korean translation of NEBPPRS-K25, which originates from the originally Turkish-developed NEBPPRS.
The item analysis results confirmed the normality of the data distribution for each item, as they met the criteria of the skewness absolute value being less than 2 and the kurtosis absolute value being less than 7 [27]. Ceiling and floor effects were evaluated by determining if the frequency of the highest and lowest scoring items was less than 30% [28]. In the development of the tool, items with high ceiling effects are considered to be of low discriminative value and contribute little to concept measurement [29]. There were 9 items with a ceiling effect exceeding 30% with item 12, "I refrain from providing care for the patients whose political opinions are different than mine", (55.6%), item 14, "I am curious about the private lives of patients", (51.4%), and item 18, "I take precautions against situations that may harm the patient", (45.7%) having the highest ceiling effects in descending order. This likely stems from the fact that nurses' professional duties inherently incorporate ethical responsibilities [30], and the ethical nature of nursing [31] leads to higher self-ratings on ethical items, resulting in elevated measured ceiling effects. As previously mentioned, specific items that were deleted or retained in the original tool were closely examined, taking into account correlation coefficient (r) values below 0.40 and discussions with the developer of the original tool. The details are as follows: item 6, "I think it is not necessary to explain the practices I will perform to the patients who lost their ability to make decisions (unconscious)", was deleted due to the presence of similar items in the tool (e.g., "I inform the patient before my professional practices") and the practicality of explaining treatment procedures to unconscious patients in a clinical setting. However, if the definition of patients with impaired decision-making capacity is expanded beyond unconscious patients to include those with dementia, mental illnesses, and children, the removal of this item could be perceived as a limitation of the Korean version of the tool. As a result, it is advised that the meaning of item 6 be carefully considered when translating and using the original tool in another language in a different country. Other deleted items such as item 14, "I am curious about the private lives of patients", and item 24, "I refrain from performing professional practices refused by the patient", were deemed non-discriminative, as they could exhibit high ceiling effects when considering the characteristics of clinical nursing practice in Korea.
The items that were retained despite having a low correlation coefficient included item 10, "I provide more attentive nursing care for the patients whose socioeconomic levels are higher", (r=.38), and item 11, "I provide more attentive nursing care for the patients whose belief are similar/close to mine", (r=.38). due to expert opinions asserting their significance in measuring the sub-scale to which they belong, namely "providing fair nursing". As a result, the modified Korean version, NEBPPRS-K25, comprising 5 factors and 25 items was finalized.
The construct validity of NEBPPRS-K25 was verified through the tool's factor structure and model fit, and both the absolute and incremental fit indices met the criteria. When the AVE value is 0.50 or higher, or the CR value is 0.70 or higher, convergent and discriminant validity can be ensured [32]. No factors fell short of these standards. Thus, item convergent validity was secured. The discriminant validity results satisfied the criterion that the range of twice the standard error of all inter-factor correlation coefficients does not include 1 [32], affirming that the 5 factors were unique, had low inter-factor correlations, and were independent factors.
According to the results of the CFA, the five sub-factors appropriately assess the ethical nursing behavior concept for protecting patients' rights, which this Korean version tool aims to measure. To begin, the first sub-factor "respect for right to information and decision making" is well measured by items such as "I make the care-related decision with the patient" and "I create an opportunity for the patient to take part in care and treatment decisions. The second sub-factor, "providing fair care", is measured by items that ask whether more attentive care is provided to patients with similar or close beliefs or with higher socioeconomic status. The third sub-factor, "providing benefit-not harming", is assessed through items that determine whether professional treatment is harmful or beneficial to patients. The fourth sub-factor, "respect for patient values and choices", is measured by items such as "I respect a patient's right to perform his/her prayers" and "I respect a patient's right to select the caregiver and health professional that will provide care and treatment". Finally, the "attention to privacy" sub-factor is assessed using items such as "I refrain from sharing patient information with the people who are not involved in the care and treatment process" and "I receive the patient's consent to get a practice done/watched on the patient with training purposes".
Based on the hypothesis that receiving nursing ethics education leads to ethical behavior [18], known-group validity was confirmed through the observation of significant differences in nurses' ethical behavior depending on their experience with ethics education. This validates the tool's ability to measure differences between groups in empirical phenomena based on the above hypothesis.
The overall reliability of NEBPPRS-K25 was satisfactory, with a Cronbach's α of .89, a figure slightly higher than the original tool's Cronbach's α of .84. The fact that the tool's Cronbach's α value did not increase even when items were removed suggests that each item contributes equally to the reliability. Consequently, the reliability coefficients for each sub-factor also met the criteria, signifying that reliability had been achieved.
The NEBPPRS-K25, as validated in this study, has adequate validity and reliability for assessing nurses' ethical behavior in the protection of patients' rights. This study specifically aimed to ensure that clinical nurses caring for adult patients uphold ethical nursing practices by prioritizing the protection of patient rights [19]. Furthermore, the objective of this study was to provide research and baseline data to promote ethical behavior among nurses and, ultimately, to enhance the protection of patient rights.
One limitation of the study was the difficulty in generalizing the research findings due to the use of data sampled from nurses working at university hospitals in three regions. Additionally, the absence of test-retest reliability implies that the tool's stability in measuring the concept over time was not ensured. Another limitation was the inability to evaluate criterion validity, as it was challenging to identify an ethical nursing behavior tool with a matching construct to serve as a gold standard. Thus, it is hoped that future validation studies will address this issue.
The NEBPPRS-K25, as validated in this study, seems suitable for assessing nurses' ethical behavior in relation to the protection of patient rights. Now that its validity and reliability have been established, the tool is expected to see widespread use. Furthermore, it should provide research and baseline data to promote ethical behavior among nurses, with the ultimate goal of bolstering the protection of patient rights.
The following recommendations are proposed: First, it is suggested that medical institutions employ this tool to safeguard patient rights while also assessing and enhancing nurses' ethical behavior. Second, future studies should conduct test-retest reliability and criterion validity analyses, which were not performed in the current study.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - YJ and OH.
Data collection - YJH.
Analysis and interpretation of the data - YJ and OH.
Drafting and critical revision of the manuscript - YJ.
Critical revision of the manuscript - OH.
Advise study process - OH.
This article is a condensed form of the first author's master's thesis from Eulji University.
 E-SUBMISSION
E-SUBMISSION