
Purpose
This study identified the experiences of self-reflection of a general ward nurses on the experience of end-of-life care for a patient who decided to suspend life-sustaining treatment and these experiences’ nature and meaning.
Methods: van Manen's hermeneutic phenomenology research method was used to qualitatively analyze the data. The study participants were 20 nurses with more than three years of working in general wards of tertiary general hospitals. Data were collected through face-to-face in-depth interviews and direct observation by the researchers. Social distancing was practiced in accordance with COVID-19 social distancing policy.
Results: Four existences were identified from which 5 main and 14 sub-themes were derived. Five essential themes emerged from the analysis: 1) Hoping to return to an undamaged body and knowing the preciousness of the body, 2) Realize that the ability to care for the dying patient becomes more mature with the increase in career, 3) The death in the treatment room like a death on street makes regrettable the absence of end-of-life rooms, 4) Seeing the preciousness of my life in accompaniment with death, and 5) Become aware of growing up as a professional nurse.
Conclusion: The results of this study provided an in-depth understanding of the end-of-life experiences of patients who decided to suspend life-sustaining treatment in general ward nurses. It can be used to develop end-of-life nursing education for nurses and students and develop nursing interventions for end-of-life patients.
This study identified the experiences of self-reflection of a general ward nurses on the experience of end-of-life care for a patient who decided to suspend life-sustaining treatment and these experiences' nature and meaning.
van Manen's hermeneutic phenomenology research method was used to qualitatively analyze the data. The study participants were 20 nurses with more than three years of working in general wards of tertiary general hospitals. Data were collected through face-to-face in-depth interviews and direct observation by the researchers. Social distancing was practiced in accordance with COVID-19 social distancing policy.
Four existences were identified from which 5 main and 14 sub-themes were derived. Five essential themes emerged from the analysis: 1) Hoping to return to an undamaged body and knowing the preciousness of the body, 2) Realize that the ability to care for the dying patient becomes more mature with the increase in career, 3) The death in the treatment room like a death on street makes regrettable the absence of end-of-life rooms, 4) Seeing the preciousness of my life in accompaniment with death, and 5) Become aware of growing up as a professional nurse.
The results of this study provided an in-depth understanding of the end-of-life experiences of patients who decided to suspend life-sustaining treatment in general ward nurses. It can be used to develop end-of-life nursing education for nurses and students and develop nursing interventions for end-of-life patients.
Nurses encounter death, an inevitable event for all humans, the most frequently while working at medical institutions [1]. Additionally, the place of death is now becoming a medical institution, breaking away from the Korean tradition that one should pass away at home, reluctant to die on the road away from home [2]. Statistics on the place of death also show that deaths in medical institutions accounted for as much as 75.6% in 2019, gradually increasing compared to 65.9% in 2009 [3]. Moreover, with the implementation of the Act on Hospice and Palliative Care and Decisions on Life-sustaining Treatment for Patients at the End of Life in 2018, there are more cases of severely ill patients or patients at the end of life in general wards deciding not to receive life-sustaining treatments and remaining in general wards, rather than being transferred to intensive care units [4]. Such a phenomenon implies that there are now increasing opportunities for nurses to witness end of life in general wards.
Most previous studies on nurses' experience of patient death were quantitative studies, with topics including death perception [5], hospice-palliative care [6], attitudes toward end-of-life care [7], terminal care performance [8], stress of end-of-life care [9], death anxiety [10], spirituality [11], and death education [12]. Prior studies that applied a qualitative research method were primarily conducted on nurses in intensive care units [13], long-term care hospitals [14], and hospice wards [15], and the topics included end-of-life experience, experience of end-of-life care, experience of caring for patients at the end-of-life, and experiences of coping with end-of-life care. In addition, in terms of studies on self-reflection on death, there has been one study on developing a program of self-reflection on dying children for pediatric and neonatal intensive care unit nurses [16]. Among the various qualitative research methods, the hermeneutic phenomenological method helps understand the meaning and essence of experiences inherent in the subject's language, beliefs, culture, and social conventions [17] and is a holistic approach to understanding the subject's experiences in the environment and situation humans encounter [18]. As there has been no qualitative study on the topic despite the recent increase in nurses caring for end-of-life patients in general wards who decided to withdraw from life-sustaining treatments, the present study attempted a qualitative investigation by applying a phenomenological research method.
In an investigation on the stress of death where the degree of fear of medical personnel in end-of-life situations was examined, 35.4% of doctors and 47.2% of nurses responded that they felt intense fear [19]. Furthermore, it has been reported that when nurses have not established appropriate coping mechanisms because they have not established the meaning of their lives, they show existential emptiness and have limitations in providing appropriate care to patients and families in end-of-life situations [20]. In this regard, self-reflection, one of an individual's internal mechanisms, has been mentioned as an appropriate method to cope with death and to aid nursing practice for nurses working in a ward with end-of-life patients [21]. Self-reflection begins by creating the right relationship with oneself by focusing on one's experience and meaning. A nurse begins to become self-aware and gain self-understanding by reflecting on one's life choices, values, and beliefs, after which one comes to perceive the commonalities and identify general meanings and creates therapeutic relationships as one understands others' experiences in the context of one's own life through human experience and its meaning. Nurses are considered selfreflective beings. It includes the connection between the world of life and the nursing experience and self-analytic perspectives, and in it can be discovered other dimensions of experience, such as the hidden meanings of behaviors, experiences, values, thoughts, and emotions [22]. Therefore, self-reflection is an indispensable aspect of caring for others, and it supports the possibility of self-fulfillment as an experience of an integrated process of all areas of nursing, including the relationships with self, others, and the world [23]. Patricia [22] stated that nurses' self-reflection allows one to examine oneself through self-awareness and creates new insights as it includes all aspects of nursing, from nursing skills to communication and interaction with others. And the growth of nurses themselves is achieved through the process of self-reflection, self-understanding, understanding and caring for others. Accordingly, nurses' self-reflection on patient death will establish nurses' perception of themselves, understanding of patients, and their philosophy on death, thereby affecting their therapeutic nursing practices that assist patients in maintaining dignity as human beings and receiving a dignified death.
Van Manen's hermeneutic phenomenology emphasizes the understanding, interpreting, and practicing phenomena related to human living [24]. It encourages nurses to obtain nursing skills and techniques for specific situations and relationships that occur in the field daily, to act more reflectively, and to practice nursing skills well. Additionally, hermeneutic phenomenology states that the self-reflection method allows us to determine whether conscious things revealed on the surface affect our perception through a hermeneutic circle [25]. Accordingly, the present study sought to explore the meaning and essence of the nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments in general wards using van Manen's hermeneutic phenomenological approach, characterized by analysis of various data such as in-depth exploration of participants' experiences, literature, artwork, and etymology, among various phenomenological methods.
The purpose of this study was to provide a framework for the development of end-of-life nursing education and intervention by understanding and describing in-depth the meaning and essence of general ward nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments. The research question of the present study is "What is the meaning and nature of the general ward nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments?"
The present study is qualitative research that applied van Manen's hermeneutic phenomenological approach to explore the essence and understand the meaning of nurses' experience of self-reflection on end-of-life care for patients who decided to suspend life-sustaining treatments.
As the participants in the study must include all attributes of the phenomenon to be studied, a purposeful sampling method was used to select 20 participants who can express insightful experiences of end-of-life care at the level of their existence and the nursing profession.
The participant inclusion criterion was general ward nurses at Y Medical Center, a tertiary general hospital, with at least three years of clinical experience and cared for patients at the end of life who decided to suspend of life - sustaining treatment in the past three years. Skilled and expert-level nurses with more than three years of experience with intuitive understanding, analytical skills, and understanding of critical aspects of a situation according to Benner's Stages of Clinical Competence were selected as participants to secure data with sufficiency [26]. The participant exclusion criteria were nurses who have not experienced patient death within the past three years and nurses from special departments, including intensive care units, hospice-palliative wards, pediatric wards, emergency rooms, and operating rooms.
After obtaining the approval for the study from the nursing department, the wards with frequent deaths identified by the nursing department were visited, and the purpose and participant standards of the study were explained to the part leader in person. When a voluntary participant presented themselves in a ward, the researcher revisited the respective ward, explained the purpose of the study again to the participant in person, conversed briefly with the participant about the topic of the study, and encouraged voluntary participation in the study. The number of participants was not established for the current study, and participants were recruited until the point of saturation when no new data was found. There were no part leaders or managers among the 20 general nurses recruited, and none withdrew their participation during the study period. The age of the participants ranged from 28 to 56, with a mean age of 35.05 years. Eight participants were married, and the rest was single. Most participants, 11, had no religion, seven were Christians, one was Catholic, and one was Buddhist. Work experience ranged from a minimum of 3 years to a maximum of 25 years, with a mean of 10.55 years. The survey of the number of times a nurse has experienced patient death was investigated based on categories because an accurate recall was challenging for the nurses. Five nurses each experienced patient death less than five times, six to ten times, and 20 or more times. Four nurses experienced patient death 11 to 20 times, and one experienced it five to 10 times (Table 1).
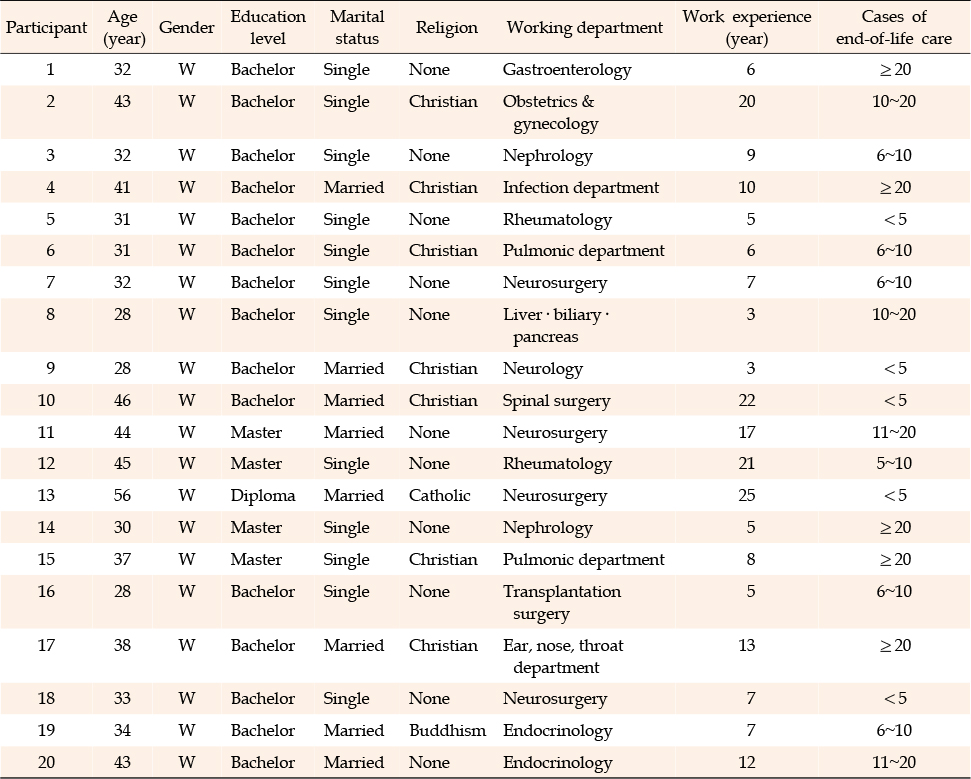
Table 1
General Characteristics of Research Participants
Data was collected directly by the researcher through 1:1 in-depth interviews from May 20 to August 20, 2022, after approval by the Institutional Review Board. One to three interviews of 50-minute to 1-hour sessions were conducted, depending on the participant. The interview began with forming rapport and trust with the participants through daily greetings and discussing overall issues at the hospital or work-related topics. The crucial parts of the interviews and insufficient information, such as ambiguous and suspicious ones, were noted, and then the meaning of the data was confirmed by asking follow-up questions after the interview or by over-the-phone reaffirmation process. The interview was conducted until no new information was available. Meeting rooms in the hospital, a space free of external distractions and guaranteed confidentiality, were designated as the place of the interview. The interviews were held after the end of a shift or on off days of the participants in a meeting room on a different floor from the floor on which participants work. At the first meeting, the researcher introduced herself, greeted the participants, and created a natural atmosphere by building rapport through general talks about the hospital and daily conversations. Then, the researcher expanded the conversation to topics related to the research topic, broadening the purpose and depth of the conversation, and allowed the participants to talk comfortably by asking open and semi-structured questions. During the interview, the researcher encouraged the participants to fully share their experiences by providing empathetic reactions, such as eye contact and nodding. If a participant showed emotional distress, such as not being able to speak or showing tears while recalling past experiences, the researcher tried to respect the participant's feelings by holding their hands and waiting in silence and encouraged honest expression.
Due to the COVID-19 pandemic in 2020, 1:1 in-person interviews were conducted in a meeting room, complying with the social-distancing and mask-wearing regulations, and the meeting room was sprayed with disinfectants, and its doors were opened for ventilation after each interview. The participants belonged to the vulnerable group working in the same hospital in this study, but there was no conflict of interest because the researcher was not applied to the vertical relationship as a fellow nurse. The final research question at the time of the interview was, "What is general ward nurses' experience of self-reflection on the experience of end-of-life care of patients who decided to suspend life-sustaining treatments?"
The interviews were recorded using the recording function on a smartphone or a recorder with the participants' consent to secure the interview data's factuality and prevent omission. The researcher transcribed the recorded data without missing any contents from beginning to end immediately after the interviews and checked whether there were any inconsistencies between the recorded and transcribed data by listening to the recordings several times. Then, the contents were confirmed by the participants. Furthermore, field notes were used to record nonverbal communication observed during the interviews, such as the participants' expressions, accents, and gestures, and to note their reactions and questions. The participants were rewarded with a small gift after the completion of the interviews.
This study was conducted with the review and approval of the institutional review board of Y Medical Center (IRB number 4-2020-0185). Before beginning the interviews, the researcher explained the purpose of the study and procedures, including recording, and obtained the participants' written consent after they had fully understood and decided to participate voluntarily. The participants were explained that the collected interview data will not be used outside of the study and that the privacy of participants and their identity or personal information will be kept anonymous and confidential. The participants were also informed of their rights to refuse interviews and withdraw their participation at any time, and the interview process was recorded with the participants' consent. The recorded and transcribed data were stored on the researcher's personal computer with a password for security. The interview materials will be stored for three years and permanently deleted in a way that cannot be restored after the study is completed in accordance with the provisions of the Institutional Review Board.
Data analysis was performed based on the hermeneutic phenomenological method presented by van Manen [17]. For data analysis, this researcher created a manuscript of the data collected during the interview with the participants, preserving their verbal expressions, tone, pronunciation, and the use of onomatopoeia, and used field notes for nonverbal expressions and behaviors. The entire transcribed interview data was reviewed while listening to the recordings repeatedly to compare the two and identify any errors or omissions in the transcribed content. Efforts were made to ensure the contents' accuracy by listening to the recordings, reading the transcriptions, and clarifying any ambiguities through double-checking on phone calls or at second or third interviews. Text separation work was performed by repeatedly reading the collected material and identifying statements that could capture the basic or primary meaning of the entire text. The separated texts from the above process were read several times to distinguish and mark any words or sentences that revealed the essence of the phenomenon or experience particularly well. The separated words and sentences were structured by finding similar concepts or contexts, and the process of changing them into a word that encompasses the meaning was repeated. The intrinsic themes with increased abstraction were classified by integrating meanings, structures, and processes, such as individual experiences derived from the data. Statements similar to the themes were derived from the researcher's own experience, literature, and artworks, compared, and reviewed to richly express the meaning of the themes derived from the participants' statements regarding their experiences. Finally, the intrinsic theme and subtopics regarding general ward nurses' experiences of self-reflection on end-of-life care of patients who decided to suspend life-sustaining treatments were derived.
The quality of the research was secured by ensuring the study's reliability and validity through applying the four evaluative criteria proposed by Lincoln and Guba [27]: applicability, factual value, consistency, and neutrality. First, to improve applicability, data was collected, and meanings were identified until no more meaningful data was found in each participant's statements. In addition, two other nurses who were not participants and witnessed patient death were asked to read the results and compare them to their own experiences to determine whether the results were meaningful and applicable. Second, to increase the factual value, three participants were shown the contents of the interview records and the analysis results to confirm whether the participants' experiences were consistent with the results of the researcher's analysis. Third, the consistency of the study was increased by thoroughly understanding and strictly observing van Manen's hermeneutic phenomenological research methods and by commissioning two professors experienced in qualitative research during the data analysis process to evaluate the study results and revise the categorization of the themes. Finally, to increase the neutrality of the study, the researcher's prior understanding of the study, prejudices, and assumptions were recorded in a personal journal to maintain neutrality throughout the study.
The present researcher worked in pediatric hematology-oncology ward, surgical oncology wards, neurosurgical oncology wards, and neurological intensive care units at tertiary general hospitals and have witnessed numerous deaths while nursing terminally ill patients. In particular, with the implementation of the Act of Hospice and Palliative Care and Decisions on Life-sustaining Treatment for Patients at the End of Life in 2018, the researcher frequently met with patients and their families who were dying in general wards after end-of-life patients made decisions about discontinuing life-sustaining treatment. The researcher tried to connect the researcher's own death in the future with the observed relationship between dying patients and their families, relatives, and surrounding individuals and made many reflections on the meaning of the researcher's life and the value of a professional as a nurse. Subsequently, the researcher came to question what meaning the nurses who have experienced patient death assign to life and the profession of a nurse. Accordingly, the researcher aimed to explore the introduced phenomenon to explore in depth the nature and meaning of general ward nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments and to help understand nurses who experienced patient death
The researcher may have prejudice in the context of the phenomenological approach due to prior experience of the phenomenon. Therefore, when writing interview questions, efforts were made to ask what the experience of the participants really was, that is, to ask what the nature of the experience was, while distancing the researcher's own prior experiences in order to ask questions oriented toward the essence. Additionally, the literature analysis that may affect the data collection or interpretation processes was conducted after completing the data collection and primary analysis.
On a different note, the assumption that the self-reflection experience of the researcher will be similar to that of other nurses may prevent the original attributes of the experience of self-reflection from being revealed. Therefore, the researcher suspended judgment and revealed and reflected on experiences of self-reflection and prior knowledge, consciously or unconsciously accumulated information, that is, prior understandings, related to end-of-life care from an insider's perspective to reveal the nature of the research phenomenon. Correspondingly, the researcher reflected on the assumptions and pre-understandings that the researcher had, compared them with the collected data, and tried to separate them from the researcher herself through a literature review. The researcher's assumptions and pre-understandings are as follows.
• The self-reflection of nurses who provide end-of-life care to patients who have decided to suspend life-sustaining treatments will be a phenomenon experienced by all nurses.
• Nurses who provide end-of-life care to patients who have decided to suspend life-sustaining treatments will feel ambivalent regarding the suspension of life-sustaining treatments during self-reflection.
• The self-reflection of nurses who provide end-of-life care to patients who have decided to suspend life-sustaining treatments will vary from individual to individual.
• The self-reflection of nurses who provide end-of-life care to patients who have decided to suspend life-sustaining treatments will affect professional improvement as a comprehensive capacity.
• The self-reflection of nurses who provide end-of-life care to patients who have decided to suspend life-sustaining treatments will affect their meaning of life and end-of-life care.
Experiential depictions in literature and artworks related to the pain of death were examined in this study to gain abundant insight into the phenomenon of caring for dying patients. Among artworks, "The Dead Mother and Her Child," "Death in the Sickroom," and "By the Deathbed" by Edvard Munch, and "Sick Bay" by Chang-ho Ahn were used in the analysis. Novels "My Brilliant Life" and "Tuesdays with Morrie" and films "Ending Note," "Seaside," "One True Thing," and "Jesus Hospital" were also analyzed. In the music, Schubert's "Death and the Maiden;" in photographs, Bohnchang Koo's "Breath" and Walter Schels' "Noch mal Leben vor dem Tod;" and in poems, Byung-wha Cho's "Man," Hae-in Lee's "Last Prayer," and Moon-jae Lee's "White Book 2" were used as materials for analysis.
The researcher nursed patients with brain tumors at the end of their lives in the neurology intensive care unit at Y Medical Center and met with and consulted patients and families after transferring to the neurosurgery ward. The researcher also tried to obtain a fundamental and in-depth understanding of qualitative research methodology by completing two courses during the doctorate program to secure sensitivity to the research phenomenon. As a member of the Korean Association for Qualitative Research and the Academy of Qualitative Research, the researcher participated in several workshops and conferences to broaden the understanding and knowledge of qualitative research and conducted two qualitative studies on the experience of diseases in patients with brain tumors and published them in academic journals.
Centered on the four lifeworld existentials (i.e., lived body, lived time, lived space, lived time, and lived human relation) in the phenomenological reflection guidelines proposed by van Manen [25], five essential themes and 14 sub-themes were derived from the data collected through interviews with participants regarding nurses' experience of self-reflection experience on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments (Table 2).
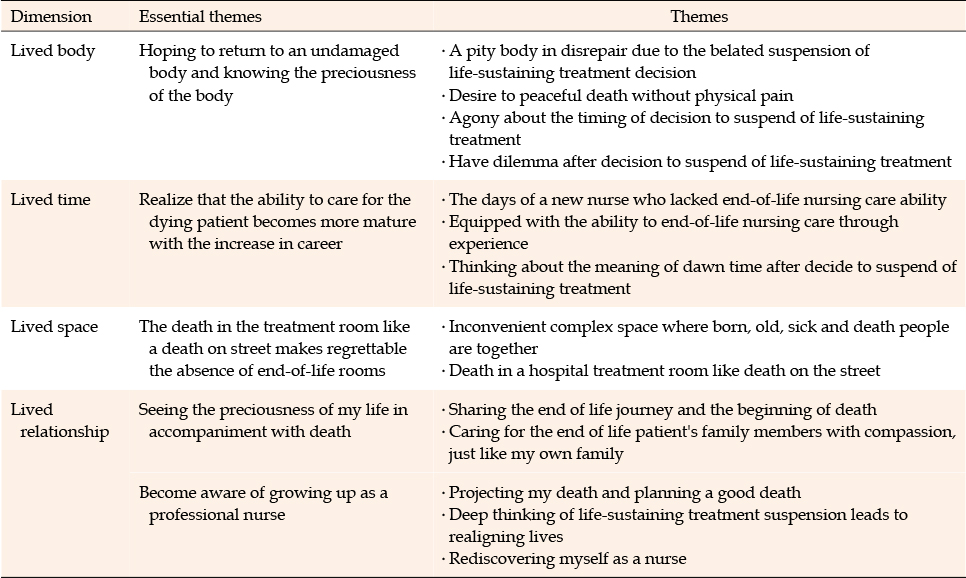
Table 2
The Themes of Self-reflection of a General Ward Nurses on the Experience of End-of-Life Care for a Patient who Decided to Suspend of Life-sustaining Treatment
The participants felt sorry and pity for patients as they saw spotted bodies full of bruises, bleeding marks, and scars caused by various treatments and procedures performed when their death was imminent due to the late decision to suspend life-sustaining treatments. Seeing these bodies, they thought of the patients' families, who would be even more sorrowful. On the other hand, they reported that it is desirable to suspend life-sustaining treatments according to a patient's own will and for them to die with the same physical integrity as when a human was born rather than creating wounds and damaging the body with meaningless procedures and invasive treatments.
I should not die like that while getting everything possible done (life-sustaining treatments, including cardiopulmonary resuscitation). Simply put, one should die well. With blood dripping down and all the ribs breaking as Cardiopulmonary Resuscitation (CPR) is performed.. It would not have gone this far if the patient had prepared the letter of intent for life-sustaining treatment in advance or decided to forgo it when they had even the slightest consciousness. Families are unable to make decisions because of the guilt caused by the suspension of life-sustaining treatments and end up deciding after the patients' bodies are broken. Still, once the patients expire, they look so pitiful that I carefully tend to every site where tubes and catheters are removed, make the bodies as clean as possible so that the families will not be upset and have the final meeting. <Participant 14>
The celebrity OO Kim was hospitalized and passed away (searching and showing the person on a cellphone). She could not have wounds on her body (pointing at the arm) because she was hospitalized during a shooting and did not even want intravenous injection marks, so she put in a venous port. The decision to suspend life-sustaining treatments was made when the patient was conscious, so not many treatments were performed, and her appearance was generally clean without injuries. A catheter was put in for ascites, and she refused to stitch out, so I used glue. No bloodwork was performed, so there was no bruising from needle insertions. Her death was the cleanest and most peaceful I have seen in clinical practice, and it made me want to die like her when I go. <Participant 1>
Fluid therapy, pain medications, and oxygenation were the last and best treatment options for patients who decided to suspend life-sustaining treatments, and the pain medication morphine sulfate could not be administered frequently due to the risk of sudden respiratory arrest. Participants reported that watching the patients suffer in pain until the moment of death with their families was also painful. The participants were disheartened and tormented to see the patients struggling with physical pain on their deathbeds. But they said that he looked very comfortable after he died. The German photographer Walter Schels Took pictures just before and after death in 'Life Before Death', showed a very comfortable state after death immediately.
Seeing patients in so much pain and their families watching that pain made me wish to die without pain. Life is struggling to survive. But immediately after death, the face seems very comfortable. Death frees from pain. Death seems like liberation from physical pain. <Participant 4>
Patients who suspended life-sustaining treatments are not put on ventilators or prescribed continuous renal replacement therapy. However, the late decisions to suspend life-sustaining treatments after having these medical devices already in place made participants experience futility and skepticism. A delayed decision to suspend life-sustaining treatments made in the event of a worsened situation after not initially having considered the suspension of life-sustaining treatments in the hope of physical recovery from the patient's perspective makes the patient endure physical and mental suffering. The participants stated that, in such a case, it is no longer a body with life, but the medical device takes over, and the last physical functions are maintained with difficulty according to the device's settings. The participants were contemplating when the appropriate time should be for suspending life-sustaining treatments in such a situation.
There was a patient who had been in good condition before and was expecting recovery. But, suddenly, her condition deteriorated, and all kinds of machines were attached to her body. She was conscious. She was on a ventilator for six months, and considered the alarm a warning of death every time it went off. Eventually, when the condition exacerbated and the alarm sounded frequently, the patient decided to suspend the life-sustaining treatment and requested to remove the ventilator, like she sensed that the time of death was near. Instead of waiting for death, not knowing when it will come, she decided her own time of death. I felt sorry for the life of relying on machines and was so disheartened about bringing it to a close with anxiety. <Participant 12>
The participants said that passive treatments such as fluid maintenance, oxygen therapy, and pain medications provided to patients who decided to suspend life-sustaining treatments seemed like a new kind of torture to wait for the uncertain time of death when respiratory or cardiac arrest naturally occurs. The participants discussed the dilemma of suspending life-sustaining treatments for reducing pain, which can result in a more painful death.
I watch the patients who suspended life-sustaining treatments until the moment they croak and expire. They did not seem like people. (Pausing for a moment, getting choked up) A person should pass peacefully, but they go in so much pain. Patients sign off on the suspension of life-sustaining treatments to die comfortably, to tell people not to do anything to them, but many die a difficult death after signing it. So I wondered,'Is this a peaceful death?' 'Who is the suspension of life-sustaining treatments for?' and 'Are they not being tortured?' <Participant 5>
In the past, when the participants were new nurses, the Act of Hospice and Palliative Care and Decisions on Life-sustaining Treatment for Patients at the End of Life, which allows the suspension of meaningless life-sustaining treatments for patients with no potential for recovery, was not legislated, so all treatments were provided to patients at the end of life, and accordingly, there was a high workload. Currently, while caring for patients who have already decided to forgo life-sustaining treatments is better than before, it is of concern whether these patients are neglected. The researcher recalled the days of being a new nurse, which began with an uncomfortable encounter with death. In particular, the shock and chaos were harsher for participants who had not yet experienced the death of family members or relatives when they were new nurses. They felt deeply timorous looking at the dead patients, did not know what to do as their minds turned blank, and reached a state of pause, or "mental breakdown."
The condition was already bad, so the patient was very swollen. There was even a tracheostomy tube, and if I touched it a little bit for suction, the oxygen saturation would drop rapidly. Their position must be changed, but if you turn the body slightly, the oxygen saturation drops fast. So I had a lot of anxiety, thinking that the patient would expire from moment to moment, and my stress and fear were bigger than the thought that I should care for this patient better. That patient was such a big stress for me, a novice, and I eventually ended up performing suction only once in a while. When I saw the patient after they expired, I felt so sorry that I had thought that was stress, and it felt like the patient died because I did not nurse them to the best of my abilities (cries).<Participant 7>
The participants underwent many trials and errors and learned end-of-life care through experiential knowledge handed down from senior nurses, like oral traditions. In particular, it was said that the role of nurses was more important than that of physicians once the suspension of life-sustaining treatments was decided. The suspension of life-sustaining treatments reduces treatment, and patients and families come to rely entirely on nurses for anxiety about the coming death. It was shared that senior nurses' role modeling in end-of-life care shown in this process was something no textbook entailed. The participants assisted patients who accepted death to receive death well and cared for and consoled their families. After patient death, they practiced holistic nursing, tidying up the bodies with care and giving their last respect to the deceased.
After watching senior nurses' role modeling for end-of-life care, shared by words and actions, my knowledge of and attitude toward end-of-life care changed. In particular, since hearing is the last intact sense of patients who die, and because patients who decided to suspend life-sustaining treatments do not receive much treatment but wait for death, senior nurses would hold the patients' hands and calmly tell them, "Do not worry and go to a good place." There also are senior nurses who change the deceased patients into clean clothes, change sheets, tidy up the bed, and neatly position the patient from head to toe. Seeing that, I try to do the same. Electrocardiography flatlines and death is declared, I give the caregivers time to say what they want to tell the patient, and then I tell them the procedures we need to do. I now can afford even to say the last goodbye, 'Thank you for all your hard work in life' to the deceased patient when an intern cleans up the lines and we change the patient's clothes. <Participant 8>
The participants gained experience in end-of-life nursing and became experienced nurses over time, and now they can perform not only physical nursing but also mental and spiritual nursing. They tried their best to provide holistic care for the patients in the face of death and prayed and talked together in the final moments. As participants gained experience caring for patients at the end of life, they have come to ponder the meaning of the remaining time of life for patients who decided to suspend life-sustaining treatments instead of solely focusing on physical end-of-life care as before. Iriryeosamchu (一日如三秋), an idiom that means that a day passes through three autumns, came to mind. The participants were saddened to think that the short time left would have felt so long because of the pain for patients who decided to suspend life-sustaining treatments.
One day of the remaining hours of a dying patient seems like three years for patients waiting for death after deciding to suspend life-sustaining treatments. But for us who are watching the dying patients who suspended life-sustaining treatments, the last hours of the patients feel like a relatively short moment. It is as though a day for us is a very short time, but a lifetime to survive for a mayfly. My heart ached while watching a lung cancer patient who suspended life-sustaining treatment roll around in bed, holding his neck, begging to help him breathe, even with the full concentration of oxygen administered (cries). Perhaps even one minute seemed too long for this patient. <Participant 20>
Participants also mentioned mixed simultaneous functions of hospital spaces with multiple duplexities. A new life is born on one end, and another dies on the other. The participants also described a hospital as a space where death is simultaneously far and close, as a patient who is suddenly deteriorated can be resuscitated with CPR or machines, such as a defibrillator, or can swiftly pass away. They also revealed an uncomfortable truth about the ornateness of funeral homes to which the deceased are transferred, while end-of-life room necessary for patients to have dignified death surrounded by family at the time of passing are nonexistent.
In my ward, a mother gives birth to a baby in the clean room, and a patient with infectious diseases in the next room faces death (sighs). On one side of the ward, a mother gives birth to a baby, and there is a celebration of birth with the baby's cry, while on the other side, a life ends, and it is full of mourning and cries of family members. It makes me think about how to live in such an ironic situation. I go into one room and congratulate... I go into the next room and mourn... This situation of alternating joy and sorrow is too difficult... (shows a perplexed expression on her face) <Participant 4>
Most hospitals do not have a separate end-of-life room, so patients whose death is imminent are transferred to a treatment room. The transfer of the treatment room of a patient nearing death is considered a sign of death, indicating that the death is imminent, and final preparations are made. For both families and nurses, this meant moving to a meaningful space for the passing. However, a treatment room in a hospital ward is a space where simple procedures, tests, and dressings are performed, filled with all kinds of devices, equipment, and treatment materials, and it is an open space where many people, including patients and medical staff, come and go. Participants said that death in such a treatment room was like death on the road. The participants said that ending life in a treatment room is too unfortunate and that it is necessary to have space where patients can spend their last moments nobly as human beings.
Once, there was a VIP, and there was a cardiac arrest in the middle of the night. But, the intensive care unit was full, so he couldn't be transferred there and was transferred to a treatment room and was performed CPR. It was mayhem. After all the first aid, the guardian decided to suspend life-sustaining treatments. The patient's condition got worse and worse, and he eventually passed away in the treatment room after two days. He should have been able to pass away with dignity, and it was a pity that he passed away in a chaotic atmosphere where the family was holding the patient's last service and singing hymns in the corner of a treatment room where central staff, doctors, and nurses constantly came and went like a market place (sighs).<Participant 15>
The participants reported that, in the case of conscious patients who decided not to receive life-sustaining treatments, they built rapport by having conversations with the patients and their families from before the last days of the patients, empathized a lot while hearing about not only the patients' diseases but also the story of their life leading up to their hospital admission and came to understand the totality of life of a human being. The participant stated that nursing the dying patients while they were alive, staying by their side at the moment of death, and providing care until after death felt like being the last witnesses of life and death in the course of a person's life. As the last people who shared the time, space, and mind with the patients, looking after their physical condition until the very end, the participants felt a sense of responsibility to aid a person to a comfortable death, and they mourned with the patients' families with compassion and sympathy for a person. In Chang-ho Ahn's painting "Sick Bay," a nurse staying by the bedside with a deceased woman's family even after the woman's passing is depicted.
There was an end-stage renal cancer patient who decided to suspend life-sustaining treatments. He was conscious, so we talked together while he was alive and formed a rapport. When I listened to his life stories, he was meeting me at the end of his entire life. When he passes away, I will be the one who saw him alive and deceased and the last nurse he sees before passing, and he will remember me in the afterlife. I am m grateful to be able to be part of that person's life and to be of help. <Participant 3>
The participants stated that they were sad as they prepared for the deaths of patients, just like the members of the dying patients' families. They said they were placed in the center of the family and joined the post-decision processes by providing detailed explanations and guidance, particularly when the families lacked the understanding of the doctor's explanation of the limitations of medical practice when contemplating the suspension of life-sustaining treatments or were flummoxed by the guilt of deciding on the suspension of life-sustaining treatment. In some cases, the participants contacted the families of the dying patients to inform them about the imminent death and stayed by the patients' side while waiting for the family members to arrive. This way, the participants became family, though they were not the real family of the dying patients. Munch's works "Death in the Sickroom" and "By the Deathbed" depict the shock and grief of death of a family caused by the daughter's death.
When a patient's family members decided to suspend life-sustaining treatments for the patient and went home, the patient suddenly deteriorated. Death was imminent, and the patient was transferred into a treatment room, but there was only a care worker and no guardians. The patient passed away while the guardian was coming. When the family arrived, they regretted suspending life-sustaining treatments because of the sudden death, so I comforted them and explained the situation. It was a very memorable death because I stayed with the patient during the last moments instead of the patient's guardian. It was remorseful and lonely that the patient received death alone. <Participant 6>
The participants also considered the death of themselves, their friends, spouses, and parents while watching the patients who passed away after deciding to suspend life-sustaining treatments. They said that they thought about the family who would be left behind after their own death when seeing the families left behind by the deceased patients and that it was as if they were rehearsing their own death. As they thought about their own good death, they hoped that they would be able to take charge of their own death by making proactive choices and decisions. They wished for a dignified and good death where they could wrap up the final moments with the whole family and acquaintances, say farewells, and receive death with the send-off of the family.
I want to prepare the decision on the suspension of life-sustaining treatments in advance when I am alive and conscious, and when I die, I want the funeral home to have a festive atmosphere as in the movie'Sunny,' and I want my headstone to read 'I had a good time.' I want to be happy, have fun doing everything I want to do, live without regret, and leave in the company of family and acquaintances. <Participant 5>
The participants said that everyone was bound to die one day and that they had come to profoundly understand the singleness of life. In particular, they said that as they saw deaths of patients who suspended life-sustaining treatments, they thought first to prepare the letter of intent for life-sustaining treatments, prepare for the unknown death, and get along well with their family and acquaintances. While patient deaths marked the end of a person's life, the participants reported that the deaths were opportunities for them to pause, reflect, look back on their lives so far, and restart. Hae-in Lee's poem "Ash Wednesday" also expresses a new learning of life in the face of death.
The experiences related to death while working at the hospital hugely impact my philosophy and meaning of life. Thinking that I could die at any time, I become faithful to the moment. I have become a realist watching patients who decided to suspend life-sustaining treatments, and sometimes I think I want to live like those who live the You Only Live Once (YOLO) life. I think one should not focus too much on the future; this moment is important enough, and if there is something good to remember, you should make the memory now (shows photos of travels on the phone). So I travel with my parents to make lots of memories. <Participant 15>
The participants said that although they experienced extreme stress from providing end-of-life care for patients who decided to suspend life-sustaining treatments, the relationship between the patients and the families at the end of the patients' lives made them realize the value of the participants' own lives and the importance of the role of a nurse. They said that the more they experienced patient death, the more they felt that they grew as a nurse, feeling proud of their own act of caring and being considerate with deep concern for the dying patients and their families. They reported that, as nurses who witness death most frequently, they reconstructed the meaning of life in a positive sense that conforms to reality rather than assigning negative meanings to these experiences, rediscovered themselves as nurses, and took the experience as an opportunity for maturity and growth as a human being and as a professional nurse.
I also feel proud of my profession as a nurse as I experience patient deaths. I intervene in the death of a person, help families, and send patients comfortably to the afterlife. The role of a nurse is especially important to patients who have suspended life-sustaining treatments and their families. Because death can be neglected if something is done wrong, more attention to patient discomfort is necessary, and it is also a big role to explain the meaning of the suspension of life-sustaining treatments to families. Families are very appreciative when I accompany them in the process of end of life. It's difficult for those who leave, but it's also difficult for those who are left behind. I think the role of a nurse there is immense (smiles).<Participant 12>
Based on the meanings revealed through hermeneutic phenomenological reflection, the story of the self-reflection experience of general nurses who decided to suspend life-sustaining treatments was composed as follows.
The participants thought that they must maintain a sound body until death as they looked at wrecked bodies on which medical treatments were suspended after so much struggle due to the delayed decision to suspend life-sustaining treatments after the realization that recovery was impossible despite all kinds of medical treatments and procedures for the final resuscitation at the end of patients' lives. They also felt compassion and pity for the irremediable bodies as they looked at lives sustained by all types of medical equipment and wished that the patients would pass away in peace, free from physical pain, while watching patients die in physical pain. They thought of the pain experienced by patients due to passive medical interventions upon the suspension of life-sustaining treatments as a new form of torture in the face of uncertain time waiting for death, believed it necessary to modify the intervention in this regard, through which the patients could receive a comfortable death, and reflected on what choices could be made in their own coming death.
Reflecting on the fear caused by the shock and confusion from deaths during the days as a new nurse and on the guilt of being unable to secure dignified deaths due to immature nursing, such burden had led them to the anguish of wanting to avoid patients' undetermined time of death. However, as they became experienced nurses with the passing time and became familiar with life that always accompanied death, they came to have a feeling that seeing the death of a patient is as seeing one's own and of one's family and tried to care for patients at the end of life at the best of their abilities.
The participants experienced hospitals as a place of physical death but not dignified death, as a place where birth, old age, illness, and death intersect and has duplexities of birth and death and of death and prolonged life after resuscitating patients in the face of death. They were deeply disheartened and regretful about the environment of medical institutions where patients cannot welcome a quiet and dignified death with their families in a separate area in the moment of death and argued that there must be end-of-life room.
The participants nursed patients at the end of life while they were alive, during their passing, and even after death. They felt the responsibility to aid a person in receiving a comfortable death as the person who looks after the physical condition and shares time, space, and mind until the very last, had compassion and sympathy for a person, and mourned with the deceased's family with empathy. Moreover, they became families of patients as they cared for the dying patients and their families, and they also projected their own death. As such, through the experience, the participants aimed to live a positive life that conforms to reality during the given time of life. As nurses who witness death most frequently, they looked back on their lives so far and reconstructed the meaning of life in a positive rather than in a negative light, and are now maturing and growing as human beings and as professional nurses.
This study attempted to explore the nature and meaning of general ward nurses' experiences of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments by applying van Manen's hermeneutic phenomenological research method.
The theme that emerged concerning lived body was "hoping to return to an undamaged body and knowing the preciousness of the body." In other words, the participants reflected that it is a natural process of human life to return to its original form, like at birth, rather than the damaged body at death. Koh et al. [28] saw a body having a different appearance from the original body at the time of death due to the damages done by life-sustaining treatments as a death in which its dignity is violated. Jo [29] also claimed that it is difficult to see a person without consciousness whose survival relies on a mechanical device as a true human being, consistent with the reflections of the participants. Physicians perform various medical treatments in their best effort to save the life of a patient when death is imminent, but in the end, it takes away the control of death from the patient with blurred consciousness and devastates the patient's body [30]. Ridder [31] referred to patients who rely on mechanical respirators due to indiscriminate medical interventions and do not receive any respect as human beings as "medical crafts." The participants ruminated over how pointless it is that patients' bodies are damaged by life-sustaining treatments and procedures and their lives are maintained using various machines on their last days. The participants believed that patients should prepare the letter of intent for life-sustaining treatments in advance and be able to have control over deciding whether to receive life-sustaining treatments and choose their death in the face of death. However, their bodies were already ruined by the delayed suspension of life-sustaining treatments. The participants felt the preciousness of their bodies while watching the thoroughly damaged bodies of patients and wished to die in their original bodies without a scratch, having maintained their wholly intact bodies as they were born. Conflict is felt whether life-sustaining treatment should be discontinued for a dignified death instead of such meaningless life-sustaining treatment. For patients who decided to discontinue life-sustaining treatment, only fluid therapy, oxygen therapy, and the use of minimal auxiliary pain relievers seemed to lead to a more painful death, which was regarded as a new type of torture. Medical staff's defensive behavior regarding the accountability for changes in patient status due to the limitations on maximum oxygen therapy in place of ventilators, restrictions on fluids that can be used in the state of electrolyte imbalance, the administration of painkillers that must observe time intervals, and frequent overdose eventually led to pain for dying patients. Jo [32] also stated that the pain of maintaining life is greater; for instance, the faces and limbs of patients who suspended life-sustaining treatments swell, and their original appearance deforms over time. The participants called out the need to discuss in-depth the appropriate timing for deciding to suspend life-sustaining treatments for a dignified death, as well as the task to reduce patients' physical pain in a more proactive direction and to allow a comfortable yet dignified death.
The theme that appeared pertaining to lived time was "realize that the ability to care for the dying patient becomes more mature with the increase in career." But it is impossible to discuss the theme as there are no studies on new nurses providing end-of-life care for patients who decided to suspend life-sustaining treatments. Nevertheless, as revealed in previous studies, new nurses had negative experiences such as hypersensitivity, helplessness, stress, guilt, instability, frustration, pushback, and anger when they watched dying patients [33]. Additionally, the new nurses' lack of knowledge on end-of-life care and lack of experience in the situation when they experienced caring for dying patients for the first time led to shock and fear. Because of the fear of death and the immense burden of caring for dying patients, the nurses even felt relief when patients at the end of life passed away before or after their shift or were discharged and returned to their homes [34]. However, as time passed, the participants became capable of terminal care while learning about end-of-life care from senior nurses. That is, the participants became experienced nurses, accumulated experiential knowledge on end-of-life care, and gained an understanding of the patients at the end of life and their families and the ability to provide end-of-life care. Participants had felt apologetic and guilty in their days as new nurses, thinking that patients' conditions deteriorated because of their inexperience in end-of-life care, and they strived to provide better end-of-life care by becoming experienced nurses. Most new nurses enter the clinical field without sufficient training on hospice or formalized education or training for death, including the suspension of life-sustaining treatments, during their undergraduate education. Currently, end-of-life patient care is an independent course in approximately 20% of schools and an elective in all others, and about three-fourths of nursing students received no or little training from field instructors during their practical [35]. Nurses in a study by Kim et al. [36] also mentioned the need for related education to solve the difficulties of end-of-life care. Therefore, in order to provide holistic care to patients and their families who have decided to suspend life-sustaining treatment from the time they were novice nurses, it is urgent to develop practical end-of-life nursing and interdisciplinary curricula suitable for Korean culture and related education.
The theme that emerged concerning lived space was "the death in the treatment room like a death on street makes regrettable the absence of end-of-life rooms." The space of a hospital connotes the function and meaning of the two sides of a coin, such as birth and death or resuscitation and expiry. The reality is that most medical institutions do not have end-of-life room, so patients pass away in treatment rooms. The participants were deeply saddened at the reality of a hospital space that could not secure dignified death due to the lack of rooms for spending one's last moments. Patients at the end of life are transferred to treatment rooms for a minimum of dignified death in an isolated space, but treatment rooms are not a space that ensures dignified death. They are merely a space where other patients and their caregivers cannot see the dreaded death. The participants thought of death in a treatment room as death on the road in a hospital because the space feels like a marketplace with the noises and all the medical staff coming and going. Ok and Yi [37] also compared treatment rooms to a place of execution because these treatment rooms are the place of death of patients. Now that death occurs frequently in hospitals, it is urgent to establish a private and separated space like a home for family members. Furthermore, while there are increasing cases of patients visiting hospitals as they approach the end of life due to family decisions regardless of the patients' will, previous studies have found that many prefer their home for the place of death where their loved ones can stay with them until the end [38]. A proactive collaboration with at-home hospice in the community is necessary so patients can die a dignified death at home.
The themes that were revealed in the context of lived relationship were "seeing the preciousness of my life in accompaniment with death" and "become aware of growing up as a professional nurse" It has been reported that the relationship between a patient facing death and the family is centered on the interaction between the patient and a nurse, comes to a state of emotional resonance, a high level of empathy through reflection and introspective thinking, and accompanies the patient as companions on the journey to the end [39]. The participants first recognized themselves in the relationships between dying patients and their families and then reflected on their relationships with family members and relatives. It was an opportunity to confirm their love for their families further, and they gained more consideration and understanding for others. Nurses should be holy and warm companions of souls who leave with human dignity in addition to serving the role of a medical practitioner [20], and reflecting on the final and dismal moments of their life together as medical practitioners will allow them to mature as medical practitioners and existential human beings. In this respect, it is necessary to set aside time to share experiences of end-of-life care and self-reflection through conferences in the ward to create empathy for dying patients and build positive end-of-life values.
Furthermore, the participants projected their own death through the patients' death and hoped for a self-directed death where they could comfortably welcome death surrounded by family and acquaintances. Such a death is in line with the "expression type for happy emotion" of good death introduced by Jo [29], which is to die a dignified death and end life warmly in the arms of the family without receiving meaningless end-of-life treatments. Death, like all afflictions, is clearly a painful thing, but it can be an opportunity to grow the dying patients or those who watch them [40]. Additionally, nurses with more experience with various and numerous deaths and life stories have more profound thoughts, which leads to growth and maturity in their lives [41, 42], and their professional and personal reflection on life can reveal transformation and growth in their lives and care philosophies [39]. Ultimately, being with patients at the end of life was an opportunity for the participants to rediscover themselves and the meaning of life, and they experienced growth. Accordingly, it will be necessary for the nurse to establish a true value of nursing that allows them to interpret life and discover the meaning of their lives through the death of patients, ponder the nature of human beings, and care for the end of life as a whole of a person who reached the end of the life. Based on the results of this study, nurses' experience of self-reflection on end-of-life care reduces nurses' exhaustion in terms of nursing practice and allows them to grow positively as specialized nurses. The results can also be utilized in developing nursing interventions for end-of-life patients who decided to suspend life-sustaining treatments to improve the care of patients who discontinued life-sustaining treatments. In addition, nurses can serve the role of facilitators by providing the correct information to dying patients and their families with accurate knowledge on the suspension of life-sustaining treatments, helping them make the optimal choice at the appropriate time to suspend life-sustaining treatments, and reducing the related psychological pressure and burden of dying patients' families. In terms of nursing education, adding education on life-sustaining treatments in job training programs for new nurses at the clinical site will help new nurses adapt well to these situations and reduce their death anxiety and end-of-life care stress. With regard to nursing research, the results of this study will be the basis for developing self-reflection programs that improve the emotional support and reflective thinking of nurses after caring for adult patients at the end of life in general wards.
This study is the first attempt at exploring general ward nurses' experience of self-reflection on end-of-life care for patients who decided to suspend life-sustaining treatments, and it has significance in that it explored the meaning and essence of self-reflection experiences and presented an in-depth understanding and diverse perspectives. Five essential themes and 14 sub-themes were derived as the result of the study. These derived themes provided an in-depth understanding of the general ward nurses' experience of end-of-life care for patients who decided to suspend life-sustaining treatments. To suspend life-sustaining treatments in practice, the patients, or their families when the patients are unconscious, decide and sign the life-sustaining treatment plan that entails the contents, such as CPR, hemodialysis, anti-cancer drug administration, and refusal to use a ventilator, at the discretion of the attending physician. Once the form for the suspension of life-sustaining treatments is signed, the only role of the physician is to prescribe pain medications and declare death, but nurses perform holistic nursing from basic physical nursing to spiritual nursing, along with nutrition and oxygen administration management. Additionally, guardians staying by the side of the patients at the end of life rely entirely on nurses due to anxiety and fear of death of their family members and frequently call for nurses, complaining of the imminence of death at even the subtlest changes of the dying patient. The nurses in charge of end-of-life patients experience exhaustion as they provide all instructions related to death, from the issuance of a death certificate to the procedure of using a funeral home, have the burden of caring for patients' families until the patients pass away, and care for other patients. Nurses caring for end-of-life patients who have completed the form for the suspension of life-sustaining treatment suggested through the discussion the educational and policy contents that should be provided for end-of-life patients and their families. The proposed content, including the development of a structured end-of-life nursing education program in the undergraduate curriculum, the establishment of end-of-life room in medical institutions, and the proactive vitalization of a home-linked hospice system, must be implemented to prepare for the dignified death of patients on the last days of their life.
The following are suggestions based on the results of the present study. The following are suggestions based on the results of the present study. First, it is believed that general ward nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments differs between novice and experienced nurses, and comparative analysis of such variance is necessary through in-depth research. Second, studies that can compare the commonalities and differences in nurses' experience of self-reflection on the experience of end-of-life care for patients who decided to suspend life-sustaining treatments according to the characteristics of clinical sites, such as hospital size, specialized intensive care units, hospice wards, or general wards, should be conducted. Third, practical training for end-of-life care of patients who decided to suspend life-sustaining treatments should be developed and systematically implemented within the curriculum, and nursing interventions for end-of-life patients appropriate for Korean culture should be developed.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - HHJ.
Data collection - HHJ.
Analysis and interpretation of the data - HHJ.
Drafting and critical revision of the manuscript - HHJ.
This manuscript is a condensed from of the first author's doctoral dissertation from Inha University.
 E-SUBMISSION
E-SUBMISSION