
Purpose
This study was conducted to provide fundamental data for improving the quality of care by investigating the relationships of critical reflection competency, nursing practice environment, job crafting, and person-centered care among tertiary hospital nurses. Additionally, the study sought to identify the factors influencing person-centered care.
Methods: Data were collected from 132 tertiary hospital nurses with at least 1 year of work experience via an online survey conducted in January 2023.
Results: Person-centered care varied significantly according to age, clinical experience, and department. Significant correlations of person-centered care with critical reflection competency (r=.77, p<.001), nursing practice environment (r=.46, p<.001), and job crafting (r=.71, p<.001) were observed. Factors contributing to person-centered care among tertiary hospital nurses included critical reflection competency (β=.46, p<.001) and job crafting (β=.40, p<.001), with an explanatory power of 70.2%.
Conclusion: To provide ethically enhanced person-centered care in tertiary hospitals, various training programs must be developed to strengthen nurses' critical reflection competency and job crafting skills.
This study was conducted to provide fundamental data for improving the quality of care by investigating the relationships of critical reflection competency, nursing practice environment, job crafting, and person-centered care among tertiary hospital nurses. Additionally, the study sought to identify the factors influencing person-centered care.
Data were collected from 132 tertiary hospital nurses with at least 1 year of work experience via an online survey conducted in January 2023.
Person-centered care varied significantly according to age, clinical experience, and department. Significant correlations of person-centered care with critical reflection competency (r=.77, p<.001), nursing practice environment (r=.46, p<.001), and job crafting (r=.71, p<.001) were observed. Factors contributing to person-centered care among tertiary hospital nurses included critical reflection competency (β=.46, p<.001) and job crafting (β=.40, p<.001), with an explanatory power of 70.2%.
To provide ethically enhanced person-centered care in tertiary hospitals, various training programs must be developed to strengthen nurses' critical reflection competency and job crafting skills.
Nursing activities should address the relational and emotional needs of patients and their families, recognizing patients as autonomous individuals and offering personalized care [1]. To achieve this, nurses must shift their perspective on healthcare from provider to patient and deliver person-centered care [2]. This approach emphasizes ethical principles, with nurses respecting the dignity and autonomy of their clients while considering their preferences and lifestyles. Patients who receive person-centered care experience positive outcomes, including reduced feelings of helplessness and depression, shorter hospital stays, and lower healthcare costs [3, 4]. However, in tertiary hospitals, which primarily focus on diagnosing and treating diseases, limitations exist in providing personalized care due to the need to address the issues of many patients within a limited timeframe [4]. According to the theory of McCormack and McCance, the provision of person-centered care by nurses is closely related to their competencies and working conditions [5]. Therefore, it is necessary to examine the relationships among nurses' provision of person-centered care in tertiary hospitals, their working conditions, and their competencies.
Nurses in tertiary hospitals in Korea must exercise prompt and accurate judgment based on critical reflection and skilled nursing interventions, as they provide advanced medical care to patients with severe illnesses, rare diseases, and high rates of complications [6]. In the nursing practice environment, critical reflection is a process in which problems are identified and evaluated by connecting existing knowledge and previous experiences, ultimately restructuring the problem. This process leads to the suggestion of alternative solutions and changes in knowledge and behavior [7]. Since critical thinking in nursing students enhances their person-centered care competencies [8] and self-reflection is known to positively impact the formation of caring relationships with patients [9], a correlation appears to exist between nurses' critical reflection competency and person-centered care.
Moreover, higher levels of job crafting, which involves actively adapting one's interests and preferences within a job, can lead to increased evidence-based practice competencies among nurses [10] and more effective patient care [11]. For nurses, job crafting is a positive activity in which they comprehend their assigned tasks based on their abilities and preferences, then restructure their responsibilities to align with their competencies. Nurses with strong job crafting skills can view themselves as professionals who take pride in saving patients' lives and improving the well-being of others [12]. As a result, job crafting among nurses is anticipated to influence the provision of care administered in consideration of patient interests and preferences. However, research on the relationship between job crafting and person-centered care among nurses in tertiary hospitals remains limited.
In addition to healthcare providers' competencies, organizational and environmental factors are crucial precursors for person-centered care [5]. It is essential to consider the nursing practice environment, which includes not only the physical hospital setting as perceived by nurses, but also organizational policies involving nurses, collaboration with the healthcare team, and the managerial skills of nurse managers [13]. Previous research has demonstrated that a positive perception of the nursing practice environment by nurses is related to the delivery of person-centered care [14, 15]. Furthermore, hospitals with stable employment situations and high institutional evaluation ratings have been found to exhibit high nursing quality [16]. Consequently, it is necessary to investigate the nursing practice environment as perceived by nurses in tertiary hospitals and to examine its relationship with person-centered care.
Previous research on person-centered care has primarily focused on nurses in nursing homes or general hospitals [17]. Few comprehensive studies have been conducted to investigate the relationships between critical reflection competency, nursing practice environment, job crafting, and person-centered care among nurses in tertiary hospitals. Consequently, this study was designed to explore critical reflection competency, nursing practice environment, and job crafting, as well as their associations with person-centered care, among nurses in tertiary hospitals. This information will serve as a foundation for identifying strategies to improve the quality of care.
The purpose of this study was to explore factors that impact person-centered care among nurses. Specifically, the objectives were: 1) to evaluate the levels of critical reflection competency, nursing practice environment, job crafting, and person-centered care; 2) to ascertain the differences in person-centered care based on general characteristics; 3) to investigate the relationships among critical reflection competency, nursing practice environment, job crafting, and person-centered care; and 4) to identify factors that influence person-centered care.
This descriptive study aimed to determine the impact of critical reflection competency, nursing practice environment, and job crafting on person-centered care among nurses in a tertiary hospital.
The participants in this study were nurses who had been working in tertiary hospitals for more than 1 year. Newly graduated nurses with less than 1 year of work experience were excluded from the study due to their potential difficulties in performing person-centered care, which emphasizes an ethical perspective on patient care, because of potential pressures and stresses experienced in a new hospital environment [18]. Nurse managers who do not directly engage in nursing activities, such as chief nurses or those in surgical rooms or outpatient departments who do not provide continuous nursing care to patients for more than 1 day during their hospitalization, were also excluded from the study. G*Power 3.1.9.4 (University of Düsseldorf, Düsseldorf, Germany) was used to calculate the sample size. Based on the effect size of 0.15 between nursing practice environment and person-centered care found in a previous study [14], with 10 predictors (gender, age, marital status, department of work, educational background, work experience, critical reflection competency, nursing practice environment, job crafting, and person-centered care) and applying a significance level of .05 and a power of .80 for regression analysis, the required sample size was determined to be 118. Considering a 10% dropout rate, a total of 132 participants were targeted. The online survey was set to automatically end when 132 responses were completed, and 4 incomplete responses with a significant number of missing items or premature termination during the survey were excluded, resulting in 128 responses (97.0%) used in the final analysis.
All survey items utilized in this study were employed with approval from the original developers and translators. General characteristics, including age, gender, educational background, marital status, work department, and work experience, were examined.
Critical reflection competency was evaluated using the instrument created by Shin et al. [7] specifically for clinical nurses. This tool comprises 19 items, with each item measured on a 5-point Likert scale, resulting in a possible minimum score of 19 and a maximum score of 95. A higher score signifies a greater degree of critical reflection competency. In research by Shin et al. [7], the tool's reliability was found to be indicated by a Cronbach's α of .85, while in the present study, Cronbach's α was .94.
The nursing practice environment was evaluated using the Korean version of the Nursing Practice Environment Tool, originally developed by Lake [13] and later modified and validated by Cho et al. [19]. This tool comprises 29 items, divided into five categories: nine items for nursing foundations for quality of care; four items for staffing and resource adequacy; four items for nurse manager ability, leadership, and support of nurses; nine items for nurse participation in hospital affairs; and three items for collegial nurse-physician relations. Each item is measured using a 4-point Likert scale, with scores ranging from a minimum of 29 to a maximum of 116. A higher score signifies a more favorable assessment of the nurses' working environment. The tool's reliability at the time of development was indicated by Cronbach's α of .83, while in the study by Cho et al. [19], Cronbach's α was .93. In the present study, the reliability was indicated by a Cronbach's α of .95.
Job crafting was evaluated using a 13-item instrument created by Slemp and Vella-Brodrick [20], which was adapted and modified for Korean nurses by Kwon and Kang [21]. This instrument comprises three items for task crafting, five items for relational crafting, and five items for cognitive crafting. Each item is scored on a 6-point Likert scale, with a potential minimum score of 13 and a maximum score of 78. A higher score signifies that organizational members modify their assigned tasks to better align with their individual abilities. The reliability of the instrument in Kwon and Kang's [21] study was indicated by a Cronbach's α of .92, while in this study, Cronbach's α was .94.
To assess the nursing activities related to person-centered care provided by nurses, we utilized the 16-item process of person-centered care from the instrument developed by Slater et al. [22], which was later modified and validated by Kim and Tak [23] to reflect the context of Korean nurses. In line with the person-centered care theory, the outcomes of such care stem from nursing activities carried out by nurses [24]. Consequently, in this study, we employed the items associated with the process of person-centered care, representing the associated nursing activities. The instrument comprises four items addressing patient beliefs and values, three items for shared decision-making, six items for empathetic presence and engagement, and three items for holistic care. Each item is measured using a 5-point Likert scale, with a minimum possible score of 16 and a maximum score of 80. A higher score signifies that nurses deliver patient-centered care, considering patient preferences. In a study by Bing-Jonsson et al. [25], the reliability of this instrument was indicated by a Cronbach's α of .89, while Kim and Tak [23] found a Cronbach's α of .91. In the present study, the reliability was indicated by a Cronbach's α of .92.
Data were collected via an online survey carried out from January 26 to January 28, 2023. Recruitment notices and survey links were posted on online nursing communities (e.g., nursing employment community and nursing graduate programs) to encourage the voluntary participation of registered nurses working in tertiary hospitals. The survey was conducted using software provided through a portal site, and the recruitment notices and survey access were restricted once the required number of responses for the study was reached. Duplicate participation in the study was prevented using the contact information collected from participants for the purpose of providing incentives.
To protect the ethical rights of the participants, this study was conducted after obtaining approval from the institutional review board (IRB: ewha-202301-0004-01) associated with the researcher's institution. Given the use of online data collection methods through remote interactions, an exemption from obtaining written consent forms was granted. Before beginning the survey, a document containing a description of the research and instructions was provided, allowing participants to take part in the survey after reading and adequately understanding the information and providing informed consent. The research explanation document included information about the study, research procedures, compensation for participation, provision and protection of personal information, and an option to withdraw consent. Contact information for the research coordinator and the ethics committee was also provided in case participants had questions or concerns. The collected data were anonymized through encoding and stored on a locked laptop belonging to the researcher, which will be permanently deleted 3 years after the study's completion. Personal identifiers, such as contact information collected for compensation purposes, were immediately and permanently deleted after providing incentives, after which the data were analyzed.
The collected data were analyzed using IBM SPSS 29.0 (IBM Corp., Armonk, NY, USA), using the specific methods outlined below. The general characteristics of the participants were analyzed using frequencies and percentages, while the levels of critical reflection competency, nursing practice environment, job crafting, and person-centered care were assessed by calculating the means and standard deviations. To analyze differences in person-centered care according to general characteristics, the independent t-test and one-way analysis of variance were employed with a significance level of .05, and post hoc testing was conducted using the Scheffé test. The correlations among critical reflection competency, nursing practice environment, job crafting, and person-centered care were examined using Pearson correlation coefficients. Hierarchical regression was utilized to investigate the factors influencing person-centered care and to identify the impact of general characteristics and key independent variables.
The study included 128 participants, with an average age of 30.93 years. Of these, 109 (85.2%) had completed a bachelor degree or higher, 106 (82.8%) were women, and 79 (61.7%) were unmarried. The largest proportion of participants worked in internal medicine wards, with 52 (40.6%) individuals, followed by surgical wards, with 50 (39.0%) individuals, and intensive care units and integrated nursing care wards, with 13 (10.2%) individuals each. A total of 57 (44.5%) participants had work experience ranging from more than 3 years to less than 5 years (Table 1).
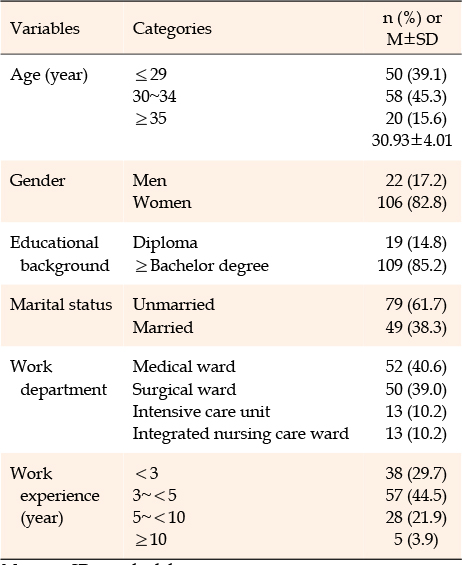
Table 1
General Characteristics of Participants (N=128)
The participants' levels of critical reflection competency, nursing practice environment, job crafting, and person-centered care were as follows. The average score for critical reflection competency was 3.69±0.60, for nursing practice environment it was 2.93±0.49, for job crafting it was 3.66±0.86, and for person-centered care it was 3.65±0.58. The absolute values of skewness for each variable were less than 3 and the absolute values of kurtosis were less than 10, confirming normality (Table 2).

Table 2
Descriptive Statistics and Normality of Variables (N=128)
Significant differences in person-centered care were observed based on age, work department, and work experience. Post hoc test results for age revealed that the group aged 35 years and above demonstrated a higher level of person-centered care relative to the groups aged 29 years and below and 30 to 34 years (F=4.21, p=.017). Post hoc test results by department showed that working in the intensive care unit was associated with significantly higher person-centered care than working in the integrated nursing care ward (F=3.19, p=.026). Additionally, post hoc test results based on work experience (F=3.98, p=.010) indicated that the group with over 10 years of experience displayed a higher level of person-centered care compared to the group with less than 3 years of experience and the group with over 3 years but less than 5 years of experience (Table 3).
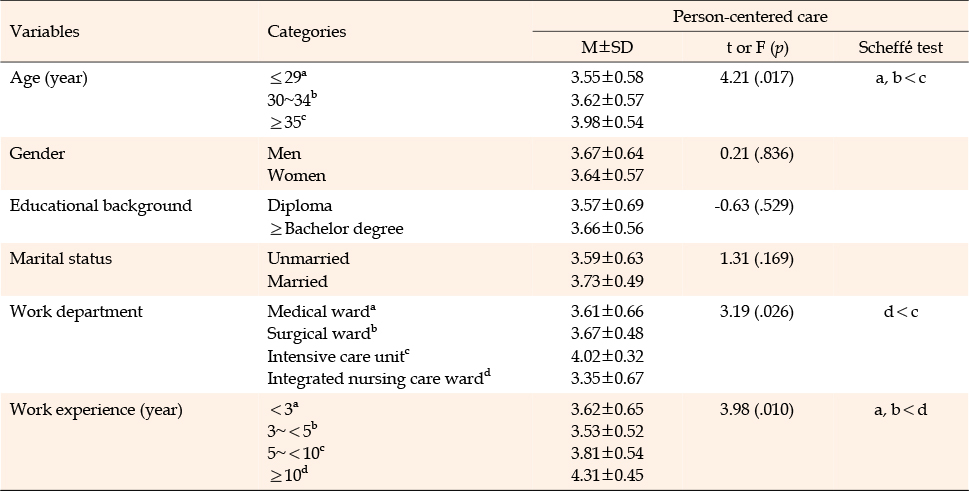
Table 3
Differences in Person-Centered Care According to General Characteristics (N=128)
The participants' critical reflection competency demonstrated positive correlations with the nursing practice environment (r=.39, p<.001), job crafting (r=.59, p<.001), and person-centered care (r=.77, p<.001). Additionally, the nursing practice environment exhibited a positive correlation with both job crafting (r=.50, p<.001) and person-centered care (r=.46, p<.001). Furthermore, job crafting was positively correlated with person-centered care (r=.71, p<.001) (Table 4).
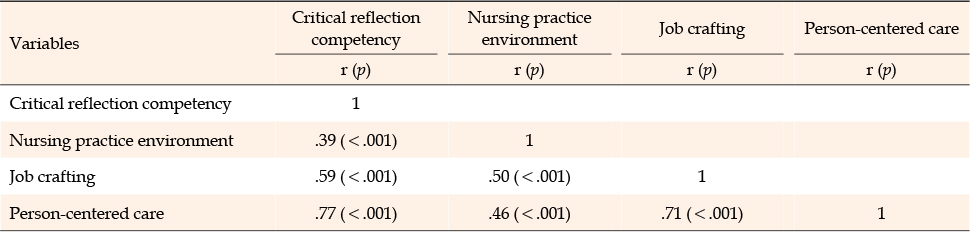
Table 4
Correlations among Critical Reflection Competency, Nursing Practice Environment, Job Crafting, and Person-Centered Care (N=128)
To ensure the independence of the residuals and satisfy the basic assumptions for multiple regression analysis, the Durbin-Watson test was performed; this yielded a value of 2.41, confirming independence. The variance inflation factors were below 10, signifying the absence of multicollinearity in this study. To investigate the impact of independent variables, excluding general characteristics, age, and work department as dummy variables, work experience was established as a control variable in the first step. This revealed statistically significant differences in person-centered care. Subsequently, critical reflection competency, nursing practice environment, and job crafting, which exhibited statistically significant correlations with person-centered care, were sequentially incorporated in the second step of the analysis (Table 5).
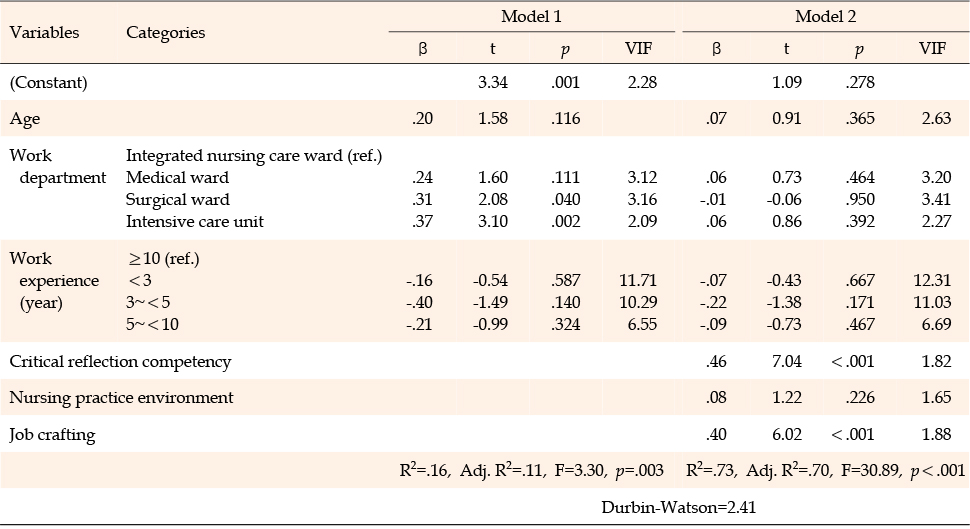
Table 5
Factors Affecting Person-Centered Care (N=128)
When general characteristics such as age, work department, and work experience were included (Model 1), the explanatory power was 11.3% (F=3.30, p=.003). The inclusion of critical reflection competency, nursing practice environment, and job crafting (Model 2) increased the explanatory power to 70.2% (F=30.89, p<.001). The factors influencing person-centered care identified in this study were critical reflection ability (β=.46, p<.001) and job crafting (β=.40, p<.001). Among these, critical reflection competency had the greatest impact on person-centered care for the participants. This suggests that as nurses' critical reflection competency increases and they effectively transform their job to adapt and reconstruct as their own through job crafting, they are more likely to provide high-quality person-centered care to patients.
This study was conducted to analyze the relationships between critical reflection competency, nursing practice environment, job crafting, and person-centered care, as well as to identify factors influencing person-centered care. The goal was to provide foundational data for improving the quality of care provided by nurses working in tertiary hospitals. The average score of person-centered care among the participants in this study was 3.65 out of 5, which was slightly lower than the scores of 3.94 to 3.98 reported in previous studies that used the same tool [14, 26]. Among the participants in this study, only 3.9% had more than 10 years of work experience, whereas previous studies reported a range of 50% to 66.6% [14, 26]. Considering the findings that nurses with longer work experience provide higher-quality person-centered care to patients [27], the difference may be attributed to variations in work experience. Since person-centered care emphasizes ethical care that respects patients' beliefs, lifestyles, and free will [3], nurses need not only proficient clinical skills but also empathy and communication skills [5, 17] to deliver accurate information to patients and establish tailored treatment processes. As nurses gain more experience in the field, their familiarity with their work increases, enhancing their ability to focus on patients [27]. Strategies to encourage long-term retention of nurses are necessary because their ability to empathize with patients' emotions and communicate effectively improves with increased patient interactions, enabling them to provide high-quality care [5]. As the size of a hospital increases, the severity of patients' conditions tends to be higher, and the workload of nurses increases. Consequently, job satisfaction among nurses decreases, leading to a higher turnover rate [28]. Therefore, it is necessary to implement strategies focused on improving the hospital working environment, securing skilled nursing personnel, and enhancing the necessary abilities for person-centered care, such as empathy and communication.
Regarding general characteristics, the results demonstrated that individuals aged 35 years and above exhibited significantly higher levels of person-centered care compared to their younger counterparts, aligning with previous studies [14]. This study's findings corroborate the notion that older nurses generally possess superior interpersonal relationship skills, including communication abilities and empathy [26]. Notably, empathy has been identified as a crucial factor influencing the provision of person-centered care [14]. In contrast, a significant difference was observed between intensive care unit nurses and those in the integrated nursing care ward, with the latter displaying a lower level of person-centered care. Considering study results indicating that nurses in the integrated nursing care ward experience heightened work stress and burnout compared to those in general wards [29], it is essential to provide support to alleviate their job stress. In these the integrated nursing care ward, nursing services are delivered by nurses and auxiliary staff without the presence of family caregivers, encompassing a wide and ambiguous range of nursing tasks such as personal hygiene, elimination, and meal assistance, in addition to diverse patient care demands. The implementation of person-centered care education programs for nurses has been demonstrated to increase awareness of person-centered care and enhance self-perception, interpersonal relationship skills, peer support, and job satisfaction among nurses [30]. As such, continuing efforts are necessary to improve nurses' self-perception, empathy, and communication skills, which are vital for person-centered care. This can be achieved through person-centered care education programs tailored to the characteristics of each department, not only in integrated nursing care wards but also in other departments.
In this study, the factors influencing person-centered care were identified as critical reflection competency and job crafting, with critical reflection competency being the most important factor. This finding aligns with previous research by Do et al. [8], which determined that critical thinking disposition is a major factor influencing person-centered care competence among nursing students. These results highlight the necessity for various training programs to enhance critical reflection competency among nurses. When critical reflection training was provided to novice nurses, it was found to improve critical thinking and communication skills as well as increase confidence in job performance [31]. By offering continuous critical reflection training at both school and hospital levels, nurses' competence can be improved, ultimately leading to better person-centered care for patients and positively impacting clinical outcomes. In contrast, job crafting emerged as the second factor influencing person-centered care, which is consistent with previous research demonstrating the impact of job crafting on care quality [12]. According to prior studies, grit, which is attained through persistent efforts to achieve long-term goals [11], and supportive leadership from managers are factors that enhance job crafting among nurses [10]. Consequently, training programs aimed at increasing nurses' grit and positive psychological capital at the hospital level, as well as empowering leadership education programs for managers, are necessary. Furthermore, person-centered care can be promoted as nurses in tertiary hospitals increase their job crafting levels, which involves taking an interest in their work, adhering to job regulations, and demonstrating their nursing competence in areas subject to change.
However, although a significant positive correlation was found between the nursing practice environment and person-centered care, it was not identified as a factor influencing person-centered care, which is inconsistent with previous studies [14, 15]. The nursing practice environment can vary based on various factors, such as the tasks performed by nurses and their work units [19]. This discrepancy may be because this study recruited participants from a wide range of regions and hospitals without limiting them to a specific area, meaning that external variables were not perfectly controlled. However, since the work environment holds considerable meaning for nurses and their care-providing activities, further research is needed to confirm the relationship between the nursing practice environment and person-centered care in tertiary hospitals, taking into account factors such as the size of the institution and nurse staffing levels.
In this study, we discovered that nurses in tertiary hospitals with higher critical reflection competency, nursing practice environment, and job crafting were more likely to deliver person-centered care. Consequently, it is essential to offer education and resources at the organizational level of hospitals to improve critical reflection competency and job crafting among nurses. Moreover, it is crucial to create person-centered care education programs that take into account the unique characteristics of each department, employing diverse strategies to ensure that nurses respect patients' opinions and provide holistic care that acknowledges their dignity.
This study aimed to investigate the critical reflection competency, nursing practice environment, job crafting, and level of person-centered care among nurses in tertiary hospitals, as well as to determine the relationships between these factors. The results revealed that critical reflection competency and job crafting were factors influencing person-centered care among nurses in tertiary general hospitals. Based on these findings, it was confirmed that educational programs are necessary not only to improve person-centered care among nurses in tertiary hospitals but also to enhance their critical reflection competency and job crafting.
Most participants in this study had less than 10 years of work experience. Therefore, we recommend that future research includes enough nurses with over 10 years of experience for comparison and analysis, as work experience is known to be a significant factor in person-centered care. Additionally, this study did not limit participant recruitment to specific regions or hospital sizes, resulting in limitations in identifying the influence of the nursing practice environment. Consequently, we suggest conducting another study that controls for external variables related to the hospital environment. Finally, further research should focus on nurses working in the nursing care integrated service unit of tertiary hospitals, as their level of person-centered care had the lowest score among departments.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - HJ and SS.
Data collection - HJ.
Analysis and interpretation of the data - HJ and SS.
Drafting and critical revision of the manuscript - HJ and SS.
 E-SUBMISSION
E-SUBMISSION