
Purpose
This study's purpose was to identify the relationship between daily vitamin intake and blood glucose in cancer patients undergoing chemotherapy and identify factors affecting blood glucose.
Methods
This descriptive study included 134 cancer patients undergoing chemotherapy at a university hospital. Data were analyzed with descriptive statistics, independent T-test, one-way analysis of variance, Pearson's correlation coefficients, and stepwise multiple regression analysis using SPSS/WIN 27.0 version.
Results
The average blood glucose of the subjects was 128.13±37.34 mg/dL and 30.6% of the subjects had readings of over 140 mg/dL. Blood glucose varied significantly by sex, age, education level, exercise frequency, and comorbidity. Vitamins A, E, and C, thiamin, riboflavin, niacin, vitamin B6, folate, and biotin were negatively correlated with blood glucose. Factors affecting blood glucose were exercising 7 times a week (β=-.61, p<.001), 4 to 6 times a week (β=-.41, p<.001), 1 to 3 times a week (β=-.38, p<.001), age (β=.18, p=.016), and vitamin A intake (β=-.16, p<.043), with a total explanatory power of approximately 31.5%.
Conclusion
Nurses should provide patients undergoing chemotherapy with lifestyle interventions including exercise at least 3 days a week and appropriate vitamin A intake, especially for older patients, to prevent hyperglycemia.
This study's purpose was to identify the relationship between daily vitamin intake and blood glucose in cancer patients undergoing chemotherapy and identify factors affecting blood glucose.
This descriptive study included 134 cancer patients undergoing chemotherapy at a university hospital. Data were analyzed with descriptive statistics, independent T-test, one-way analysis of variance, Pearson's correlation coefficients, and stepwise multiple regression analysis using SPSS/WIN 27.0 version.
The average blood glucose of the subjects was 128.13±37.34 mg/dL and 30.6% of the subjects had readings of over 140 mg/dL. Blood glucose varied significantly by sex, age, education level, exercise frequency, and comorbidity. Vitamins A, E, and C, thiamin, riboflavin, niacin, vitamin B6, folate, and biotin were negatively correlated with blood glucose. Factors affecting blood glucose were exercising 7 times a week (β=-.61, p<.001), 4 to 6 times a week (β=-.41, p<.001), 1 to 3 times a week (β=-.38, p<.001), age (β=.18, p=.016), and vitamin A intake (β=-.16, p<.043), with a total explanatory power of approximately 31.5%.
Nurses should provide patients undergoing chemotherapy with lifestyle interventions including exercise at least 3 days a week and appropriate vitamin A intake, especially for older patients, to prevent hyperglycemia.
As of 2019, the lifetime risk of developing cancer among the Korean population was 37.9%, with 1 out of every 25 people of all ages and 1 out of every 8 older adults (≥65 years) being diagnosed with cancer. The 5-year survival rate of cancer patients has continuously improved thanks to advancements in cancer treatment, and 7 out of 10 cancer patients survive for 5 years or more [1]. This is a result of groundbreaking developments in therapeutic options for cancer and chemotherapy, a representative cancer treatment performed for 60~70% of cancer patients [2]. However, chemotherapy can cause side effects, such as nausea, vomiting, diarrhea, liver, heart, and kidney dysfunction, and hyperglycemia [2]. Hyperglycemia is experienced by 10~30% of patients who undergo chemotherapy, and anticancer drugs can increase the blood glucose levels of nondiabetic cancer patients or worsen existing diabetes [3].
In hyperglycemia, excessive amounts of glucose circulate in the blood plasma owing to insufficient insulin secretion or inability to effectively use insulin. In severe systemic diseases like cancer, random plasma glucose levels of 140 mg/dL or higher is considered hyperglycemic, regardless of history of diabetes or fasting [4, 5]. Anticancer drugs known to cause hyperglycemia include 5-fluorouracil [6, 7], cisplatin [7, 8], carboplatin [8], docetaxel [5, 9], and steroids [3, 9]. 5-fluorouracil increases the blood glucose levels of cancer patients by causing toxicity in the β-cells of the pancreas that secrete insulin [6]. In a study in which nondiabetic cancer patients were given the 5-fluorouracil and cisplatin regimen, 77% experienced hyperglycemia [7]. In another study in which nondiabetic patients with gynecologic cancer were treated with the cisplatin and carboplatin regime, 4.8% were diagnosed with diabetes after the intervention [8]. The mechanism by which docetaxel raises blood glucose levels is unclear, but hyperglycemia has been reported in 6~15% of patients who receive a combined therapy of docetaxel and other antineoplastic agents [5, 10].
Chemotherapy can cause hyperglycemia, which may have implications for treatment efficacy, prognosis, and adverse effects in cancer patients [5, 11]. Breast cancer patients who develop hyperglycemia after chemotherapy have a 9.7% higher risk of recurrence and a 2.6% lower 5-year survival rate than patients with normal blood glucose levels, suggesting greater risk of recurrence and mortality in hyperglycemic patients [5]. Moreover, up to 50% of patients who undergo chemotherapy and consequently develop hyperglycemia may have a higher incidence of chemotherapy-induced adverse effects, including leukopenia, thrombocytopenia, anemia, diarrhea, peripheral neuropathy, nausea, and vomiting [11]. To reduce hyperglycemia-induced side effects, interventions are needed to prevent and manage hyperglycemia in patients undergoing chemotherapy. Therefore, it is crucial to identify factors that can reduce blood glucose levels and incorporate them into nursing interventions to manage hyperglycemia in this patient population.
Recent studies on diabetic patients and the general population have reported that vitamin intake significantly reduces excessive blood glucose levels [12]. Studies have found that the intake of vitamins C and A and their metabolites, such as retinol, vitamin B2 (riboflavin), and vitamin B1 (thiamine), was significantly lower in the diabetic group compared with the nondiabetic group [12, 13]. However, research is lacking on the impact of vitamin intake on blood glucose levels in cancer patients undergoing chemotherapy. Vitamins are crucial in improving various physiological functions and immunity, and recent studies have reported their significant effects on reducing blood glucose levels [12, 13, 14]. Hence, it would be of great significance in nursing practice to examine the impact of vitamin intake on high blood glucose levels in cancer patients undergoing chemotherapy and incorporate the findings into nursing interventions for hyperglycemia management in cancer patients. Therefore, this study aims to understand the effect of vitamin intake on blood glucose levels in cancer patients undergoing chemotherapy and provide basic data necessary for nursing interventions and patient education to prevent and manage hyperglycemia in this patient group.
This study aims to understand the relationship between vitamin intake and blood glucose levels in cancer patients undergoing chemotherapy. Hence, three objectives were specified: (1) Identifying the differences in blood glucose levels according to the general and disease-related characteristics of patients undergoing chemotherapy; (2) Investigating the correlation between the intake of vitamins A, D, E, C, thiamine, riboflavin, niacin, B6, folate, B12, pantothenic acid, and biotin and blood glucose levels in patients undergoing chemotherapy; and (3) Identifying factors that affect blood glucose levels in patients undergoing chemotherapy.
A descriptive survey design was used to examine the effect of vitamin intake on blood glucose levels in cancer patients undergoing chemotherapy.
Cancer patients who had received at least three chemotherapy cycles with 5-fluorouracil, cisplatin, carboplatin, or docetaxel at K University Hospital in D City were recruited from July 1, 2021 to March 31, 2022. Inclusion criteria were (i) 18 years and older, (ii) capability of communication necessary for answering questionnaires, and (iii) submission of signed informed consent form to participate in the study. Patients undergoing complete non-oral nutrition therapy or steroid therapy combined with chemotherapy, and those diagnosed with diabetes before chemotherapy were excluded from the study.
The sample size was calculated using G*Power 3.1.9.4 program, with the effect size set to 0.15, significance level to .05, and power to 80%, drawing on a previous study's results [15]. Thus, the minimum required sample size for regression analysis was calculated to be 129 participants. Considering a dropout rate of 10%, the minimum sample size was set at 144, and data were collected from 144 subjects. After excluding 10 dropouts, 134 patients were finally selected as study subjects.
Data regarding general characteristics, such as sex, age, occupation, marital status, education level, alchol use, smoking, Body Mass Index (BMI), and exercise frequency, were collected through a questionnaire survey. Diseaserelated data, such as diagnosed disease name, stage, comorbidities, and random plasma glucose levels, were obtained from Electronic Medical Records (EMR).
Drawing on a previous study [5] that analyzed factors affecting chemotherapy-induced hyperglycemia using random plasma glucose, this study used mean random plasma glucose levels of the last and penultimate blood tests from the time of investigation among the regular tests administered before each chemotherapy cycle. Blood samples were collected from the basilic or median cubital vein, and glucose levels were measured using the enzymatic UV hexokinase method on the Cobas Connection Modules System (Roche, Basel, Switzerland) at the Department of Laboratory Medicine of K University Hospital. Hyperglycemia was defined as a mean random plasma glucose level of 140 mg/dL or higher [4, 5].
Vitamin intake was assessed using the Food Frequency Questionnaire, a survey tool utilized in the 7th Korean National Health and Nutrition Examination Survey (KNHANES-VII). It comprises 112 items and rates food intake on a scale of nine frequency categories (almost none, 1/day, 2/day, 3/day, 1~2/week, 3~4/week, 5~6/week, 1/month, and 2/month) and three quantity categories (small, moderate, and large) [16]. Each participant's vitamin intake was analyzed using CAN pro 4.0, a nutrition assessment program developed by the Korean Nutrition Society.
Data were collected from June 2021 to March 2022, after obtaining approval from the institutional review board of K University in D City (IRB No. 40525-202011-HR-057-02). Data were collected by a single researcher who read the questionnaire to the participants and recorded their responses sequentially. The researcher explained the study's purpose to the participants, ensured anonymity of their personal information, and informed them that disease-related characteristics would be obtained from EMR and that the collected data would be securely stored and destroyed after a retention period of three years. Participants were informed that they could refuse participation or withdraw from the study at any time. After obtaining each participant's signed informed consent form, the survey was conducted. General characteristics and food frequency questionnaires were administered in person, and they took an average of 30 minutes to complete. After completing the questionnaire, participants were given a token of appreciation. The filled-in questionnaires were coded to ensure anonymity and confidentiality, and the program file containing the study data was password-protected and managed exclusively by the researcher.
The data collected in this study were analyzed using SPSS/WIN 27.0 as follows:
• Differences in blood glucose levels depending on patients' general and disease-related characteristics were analyzed using independent samples t-test, one-way analysis of variance, and Scheffé post hoc test.
• Correlation between vitamin intake and blood glucose levels was analyzed using Pearson's correlation coefficient.
• Factors influencing blood glucose levels were analyzed using stepwise multiple regression.
The general characteristics are as follows: 55.2% were male and 44.8% were female; mean age was 64.5 years, with the highest proportion (38.8%) aged 70 and above; 41.8% were employed; 82.1% were married; the highest proportion of participants (39.6%) had graduated high school; 3.7% reported alchol use, and 3.0% were smokers; the mean BMI was 23.48 kg/m2, with the normal-weight group accounting for the largest proportion (40.3%); 39.6% of the patients exercised every day, and 38.8%, 3 times or less per week (Table 1).
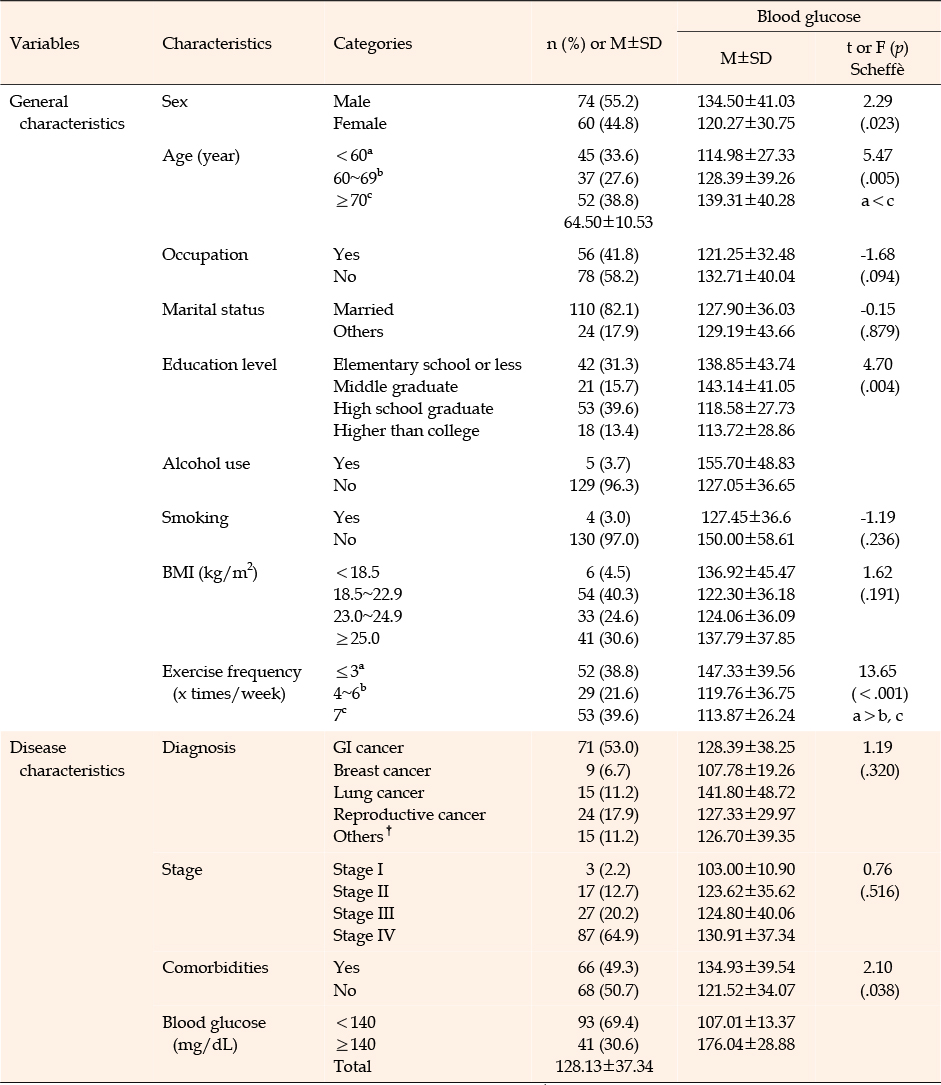
Table 1
General and Disease Characteristics Based on Participants’ Blood Glucose Status
The disease-related characteristics are as follows: gastrointestinal cancer was the most common type of cancer (53.0%), stage IV or higher was the most prevalent stage (64.9%), and 49.3% had comorbidities. The mean blood glucose level was 128.13 mg/dL, with 30.6% having levels of 140 mg/dL or higher (Table 1).
Significant differences in blood glucose levels were observed by sex (t=2.29, p=.023), age (F=5.47, p=.005), education level (F=4.70, p=.004), weekly exercise frequency (F=13.65, p<.001), and comorbidities (t=2.10, p=.038). Mean blood glucose level was higher in males than females. Participants in their 70s and above had a higher mean blood glucose level than those in their 60s and below. Those who exercised three times or less per week had a significantly higher mean blood glucose level than those who exercised 4~6 times per week and 7 times per week. Those with comorbidities had a significantly higher mean blood glucose level than those without comorbidities (Table 1).
Vitamin intake was assessed using the Food Frequency Questionnaire. Survey results were analyzed as follows: the participants consumed more than the recommended amounts of vitamin A, vitamin E, vitamin C, thiamine, riboflavin, niacin, vitamin B6, folate, pantothenic acid, and biotin, but less than the recommended amount of vitamin D (Table 2).
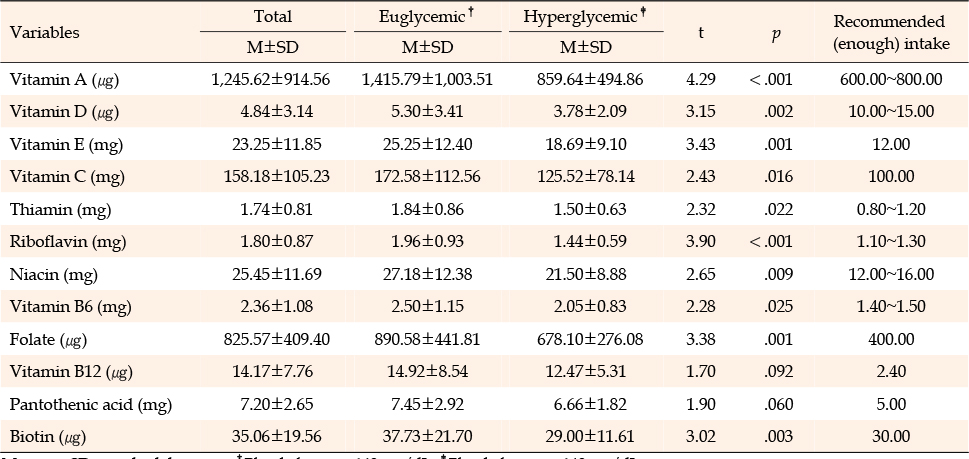
Table 2
Daily Vitamin Intake
Participants were divided into euglycemic and hyperglycemic groups to compare their vitamin intake status. Analysis revealed significant differences in vitamin A (t=4.29, p<.001), vitamin D (t=3.15, p=.002), vitamin E (t= 3.43, p=.001), vitamin C (t=2.43, p=.016), thiamine (t=2.32, p=.022), riboflavin (t=3.90, p<.001), niacin (t=2.65, p=.009), vitamin B6 (t=2.28, p=.025), folate (t=3.38, p=.001), and biotin (t=3.02, p=.003), with the euglycemic group having a higher average intake than the hyperglycemic group (Table 2).
Correlation analysis between vitamin intake and mean blood glucose revealed that mean blood glucose levels are negatively correlated with vitamin A (r=-.31, p<.001), vitamin E (r=-.25, p=.004), vitamin C (r=-.19, p=.027), thiamine (r=-.17, p=.046), riboflavin (r=-.27, p=.027), niacin (r=-.19, p=.027), vitamin B6 (r=-.21, p=.016), folate (r=-.23, p=.007), and biotin (r=-.14, p=.008) (Table 3).
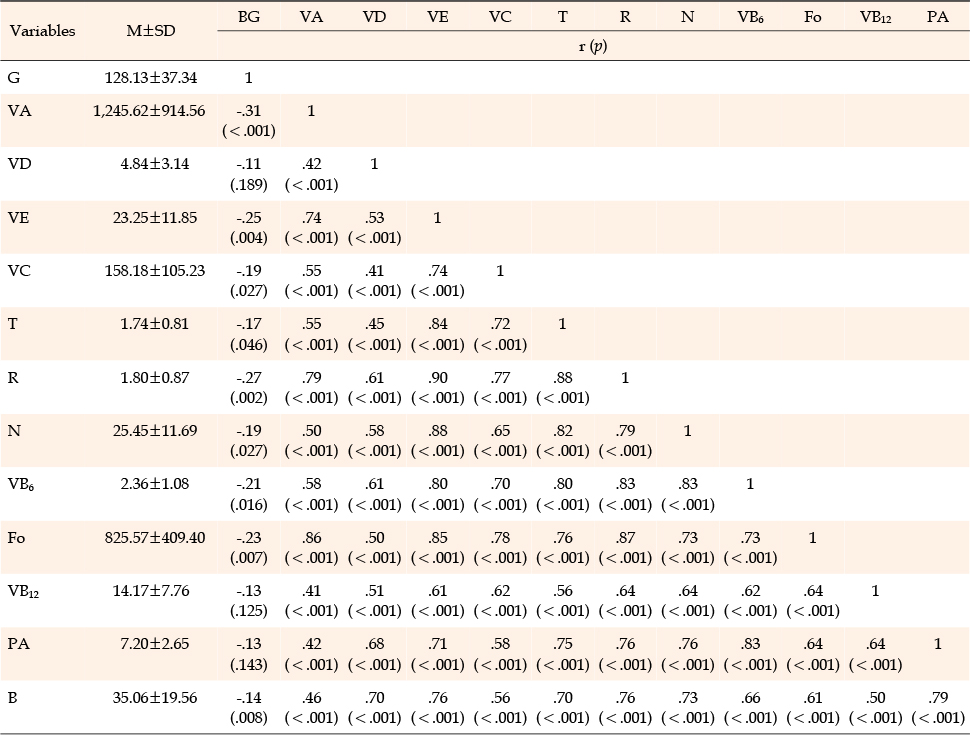
Table 3
Correlation between Daily Vitamin Intake and Blood Glucose
Factors influencing blood glucose levels were analyzed through multiple stepwise regression analysis using significant independent variables: sex, age, education level, weekly exercise frequency, comorbidities, and vitamin intake (vitamins A, E, and C, thiamine, riboflavin, niacin, vitamin B6, folate, and biotin). In order to figure out how blood sugar changes with increasing exercise, we analyzed the other groups against a group that did not exercise at all for one week. The analysis results are outlined in Table 4. First, the multicollinearity of the independent variables was confirmed by checking the tolerance and Variance Inflation Factor (VIF) values. Tolerance values above 0.1 and VIF values less than 10 indicated multicollinearity was not a problem. The Durbin-Watson statistic, which checks the independence of residuals, was 1.67, indicating no autocorrelation, and the Cook's distance statistic was less than 1.0, confirming the absence of outliers. Additionally, the Breusch-Pagan test for homoscedasticity resulted in p=.138, satisfying the assumption of homoscedasticity, and the adequacy of the regression model was confirmed.
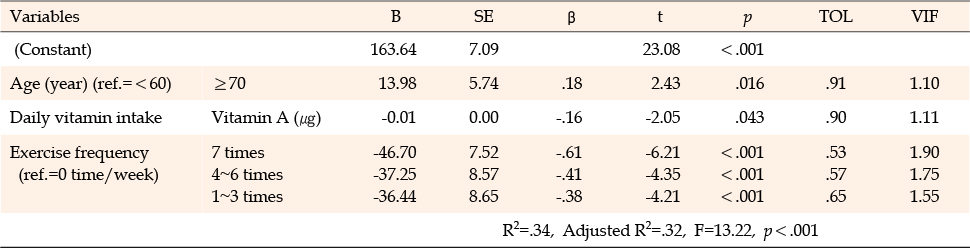
Table 4
Factors Influencing Blood Glucose
The following factors were identified as contributing to decreasing blood glucose levels of cancer patients undergoing chemotherapy, with a total explanatory power of 32.0% in descending order of impact: exercise frequency of 7 times a week (β=-.61, p<.001), 4-6 times a week (β=-.41, p<.001), and 1-3 times a week (β=-.38, p<.001) vs. no exercise, age group of 70s and over (β=.18, p=.016) vs. ≤60s, and vitamin A intake (β=-.16, p=.043) (Table 4).
This quantitative descriptive study examined the effect of vitamin intake on blood glucose levels in patients undergoing chemotherapy with the aim of providing basic data for developing nursing intervention programs to help prevent chemotherapy-induced hyperglycemia in cancer patients. The mean blood glucose level of the participants was 128.13±37.34 mg/dL, with 30.6% of them having levels of 140 mg/dL or higher, which is the screening threshold for hyperglycemia. This finding is similar to those of previous studies that 10-30% of patients undergoing chemotherapy develop hyperglycemia [3], indicating that a significant proportion of cancer patients undergoing chemotherapy are at risk of developing hyperglycemia. Hence, the prevention and management of hyperglycemia in patients undergoing chemotherapy should be strengthened to prevent complications and enhance therapeutic effectiveness.
The general characteristics of age, weekly exercise frequency, and vitamin A intake were identified as factors that significantly affect blood glucose levels in patients undergoing chemotherapy. Among them, exercise frequency has the greatest impact on blood glucose levels in the order of 7 times, 4~6 times, and 1~3 times a week (reference: no exercise), with the lowest blood glucose levels observed in those who exercised every day. This finding is supported by a previous study [17] that compared the risk of developing diabetes between non-exercise and regular exercise (≥3 times a week) groups and found the nonexercise group had a 21% higher risk of diabetes than the regular exercise group. Another study [18] found that blood glucose was better controlled by increasing weekly exercise frequency, with a 4.55-fold blood glucose decrease in the 2~4 days/week group and a 15-fold decrease in the 5~7 days/week group vs. ≤1 day/week group, similar to the results of this study.
While muscle glycogen is the primary energy source in the initial phase of exercise, as exercise time increases, muscle glycogen decreases and the use of blood glucose increases. Insulin sensitivity continues to increase for about 60 hours after exercise, returning to pre-exercise levels after 3~5 days [19]. This suggests that regular exercise at 2~3-day intervals can contribute to maintaining insulin sensitivity. The risk of developing diabetes reduces by 21% in those who engage in exercise until sweating at least three times a week compared with those who do not exercise [17]. In this regard, follow-up research is proposed to measure the exact amount and intensity of exercise for cancer patients undergoing chemotherapy and compare the risk of hyperglycemia according to exercise amount and intensity.
This study identified age as the second factor that affects blood glucose levels in patients undergoing chemotherapy. The mean blood glucose level increases with age, and those in their 70s and older had significantly higher blood glucose levels than those in their 60s and younger. This finding is consistent with that of a previous study with nondiabetic subjects, which found that the risk of hyperglycemia increases with age [20]. Aging is accompanied by a significant increase in abdominal fat mass, mitochondrial dysfunction, oxidative stress, and inflammatory response, as well as muscle mass loss, leading to insulin resistance and elevated blood glucose levels [21]. Therefore, preventive management to avoid the onset of hyperglycemia is even more important as one ages.
Vitamin A intake also affects blood glucose levels in patients undergoing chemotherapy, with a higher amount of vitamin A intake associated with lower blood glucose levels. Participants' average vitamin A intake was higher than the recommended amount, and it was significantly higher in the euglycemic group (<140 mg/dL) than in the hyperglycemic group (≥140 mg/dL). This is consistent with studies in which serum vitamin A concentration was found to be lower in diabetic patients than in healthy individuals [14, 22]; for example, a Korean study with diabetic patients measured 630 µg/day lower average vitamin A intake in the group with poor blood glucose control compared with the group with good blood glucose control [23], and a US study that compared insulin-mediated glucose disposal after consuming grape sugar between the high vitamin A intake group (≥3,000 µg/day) and low vitamin A intake group (≤2,400 µg/day) found that the high vitamin A intake group had significantly lower plasma glucose responses [24]. In combination with previous research findings that chemotherapy decreases the serum concentrations of beta-carotene, alpha-carotene, and retinol, which are precursors of vitamin A [25], this study's vitamin A-related result provides evidence that the decreased amount of vitamin A due to decreased vitamin A precursor levels is a significant factor affecting hyperglycemia.
Vitamin A is an essential fat-soluble vitamin that plays a crucial role in normal growth and development, reproduction, epithelial cell differentiation, cell proliferation, and normal immune responses. Vitamin A and its derivatives are involved in biological development and aging [26]. Vitamin A also influences the development of the pancreas and regulation of the Langerhans islets. Vitamin A deficiency can lead to hyperglycemia by causing destruction of beta cells that secrete insulin and decreasing insulin synthesis [14, 22]. Therefore, it is necessary to recommend vitamin A-rich green and yellow vegetables, fruits, fish, poultry, and dairy products to cancer patients undergoing chemotherapy [14, 26]. However, since excessive vitamin A intake can cause toxicity in the skin, mucous membranes, liver, and bones as well as side effects such as nausea and vomiting, it is essential to limit its intake to an appropriate amount [27]. The Ministry of Health and Welfare recommends a daily intake of 700~800 µg and 600~650 µg for adult men and women, respectively, setting the upper limit to 3,000 µg/day [26]. When providing dietary education to patients, it is important to guide them to comply with the appropriate vitamin A intake and provide continuous monitoring to check for deficiency symptoms and toxicity responses due to excessive intake.
Additionally, although not identified as factors affecting blood glucose levels in this study, vitamin E, vitamin C, thiamine, riboflavin, niacin, vitamin B6, folate, and biotin were found to be inversely correlated with blood glucose levels. Vitamin E is a fat-soluble vitamin that prevents organ damage caused by reactive oxygen species, improves blood oxygen supply, and removes toxins from the system, all of which enhance insulin function while significantly reducing C-reactive protein, cytokines, and tumor necrosis factors [14]. A Korean study comparing good and poor glycemic control groups found that the good glycemic control group had two-fold the intake of vitamin E of the poor glycemic control group (12.9±5.90 vs. 6.5±3.70 mg/day) [23], similar to our finding that the euglycemic group had a significantly higher mean vitamin E intake than the hyperglycemic group (24.25±12.40 vs. 18.69±9.10 mg/day). Vitamin E deficiency is associated with health problems such as muscle weakness, skeletal myopathy, and retinopathy, which highlights the importance of educating patients to consume vegetable oils, seeds, and nuts to ensure adequate vitamin E intake [14, 26]. However, excessive vitamin E intake can lead to side effects such as creatinuria, decreased platelet aggregation, delayed wound healing, amenorrhea, fatigue, diplopia, and muscle weakness [26]. Therefore, patients should be educated to consume an appropriate amount of vitamin E, not exceeding the upper limit of 540 mg/day [26].
Regarding the vitamins C and B group, the higher their intake, the lower the level of homocysteine, which increases oxidative stress, insulin resistance, beta-cell dysfunction, systemic inflammation, and endothelial dysfunction, and the lower the likelihood of developing diabetes [14]. A Korean study comparing nondiabetic and diabetic groups found that the intake of the vitamins C and B group (thiamine, riboflavin, niacin, biotin, and folate) was significantly lower in the diabetic group [12]. In this study, the vitamin C (t=2.43, p=.016), thiamine (t=2.32, p=.022), riboflavin (t=3.90, p<.001), niacin (t=2.65, p=.009), vitamin B6 (t=2.28, p=.025), folate (t=3.38, p=.001), and biotin (t=3.02, p=.003) intake of the hyperglycemic group was significantly higher than that of the euglycemic group. Since vitamin C is not synthesized in the body, adequate intake should be ensured by consuming sufficient fresh fruits and vegetables [14]. However, excessive vitamin C intake can cause gastrointestinal disorders, such as nausea, vomiting, abdominal bloating, and osmotic diarrhea, so patients should be educated not to exceed the upper limit of 2,000 mg/day [26]. Similarly, although harmful effects of niacin intake through food have not been reported, excessive intake through supplements and niacin-enriched foods can cause gastrointestinal disorders, such as nausea, and liver toxicity [26]. Therefore, patients using anticancer drugs that can cause nausea, vomiting, stomatitis, and diarrhea should be monitored to prevent excessive niacin intake and to assess nutritional status, including dietary supplements, and be educated to consume niacin within the limit of 1,000 mg/day (reference: niacinamide). Regarding folate and vitamin B6, since they are found in fruits, grains, poultry, eggs, nuts, chickpeas, dairy products, meat, and seafood, patients should be educated to eat a balanced diet rather than recommending specific foods [14].
In this study, vitamin D showed no correlation with blood glucose levels, but differed significantly between the euglycemic and hyperglycemic groups. However, several studies have reported a correlation between vitamin D and blood glucose levels [14, 28]. A specific receptor in pancreatic beta cells responds only to vitamin D, and vitamin D attaches to this receptor, which prevents beta cell death and stimulates insulin secretion, thus preventing diabetes or metabolic syndrome. This suggests that vitamin D deficiency is a risk factor for diabetes as it worsens insulin resistance and reduces beta cell function [14]. In this study, the euglycemic group had a mean vitamin D intake of 5.30±3.41 µg/day, while the hyperglycemic group had a significantly lower intake of 3.78±2.09 µg/day, supporting the research finding that diabetic patients with vitamin D deficiency have a 22.55-fold risk of poor glycemic control [28]. Unlike with other vitamins, the participants had a much lower vitamin D intake (4.84±3.14 µg/day) than the recommended intake (10-15 µg/day). Inadequate vitamin D intake increases not only the risk of hyperglycemia, but also that of osteomalacia, osteoporosis, falls, and deterioration in physical function in the elderly and vulnerable populations [26]. Therefore, patients should be educated to increase their consumption of vitamin D-rich fish, such as salmon, tuna, mackerel, and sardines, as well as dairy products and cereals, and increase their outdoor activity during sunny days [14, 28].
This study explored factors that influence blood glucose levels in cancer patients undergoing chemotherapy, focusing on the relationship between vitamin intake and blood glucose levels. Despite the potential impact of hyperglycemia on various side effects and treatment outcomes in cancer patients undergoing chemotherapy, understanding is lacking of the factors that affect blood glucose levels in these patients. Currently, most cancer patients receive uniform dietary education rather than customized nursing interventions based on their personal exercise and dietary practices, which is especially important for cancer patients. This study is significant in this context because it provides important evidence-based data for the development of hyperglycemia prevention and blood glucose management programs for cancer patients undergoing chemotherapy, considering major influencing factors such as weekly exercise frequency, age, and vitamin A intake.
Nevertheless, this study has several limitations. First, it was conducted at a single university hospital, so caution is warranted in generalizing its findings. Second, it only investigated food-based vitamin intake, disregarding the use and types of dietary supplements, which should be considered in follow-up research. Finally, it investigated weekly exercise frequency without differentiating exercise intensity or duration, which should be considered in follow-up research.
This study aimed to examine the effect of vitamin intake on blood glucose levels in cancer patients undergoing chemotherapy and provide basic data for the development of nursing interventions for hyperglycemia prevention and blood glucose management in these patients. This study's analyses categorized 30.6% of the participants as hyperglycemic and identified weekly exercise frequency, age, and vitamin A intake as major factors affecting blood glucose levels. Since hyperglycemia can have various side effects and affect cancer treatment outcomes, blood glucose levels should be regulated. Therefore, personalized dietary education and exercise interventions should be provided for patients undergoing chemotherapy to encourage them to engage in exercise at least three times a week and take vitamin A from food, including dietary supplements, if necessary, within the toxic safety limit, by assessing vitamin A intake, especially in older adults.
Based on the study results, the following proposals are made: First, research extending this study is suggested by expanding sample size and including variables found to have significant correlations with hyperglycemia in previous studies in addition to those identified as influencing factors in this study. Second, research to investigate exercise quality in terms of type, intensity, and duration in addition to exercise frequency, which was identified as the most influential factor for blood glucose in this study, is suggested to determine the effects of optimized exercise on blood glucose levels.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - KJY and LKH.
Data collection - KJY.
Analysis and interpretation of the data - KJY and LKH.
Drafting and critical revision of the manuscript - KJY and LKH.
This article is based on a part of the first author's master's thesis from Keimyung University.
This article was supported by the Keimyung University Dongsan Medical Center Research Funds (No.2021-003) in 2021.
 E-SUBMISSION
E-SUBMISSION