
Purpose
The aim of this study was to identify factors associated with stress among Korean cancer survivors who are employed.
Methods: A cross-sectional descriptive methodology was applied, and secondary analysis was performed using data from the Korea National Health and Nutrition Examination Survey from 2014 to 2018. A total of 245 employed cancer survivors were included, and data were analyzed using either the χ2 test or the independent t-test, as well as multiple logistic regression analysis.
Results: Four factors were found to be associated with stress among employed cancer survivors: age (Odds Ratio [OR]=0.96, 95% Confidence Interval [CI]=0.94~0.98), gender (with men less likely to be stressed; OR=0.46, 95% CI=0.23~0.91), self-rated health status (OR=1.44, 95% CI=1.03~2.02), and having planned suicide in the previous year (OR=22.98, 95% CI=2.10~251.83).
Conclusion: To facilitate a successful return to work for cancer survivors, it is necessary to develop a stress intervention and/or rehabilitation program that comprehensively considers sociodemographic characteristics, current health status, health behaviors, and mental health.
The aim of this study was to identify factors associated with stress among Korean cancer survivors who are employed.
A cross-sectional descriptive methodology was applied, and secondary analysis was performed using data from the Korea National Health and Nutrition Examination Survey from 2014 to 2018. A total of 245 employed cancer survivors were included, and data were analyzed using either the χ2 test or the independent t-test, as well as multiple logistic regression analysis.
Four factors were found to be associated with stress among employed cancer survivors: age (Odds Ratio [OR]=0.96, 95% Confidence Interval [CI]=0.94~0.98), gender (with men less likely to be stressed; OR=0.46, 95% CI=0.23~0.91), self-rated health status (OR=1.44, 95% CI=1.03~2.02), and having planned suicide in the previous year (OR=22.98, 95% CI=2.10~251.83).
To facilitate a successful return to work for cancer survivors, it is necessary to develop a stress intervention and/or rehabilitation program that comprehensively considers sociodemographic characteristics, current health status, health behaviors, and mental health.
Having an occupation can positively impact cancer survivors not only economically, but also physically and mentally, contributing to an improvement in their Quality of Life (QOL) [1]. Employment can also foster a sense of normalcy and invigorate their zest for life [2]. Furthermore, when survivors Return to Work (RTW), it can help reduce societal costs by promoting labor participation and decreasing the amount of sick leave related to the disease [3].
The physical symptoms of cancer often persist even after treatment has concluded. Furthermore, cancer survivors face numerous challenges during treatment and may experience cognitive impairment and physical fatigue post-treatment. These issues can jeopardize their continued employment and result in additional stress [4, 5]. Survivors may also experience RTW hesitancy due to anxiety about potential recurrence, or they may struggle to continue working even after they have returned [1]. Such stresses can diminish their capacity to manage workplace issues and maintain mental stability, resulting in decreased job satisfaction and QOL [6]. Cancer survivors often endure stress related to mental, physical, and economic hardships, social role confusion, and an elevated risk of mortality [7]. These factors, along with the possibility of recurrence and an unpredictable prognosis post-treatment, can significantly impact their return to social life [1]. Furthermore, the ordeals of having cancer, experiencing disease progression, and receiving a diagnosis at a young age can trigger Post-Traumatic Stress Disorder (PTSD) in many cancer survivors. In fact, more than 50% of breast cancer patients report having this condition [8, 9].
Office workers often face numerous stress-related factors, such as heavy workloads, unclear role definitions, and social issues within the workplace [10]. Those who are also cancer survivors must contend with additional challenges stemming from their treatment, including cognitive impairment, restrictions on physical activity, anxiety, depression, and difficulty maintaining eye contact [4]. Furthermore, they grapple with disease progression-associated distress, a term encompassing a range of emotions including anxiety, stress, worry, panic, and fear. This distress has been identified as a factor impacting their work [11].
The stress experienced by cancer survivors is an important issue that affects daily life and symptom management. However, existing research has been limited to the survivors of certain specific cancers, such as breast and colorectal cancer [7, 12]. Previous studies of breast cancer survivors have demonstrated that current health status, including self-rated health, activity limitations, and physical discomfort, influences stress levels [13, 14, 15]. Furthermore, past research has indicated that health behaviors, such as perceived body image, smoking and alcohol consumption, and physical activity, can also contribute to stress. These findings were observed in studies involving breast cancer and head and neck cancer [13, 14, 16, 17]. Additionally, prior research exploring the relationship between mental health and stress in cancer survivors has found a correlation between stress and mental health issues, such as depression and suicidal ideation [18, 19, 20]. Moreover, while studies have been published on PTSD, psychological stress, and physical stress in cancer survivors, little research has focused on the comprehensive identification of stress-related factors [2, 4, 8].
While some studies have explored stress-related issues in cancer survivors overall, this research has certain limitations. These include small sample sizes and a lack of generalizability to various types of cancer and to survivors of single-organ cancers [8, 9]. Additionally, these studies utilized only 1 year of national data, had limited numbers of participants, and focused solely on specific types of cancer. None of these studies aimed to identify stress factors using comprehensive indicators such as sociodemographic factors, current health status, health behaviors, and mental health characteristics [21]. In certain countries, research has been conducted on the reintegration into the workforce of cancer survivors, with a focus on job type [3, 5]. However, similar research is scarce in Korea. Notably, policies and support projects are currently being implemented in Korea to benefit cancer survivors as a whole [22, 23]. Employment has been shown to positively impact the QOL of cancer survivors [1]. However, cancer survivors face many challenges in maintaining their employment due to additional stressors such as physical fatigue. Research has indicated that a higher percentage of cancer survivors (18.4%) experience job-related stress than the general population (11.3%) [4, 5, 24]. Therefore, a need exists for information that can assist cancer survivors in maintaining their employment by comprehensively identifying and addressing their stress factors. The objectives of the present study were to identify factors associated with the stress experienced by working Korean cancer survivors using 5 years of national data (including cancer types and age groups), as well as to provide foundational data for the development of stress management intervention programs for this patient population.
This cross-sectional descriptive study was designed to identify factors associated with perceived stress among working cancer survivors. In addition, a secondary analysis was performed using 5 years of data (2014~2018) from the Korea National Health and Nutrition Examination Survey (KNHANES).
For this study, 5 years of raw data were retrieved, spanning from the second year of the sixth KNHANES (2014) to the third year of the seventh KNHANES (2018). The survey employed a multi-sample design, stratifying cities, neighborhoods (dongs), townships, and housing types across the 960 survey districts nationwide. It also stratified the embedded layers (gender, age, residential area, head of household, and education level) of 36,931 people, including infants and the elderly. Among the respondents, 245 reported being employed and having stomach, liver, colon, breast, cervical, lung, thyroid, or other cancers. For instance, respondents who reported currently having stomach cancer and who confirmed their employment status were selected for the study and categorized as having an occupation. Each participant was also assigned a value for the stress variable, which served as a dependent variable in this study. Participants with missing values were excluded. Ultimately, a total of 245 participants were included in the statistical analyses (Figure 1).
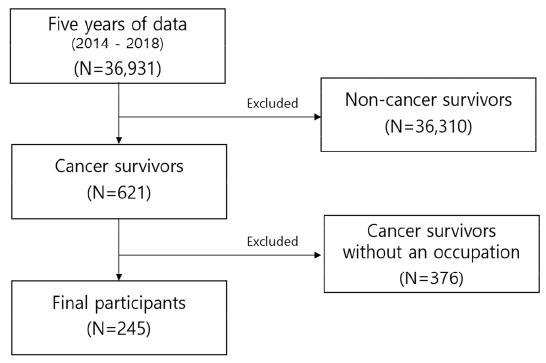
Figure 1
Participant selection flow diagram.
The institutional review board of the researchers' affiliated institution waived the requirements for ethical approval and informed consent for this study.
To evaluate stress levels, we utilized a fixed response to the question "How much stress do you feel in your daily life?" from the KNHANES database. Participants were categorized into two groups according to their responses: those who indicated they felt "very much" or "much" stress in their daily lives were deemed to have high stress levels (the stress group), while those who answered "little" or "hardly any at all" were classified as having low or no stress (the non-stress group).
Sociodemographic characteristics (including age, gender, and education level) were examined as variables within the KNHANES questionnaire data.
Current health status was selected as a variable based on the findings of previous studies of breast cancer survivors, which indicated that health status impacts stress [13, 14, 15]. Characteristics of current health status were identified, including self-rated health status, activity limitations, experiences of being bedridden in the past month, physical discomfort experienced in the past two weeks, and QOL. Self-rated health status was classified as very good, good, moderate, bad, or very bad in accordance with the KNHANES questionnaire, which asked the question "How do you usually feel about your health?" Activity limitations were determined by a yes-or-no response to the question "Do you currently have limitations on your daily life and social activities due to health problems or physical/mental disabilities?" Being bedridden in the past month was defined by a yes-or-no response to the question, "Have you had to spend most of the day bedridden due to an illness or injury in the last month?" Physical discomfort in the previous 2 weeks was determined by a yes-or-no response to the question "Have you felt sick or uncomfortable due to chronic/acute illness or accidental poisoning in the last 2 weeks?" QOL was assessed using raw data from the EuroQoL-5D questionnaire, approved by the EuroQoL Group (www.euroqol.org). This questionnaire uses a 3-point scale with 5 items: mobility, self-management, daily activities, pain/discomfort, and anxiety/depression. Each is rated from 1 to 3 points, indicating no problem, some problem, and inability to do a certain activity, respectively, or indicating no, moderate, or severe levels of pain/discomfort or anxiety/depression.
Health behavior was chosen as a variable due to evidence suggesting its impact on stress in studies of breast cancer and head and neck cancer [13, 14, 16, 17]. Health behavior-related variables included perceived body image, weight control over the previous year, alcohol consumption, smoking status, moderate-intensity physical activity, walking over the previous week, and nutrition label literacy. Perceived body image was assessed using the question "How do you perceive your current body shape?" with possible answers of skinny, underweight, normal, overweight, and obese. Weight control over the previous year was determined by the response to the question "Have you voluntarily tried to control your weight in the past year?", with possible answers including "weight loss," "weight maintenance," "weight gain," and "no." Alcohol consumption was assessed using the question "Have you ever had more than one drink in your life?", with possible responses of "yes" and "no." Smoking status was determined by the response to the question "Do you currently smoke cigarettes?", with "I smoke every day or occasionally" reclassified as "yes" and "I smoked in the past, but not currently" reclassified as "no." Moderate-intensity physical activity was assessed by the question "Do you usually engage in moderate-intensity sports, exercise, or leisure activities that cause slight shortness of breath or slightly fast heartbeats for at least 10 minutes?", with possible answers of "yes" or "no." Walking over the previous week was determined by the question "How many days did you walk for at least 10 minutes at a time in the last week?", with reclassification of 1 to 7 days to "yes" and 0 days to "no." Nutrition label literacy was assessed by the question "Are you familiar with nutrition labels?", with possible answers of "yes" or "no."
The selection of mental health variables was informed by the findings of prior studies, which established a reciprocal relationship between mental health and stress in cancer survivors [14, 18, 19, 20]. These variables included current depression, depressive symptoms persisting for over 2 weeks, suicidal ideation in the past year, having a suicide plan in the past year, and psychiatric consultation in the past year. The term "current depression" was defined by a response of "currently suffering" to a question about the present experience of depression. The presence of depressive symptoms for more than 2 weeks was determined by a yes-or-no response to the question, "In the past year, have you ever felt so sad or hopeless that it disrupted your daily life for two or more consecutive weeks?" Suicidal ideation in the past year was gauged by a yes-or-no answer to the question "In the past year, have you ever seriously contemplated suicide?" The existence of a suicide plan in the past year was assessed by a yes-or-no response to the question "In the past year, have you devised a specific plan to commit suicide?" Finally, visitation with a psychiatrist in the previous year was determined by a yes-or-no answer to the question "In the past year, have you sought counseling for mental issues through visits, phone calls, or the internet?"
Given the complex sampling design, statistical analyses were performed using SPSS (version 25.0; IBM Corp., Armonk, NY, USA). All sampling and weighted variables were stratified, and survey sample weights were used for all analyses to generate unbiased estimates for the descriptive and analytical data analyses. The weighted values were created over the 5-year period, and estimates were not provided for missing values. Any differences in sociodemographic and health-related data (based on perceived stress levels) were tested using either a χ2 test or an independent t-test. Furthermore, multiple logistic regression analyses were performed to evaluate the associations between perceived stress levels and the included variables. Finally, Odds Ratios (ORs) and 95% Confidence Intervals (CIs) were estimated.
The mean age of participants was 53.56±10.57 years in the stress group and 57.42±11.40 years in the non-stress group. On average, the stress group was younger than the non-stress group, a difference that was statistically significant (t=5.04, p=.025). A significant gender difference was also observed between the stress groups (χ2=7.32, p=.006), which included 65.5% of women but only 34.5% of men. However, no significant difference in education level (χ2=7.16, p=.067) was found between the stress groups. In terms of health status characteristics related to stress, we observed a significant difference in bedridden experience in the previous month between the stress groups (χ2=6.45, p=.011). In addition, the patients in the stress group comprised 18.2% of those with bedridden experience but 81.8% of those without such experience. However, we observed no significant differences between the stress groups in terms of self-rated health status (χ2=8.38, p=.078), activity limitations (χ2=0.01, p=.973), physical discomfort experienced in the previous 2 weeks (χ2=0.01, p=.932), and QOL (t=2.13, p=.146).
Regarding health behavior characteristics associated with stress, we noted a significant difference in perceived body image across groups (χ2=11.08, p=.026). Categories included underweight (in which the stress group accounted for 3.6% of total participants), skinny (3.6%), obese (16.4%), with normal (38.2%) and overweight (38.2%) having the highest proportion accounted for by the stress group. However, over the past year, we found no significant differences between the stress groups in terms of body weight control (χ2=7.11, p=.069), lifetime drinking experience (χ2=0.50, p=.481), smoking status (χ2=0.27, p=.604), moderate-intensity physical activity (χ2=0.01, p=.981), walking in the last week (χ2=0.03, p=.866), and nutrition label literacy (χ2=2.73, p=.098).
Regarding mental health characteristics related to stress, we found a statistically significant difference in the presence of depression across groups (χ2=4.98, p=.026). Specifically, participants in the stress group accounted for 7.3% of those currently experiencing depression, compared to 92.7% of those not experiencing it. A significant difference among groups was also observed in the presence of a suicide plan in the previous year (χ2=6.45, p=.011). Participants in the stress group accounted for 5.5% of those with a suicide plan in the past year and 94.5% of those without such a plan. However, we observed no significant differences between the stress groups regarding the presence of depressive symptoms for more than 2 weeks (χ2=3.50, p=.061), suicidal ideation in the previous year (χ2=0.58, p=.445), or visiting a psychiatrist in the previous year (χ2=2.68, p=.102) (Table 1).
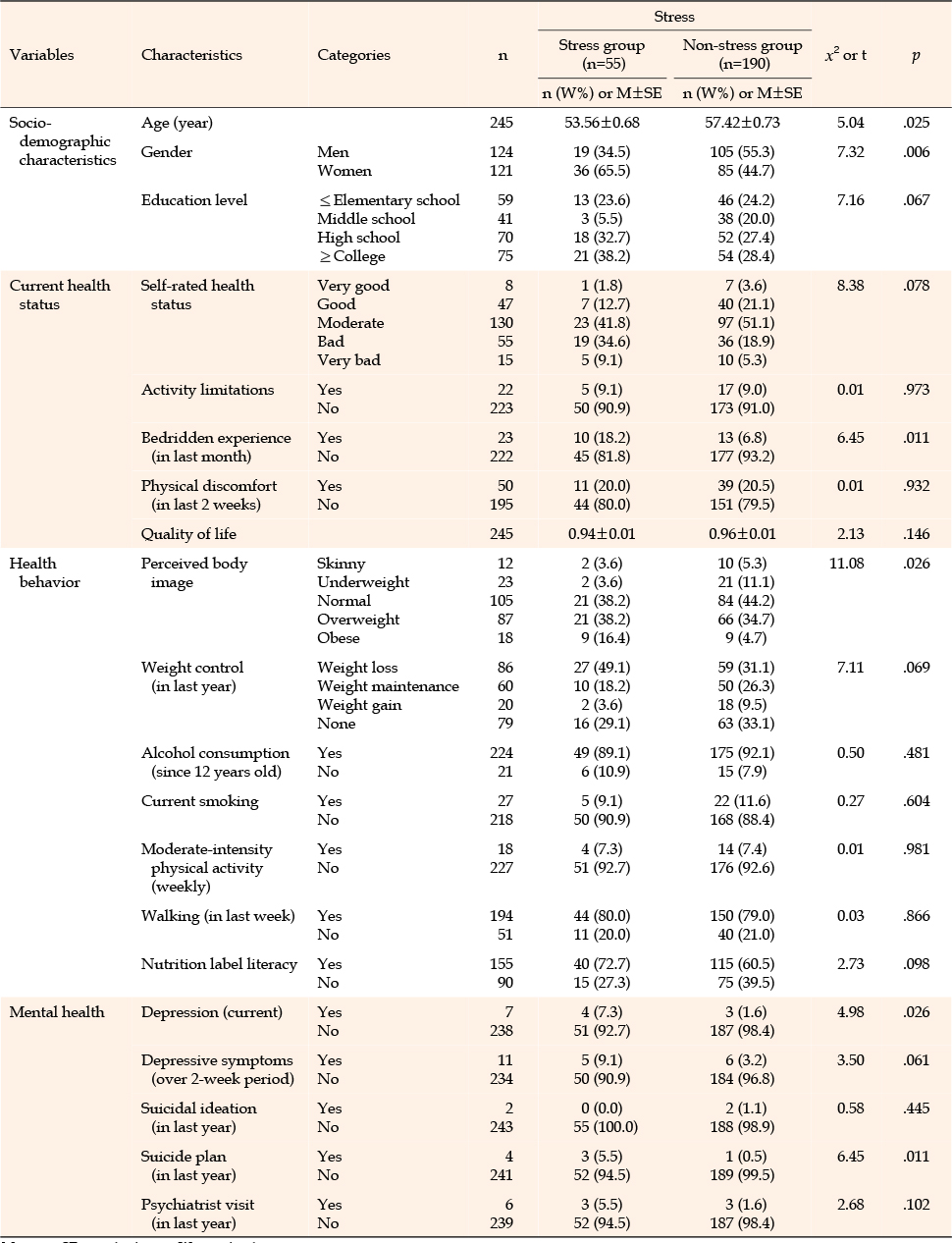
Table 1
Differences in Participant Characteristics by Stress Group (N=245)
We utilized sociodemographic characteristics, current health status, health behavior, and mental health in a regression analysis to identify factors associated with stress among employed Korean cancer survivors. The criteria for inclusion in the analysis was a p-value of less than .100, as suggested by previous studies [25]. Independent variables were included in the univariate logistic regression analysis if they had a p-value of less than .100. The regression model was deemed suitable (χ2=114.30, p<.010); the Cox-Snell coefficient of determination (R2) was 37.3%, and the Nagelkerke coefficient of determination (R2) demonstrated an explanatory power of 50.0% (Table 2).
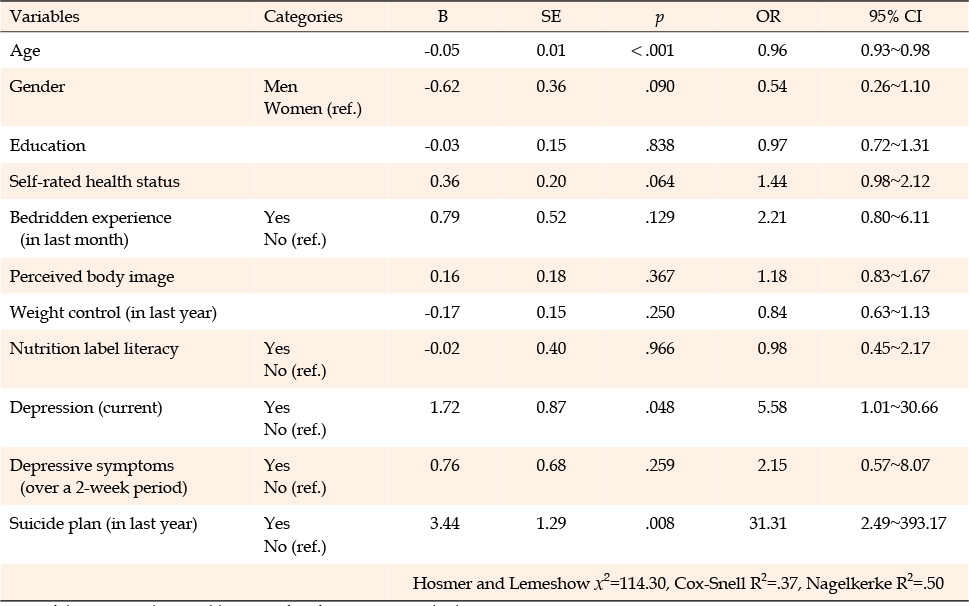
Table 2
Factors Associated with Stress Levels in Employed Korean Cancer Survivors (Univariate Logistic Regression) (N=245)
The multivariate logistic regression analysis, performed using significant variables from the univariate analysis, revealed that age, gender, self-rated health status, and having planned suicide within the previous year were relevant factors. Specifically, with each additional year of age, the likelihood of being in the stress group increased by 0.96 (95% CI=0.94~0.98). The probability of a man being in the stress group was 0.46 times that of a woman (95% CI=0.23~0.91). A self-rated health status score increase of one of five levels (ranging from "very good" to "very bad") carried 1.44 times (95% CI=1.03~2.02) greater likelihood of being in the stress group. Furthermore, individuals with a suicide plan were 22.98 times (95% CI=2.10~251.83) more likely to be in the stress group compared to those without a suicide plan (Table 3).
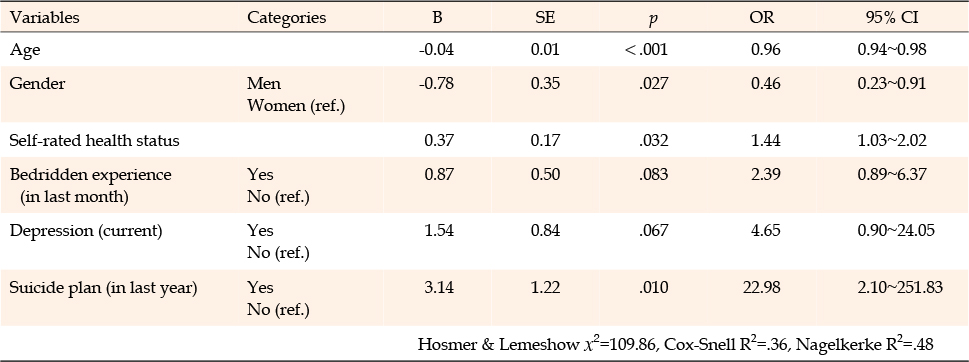
Table 3
Factors Associated with Stress Levels in Employed Korean Cancer Survivors (Multivariate Logistic Regression) (N=245)
Multivariate logistic regression analysis revealed that age, gender, self-rated health status, and suicide planning in the previous year were associated with stress among employed Korean cancer survivors. Regarding age, the average age of the stress group was lower than that of the non-stress group. This finding aligns with a study reporting high stress levels in young cancer patients and a separate study in which younger cancer patients were found to be more susceptible to PTSD than older patients [8, 9]. Similarly, a study of women with breast cancer revealed that the younger the patient, the higher the stress level [12]. Young cancer survivors, in particular, have been reported to experience work-related stress and serious financial difficulties due to physical and cognitive impairments [26]. Therefore, it is crucial to implement stress management strategies for young cancer survivors, who typically have relatively promising social and RTW opportunities.
Gender was also identified as a factor influencing stress levels, with a higher proportion of women than men in the stress group. A study focusing on typical office workers revealed that women were more susceptible to stress and anxiety disorders than men due to job-related demands [27]. Another study suggested that female cancer survivors experience greater depression when undergoing cancer treatment while also managing household tasks, which can negatively impact QOL [28]. This may be attributed to the fact that male cancer survivors are more likely to be employed than their female counterparts, while women often face work-family conflicts due to the dual burden of work and family responsibilities [29]. Therefore, when designing a stress intervention program for working cancer survivors, it is crucial to consider the lifestyle of women who, in addition to their jobs, often devote more time to housework and childcare than men.
Self-rated health status was also found to be associated with stress among employed Korean cancer survivors. In a previous study of patients with rectal or anal cancer, depression and anxiety accounted for a large proportion of the causes of stress. Furthermore, depression was linked to negative perceptions of physical health [30]. In a similar study, self-rated health status was revealed to have substantial impacts on QOL, RTW, and job satisfaction among cancer survivors [31]. Interventions involving physical activity can positively influence the subjective self-rated health status of cancer survivors, potentially reducing the risk of several cancer-related symptoms such as pain, depression, and anxiety. These interventions can also aid cancer survivors attempting to RTW [3]. As such, self-rated health status is an important factor in stress management for working cancer survivors. Therefore, it is vital to develop an intervention program targeting self-rated health status, such as a physical activity intervention involving 30 minutes of low-to-moderate-intensity exercise [32].
Participants who had a suicide plan over the previous year were more likely to be in the stress group. This relates to the elevated suicide rate associated with a cancer diagnosis, mirroring the findings of earlier studies that discovered high stress levels among cancer survivors who had suicidal thoughts or plans [18]. Research conducted in the United States revealed that cancer survivors had statistically higher suicide rates than the general population [33]. Furthermore, in Korea, cancer survivors exhibited higher rates of depression and suicide attempts in the previous year compared to the general population [18]. Consequently, suicide planning is an important factor to consider when managing cancer survivors, and stress management interventions such as mindfulness-based techniques and mobile health interventions are needed [34, 35].
In this study, with the goal of increasing RTW success among cancer survivors, the factors associated with stress among employed survivors were identified as comprehensive indicators. These factors included sociodemographic characteristics, current health status, health behaviors, and mental health characteristics. This contrasts with studies on head and neck cancer survivors, which highlighted financial stress as a prominent factor for those unemployed [25, 36]. Employment can positively impact the physical and mental health of cancer survivors, beyond its economic benefits, and can contribute to improved QOL [1]. Furthermore, stress and QOL have been found to be influenced by different factors depending on the employment status of the cancer survivors [37]. Notably, employed survivors exhibit better QOL and lower symptoms of stress and depression compared to their unemployed counterparts [37]. These findings underscore the need for stress-reducing interventions and/or rehabilitation programs, such as mindfulness-based stress management intervention, mobile health intervention, and low-to-moderate-intensity exercise for cancer survivors planning to RTW. These measures could enhance the success rate of RTW and job retention. Consequently, we recommend that future research should focus on developing a nursing stress management intervention program for Korean cancer survivors who are employed or planning to RTW. This could facilitate their post-traumatic growth. We also propose a future study on the stress factors of employed cancer survivors, incorporating data from the eighth KNHANES.
This study had several limitations. First, it was based on an analysis of secondary data; thus, only variables present in the raw data could be utilized, restricting generalizability. Moreover, the application of stress relative to the condition of the cancer patient is challenging due to the absence of detailed information about the cancer survivor, such as the survival period post-diagnosis and the cancer stage. Second, the data item evaluated in the analysis was daily life stress, which may have included stress unrelated to returning to work. Third, the stress evaluation items in the KNHANES were assessed by selecting a fixed response on a 4-point scale for a single item concerning stress perception level. As a result, specific aspects of stress in cancer survivors could not be assessed. Furthermore, participants were divided into a stress group (those who responded "very much" or "much") and a non-stress group (those who responded "little" or "hardly any at all") based on their answers to the stress question. However, dividing the stress group into four subgroups and analyzing data from additional survey years would yield more detailed study results. Additionally, the KNHANES provides national data for Koreans, with potential differences from Western culture and institutions. Finally, this study was conducted using KNHANES data through 2018, so a need exists to better reflect the latest trends. Therefore, we propose a follow-up study using data from the eighth KNHANES. Despite these limitations, this study was meaningful through its use of comprehensive data. By utilizing national data spanning 5 years (2014~2018) that included a full set of cancer types and various age groups, we could comprehensively identify the factors associated with stress among employed Korean cancer survivors.
Cancer survivors often experience considerable stress during and after treatment, which can manifest as cognitive impairment and physical fatigue. Consequently, these individuals may struggle to maintain their employment or RTW. Therefore, it is crucial to provide effective stress interventions to cancer survivors at an early stage. The findings of this study are anticipated to serve as foundational data for developing interventions aimed at reducing stress among working cancer survivors.
This study was conducted to identify the factors influencing stress among employed Korean cancer survivors, using KNHANES data. The overall predictors of these factors were identified in this research. Logistic regression analyses revealed that younger age, being a woman, self-rated health status, and having planned suicide in the past year all impacted stress in working cancer survivors. These findings suggest that these factors should be considered when designing stress intervention programs for survivors. Furthermore, this research can inform the development of a stress intervention program for Korean cancer survivors who are employed, whether in the workplace or the community. Consequently, we recommend that future research should focus on creating a nursing stress management intervention program for Korean cancer survivors who are employed or about to RTW, to facilitate their post-traumatic growth.
CONFLICTS OF INTEREST:Kisook Kim has been the Editor-in-Chief of the Korean Journal of Adult Nursing since 2022. She was not involved the review process. Otherwise, no potential conflict of interest relevant to this article was reported.
AUTHORSHIP:
Study conception and design acquisition - KK.
Data collection - KK.
Analysis and interpretation of the data - KK and OB.
Drafting and critical revision of the manuscript - KK and OB.
This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (NRF-2020R1F1A1048591).
 E-SUBMISSION
E-SUBMISSION