
Purpose
This study identified and compared the pain and associated symptoms of stable coronary artery diseases and acute coronary syndrome.
Methods
The study participants comprised 180 patients with stable coronary artery diseases and acute coronary syndrome. The data were collected from August 25, 2020, to October 30, 2020.
Results
We found that 77.2% of participants had pain and associated symptoms, and 85.6% had one or more associated symptoms. In the associated symptoms, patients with acute coronary syndrome expressed squeezing, and patients with stable coronary artery diseases expressed expanding. Patients with stable coronary artery diseases reported increased pain during exercise. Moreover, although there was no statistically significant difference, drinking, eating, and cold weather often exacerbated pain in patients with acute coronary syndrome.
The average pain intensity of patients with stable coronary artery diseases was moderate (4.09±2.79). The average pain intensity of acute coronary syndrome patients was severe (5.68±3.34). Patients with acute coronary syndrome mainly reported cold sweat and loss of consciousness. Palpitations and dizziness were prevalent complaints in patients with stable coronary artery diseases.
Conclusion
Based on this study's results, a nursing assessment can be performed when managing patients with coronary artery disease. In addition, a nursing assessment protocol could be developed based on the analysis results regarding pain and associated symptoms in patients with stable coronary artery diseases and acute coronary syndrome.
This study identified and compared the pain and associated symptoms of stable coronary artery diseases and acute coronary syndrome.
The study participants comprised 180 patients with stable coronary artery diseases and acute coronary syndrome. The data were collected from August 25, 2020, to October 30, 2020.
We found that 77.2% of participants had pain and associated symptoms, and 85.6% had one or more associated symptoms. In the associated symptoms, patients with acute coronary syndrome expressed squeezing, and patients with stable coronary artery diseases expressed expanding. Patients with stable coronary artery diseases reported increased pain during exercise. Moreover, although there was no statistically significant difference, drinking, eating, and cold weather often exacerbated pain in patients with acute coronary syndrome. The average pain intensity of patients with stable coronary artery diseases was moderate (4.09±2.79). The average pain intensity of acute coronary syndrome patients was severe (5.68±3.34). Patients with acute coronary syndrome mainly reported cold sweat and loss of consciousness. Palpitations and dizziness were prevalent complaints in patients with stable coronary artery diseases.
Based on this study's results, a nursing assessment can be performed when managing patients with coronary artery disease. In addition, a nursing assessment protocol could be developed based on the analysis results regarding pain and associated symptoms in patients with stable coronary artery diseases and acute coronary syndrome.
Coronary Artery Disease (CAD) is a condition caused by atherosclerotic plaque buildup in the wall of the coronary arteries in the epicardium. It causes the lumen of the coronary arteries to narrow and obstructs blood flow to the heart, resulting in difficulty supplying oxygen and nutrients to the heart [1]. Stable Coronary Artery Disease (SCAD) and Acute Coronary Syndromes (ACS) are subcategories of CAD [2, 3]. SCAD is a symptom of myocardial ischemia caused by insufficient blood supply to the coronary arteries [4] and includes stable angina, variant angina, asymptomatic ischemia, and microvascular angina [5]. ACS is a generic term for acute cardiac events caused by a sudden blockage of blood supply to the myocardium [6]. It includes unstable angina, ST-segment Elevation Myocardial Infarction (STEMI), and Non-STsegment Elevation Myocardial Infarction (NSTEMI) [7].
CAD symptoms include chest pain, pressure, and discomfort; fatigue; cold sweat; pain in the back, neck, shoulders, arms, and jaw; confusion; changes in vision; brain fog; dizziness; palpitations; nausea; reflux; anxiety; shortness of breath; and indigestion [8, 9, 10, 11]. Most people know that the main symptom of CAD is chest pain, but only 5.1% of patients who come to the emergency room with chest pain are diagnosed with CAD, and many CAD patients come to the emergency room complaining of symptoms other than chest pain. [12]. Also, chest pain in CAD patients is aggravated by exercise or mental stress, or relieved by rest or nitroglycerin [9].
The 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain (hereinafter, the US AHA/ACC Guideline) [13] describes chest pain as a retrosternal chest discomfort (heaviness, squeezing, pressure, tightness, or burning). It gradually builds in intensity (over several minutes) and is provoked by physical exertion or emotional stress. Symptoms associated with myocardial ischemia presented in the guideline include dyspnea, palpitations, diaphoresis, dizziness, syncope, pre-syncope, upper abdominal pain, heartburn not related to meals, and nausea or vomiting. The guideline also defines chest pain occurring at rest or with minimal exertion as ACS [13].
According to recent studies on CAD-related pain and associated symptoms, 92.9% of patients with Ischemia with No Obstructive Coronary Artery disease (INOCA) complained of chest pain, pressure, and discomfort without any obstruction in the coronary arteries [8]. Patients with angina complain of moderate pain (60.2%) for at least five minutes (53.8%) approximately five times a week [14]. Patients with diabetes have a high risk of developing CAD [2], often complaining of discomfort in the neck or abdomen [13]. Women diagnosed with CAD typically complain of nonspecific symptoms [3, 7, 9, 10, 11, 12, 13, 14]. There are also studies on associated symptoms other than chest pain in CAD patients [8, 12], and the US AHA/ACC Guideline [13] presents a compendium of symptoms associated with angina. However, previous studies have mostly focused on specific CAD conditions such as angina [14], INOCA [8], or acute myocardial infarction [10]. Other studies investigated CAD symptoms without considering its subcategories [13]. These studies mainly aimed to differentiate between cardiac and non-cardiac chest pain among patients who present to the emergency room with chest pain [12]. However, ACS is an emergency requiring rapid nursing assessment and intervention [13] due to the sudden occlusion of coronary arteries [6] compared to SCAD. Thus, it is beneficial to quickly assess patients with chest pain based on their respective pain and associated symptoms.
Therefore, this study was conducted to identify and compare the pain and associated symptoms of SCAD and ACS. This study aimed to provide theoretical evidence for quickly assessing and addressing the nursing needs of CAD patients, providing optimal nursing care, and preventing progression to severe outcomes with pain. Based on the study results, nurses can provide evidence-based nursing care to CAD patients in clinical settings. The study findings can also be used as basic data for training nursing students and nurses to rapidly assess pain and associated symptoms.
This study is a comparative study conducted to identify and compare the pain and associated symptoms of SCAD and ACS.
A total of 180 participants, 90 with SCAD and 90 with ACS, were recruited by nonrandom sampling. The target population was patients diagnosed with ischemic heart disease who received coronary angiography at the cardiology outpatient clinic of a tertiary hospital. The inclusion criteria were adults (≥18 years) who could communicate and express their pain and associated symptoms, understood the purpose of the study, and voluntarily signed written informed consent.
The exclusion criteria were: (i) diagnosis of other heart diseases such as aortic stenosis, aortic regurgitation, hypertrophic cardiomyopathy, systemic arterial hypertension, pericarditis, aortic dissection, and mitral valve prolapse; (ii) history of other conditions associated with chest pain aggravated by respiration and coughing, including respiratory system diseases such as pleurisy, pneumothorax, pneumonia, tuberculosis, bronchitis, pleuritis, and pulmonary embolism; (iii) digestive system diseases such as reflux esophagitis, enteritis, esophageal spasm, peptic ulcer, gastritis, and acute pancreatitis; (iv) viral diseases such as herpes zoster, skin diseases, and Coronavirus Disease 2019 (COVID-19); (v) musculoskeletal disorders such as chest muscle pain accompanied by swelling or bruising, costochondritis, dislocation due to trauma, and thoracic outlet syndrome; and (vi) neurological and psychiatric abnormalities such as panic or anxiety disorder.
The minimum required sample size was obtained using Cohen's formula [15] and G*Power Program 3.1.9.1. We intended to conduct an independent t-test to compare pain and associated symptoms between the SCAD and ACS groups. Thus, a related previous study [16] was consulted to derive the appropriate sample size. However, applying the same effect size to this study was unsuitable. Therefore, a pilot study was conducted with several SCAD and ACS patients (5 for each group) for a week (June 22-28, 2020) in the cardiology ward of a tertiary hospital, and their pain and associated symptoms were investigated. A medium effect size of 0.50 was selected based on the mean and standard deviation for the t-test of the pilot study. Therefore, assuming an effect size (d) of 0.50, a significance level (α) of .05, and a power (1-β) of .95, the minimum required sample size was calculated at 176. There was little or no heterogeneity among the pilot study participants recruited for this study and all of them were cooperative in responding to the survey items without any coercion. Thus, a low dropout rate of 3% was considered, and 182 questionnaires were distributed to the SCAD and ACS groups (91 each). After excluding two incomplete questionnaires (one from each group), the data collected from 180 respondents were included for analysis.
Data collection was performed after obtaining approval from the Institutional Review Board (IRB) of the survey site (IRB No. 1040173-202008-HR-027-02) and permission for cooperation from the cardiology department and nursing department of the general hospital. After explaining the purpose of the study to the respondents and obtaining the signed Informed Consent Form (ICF) from each who agreed to participate, we distributed the structured questionnaire. Before conducting the survey, the participants were informed that they could withdraw from the study at any time, and that the collected data would be used for research purposes only. If consent was withdrawn during the survey, the ICF and questionnaire were immediately disposed of.
To collect data on the participants' pain and associated symptoms, a survey form was developed based on a prior study and the pilot study. Pain was assessed using the PQRST model [17] with five assessment criteria: P (palliative factors/provocative factors), Q (quality), R (radiation), S (severity), and T (temporal factors). Associated symptoms were assessed using the items confirmed in the aforementioned previous study and our pilot study. All items related to pain and associated symptoms were formulated with the agreement and confirmation by an expert panel consisting of one cardiovascular research nurse, two cardiovascular specialists, and one adult nursing professor.
Factors relieving and aggravating pain were derived from previous research and the pilot survey.
A total of nine relieving factors were collected by deriving four factors (resting, sleeping, nitroglycerin, and morphine) from a previous study [13], and an additional four factors (massage, water intake, deep breathing, and vomiting) and the "others" category from our pilot survey. The "others" category consists of the factors described by the respondents in an open-ended question.
A total of nine aggravating factors were collected by deriving eight factors (exercise, stress, smoking, cold weather, alcohol drinking, eating, early morning, and position changes) from previous studies [18, 19, 20] and adding only the "others" category from the pilot study. All other items overlapped with the factors derived from previous studies. The "others" category consists of factors other than the eight that the respondents described in an open-ended question. Multiple selections were allowed.
A total of 14 pain qualities were collected by deriving 12 pain perceptions (burning, sharp, grabbing, squeezing, tightness, contracting, heaviness, pressure, stuffy, aching, dull, and bursting) from previous studies [18, 21, 22]. We added "hitting" from our pilot survey and "others" containing the respondents' descriptions of pain in an openended question not covered by the 13 categories. Multiple selections were allowed.
The location of pain was classified into nine main areas (chest, abdomen, back, loin, shoulder, arm, neck, jaw, and finger) based on previous studies [13, 23, 24, 25]. The chest, abdomen, back, and loin were further divided into three sections (left/mid/right). The shoulder and arm were divided into four sections (right anterior, left anterior, right posterior, and left posterior). The neck was divided into anterior and posterior sections. Jaw and fingers were not subdivided. In total, the location of pain was divided into 24 sections. If the respondents experienced pain in other parts of the body, they were asked to specify it in the "other" category. The chest was defined as the area between the clavicle and the xiphoid bone, and the abdomen as the area below the xiphoid bone and the rib cage. They were divided vertically into three sections: from the left anterior axillary line to the left midclavicular line, between the left and right midclavicular lines, and from the right midclavicular line to the right anterior axillary line. The back and loin were defined as from the seventh cervical vertebra to the scapula's lower edge and from the scapula's lower edge to the posterior iliac crest, respectively. They were divided vertically into three sections: from the right posterior axillary line to the right mid-scapular line, between the right and left mid-scapular lines, and from the left mid-scapular line to the left posterior axillary line. Respondents were allowed to select multiple locations.
The intensity of pain was assessed using the visual analog scale (VAS). Participants were presented with a 10-cm straight line representing a continuum between "no chest pain" (left end) to "worst possible chest pain" (right end). Participants were asked to mark their level of pain intensity on the line.
The duration and interval of pain were assessed in minutes on the questionnaire. If participants were unsure of the exact duration or interval of pain, they were asked to provide their best estimate.
Associated symptoms were categorized into 14 symptoms (fatigue, cold sweats, shortness of breath, dizziness, nausea, palpitation, syncope, abdominal pain, vomiting, headache, indigestion, loss of consciousness, cough, and chills) based on previous studies [18, 22, 23, 26, 27] and the "others" category. The "others" category consisted of symptoms other than the 14 categories the respondents described in an open-ended question. Respondents were allowed to select multiple symptoms.
Data were collected from August 25 to October 30, 2020, from patients with CAD who visited the cardiology outpatient department of a general hospital located in a Korean city. The survey on chest pain and associated symptoms was conducted one week after patients received coronary angiography and had their first outpatient visit. After obtaining written consent, the researcher read the survey questions and recorded the patient's oral responses. Disease-related characteristics were directly written by the researcher on the survey form. If the patient's pain, aggravating and relieving factors, or associated symptoms had multiple descriptions, multiple items were selected. If they did not fit into predefined categories, they were recorded as described by the patient. Pain intensity was recorded by having the patient indicate the level of pain perceived on the VAS line and measuring the length in centimeters. Two cardiologists confirmed associated symptoms before being recorded. As data collection was performed during the COVID-19 pandemic, the researcher wore a KF94 mask and vinyl gloves before meeting with patients to ensure both parties' safety. The utmost precautions for infection prevention were taken through proper hand hygiene and periodic ventilation of the survey area. In addition, hand sanitizer and a face mask were provided to each patient before the survey.
The data collected in this study were analyzed using IBM SPSS Version 26. Descriptive statistics were used for the participants' general and disease-related characteristics. Independent t-test, χ2 test, and Fisher's exact test were used to test the homogeneity of general and disease-related characteristics between the SCAD and ACS groups and differences in pain and associated symptoms.
Table 1 shows the results of general characteristics and homogeneity between the groups.
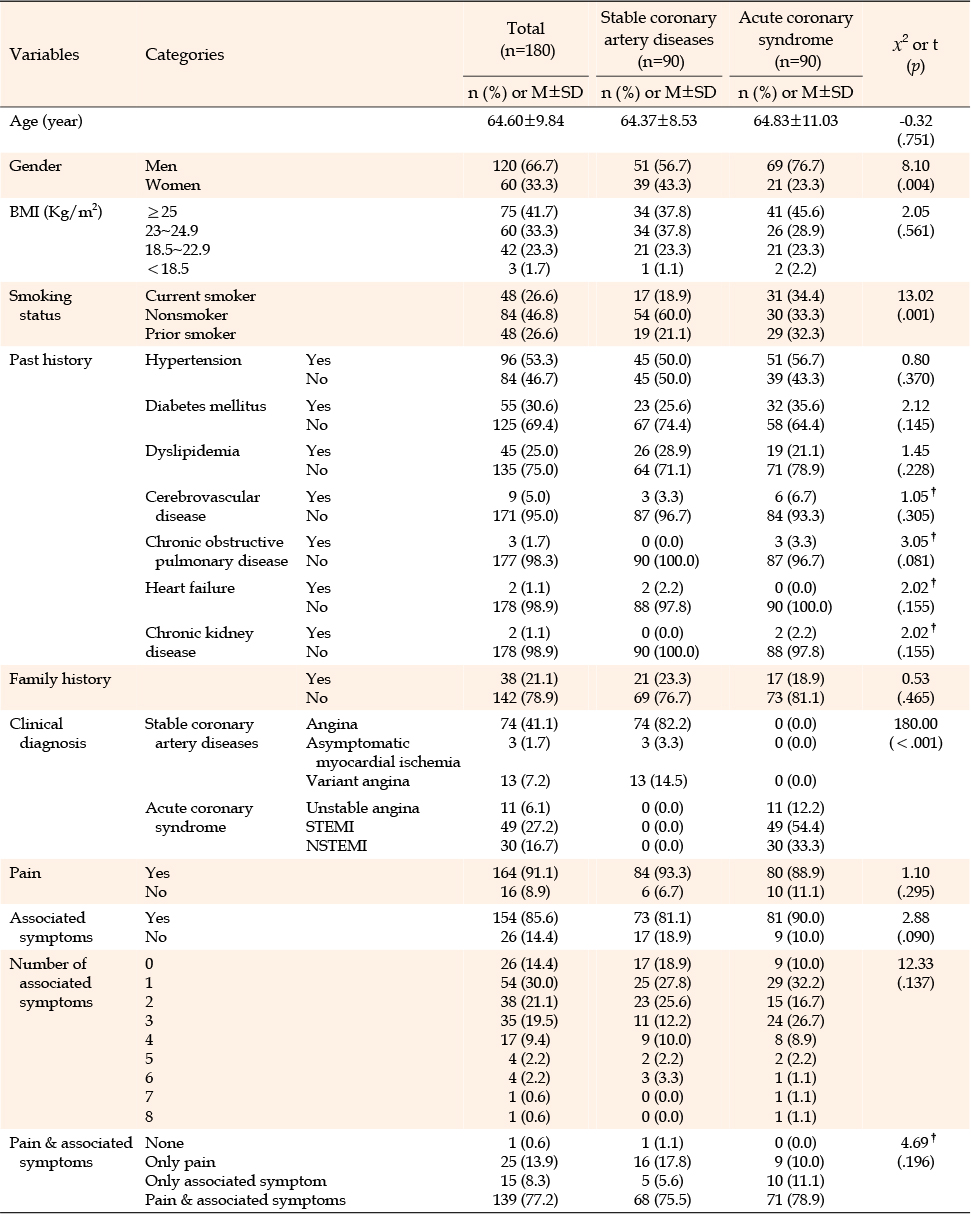
Table 1
General Characteristics and Homogeneity of the Stable Coronary Artery Diseases and Acute Coronary Syndrome Groups (N=180)
The general characteristics are summarized as follows: the mean age was 64.60±9.84 years; 120 (66.7%) were men; 75 (41.7%) were Body Mass Index (BMI) 25≥; 84 (46.8%) were nonsmokers, 48 (26.6%) prior smoker, and 48 (26.6%) current smokers; 96 (53.3%) were diagnosed with hypertension, and 55 (30.6%) with diabetes mellitus; 38 (21.1%) had a family history of cardiovascular disease.
The SCAD and ACS groups were composed as follows: there were 90 cases (50.0%) in each group. In the SCAD group, there were 74 cases (82.2%) of angina, 3 cases (3.3%) of asymptomatic myocardial ischemia, and 13 cases (14.4%) of variant angina. In the ACS group, there were 49 cases (54.4%) of ST-elevation myocardial infarction, 30 cases (33.3%) of non-ST-elevation myocardial infarction, and 11 cases (12.2%) of unstable angina.
Regarding pain and associated symptoms, the following results were obtained: 164 participants (91.1%) complained of pain, 154 (85.6%) had associated symptoms, 139 (77.2%) had both pain and associated symptoms, 25 (13.9%) only pain, 15 (8.3%) only associated symptoms, and 1 (1.6%) neither pain nor associated symptoms. Among those with associated symptoms, 54 (30.0%) had one symptom, 38 (21.1%) had two symptoms, and 35 (19.4%) had three or more symptoms.
Comparing sex between the SCAD and ACS groups, Comparing sex between the SCAD and ACS groups, 51 (56.7%) and 39 (43.3%) in in the SCAD group were men and women, respectively, compared to 69 (76.7%) and 21 (23.3%) in the ACS group. This showed a statistically significant difference (χ2=8.10, p=.004). Comparing smoking status between the SCAD and ACS groups, 54 (60.0%) and 17 (18.9%) in the SCAD group were nonsmokers and current smokers, respectively, compared to 30 (33.3%) and 31 (34.4%) in the ACS group. This showed a statistically significant difference (χ2=13.02, p=.001). No statistically significant differences were observed in age, BMI, past history, family history, pain, and associated symptoms.
Table 2 shows the results of Pain (PQRST) comparison between the SCAD and ACS groups.
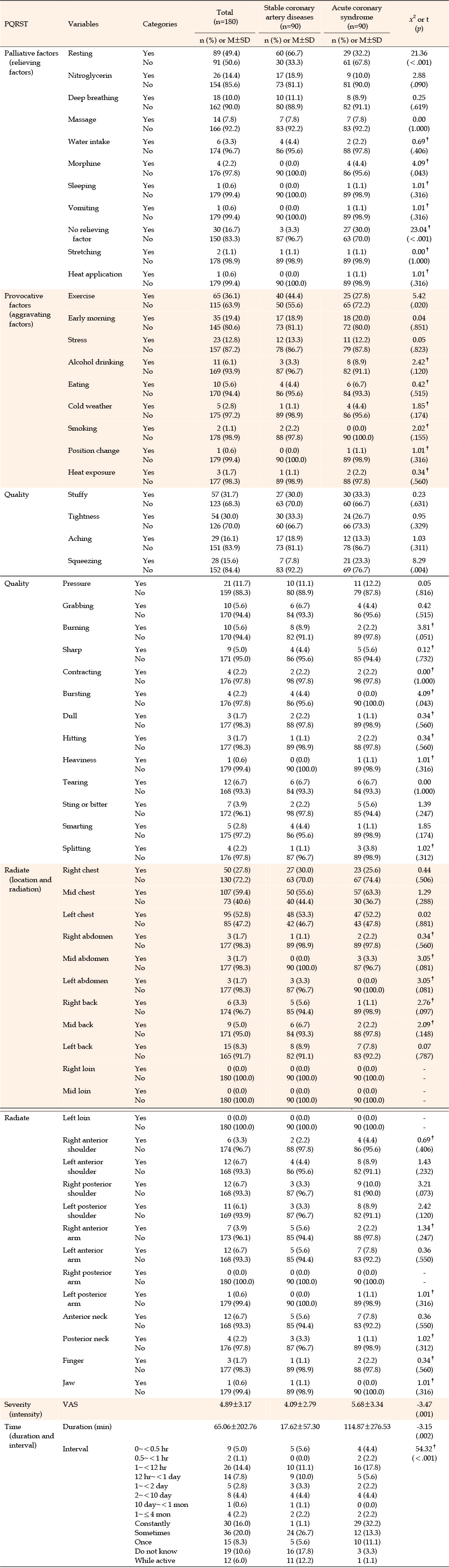
Table 2
Comparison of Pain in Stable Coronary Artery Diseases and Acute Coronary Syndrome (N=180)
The relieving factor of pain in CAD patients was resting (n=89, 49.4%), followed by nitroglycerin (n=26, 14.4%), deep breathing (n=18, 10.0%), and massage (n=14, 7.8%). Broken down by group, the relieving factors was as follows: resting in 60 (66.7%), nitroglycerin in 17 (18.9%), deep breathing in 10 (11.1%), and massage in 7 (7.8%) SCAD patients; resting in 29 (32.21%), nitroglycerin in 9 (10%), deep breathing in 8 (8.9%), and massage in 7 (7.8%) ACS patients. The intergroup difference in the distribution of relieving factors was as follows: in a resting state, pain was relieved more efficiently in SCAD patients (66.7%) than in ACS patients (31.1%) with a statistically significant difference (χ2=22.77, p<.001). To relieve their pain, ACS patients received morphine more frequently than SCAD patients (4.4 vs. 0.0%) with a statistically significant difference (χ2=4.09, p=.043).
The factor with the greatest impact in aggravating pain in CAD patients was exercise (n=65, 36.1%), followed by early morning (35, 19.4%), stress (23, 12.8%), and alcohol drinking (11, 6.1%). Broken down by group, the aggravating factors was exercise in 40 (44.4%), early morning in 17 (18.9%), and stress in 12 (13.3%) SCAD patients, and exercise in 25 (27.8%), early morning in 18 (20%), and stress in 11 (12.2%) ACS patients. The intergroup difference of aggravating factors was as follows: exercise aggravated pain more significantly in SCAD patients (44.4%) than in ACS patients (28.9%) with a statistically significant difference (χ2=5.42, p=.020). Though not statistically significant, alcohol drinking, eating, and exposure to cold weather tended to aggravate pain more severely in ACS patients than in SCAD patients.
The pain qualities frequently described by the CAD patients were "stuffy" (n=57, 31.7%), "tightness" (n=54, 30.0%), "aching" (n=29, 16.1%), "squeezing" (n=28, 15.6%), and "pressure" (n=21, 11.7%). Other descriptions of pain included "tearing" (n=12, 6.7%), "sting or bitter" (n=7, 3.9%), "smarting" (n=5, 2.8%), and "splitting" (n=4, 2.2%).
Broken down by group, the most frequent distribution of pain quality for the SCAD group was "tightness" (n=30, 33.3%), followed by "stuffy" (n=27, 30.0%), "aching" (n=17, 18.9%), and "pressure" (n=10, 11.1%). For the ACS group, the order was "stuffy" (n=30, 33.3%), "tightness" (n=24, 26.7%), "squeezing" (n=21, 23.3%), and "aching" (n=12, 13.3%).
Statistically significant differences were observed in "squeezing" (χ2=8.29, p=.004) with 7 (7.8%) in SCAD and 21 (23.3%) in ACS, and "expanding" (χ2=4.09, p=.043) with 4 (4.4%) in SCAD and 0 (0.0%) in ACS. "Expanding" was reported only in the SCAD group.
The locations of pain reported by the CAD patients were as follows in descending order of frequency: chest (left/mid/right: 52.8%/59.4%/27.8%), back (left/mid/right: 8.3%/5.0%/3.3%), shoulder (left anterior/right anterior/left posterior/right posterior: 6.7%/3.3%/6.1%/6.7%), arm (left anterior/right anterior/left back/right back: 6.7%/3.9%/0.6%/0%), neck (anterior/posterior: 6.7%/2.2%), abdomen (left/mid/right: 1.7%/1.7%/1.7%), fingers (1.7%), jaw (0.6%), and loin (left/mid/right: 0%/0%/0%).
For the SCAD group, the most frequently reported location of pain was the mid-chest (n=50, 55.6%), followed by left chest (n=48, 53.3%), right chest (n=27, 30%), left back (n=8, 8.9%), and mid-back (n=6, 6.7%). For the ACS group, the most frequently reported location was the mid-chest (n=57, 63.3%), followed by left chest (n=47, 52.2%), right chest (n=23, 25.6%), right posterior shoulder (n=9, 10%), left posterior shoulder (n=8, 8.9%), left anterior shoulder (n=8, 8.9%), and anterior neck (n=7, 7.8%).
There were no statistically significant differences in the locations of pain reported by the SCAD and ACS groups.
The mean VAS score of CAD patients was 4.89±3.17. Broken down by group, that of SCAD patients was 4.09±2.79, and ACS patients was 5.68±3.34, indicating a statistically significant difference (t=-3.62, p=.001).
The mean duration of pain reported by CAD patients was 65.06±202.76 minutes. Broken down by group, that of SCAD patients was 17.62±57.30 minutes, and ACS patients was 114.87±276.53 minutes, indicating a statistically significant difference (t=-3.15, p=.002).
The pain interval most frequently reported by the participating CAD patients was "sometimes" (n=36, 20.0%), followed by "constantly" (n=30, 16.0%) and "every 1~<12 hr" (n=26, 14.4%). Broken down by group, that of the SCAD patients was "sometimes" (n=24, 26.7%), followed by "while active" (n=11, 12.2%) and "every 1~<12 hr" (n=10, 11.1%). That of the ACS group was "constantly" (n=29, 32.2%), followed by "every 1~<12 hr" (n=16, 17.8%) and "sometimes" (n=12, 13.3%), indicating a statistically significant difference (χ2=54.32, p<.001).
Table 3 shows the results of comparing the associated symptoms between the SCAD and ACS groups.
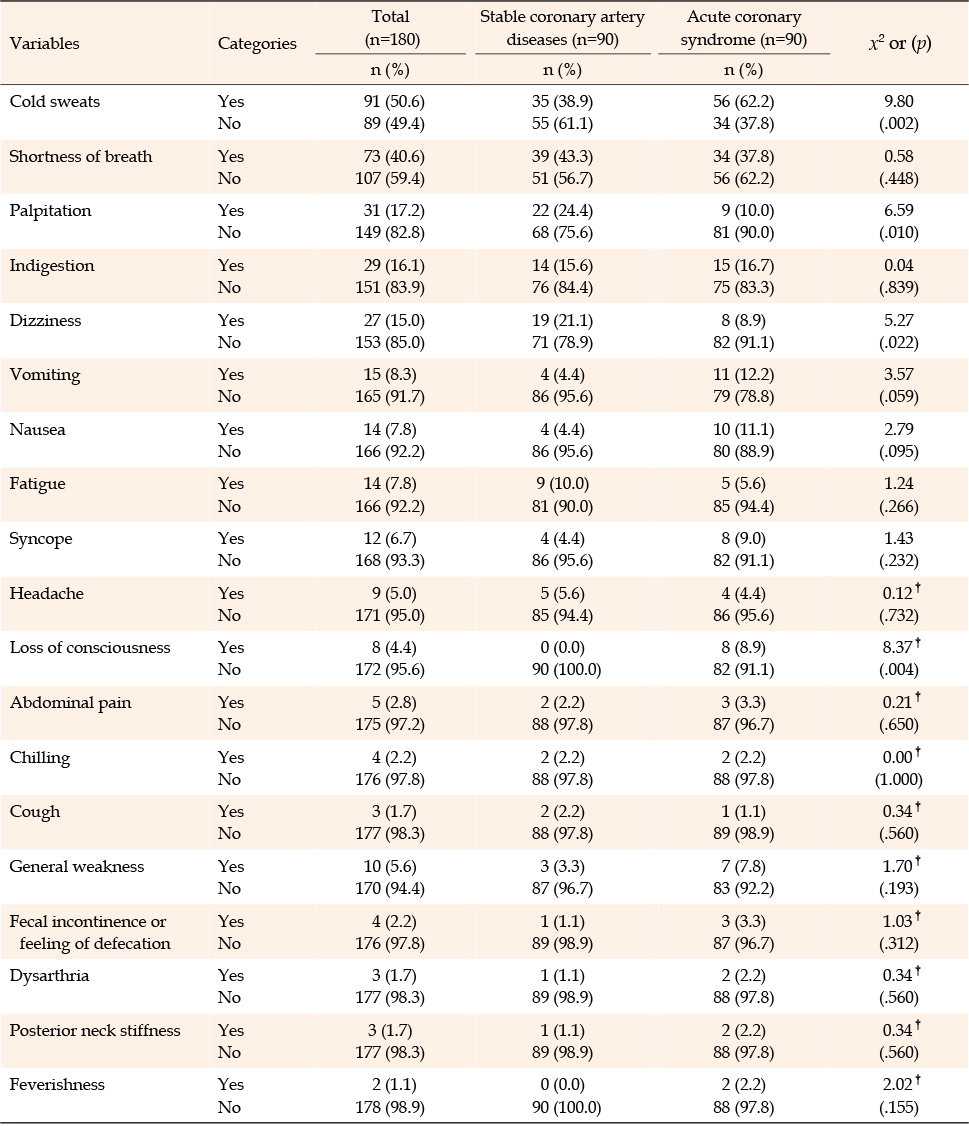
Table 3
Comparison of Associated Symptoms in Stable Coronary Artery Diseases and Acute Coronary Syndrome (N=180)
Regarding associated symptoms, the most frequently reported symptom by the CAD patients was cold sweats (n=91, 50.6%), followed by shortness of breath (n=73, 40.6%), palpitation (n=31, 17.2%), indigestion (n=29, 16.1%), and dizziness (n=27, 16.1%). Other reported symptoms included general weakness (n=10, 5.6%), fecal incontinence or feeling of defecation (n=4, 2.2%), dysarthria (n=3, 1.7%), posterior neck stiffness (n=3, 1.7%), and feverishness (n=2, 1.1%). Additionally, changes in voice, feeling of paralysis, feeling of bulging eyeballs, and paleness were also reported (n=1 each).
The associated symptoms reported by the SCAD group included shortness of breath (n=39, 43.3%), cold sweats (n=35, 38.9%), palpitation (n=22, 24.4%), dizziness (n=19, 21.1%), and indigestion (n=14, 15.6%). Those reported by the ACS group included cold sweats (n=56, 62.2%), shortness of breath (n=34, 37.8%), indigestion (n=15, 16.7%), vomiting (n=11, 12.2%), and nausea (n=10, 11.1%). Cold sweats and loss of consciousness were reported significantly more frequently in the ACS group than in the SCAD group (62.2% vs. 38.9% [χ2=9.80, p=.002] and 7.8% vs. 0% [χ2=8.37, p=.004], respectively). Palpitation and dizziness were reported significantly more frequently in the SCAD group than in the ACS group (24.4% vs. 10.0% [χ2=6.59, p=.010] and 21.1% vs. 8.9% [χ2=5.27, p=.022], respectively).
This study was conducted as a comparative study to identify and compare the pain and associated symptoms of SCAD and ACS patients to provide scientific evidence for nursing assessment. CAD is a medical emergency that requires prompt intervention [13], and this study is significant because our findings provide scientific evidence for assessing pain and associated symptoms of CAD patients and applying appropriate measures in various settings, including the home, local community, and healthcare practice.
This study adopted the PQRST (palliative/provocative, quality, radiate, severity, time) method as the pain assessment tool to compare the SCAD and ACS patient groups. In comparing provocative factors (aggravating factors) (provocative factors in PQRST), exercise was the most frequently reported aggravating factor for SCAD groups. Alcohol drinking, eating, and exposure to cold weather were more frequently reported as factors provoking pain in the ACS group than in the SCAD group, albeit without a statistically significant difference. However, SCAD patients were more susceptible to negative effects from exercise, early morning, stress, alcohol drinking, and cold weather. In a UK study, stress (79.8%), exercise (73.4%), and cold weather (59.9%) were reported as triggers for chest pain in patients with INOCA [8]. Although these provocative factors were almost identical to those identified in our study, the proportions of patients who reported them as aggravating factors were lower. This may be because in the UK study on INOCA, the survey was conducted between October and December, which increased the proportion of participants perceiving cold weather as a provoking factor. Conversely, the data collection in our study occurred during the warmer months of August to October.
Regarding pain quality (quality in PQRST), the most frequently reported ones among the SCAD patients were "tightness," "stuffy," and "aching," while those among the ACS patients were "stuffy," "tightness," and "squeezing." The US AHA/ACC Guideline [13] suggests that the anginal symptoms are perceived as retrosternal chest discomfort, such as heaviness, tightness, pressure, contraction, and squeezing, which closely matches the results of our study. "Squeezing" and "expanding" were more commonly reported by ACS and SCAD patients, respectively. In particular, "squeezing" was much more frequently reported by ACS patients compared to SCAD patients. This is consistent with the US AHA/ACC Guideline report that "squeezing" pain is commonly perceived in severe ischemic conditions. However, "expanding" was reported by only SCAD patients in our study; it was not mentioned in the US AHA/ACC Guideline. This suggests that it is important not to overlook detailed pain descriptions during nursing assessments, including those not mentioned in the clinical practice guidelines.
In comparing radiate (location and radiation in PQRST), patients of both the SCAD and ACS groups primarily complained of mid-chest pain, which is consistent with the US AHA/ACC Guideline report [13] that anginal symptoms are perceived as retrosternal chest discomfort. This finding reaffirms that patients with CAD complain more commonly of mid-chest pain than left-chest pain.
Finger pain was also mentioned in the SCAD (1.1%) and ACS (2.2.%) groups, which is similar to the finding of a previous study [23] that finger discomfort was prevalent in 4.3% of patients. This highlights the need to pay attention to finger pain in addition to the typical chest pain that radiates to the left chest, shoulder, arm, or jaw [13].
The mean VAS score for pain intensity (severity in PQRST) was 4.09±2.79 in SCAD patients and 5.68±3.34 in ACS patients. This was lower than the estimate of a Chinese study that 60.2% of patients with angina pectoris experience moderate to severe pain [14]. The US AHA/ACC Guideline states that chest pain may be expressed differently among different races, ethnicities, and cultures, emphasizing the importance of considering the racial, ethnic, and cultural backgrounds of patients [13]. This suggests the research results may reflect the demographic characteristics of the study population, and requires additional research to compare by country or age group.
An intergroup comparison of associated symptoms revealed that palpitation and dizziness were more prevalent in the SCAD group and cold sweats and loss of consciousness in the ACS group. This emphasizes the need for follow-up research to identify specific associated symptoms of CAD that vary depending on the ischemia progression and coronary artery occlusion [13]. The clear differences in SCAD- and ACS-associated symptoms, as demonstrated in this study, can be presented as theoretical evidence for nursing assessment of associated symptoms.
In this study, major ACS-associated symptoms were identified as cold sweats, shortness of breath, indigestion, vomiting, and nausea. This is consistent with the findings of a previous study [23] that examined ACS-associated symptoms in 806 ACS patients and identified weakness, sweating, shortness of breath, fatigue, and dizziness as major ACS-associated symptoms, in decreasing order of frequency. Another study on ACS [28] also found similar clinical manifestations, such as cold sweats and shortness of breath. While cold sweats was reported in similar percentages across the studies, other symptoms showed differences in prevalence rates. While some studies with Chinese patients diagnosed with ACS reported feverishness [27], symptoms such as fecal incontinence or feeling of defecation, dysarthria, bulging eyes, and changes in voice have not been reported in previous studies. Therefore, a systematic literature review of SCAD- and ACS-associated symptoms appears necessary to develop preventative nursing education materials.
Among the general characteristics, a statistically significant difference in gender distribution was observed between the SCAD and ACS groups. Although chest pain is reported as the predominant symptom for both men and women in most studies related to ACS [28], women with typical/atypical angina complain not only of thoracic pain but also of pain in the arm, jaw, and neck [28]. As SCAD has a higher prevalence in women, who tend to present with more associated symptoms, future studies must adjust for gender ratio from the research design stage accordingly.
A statistically significant difference was also observed in smoking status. Smoking is well-known to increase the risk of CAD [13, 29, 30]. However, no research has examined whether smoking history is associated with differences in pain or associated symptoms in CAD patients. In contrast, research on demographic characteristics that may trigger CAD with mild or no pain has focused on risk factors such as race, gender, patients with diabetes, and older adults [13]. Therefore, further research is needed to investigate the impact of smoking history on the pain and associated symptoms of SCAD and ACS.
Among the CAD patients (n=180), 164 (91.1%) reported experiencing pain, which is almost identical to a survey outcome that 92.9% of patients with INOCA reported chest discomfort [8]. As chest pain is a common symptom in most CAD patients, it was reaffirmed as a major issue requiring careful and thorough assessment.
The pain locations reported by CAD patients were chest, back, abdomen, loin, shoulder, arm, neck, finger, and jaw. This is consistent with the locations identified in previous studies [8, 13] that already established the chest, back, shoulder, arm, neck, and jaw as the pain locations in CAD patients. However, this study differs from previous studies [8, 13] as it subdivided the major locations into 24 sectional locations where CAD patients perceive pain and found that no participants had perceived pain in the loin and right posterior arm areas. This finding must be confirmed in follow-up research.
The associated symptoms of CAD patients included cold sweats, shortness of breath, palpitation, indigestion, dizziness, general weakness, fecal incontinence or feeling of defecation, dysarthria, posterior neck stiffness, and feverishness. Other symptoms such as a change in voice, feeling of paralysis, feeling of bulging eyeballs, and paleness were also reported. These symptoms mostly coincide with the results of previous studies [8, 10, 13, 18, 22, 26, 27]. These findings emphasize the significance of conducting a thorough assessment and observation of the various associated symptoms that CAD patients may experience.
Regarding the manifestation of pain and associated symptoms in the participating CAD patients, 77.2% experienced both pain and associated symptoms, 13.9% reported only pain without associated symptoms, 8.3% reported only associated symptoms without pain, and 1.6% reported neither pain nor associated symptoms. Previous research [8] presented the frequency of CAD symptoms as their ratio to the study population, such as chest discomfort (92.9%), fatigue and diaphoresis (87.5%), pain in the back, shoulder, arm, neck, and jaw (81.5%), and shortness of breath (80.6%). This study emphasizes the importance of comprehensively assessing pain and associated symptoms in CAD patients to provide appropriate nursing interventions by correctly understanding their nursing needs.
Of the data on the number of associated symptoms selected by the participants, 70% of the CAD patients in this study experienced two or more associated symptoms along with pain. Identifying these symptoms in advance and incorporating them into nursing education materials could help prevent disease progression in situations requiring prompt nursing interventions. Therefore, conducting a study on the consistent associated symptoms is recommended to further investigate their relationships and better understand the needs of CAD patients.
The limitations of this study are as follows: First, the data was collected from CAD outpatients in one hospital in one region, which may limit the coverage of pain characteristics or associated symptoms, with severe cases or deaths excluded. Second, due to the high average age of the study participants, survey data may not be accurate as they relied on participants' memory to answer the survey questions. Third, if patients had difficulty describing their pain and associated symptoms, some important data may have been excluded. Fourth, the study did not maintain intergroup homogeneity regarding sex and smoking history, which can affect the results regarding pain and associated symptoms. Finally, although the study's sample size was estimated in advance based on the t-test statistic, the pilot survey's sample size was too small, and statistical validity could not be secured in case of a too low frequency of pain and associated symptoms. To overcome these limitations, an appropriate sample size should be determined for research, multisite research across various regions, including emergency room patients, should be conducted, and the homogeneity of participants should be ensured. Additionally, surveys should be conducted during hospital visits immediately after symptom onset.
This study was a comparative study of pain and associated symptoms of SCAD and ACS. There was no difference in pain location between SCAD and ACS patients, but ACS patients described more 'squeezing' pain quality and SCAD patients described more 'expanding' pain quality. The aggravating factor in patients with SCAD was exercise, but drinking, eating, and exposure to cold weather often aggravated pain in patients with ACS. As associated symptoms, cold sweats and loss of consciousness occurred more in ACS patients, and palpitations and dizziness occurred more in SCAD patients. The results of this study can be effectively applied in clinical nursing practice, particularly in situations that require prompt nursing assessment and intervention for CAD patients. Additionally, these results can serve as basic data for providing theoretical evidence-based nursing education to the general public, nursing students, and clinical nurses in various educational settings. Moreover, in the field of research, the analysis results of this study on pain and associated symptoms in CAD patients can serve as the groundwork for developing nursing protocols for CAD patients.
CONFLICTS OF INTEREST:Yoonyyoung Lee has been the Editorial board member of the Korean Journal of Adult Nursing since 2022. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - KIY and LY.
Data collection - KIY and LY.
Analysis and interpretation of the data - KIY and LY.
Drafting and critical revision of the manuscript - KIY and LY.
This article is a revision of the first author's master's thesis from Sunchon National University.
 E-SUBMISSION
E-SUBMISSION