
Purpose
The purpose of the study was to describe andropause-related difficulties experienced by men.
Methods: Two focus group interviews were conducted to collect the data from 10 Participants with andropause-related difficulties experienced. All interviews were audio-recorded and transcribed verbatim. The data were analyzed using content analysis.
Results: We organized the responses concerning andropause symptoms into five essential categories: 1) uncontrollable physical changes, 2) intellectual decline, 3) changes in sexual function, 4) difficulties in controlling emotions, and 5) separation from society. The attempts to alleviate andropause were classified into seven distinct categories: 1) dietary modifications, 2) engaging in physical activities, 3) pursuing leisure and hobbies, 4) enhancing self-esteem and self-perception, 5) seeking support and comprehension from one's social circle, 6) utilizing informational resources concerning andropause, and 7) embracing and accepting andropause reality.
Conclusion: We analyzed the issues arising from andropause and the corresponding efforts to address them. A comprehensive understanding of andropause's causes, mechanisms, effective nursing interventions, and essential development of management programs, including education, is imperative.
The purpose of the study was to describe andropause-related difficulties experienced by men.
Two focus group interviews were conducted to collect the data from 10 Participants with andropause-related difficulties experienced. All interviews were audio-recorded and transcribed verbatim. The data were analyzed using content analysis.
We organized the responses concerning andropause symptoms into five essential categories: 1) uncontrollable physical changes, 2) intellectual decline, 3) changes in sexual function, 4) difficulties in controlling emotions, and 5) separation from society. The attempts to alleviate andropause were classified into seven distinct categories: 1) dietary modifications, 2) engaging in physical activities, 3) pursuing leisure and hobbies, 4) enhancing self-esteem and self-perception, 5) seeking support and comprehension from one's social circle, 6) utilizing informational resources concerning andropause, and 7) embracing and accepting andropause reality.
We analyzed the issues arising from andropause and the corresponding efforts to address them. A comprehensive understanding of andropause's causes, mechanisms, effective nursing interventions, and essential development of management programs, including education, is imperative.
According to the life table published by the National Statistical Office in 2020, life expectancy in Korea increased from 80.04 to 83.30 years, from 2009. Further, 40-year-old women and men, starting middle age, are predicted to live another 40 years or more [1]. During the human life cycle, middle age proceeding to old age has various effects on oneself, family, or social environments and carries on a stable life [2]. However, middle-aged men inevitably experience psychological, physical, psychiatric, and social changes, followed by gradually decreasing health as they prepare for retirement [2]. This may have negative effects in old age [3].
During middle age, it has been demonstrated that individual differences are clearly shown by various variables, such as the social environment, material resources, health, and various developmental patterns [4]. Since current life features and attitudes toward middle-aged men will affect their lives after middle age, exploring how they spend their middle-aged years will help them find a direction for a healthy life in the future.
Men have a high prevalence of chronic diseases caused by occupational stress and lifestyle-related diseases, such as hypertension, coronary artery disease, and diabetes, aggravated by drinking and smoking [5]. Additionally, it has been reported that a decrease in testosterone, a male hormone, increases the risk of andropause syndromes, such as nervousness, depression, decreased libido, changes in sexual behavior, emotional instability, hot flashes, sweating, and metabolic syndrome [5], which affect men's quality of life and health of older men [6]. Thus, if men do not adapt well to these changes, their health status, lifestyle, and quality of life in older age may deteriorate.
The quality of life after andropause depends on how successfully men manage physical and mental changes and adapt to loss [7]. Proper management of the physical and mental changes and symptoms of andropause can maintain their health and life after andropause and improve their quality of life [7]. Attention should be paid to health problems during andropause to ensure a happy and healthy life after middle age [8].
Diverse studies have been conducted on andropause in Korea. Studies have shown that stress and quality of life are the major variables of andropause [9, 10, 11]. Studies have focused on a sense of crisis in men with andropause [12], andropause syndrome, hormones, and drug treatment [13, 14], the effects of hormones, stress levels, and perceived symptoms of andropause [15], including andropause awareness studies [16]. However, they focus on the experience of andropause diseases are insufficient to help understand the challenges of andropause. Accordingly, an indepth study focusing on the difficulties of the andropause experience is required.
Focus group interviews were conducted to gain a comprehensive and in-depth understanding of andropauserelated difficulties experienced by men. Focus group interviews can obtain a wealth of focused data on psychosocial challenges that are otherwise difficult to observe [17]. Further, it is possible to collect data from various perspectives through interactions among group members [18]. This study aimed to comprehensively understand and grasp the difficulties experienced by men during "andropause" from a participant's perspective. Therefore, it is intended to be used as basic data to prepare specific measures for identifying and overcoming the difficulties experienced by men at an early stage of "andropause."
This qualitative research applied focus group interviews to understand and describe men's andropause experiences in depth.
To recruit candidates, we posted a research announcement in Seoul and Gangwon-do community cultural centers, and those who could explain their menopausal experiences were selected. The selection criteria were as follows.
Middle-aged men over 40 years of age who have experienced andropause based on the World Health Organization [19] and previous studies [20]. To identify andropause symptoms, we used 10 items: decreased libido, decreased energy, decreased physical strength and endurance, decreased height (height), decreased enjoyment of life, depression or irritability, decreased erectile function, decreased exercise capacity, lethargy, and decreased work performance. A dichotomous scale, just answering "yes" or "no," was used. We decided to have the andropause when a "yes" reply on decreased libido or decrease in erectile function or more than three "yes" from remnant eight items [20].
A total of 10 men agreed to participate in this study after being informed about the study and the focus group interview. A comfortable and productive conversation is the key to success in organizing focus groups [17]. Therefore, during the interviews, the same men were organized into the same group according to their region to ensure a smooth conversation between them. Although a typical focus group size is preferably 7 to 10 individuals [17], each group included five men in this study. Two focus groups were formed, one organized in each community.
We collected data from each of the five participants: the first group on March 28, 2023, and the second group on April 11, 2023; the first group resided in City S; and the second group resided in City C. The interviews started at a convenient time for the candidates, and the venue was a rented seminar room of a community organization where the participants lived. The duration of the interviews ranged from 2 h to 2 h, 30 min per session.
At the beginning of each interview, the researcher clarified the purpose of the study and asked semi-structured questions. To avoid deviations from the purpose of the study, introductory and transition question guides were developed and used.
The opening question was, "What do you think about andropause?" The introductory question was, "How did you experience andropause?" while the transitional question was, "Have you overcome andropause?" with the key questions, "What were your perceptions and emotions when you experienced andropause?" and "What were the conflicts and difficulties you felt while experiencing andropause?" The closing questions were, "Do you have a way to manage andropause?" "How did you overcome andropause?" and "What is the most important method to achieve this?" By inducing participant's thoughts about andropause naturally, questions were asked about their andropause experiences, feelings and perceptions of andropause experiences, conflicts, and difficulties, and finally, they were asked how to overcome and manage andropause.
Focus group interviews were conducted by a researcher with sufficient experience in qualitative research and who had taught nursing methodology and qualitative research at a college. The researcher secured the locations and was in charge of recording. Data analysis from the first interview was completed before the second interview to ensure it could serve as a guide for the second interview. Based on thematic analysis after the two interviews, it was confirmed that the statements were repeatedly categorized and the data were saturated.
The Research Ethics Committee of S Hospital in City S approved this study (Approval No. DGU-IRB-20190021). Before data collection, the researcher informed the participants about the purpose of the research, confidentiality, no direct compensation or risk, their right to not respond to the research questions according to their free will, and the possibility of withdrawal during participation. After obtaining written informed consent from the participants, interviews were conducted. All interviews were recorded, and the recordings were paused whenever they did not want to be recorded. The data transcribed from the recordings were randomly assigned an anonymized number so the participant could not be identified. The participant's ethics were considered by explaining that anonymity would be ensured even at the risk of unexpectedly revealing information.
The collected data were analyzed using the content analysis method suggested by Elo and Kyngas [21]. This study generalized the participants' experiences by identifying and categorizing common elements from specific and individual facts about health problems revealed through the interviews.
Based on the content analysis procedure, words or phrases were selected as analysis units in the preparation stage. A detailed data analysis procedure in the organizing stage followed open coding, category formation, and abstraction [21]. First, the essential content and flow of the overall interview were understood through repeated reading of the transcribed data. Second, codes were extracted from repeated words or phrases by cross-checking the transcripts. Third, we reviewed the organized codes and categorized them by grouping and comparing their characteristics. Fourth, the categorical contents were confirmed, and the naming task was repeated to encompass their meaning and relevance. Finally, abstracted categories reflecting the core content and relevance of the categorized interviews were organized to describe the phenomena that met the purpose of the study. Furthermore, an attempt was made to clarify the concepts related to the derived topics by organizing tables and confirming the validity and appropriateness of the data analysis.
According to the rigorous standards of qualitative research presented by Guba and Lincoln [22], we referenced the item's truth value, consistency, applicability, and neutrality to ensure the reliability and validity of the study. First, a focus group interview was conducted with middle-aged men from the local community to secure the truth value. Furthermore, the researcher recorded and summarized the oral statements during the interview and checked whether the contents matched those of the interviewed men. The interviews were transcribed verbatim and later confirmed by interviewees. Second, to meet the standard of consistency, the researchers followed the content analysis method of Elo and Kyngas [21] throughout the entire data analysis process and continuously shared the records and contents of the process. The detailed contents of each stage of the research process were described, and all statements of the researcher, applied to the subcategories, were quoted in the summary of the final data analysis.
Furthermore, this researcher, who used many qualitative research methods, including focus group interviews, conducted the data collection and analysis to ensure consistency. Third, in terms of applicability, the characteristics of the participants were summarized and described according to the general characteristics of the survey conducted before the focus group interview. In ensuring applicability, the results were reviewed with three middle-aged men who did not participate in the interview, and the possibility of empathy and repeated research was confirmed.
Finally, to secure research neutrality, the two researchers maintained a value-neutral attitude throughout the research process, continuing discussion and agreement on all interim and final results derived from field notes or transcripts. Based on a mutual understanding, the researchers tried to minimize individual biases.
A total of 10 men who had experienced andropause participated in the study. One person was 49 years old, five were between the age of 50~54, three were between 55~60 years, and one was 61-years-old. The average work experience of the participants was 23 years and three months (18~31 years). Four were employed and six were unemployed. Eight were college graduates and two were high school graduates. Seven were married, two were divorced, and one was bereaved. Hypertension and diabetes were diagnosed in seven and four (Table 1).
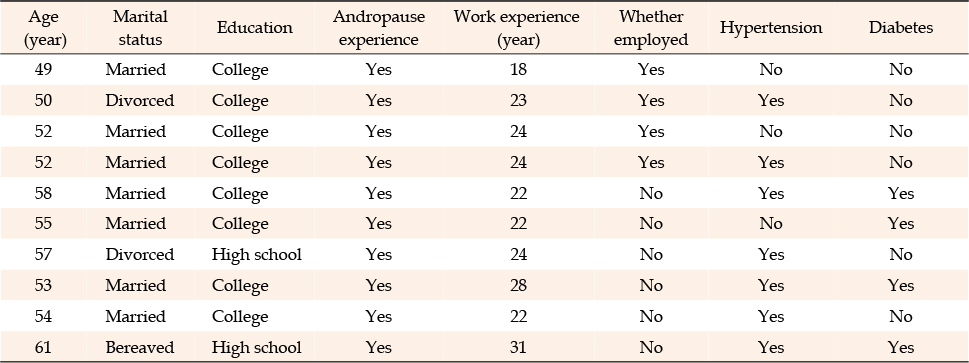
Table 1
General Characteristics of the Participants (N=10)
A total of 43 codes were generated from the content analysis of the transcribed data, and we created 19 subcategories according to their relevance: 1) Fear of body changes; 2) insomnia; 3) enuresis; 4) changes in body hair; 5) loss of memory; 6) loss of sexual interest; 7) meaninglessness of life; 8) helplessness and depression; 9) increased anger; 10) accumulation of stress; 11) hiding one's changes; 12) feeling lonely in a dark world; 13) dietary modifications; 14) engaging in physical activities; 15) pursuing leisure and hobbies; 16) enhancing self-esteem and self-perception; 17) seeking support and comprehension from one's social circle; 18) utilizing informational resources concerning andropause; and 19) embracing and accepting andropause reality. Simultaneously, the six categories were: 1. Uncontrollable physical changes, 2. intellectual decline, 3. changes in sexual function, 4. difficulties in controlling emotions, 5. separation from society, and 6. attempts to overcome andropause. These subcategories are further divided into five essential categories (Table 2).
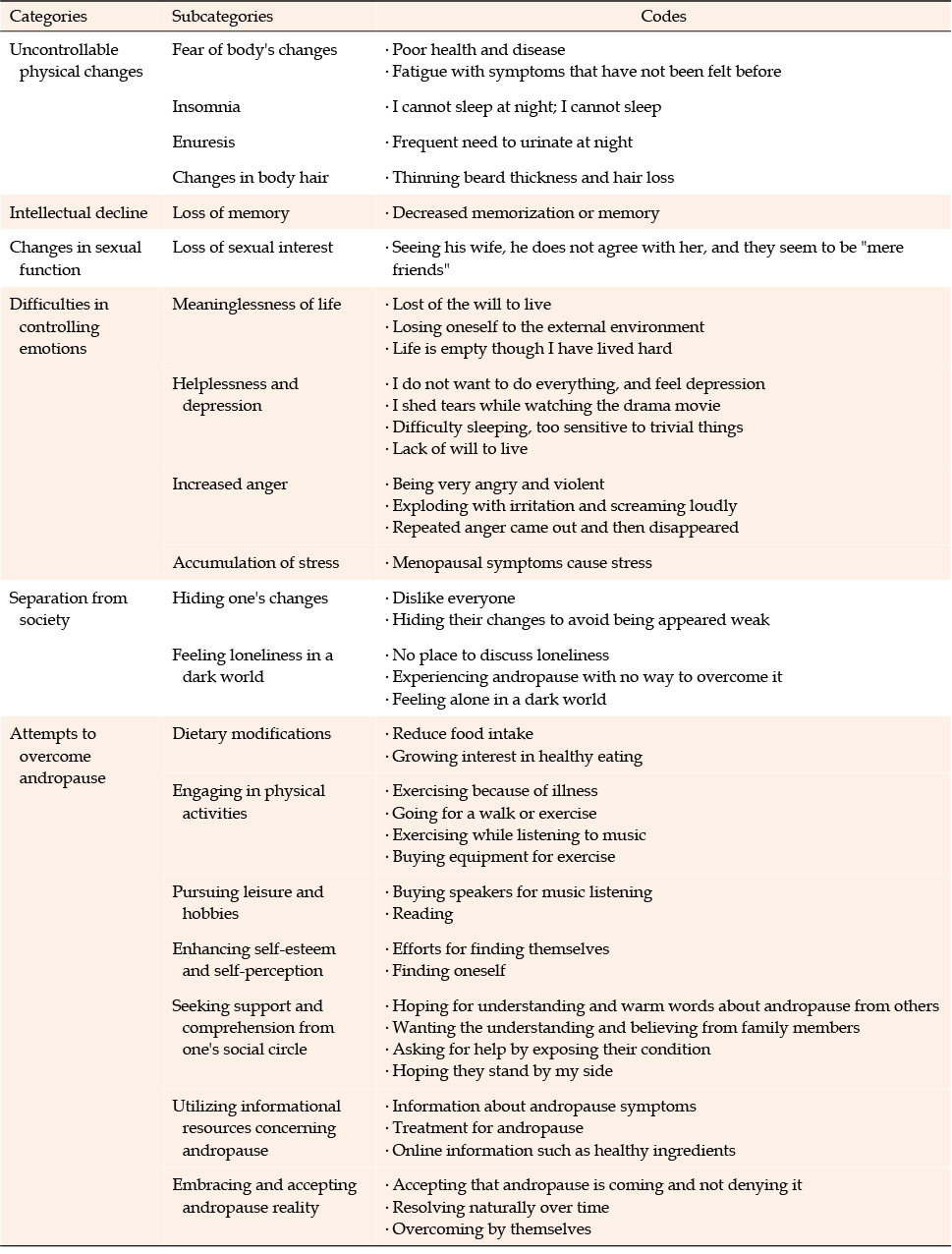
Table 2
Andropause, as Experienced by the Participants
Four subcategories and five codes were derived from the uncontrollable changes in the body, and they were expressed as "fear of body changes," "insomnia," "enuresis," and "changes in body hair." It turned out that the pharisaical changes occurred after andropause. This has an overall impact on the daily life and work. Some of them could not sleep because of insomnia and enuresis, so they had to stop working and take breaks when they felt uncomfortable in their daily lives. In particular, they suffered more serious changes in their body hair and lost confidence in their manhood.
As men grow older, various diseases develop, and they feel that their health gradually deteriorates. Symptoms they did not previously have appeared, and they felt fear and tiredness about ageing.
• Poor health and disease
My body is more uncomfortable than before, it hurts here and there, how will it change when I get old? I am afraid too... Now only a useless body will remain... (Group 2-A)
• Fatigue with symptoms that have not been felt before
I do not know if it is andropause, but maybe it is because I am getting older, and symptoms I did not feel before appear, affecting my life. Nonetheless, it is a little better if I rest well on the weekend.. However, I get tired because my family keeps asking me to go somewhere on the weekend! (Group 2-B)
Some participants could not sleep at night or fell asleep late, so they were always tired.
• I cannot sleep at night; I cannot sleep!
I cannot sleep at night; therefore, I wonder if I am going through andropause. On such days, I lose sleep. I sometimes go to bed past 3 A.M. I am going crazy because I cannot sleep. I am so tired because I cannot sleep. (Group 2-D)
Some patients complained of changes in urinary function, such as waking up frequently at night to urinate.
• Frequent need to urinate at night
I did not do that before, but I think I wet the bed once in my sleep. Having to wake up with a lot of urine... (Group 2-E)
The participants in the study demonstrated changes in beard thickness and hair loss.
• Thinning beard thickness and hair loss
I think these days my beard is getting thinner and my hair is getting shorter. (Group 2-B)
One subcategory and one code were derived from the decline in intellectual ability. The subcategory was "gradual loss of memory." The participants experienced several challenges in daily life due to memory loss, which is a symptom of andropause. They were confused by injuries from family members and difficulties at work due to memory loss.
The participants complained that their families blamed them for poor memory and that they could not remember something if they did not write it down.
• Decreased memorization or memory
I was blamed a lot by my family due to forgetting. I feel like my stamina is gradually disappearing. In the past, memorization was very good, but it is difficult to write it down on a cellular phone these days. (Group 2-A)
For sexual change, one subcategory and one code were derived; the subcategory was "declining sexual interest." The participants were aware that their sexual desire had changed during andropause because of changes in sexual function, and they experienced difficulties in marital relationships.
The participants in the study recognized that their sexual interest had decreased because they felt like friends and did not show interest in sex, even when they saw their wives.
• Seeing his wife, he does not agree with her, and they seem to be "mere friends."
They say that andropause also causes problems related to sex. I do not feel the same when I look at my wife. I only see her as I would a mere friend, not a sexual partner. The friend you live with. (Group 1-C)
Challenges in controlling emotions were derived from four subcategories, including "meaninglessness in life," "helplessness and depression," "increased anger," and "accumulation of stress" and 11 codes. All participants experienced negative emotions throughout the entire process of perceiving andropause symptoms. They encountered various emotions such as embarrassment, anxiety, denial, anger, sadness, depression, disappointment, and frustration when their andropause appeared.
One of the participants suddenly questioned why he should live and had suicidal thoughts and feelings similar to those of adolescents. Although he lived a hard and diligent life, he felt a sense of losing himself when he perceived his diminished external environment.
• Loss of the will to live
What? Suicide? Suddenly it comes up in my thoughts from time to time. (Group 1-D)
• Losing oneself to the external environments
I think andropause is the same as puberty, like losing myself in the external environment. I think it is important not to lose myself no matter what I do... (Group 2-D)
• Life is empty though I have lived hard
I just think so. Why should I have lived such a hard life? Why did I do that? This might have made me feel emptiness. (Group 1-E)
The participants felt depressed over trivial things, such as crying while watching dramas, experienced emotional changes without their perception, and became sensitive and lethargic to trivial things.
• I do not want to do everything, and feel depressed
I hate doing anything. I was depressed. It has been a month. I could not find any answer to this for a month. There should be no more depression. (Group 1-D)
• I shed tears while watching a drama movie
I cry a lot these days while watching dramas. Last time, my wife mocked me at that time, but strangely, tears came out without my knowledge. (Group 2-A)
• Difficulty sleeping, too sensitive to trivial things
I become sensitive to trivial things, and I cannot overcome it. I cannot sleep for a day or two. (Group 1-E)
• Lack of will to live
My wife gave up on us because I had no will to live... (Group 1-D)
The participants could not tolerate trivial things, showing violent changes, becoming angry, and shouting. They repeatedly demonstrated aspects of rough, cursing, anger, and then disappearing.
• Being very angry and violent
On the contrary, my wife blamed me for getting angry a lot. What made me violent? (Group 2-D)
• Exploding with irritation and screaming loudly
I was yelling at myself while working, it started with a low tone, but now I scream so much that it may hurt my throat! (Group 1-D)
• Repeated anger came out and then disappeared
I felt that the anger suddenly came out, then disappeared completely. I have not experienced such feelings before, but it disappeared completely, then showed up again. (Group 1-B)
• Menopausal symptoms cause stress
The participants thought that the accumulation of daily stress caused andropause.
I seem to be even more stressful, with increasing body changes! (Group 1-D)
Separation from society was derived from two subcategories, "hiding one's changes" and "being alone in a dark world," and five codes.
As thinking and worrying about their emotional changes increased, the participants did not want to discuss or hide their emotional changes, even when it was the main topic of their talk at work, to avoid the fear of appearing weak or becoming weak.
• Disliking everyone
I knew it was all on me, and it was over. I did not even talk about it because I abhorred talking itself at that time.. (Group 1-D)
• Hiding their changes to avoid appearing weak
I do not even talk about it at work... If my weak side were exposed to the outside, it would be used against me as my weak point; therefore, I must hide it well... (Group 2-E)
The participants were aware that they were in andropause when they felt trapped in a dark world alone, without any support from their families.
• No place to discuss loneliness
I am lonely, but I have no one to talk about this with. I wanted to be encouraged by my family, but I cannot start it. (Group 2-F)
• Experiencing andropause with no way to overcome it
I knew how hard it was to survive without any way to overcome it, even just for one month. (Group 1-D)
• Feeling alone in a dark world
I felt alone in a dark world of my own. I could not see anyone around me at all (Group 1-D)
Attempts to overcome andropause were derived from seven subcategories, "dietary modifications," "engaging in physical activities," "pursuing leisure and hobbies," "enhancing self-esteem and self-perception," "seeking support and comprehension from one's social circle," "utilizing informational resources concerning andropause," and "embracing and accepting andropause reality." They tried to manage their health by improving their basic lifestyle to overcome andropause. It was confirmed that they could overcome andropause by asking for help from people around them, increasing their self-esteem, and accepting andropause.
They try to be healthy by reducing the amount of food consumed to prevent disease or by learning to cook healthy foods, which creates new relationships with their family members.
• Reducing food intake
I tried to reduce the amount of food because I was suffering from hyperlipidemia. (Group 2-A)
• Growing interest in healthy eating
As I learn and practice healthy cooking with my family, our relationship is improving, and my health too! (Group 1-A)
When the participants had a family history or suffered from illnesses such as diabetes or angina, they started to walk with their wives, talk, listen to music, and exercise. They wanted to be healthy both physically and mentally.
• Exercising because of illness
I am also taking care of this body in my way since I received the diagnosis of DM from routine health check-ups. (Group 1-B)
• Going for a walk or exercise
I have gone for a walk these days. I thought doing it with someone else would be better, so I suggested my wife go with me. At first, I tried to walk quickly, but my wife could not catch up, and I found myself walking alone. Therefore, now I walk more slowly along with her for a longer time. Then we walked together and talked about this and that, and my body felt much lighter and nicer. (Group 2-B)
• Exercising while listening to music
I have a hobby of music listening, especially operas. I like opera, so whenever I walk or run on a treadmill, I turn on the CD or DVD during the exercise. (Group 2-D)
• Buying equipment for exercise
I used to do squats and attend gym sessions. Fortunately, I was lucky enough to buy full equipment (Group 2-F)
Participants purchased the speakers themselves. They appeased their emptiness through hobbies, such as listening to music or reading.
• Buying speakers for music listening
Furthermore, I feel like I did nothing with my money for myself all through my life. It was the emptiness that made me do something for myself. Then I bought a pair of speakers to listen to my favorite music! (Group 2-D)
• Reading
I guess... Reading seems to enrich me... (Group 1-B)
The participants were trying to get the assurance that they would not be shaken by their body changes, even though they were getting older.
• Efforts for finding themselves
I think it is important to raise my self-esteem; I think it is so important for me to find the assurance that hormones will not shake me. I have lived that way all my life (Group 2-A)
• Finding oneself
As I am getting older and more difficult, I have tried to read more books and find myself! (Group 2-D)
The participants wanted their family members to be gentle and warm, say warm and kind words, stay quietly and comfortably by their side, and understand and trust them without blaming them. They also claimed that it was necessary to ask for help when in trouble.
• Hoping for understanding and warm words about andropause from others
I am experiencing andropause and hard times. Why are they not offering me words of comfort and being nice to me, rather than scolding me for andropause? (Group 1-C)
If they hug me warmly like this, then it would be helpful, and it will give me strength.. They said to me that andropause is not a scary disease, it is not a disease. (Group 1-B)
• Wanting the understanding and belief of family members
I want my family to believe what I am saying or trying to say! It is my family. Why should I have another ulterior motive and hide my intention? I do not want to be criticized even by my family! (Group 2-B)
• Asking for help by exposing their condition
It is good that you let them know about my condition. I think I will be rewarded with their help. It is a good feeling that they will take care of me (Group 1-B)
• Hoping they stand by my side
I do not want them to pay attention to me. I want them to stand by me. That will be the best. Just let me be comfortable and still, just leave me alone. (Group 1-E)
The participants did not know much about andropause and its symptoms, medication, or treatments, and they thought that they needed treatment, such as hormone therapy. They searched the Internet to obtain health-related information, such as healthy ingredients.
• Information about andropause symptoms
I think men do not know well about andropause symptoms. Thus, it would be nice if andropause is confirmed through the andropause symptom check or explanation of the symptoms? (Group 2-A)
• Treatments for andropause
I heard that women receive hormone treatment during menopause, and I think we also sometimes need this kind of treatment. (Group 2-D)
We talked about urology earlier, but it would be nice to have information about medicines and treatments... (Group 2-E)
• Online information, such as health ingredients
We searched the Internet together to find healthy ingredients, and these days, we bake our bread at home with gluten-free flour and bananas (Group 2-A)
Participants claimed that andropause is an unavoidable phenomenon that can occur in anyone. It should not be denied but should be accepted and overcome by oneself, although it may resolve naturally over time.
• Accepting that andropause is coming and not denying it
It seems impossible to avoid it, but it is inevitable because it can come to anyone! (Group 1-B)
Maybe it is due to the hormone that made my body ache here and there, and my body is not the same as before. I feel uncomfortable, but I must accept that it is the time to come. Would not it be more difficult for me if I denied it? (Group 2-A)
• Resolving naturally over time
Andropause comes two times lasting four hours each, and it resolves itself naturally about one month after. (Group 1-D)
When the andropause passed, I experienced similar feelings that come after overcoming a severe cold. I felt that my body is getting lighter. (Group 1-D)
• Overcoming by themselves
Andropause is the problem of nothing but self! Then what should I do? I know I have to overcome it (Group 1-B)
This study was conducted to provide a comprehensive and in-depth understanding of andropause difficulties using the coping strategies experienced by men. The essential themes of andropause experiences were an uncontrollable body, decline in intellectual ability, changes in sexual function, difficulty in emotion control, and finding ways to overcome andropause.
It was confirmed that the participants had a difficult time at first, with various changes, and experienced negative feelings during the andropause experience. However, these experiences could be improved through andropause coping methods. Jeon and Kim [4] confirmed the results of physical changes, psychological changes, changes in work performance, and overcoming andropause, which are similar to the results of this study. If the basic causes of these changes in andropause are identified, and ways to manage andropause are suggested, it will significantly help individuals with andropause.
The first topic was uncontrolled physical changes; the subtopics were fear, insomnia, enuresis, and changes in body hair. In a study of middle-aged men's andropause experiences, Jeon and Kim [4] identified uncontrolled physical changes as the main topic and confirmed subtopics such as changes in body shape and physiological changes that were different than before. These results are consistent with those of the present study. Furthermore, in a study by Kim [23], middle-aged men precepted andropause with feelings such as, "lost vitality," "decreased energy," and "not as good as before," because of their physical changes comparing their younger days. This finding is consistent with the results of the present study. Physical changes such as andropause symptoms appear according to men's biological changes, and guidance on men's physical change and management is needed. Min and Kang [24] confirmed that men may not recognize andropause and that this ignorance is recognized as a risk factor for their health. When evaluating men's health, it is necessary to identify the symptoms of andropause syndrome and approach them to alleviate them.
The second topic was the decline in intellectual ability. This phenomenon has been identified as a subtopic of gradual memory loss. In this study, the participants experienced changes in cognitive function and deterioration in memory or concentration and recognized these important factors. Andropause is a condition that affects cognitive function, causing memory loss and concentration difficulties. These changes significantly affect the quality of life. Men with these symptoms may experience problems that affect their daily work or social activities [24]. Therefore, additional studies on the relationship between andropause and testosterone levels are required. Further, developing interventional methods that improve cognitive function, including lifestyle habits, medications, and treatment modalities, is important.
The third topic was changes in sexual function, and the subtopic was confirmed to be a decrease in sexual interest. Jeon and Kim [4] identified a decrease in sexual function as a subtopic. The most common changes caused by andropause are erectile dysfunction and reduced or difficulties in marital relationships. These changes in sexual function are recognized as the most significant changes in andropause. Seo et al. [25] also reported that andropause symptoms significantly influenced spouses and their sexual lives, which is consistent with the results of this study. According to Ha [26], a good relationship with their spouse is an important factor affecting life satisfaction in men. Hence, it is important to develop guidelines that will help men understand the relationship between testosterone levels and sexual function during the aging process. Moreover, for these participants, effective treatment and intervention for andropause sexual dysfunction are needed.
The fourth topic was difficulty in controlling emotions. Andropause is a gradual decline in testosterone levels in older men [9]. Although not all men experience andropause symptoms, some experience various emotional changes during andropause [9]. In this study, symptoms such as hiding one's changes, meaninglessness of life, helplessness, depression, feeling lonely in a dark world, increasing anger, and increasing stress were confirmed. Heo and Im [27] also expressed emotional changes during andropause, such as depression, irritation, and anger. Jo and Seong [9] suggested combining lifestyle changes and medical treatment to manage emotional changes during andropause. Hence, medical staff and nurses should be acquainted with the intervention method for individual nursing guides that support and help emotional changes during andropause, and the participants should cooperate with medical service providers to manage their andropause.
The fifth topic was separation from society; the subtopics were hiding andropausal changes about oneself and feeling lonely in a dark world. All human beings interact with others, and nobody can be free from the eyes of others [2]. In this study, unlike women, men evaluated their diseases based on distorted standards regarding their andropause experience. Further, they experience more difficulties in finding themselves in andropause. In particular, they experience psychosocial difficulties because they would hide and do not talk about their changes, even to family or friends with whom they frequently interact. Hence, to solve these men's social difficulties, it is necessary to introduce appropriate guidelines and knowledge about andropause. Simultaneously, educational counseling is needed to help participants develop the ability to deal with social prejudice and attitudes.
The sixth topic concerns finding ways to overcome andropause. The subtopics were adjusting diet, going for a walk or exercise, engaging in hobbies, increasing self-esteem, understanding and asking for help from people around them, using information about andropause, and accepting andropause. Among previous studies on andropause, Jeon and Kim [4] and Kim and Kim [28] explained that the factors improving men's quality of life and overcoming crises were peer understanding, requesting help, regular exercise, health maintenance, and information utilization. These results are consistent with those of the present study. Medical and psychological interventions are needed to reduce andropause syndrome in men. Furthermore, support on social and national levels are needed to increase men's physical and mental stability during andropause. Furthermore, it is necessary to implement a systematic andropause management program to promote men's health to overcome andropause and reach a healthy old age.
This study confirmed that andropause is important in men's health and lives. Hence, this study is meaningful because it provides basic data based on andropause experiences for developing a systematic andropause management program. Furthermore, this study suggests that a continuous and systematic education program is needed to manage andropause in male participants experiencing andropause.
This study selected participants based on the presence or absence of andropause symptoms. There were limitations in detailing the period of andropause experience, types of treatment, and overcoming processes. In the future, in-depth studies on symptoms, treatment contents, and overcoming processes are needed according to age.
This study investigated the difficulties experienced by middle-aged men during andropause using focus group interviews. The findings of this study yielded a set of representative themes, including "uncontrollable physical changes," "intellectual decline," "changes in sexual function," "difficulties in controlling emotions," and "separation from society."
Research has substantiated that middle-aged men undergoing andropause encounter a range of challenges markedly, from physical and psychological changes to alteration of sexual or cognitive function. Middle-aged men adapted various coping strategies to overcome andropause independently. They embraced the changes associated with andropause and managed diverse lifestyle modifications that could help alleviate symptoms and enhance their overall quality of life.
CONFLICTS OF INTEREST:The author declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - PSJ and LYS.
Drafting and critical revision of the manuscript - PSJ and LYS.
Data collection - PSJ and LYS.
Analysis and interpretation of the data - PSJ and LYS.
Discussion and conclusions, suggestions - PSJ.
English review - PSJ and LYS.
Abstract and References and Final Submission- LYS.
This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT)(No. RS-2022-00166296).
 E-SUBMISSION
E-SUBMISSION