
Purpose
This study employed structural equation modeling to verify the suitability and causality of a hypothetical model constructed based on Wilson and Cleary's health-related quality of life model. The aim was to explain and identify the factors that influence quality of life in middle-aged men with prostatic hyperplasia.
Methods
The study included 217 middle-aged men diagnosed with prostatic hyperplasia between February and March 2022 at the urology department of a general hospital in UJB city. The measurement tools used included biological characteristics, International Prostate Symptom Scores, functional health, general health perceptions, social support, and quality of life. The data collected were analyzed using the SPSS 25.0 and AMOS 25.0 programs.
Results
The final model revealed that the variables with the highest explanatory power for quality of life in middle-aged men with prostatic hyperplasia were general health perceptions, followed by the International Prostate Symptom Score, functional health, and prostate size. The explanatory power of the variables for quality of life in middle-aged men with prostatic hyperplasia was 89.7%.
Conclusion
The model used in this study was found to be suitable for assessing quality of life in middle-aged men with prostatic hyperplasia. Based on the study's findings, it is deemed necessary to foster competencies for managing the disease through the development of educational programs, nursing interventions, and countermeasures. These should be based on general health perceptions, symptoms, and functional health, with an accurate knowledge of the characteristics of prostatic hyperplasia, as per Wilson and Cleary (1995)'s health-related quality of life theory.
This study employed structural equation modeling to verify the suitability and causality of a hypothetical model constructed based on Wilson and Cleary's health-related quality of life model. The aim was to explain and identify the factors that influence quality of life in middle-aged men with prostatic hyperplasia.
The study included 217 middle-aged men diagnosed with prostatic hyperplasia between February and March 2022 at the urology department of a general hospital in UJB city. The measurement tools used included biological characteristics, International Prostate Symptom Scores, functional health, general health perceptions, social support, and quality of life. The data collected were analyzed using the SPSS 25.0 and AMOS 25.0 programs.
The final model revealed that the variables with the highest explanatory power for quality of life in middle-aged men with prostatic hyperplasia were general health perceptions, followed by the International Prostate Symptom Score, functional health, and prostate size. The explanatory power of the variables for quality of life in middle-aged men with prostatic hyperplasia was 89.7%.
The model used in this study was found to be suitable for assessing quality of life in middle-aged men with prostatic hyperplasia. Based on the study's findings, it is deemed necessary to foster competencies for managing the disease through the development of educational programs, nursing interventions, and countermeasures. These should be based on general health perceptions, symptoms, and functional health, with an accurate knowledge of the characteristics of prostatic hyperplasia, as per Wilson and Cleary (1995)'s health-related quality of life theory.
Middle age is a transitional period that bridges the gap between the younger and older stages of the life cycle. This phase signifies the commencement of various biological, sociological, familial, and career-related changes. It is a critical stage marked by the onset of physical and mental aging, among other transformations. Middle age is typically defined as the period between 45 and 65 years of age, which is also referred to as midlife. During this phase, individuals must adjust to a variety of circumstances, including declining physical function, changes in social status, and role shifts within the family and toward parents [1]. According to 2019 data from Statistics Korea, the average age of middle-aged individuals in South Korea is expected to rise from 43.1 years in 2019 to 49.5 years in 2030, and further to 61.3 years by 2060. As people are living a larger portion of their lives in middle age, there is an increasing interest in the quality of life during this stage [2]. Middle age, viewed as a potential pre-elderly stage, poses a significant concern, particularly as it has been found to have the highest prevalence of non-cancerous diseases. These include cardiovascular diseases, depression, erectile dysfunction, and benign prostatic hyperplasia [3].
In 2021, an analysis of the National Health Insurance Big Data showed that 1,195,000 patients, or 5.1% of all healthcare recipients, received medical treatment for prostatic hyperplasia. Importantly, 92.1% of these were initial diagnoses in patients in their 50s. This number signifies a significant increase, amounting to 1.3 times the patient count from 2012 to 2017, with an average annual growth rate of 5.9%. This data indicates an upward trend in the incidence of prostatic hyperplasia among middle-aged men [3].
Prostatic hyperplasia is a prominent disorder of the male urinary tract. It arises when the prostate gland, a component of the male reproductive system, experiences enlargement. This enlargement results in obstruction of the lower urinary tract, causing various symptoms associated with the lower urinary tract that involve the bladder, prostate, and urethra [4]. The primary causes of prostatic hyperplasia include genetic factors, chronic conditions such as hypertension and diabetes, and decreased secretion of male hormones. However, the most significant contributing factor to the prevalence of prostatic hyperplasia is the rapidly aging population coupled with shifts in dietary habits towards a Western-style diet [5]. While prostatic hyperplasia is not a life-threatening condition, it does affect quality of life due to various lower urinary tract symptoms, impacting physical, psychological, and daily activities [6]. This leads to increased healthcare costs and diminished economic activities in society, while individuals experience a decline in their quality of life and life expectancy [7]. Therefore, it is crucial to identify the factors that influence the quality of life for patients with prostatic hyperplasia and to develop nursing interventions aimed at improving their quality of life.
Wilson and Cleary's model [8] encompasses five dimensions of health-related quality of life: biological function, symptoms, functional status, general health perceptions, and overall quality of life. This model has been employed in numerous studies investigating the quality of life in patients with chronic diseases. It incorporates individual characteristics that impact health, biological factors that support life, environmental characteristics that include social and physical elements, symptoms that reflect the patient's subjective health-related experiences, functional status that measures the ability to carry out daily activities, and general health perception, which assesses both physical and mental health. In this study, our objective was to utilize Wilson and Cleary's [8] health-related quality of life model to explore the comprehensive causal relationships among individual characteristics, environmental characteristics, biological function, symptoms, functional status, and general health perception. We aimed to identify the factors that influence quality of life in middle-aged men with prostatic hyperplasia, as indicated in prior studies.
Previous studies on quality of life in men with prostatic hyperplasia have identified a variety of factors that influence their quality of life. These factors encompass physiological elements such as symptoms of prostatic hyperplasia, prostate size, lower urinary tract symptoms, and functional status [4, 9, 10, 11]. Personal factors such as age, alcohol consumption, education level, occupation, sleep duration, physical inactivity, economic status, unmet medical needs, and sedentary time [11, 12, 13, 14, 15, 16] have also been found to affect quality of life. Psychological and social factors, including depression, perceived health status, and support from family and friends [4, 9, 10, 11, 14], have been recognized as significant factors contributing to a decreased quality of life. Among these factors, age is often cited as one of the most critical determinants of quality of life. Furthermore, the incidence rate peaks in individuals in their 50s, typically considered middle age. Given that the onset of the condition often occurs during middle age, it is crucial to develop suitable health education and nursing interventions to prevent the disease's severity from escalating. Consequently, this study was designed to examine the structural causal relationships between various variables that influence the quality of life of middle-aged men with prostatic hyperplasia. By creating a model that clarifies the direct and indirect pathways and their effects, we aim to identify practical and effective nursing interventions to improve the quality of life for middle-aged men with prostatic hyperplasia. The objectives of this study were two-fold. First, we aimed to construct a hypothetical model of quality of life in middle-aged men with prostatic hyperplasia and to validate its adequacy. Second, we sought to identify and quantify the direct and indirect effects of the factors that influence quality of life in middle-aged men with prostatic hyperplasia, thereby clarifying the causal relationships among these factors.
Wilson and Cleary's [8] conceptual model of health-related quality of life provides a comprehensive framework for evaluating overall quality of life. It merges the clinical viewpoint of the biomedical paradigm with the non-clinical viewpoint of the social science paradigm. This model is made up of various concepts that elucidate the quality of life, such as biological functioning, symptoms, functional status, general health perception, quality of life, individual characteristics, and environmental characteristics. Essentially, external variables include individual and environmental characteristics, while internal variables consist of biological functioning, symptoms, functional status, general health perception, and overall quality of life. These elements create a unidirectional five-stage context (Figure 1).
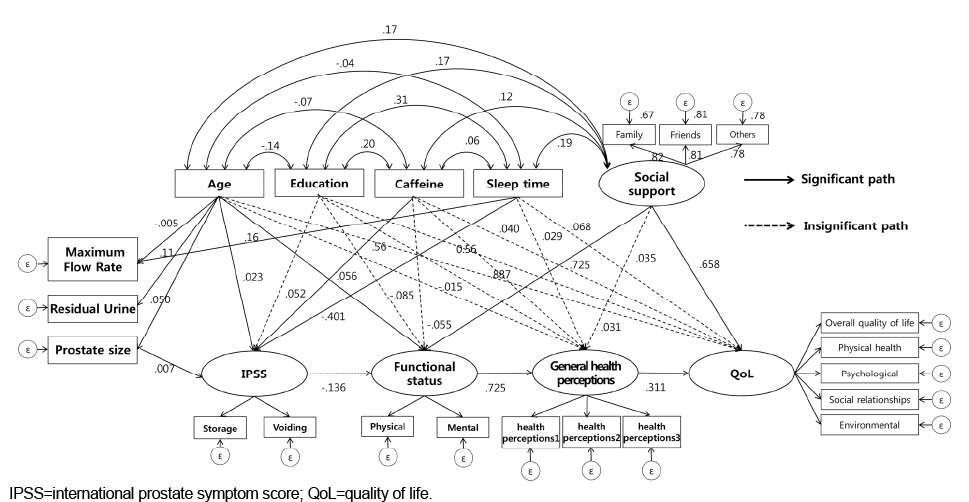
Figure 1
Path diagram of the final model.
Individual characteristics are understood to be unique attributes of an individual [8]. Upon reviewing both domestic and international previous studies, it was found that certain variables frequently impacted the quality of life of patients with prostatic hyperplasia. These variables, often featured in research and studies applying Wilson and Cleary's theory [8], typically include elements that enhance both intrinsic and extrinsic motivation in behaviors through knowledge, beliefs, and attitudes. Consequently, this study incorporated age [9, 11, 17, 18, 19], educational level [9, 11, 17, 20], caffeine consumption [11, 18, 20], and sleep duration [9, 20] as individual characteristics. Furthermore, sleep duration was treated as an external variable because it has been reported to have varied outcomes in previous studies, despite the belief that it influences quality of life through its effect on nocturia.
The environment, categorized into social and physical aspects, plays a pivotal role in health outcomes. Social factors include interpersonal relationships with family, friends, and others, which can significantly impact health management and therapeutic actions. Conversely, physical factors pertain to the positive and negative aspects of the community that can influence health outcomes. A variety of factors shape an individual's social environment, which includes supportive elements that can bolster a patient's physical, social, and functional capabilities [21]. Research has shown that social support for middle-aged men is linked to their quality of life [22], affecting a patient's physical and emotional symptoms and overall quality of life [23]. Furthermore, social support for patients with prostatic hyperplasia has been demonstrated to enhance their quality of life [4]. Therefore, this study incorporated social factors that influence health management and therapeutic actions.
Biological function is the primary determinant of an individual's health status. In the diagnosis of prostatic hyperplasia, it is crucial to conduct tests that concentrate on the performance of cells, organs, and organ systems. These tests include the maximum urinary flow rate, post-void residual volume, and the size of the prostate as measured using transrectal ultrasonography [5].
Symptoms represent an individual's subjective experiences, evaluations, and interpretations of their own physical health. These are physical sensations or feelings tied to one's bodily state, which can be influenced by a variety of demographic, environmental, and cultural factors [20]. The International Prostate Symptom Score (IPSS) was utilized to assess these symptoms.
Functional status refers to an individual's capacity to execute tasks across a range of domains, such as physical, social, role, and psychological functioning. This status can be influenced by present symptoms, with an emphasis on enhancing the remaining functions [24]. The functional status has a consequential effect on the subsequent domain, known as general health perceptions. In the context of this study, functional status was evaluated in terms of functional health.
General health perceptions are defined in two ways within this model. First, they represent the amalgamation of all health concepts previously discussed in this model. Second, they underscore the importance of subjectivity. Health perception is a subjective assessment of one's health, which serves as a potent predictor of mortality rates and is a critical predictive factor commonly utilized in medical and mental health services [25]. As noted by Wilson and Cleary [8], perceived health status typically has a significant impact on quality of life. Subjective health perception embodies the collective subjective experience of diseases, whether they are acute or chronic and fatal or non-fatal, and mirrors an individual's overall health status, encompassing physical, mental, and social well-being. Consequently, subjective health evaluation is a comprehensive approach to representing an individual's holistic health status [24]. When subjective health status is deemed good, physical, mental, and sensory fatigue symptoms are found to be low. It has been observed that not only is one's health status perceived as good, but the health of the family is also perceived positively, thereby influencing family health [25]. In this study, general health perceptions were evaluated as perceived health status.
Quality of life is the final construct in this model. It is influenced by general health perceptions, and it represents the subjective state of well-being, encapsulating an individual's level of happiness and satisfaction with life. Subjective well-being includes both positive and negative emotions, comprehensive assessments of life satisfaction, and personal contentment [26]. In essence, it is subjectively characterized as an individual's total happiness and satisfaction with life, influenced by their general health perceptions.
This study employed a structural model to explain and identify the factors affecting quality of life in middle-aged men with prostatic hyperplasia based on Wilson and Cleary's conceptual model of health-related quality of life. A hypothetical model was constructed to describe the quality of life of middle-aged men with prostatic hyperplasia, and the model fit and hypotheses were tested through structural modeling.
The study subjects were 220 middle-aged men (aged 45~64) diagnosed with prostatic hyperplasia at the Department of Urology of a general hospital in Uijeongbu City, Gyeonggi Province. To be included in the study, participants needed to understand the research purpose and provide consent. Those with a history of prostate cancer, urological surgery, or who were undergoing cancer or radiation treatment after a cancer diagnosis were excluded. This is because cancer, cancer treatment, and radiation can influence urinary volume, the degree of prostatic urethral obstruction, and bladder function and capacity [5]. While there is no definitive sample size requirement for structural equation modeling, a sample size of 200 is often considered a benchmark [27]. The optimal sample size for maximum likelihood typically falls between 150 and 400, with more than 400 samples potentially leading to a decrease in model fit [28]. In this study, we initially selected 220 participants, which is ten times the number of observed variables (22 variables). Taking into account a 10% attrition rate, we collected data from a final 240 participants [27]. After excluding 23 participants due to incomplete responses, we ultimately used data from 217 participants.
Based on a review of various previous studies, a questionnaire was designed to collect participants' general characteristics. These characteristics were divided into two categories: demographic and health-related attributes. The demographic characteristics encompassed factors such as age, marital status, level of education, economic status, religious beliefs, type of housing, and occupation, among others. Health-related attributes, meanwhile, included habits such as smoking, alcohol consumption, caffeine consumption, exercise routines, and sleep duration.
Social support was evaluated using the Multidimensional Scale of Perceived Social Support (MSPSS), originally developed by Zimet et al. [29] and later adapted by Shin and Lee [30]. The original and adapted versions were utilized with the authors' permission. This scale assesses three distinct aspects of social support: support from family, friends, and significant others. Each aspect is represented by four items, culminating in a total of 12 items. Participants' responses are scored on a 5-point Likert scale, with "not at all" corresponding to 1 point and "very much" corresponding to 5 points. The total score can range from a minimum of 12 to a maximum of 60, with higher scores signifying greater perceived social support. The original scale by Zimet et al. had a Cronbach's α of .95 [29], while in this study, Cronbach's α was .96.
The maximum flow rate denotes the peak urinary flow rate per second. This single index measurement serves as a valuable indicator for urinary flow measurement. A normal range falls between 20 and 25 mL/s, with values under 15 mL/s potentially indicating bladder outlet obstruction [5]. The researchers conducted the assessment themselves, and the equipment required no additional calibration. The maximum speed was measured using MMS Solar equipment.
Residual urine measurement quantifies the volume of urine remaining in the bladder following urination. A normal measurement is typically 50 mL or less [5]. The researchers themselves served as the assessors, with no additional calibration required for the equipment. The highest value from three separate measurements was documented. The BIOCON-900 equipment from Emcube Technology was utilized to conduct the residual urine measurements.
using transrectal ultrasound, typically falling within a normal range of 20 g or less [5]. These measurements were performed by a specialist in urology, and there was no need for further calibration of the equipment. The device utilized for this procedure was an SSD-3500SV, manufactured by Aroka.
The IPSS, which was developed by Barry et al. [31] and translated and adapted to the Korean language by Choi et al. [32] was utilized in this study, with the approval of the authors of the adapted version. The IPSS comprises eight lower urinary tract symptoms: frequency, intermittency, incomplete emptying, weak stream, daytime frequency, nocturia, hesitancy, and urgency, along with a question regarding quality of life. These symptoms are divided into two categories: voiding symptoms (questions 1, 3, 5, 6) and storage symptoms (questions 2, 4, 7). For the purposes of this study, question 8, which duplicates the quality of life assessment, was omitted. Each question is scored on a 6-point Likert scale, with "not at all" and "none" scoring 0 points, and "almost always" and "5 times or more" (for nocturia) scoring 5 points. The scores are then calculated as the average of the voiding and storage symptom scores [4, 28], with higher scores indicating more severe symptoms. The original tool by Barry et al. had a Cronbach's α of .86 [31], while in this study, Cronbach's α was .79.
Functional status was evaluated using the Short Form-12 health survey questionnaire (SF-12), a tool developed by Ware et al. [33]. We obtained permission to use the Korean version of this tool from http://www.OPTUM.com. The SF-12 questionnaire consists of 12 items that assess two domains: the Physical Component Score (PCS) and the Mental Component Score (MCS). The PCS covers aspects such as pain, general health, physical function, and physical role limitations, while the MCS encompasses social functioning, vitality, mental health, and emotional role limitations. Each item utilized a different response scale. The scores for the PCS and MCS were calculated using QualityMetric health outcomes scoring software version 5.0 and were subsequently used in this study. Higher scores are indicative of better functional health. During the tool's development by Ware et al. [33] Cronbach's α was .89 for the PCS and .81 for the MCS [4]. In this study, Cronbach's α was .86 for the PCS and .84 for the MCS.
The health status self-assessment measurement tool developed by Lawton et al. [34] and translated and adapted into Korean by Shin et al. [35] was used in this study with the permission of the authors of the adapted version. The tool consists of three items, each rated on a 5-point Likert scale, with a total possible score of 15 points. Each item is scored from 1 point, indicating "very poor," to 5 points, indicating "very good." Higher scores correspond to a better perceived health status. In the study conducted by Shin et al. [35], Cronbach's α for this tool was reported as .91 [34]. In our study, Cronbach's α was .90.
The World Health Organization Quality of Life (WHO QOL-BREF) [36] is a simplified quality of life scale developed by the World Health Organization. This scale was adapted by Min et al. [37] to create a Korean version, utilizing the summation method of Hwang et al. [38]. With permission from the Korean developers, we used this tool in our study. The tool comprises 26 questions divided into five subdomains: overall quality of life (2 questions), physical health (7 questions), psychological health (6 questions), social relationships (3 questions), and environmental conditions (8 questions). The questions are scored on a 5-point Likert scale, with questions 3, 4, and 26 being negatively phrased and therefore reverse-scored. The total score can range from 26 to 130 points, where a higher score signifies a better quality of life. During its development, the tool had a Cronbach's α of .89 [36], while in this study, it was .97.
The Institutional Review Board of a general hospital in Uijeongbu City, Gyeonggi Province, South Korea, approved the data collection for this study (project number: UC21QASI0156). The data collection process took place in February and March 2022. After obtaining permission from the Departments of Urology and Nursing at the hospital, the researchers personally stationed themselves in the outpatient Department of Urology to recruit eligible participants based on pre-established criteria. The participants were briefed about the study's purpose, procedures, methods, benefits, and potential risks. They were invited to participate voluntarily and provide written consent. It was emphasized that they could withdraw from the survey at any point without facing any repercussions. The anonymity of the participants was assured, and it was clarified that the survey data would be used exclusively for research purposes. All participants provided written consent in agreement with these terms. To prevent any potential breach of personal information, the completed surveys were promptly secured in a locked cabinet. The collected data are stored securely, encrypted, and will be disposed of 3 years after the conclusion of the study.
Data were analyzed using SPSS 25.0 and AMOS 25.0 software. The general characteristics of the participants were analyzed using frequency and percentage. Descriptive statistics were employed to examine the levels of the study variables. To verify normality, skewness and kurtosis were analyzed. Pearson's correlation coefficient, Variation Inflation Factor (VIF), and tolerance were utilized to analyze correlations between measurement variables and to assess multicollinearity. Confirmatory factor analysis was conducted to validate the observed variables that make up the latent variables. Both convergent validity and discriminant validity were confirmed. The hypothetical model's parameter estimation was performed using maximum likelihood estimation. Absolute fit indices such as chi-square (χ2), χ2 divided by degrees of freedom (χ2/df), Goodness of Fit Index (GFI), Root Mean Square Error of Approximation (RMSEA), Normed Fit Index (NFI), Incremental Fit Index (IFI), Tucker-Lewis Index (TLI), and Comparative Fit Index (CFI) were analyzed to evaluate the model's fit. A Structural Equation Model (SEM) analysis was carried out to verify the causal relationships between variables. Bootstrapping was employed to test the significance of direct and indirect effects within the model.
In terms of sociodemographic characteristics, the majority of participants fell within the 60~64 years age group, comprising 147 individuals (67.8%). Regarding education, 93 participants (42.9%) had completed high school. When considering health-related characteristics, 124 participants (57.1%) reported being smokers, 49 participants (22.6%) had quit smoking, and 44 participants (20.3%) were non-smokers. As for alcohol consumption, 93 participants (42.9%) reported drinking alcohol 3~4 times per week. Caffeine consumption was reported by 131 participants (60.4%), while 124 participants (57.1%) reported not engaging in regular exercise. Almost half of the participants reported sleeping for 7~8 hours (n=102; 47.0%) (Table 1).
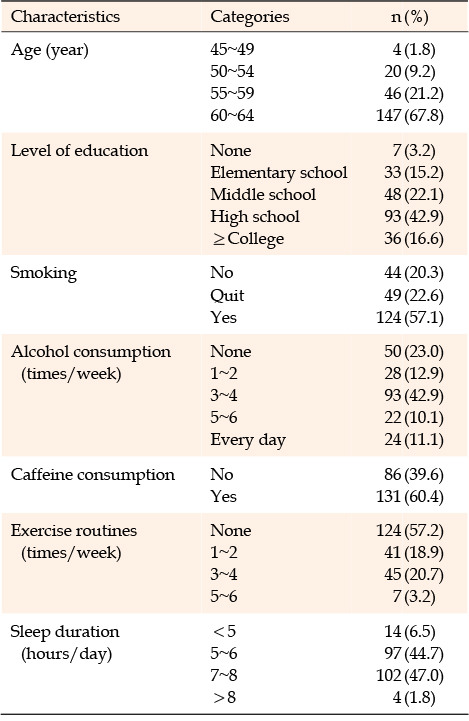
Table 1
General Characteristics of Participants (N=217)
The mean social support score was 3.51 on a 5-point scale. The subscale mean values were as follows: family support, 3.71; friend support, 3.55; and special support from others, 3.29. The mean maximum flow rate, a biological function measure, was 14.08 mL/s. The mean IPSS was 3.25 on a 6-point scale. The mean functional health score was 3.19 on a 5-point scale. The perceived health status had a mean score of 3.50 on a 4-point scale. The mean quality of life score was 3.44 on a 5-point scale. Subscale averages for quality of life were as follows: overall domain (3.34), physical domain (3.56), psychological health domain (3.44), social domain (3.33), and environmental domain (3.40). To verify the assumptions of normality, skewness and kurtosis values were computed. Skewness values less than 3 and kurtosis values less than 10 are deemed to approximate a normal distribution [27]. However, since the skewness and kurtosis values for residual urine and prostate size exceeded the threshold, these variables were logarithmically transformed for subsequent analysis [27]. The Average Variance Extracted (AVE) for all items surpassed the threshold, confirming convergent validity. Moreover, discriminant validity is deemed acceptable if the 95% confidence interval of the correlation coefficients does not encompass 1 or -1 [39]. As the confidence intervals of the correlation coefficients between all variables did not encompass 1 or -1, discriminant validity can be considered satisfactory. A correlation coefficient greater than or equal to .90 indicates a multicollinearity issue [27]. However, in this study, the correlation coefficients were less than .90, the tolerance values ranged from 0.35 to 0.80, with a minimum threshold of 0.1, and the VIFs ranged from 0.88 to 3.70, well below the threshold of 10, indicating no multicollinearity among all measured variables (Table 2).
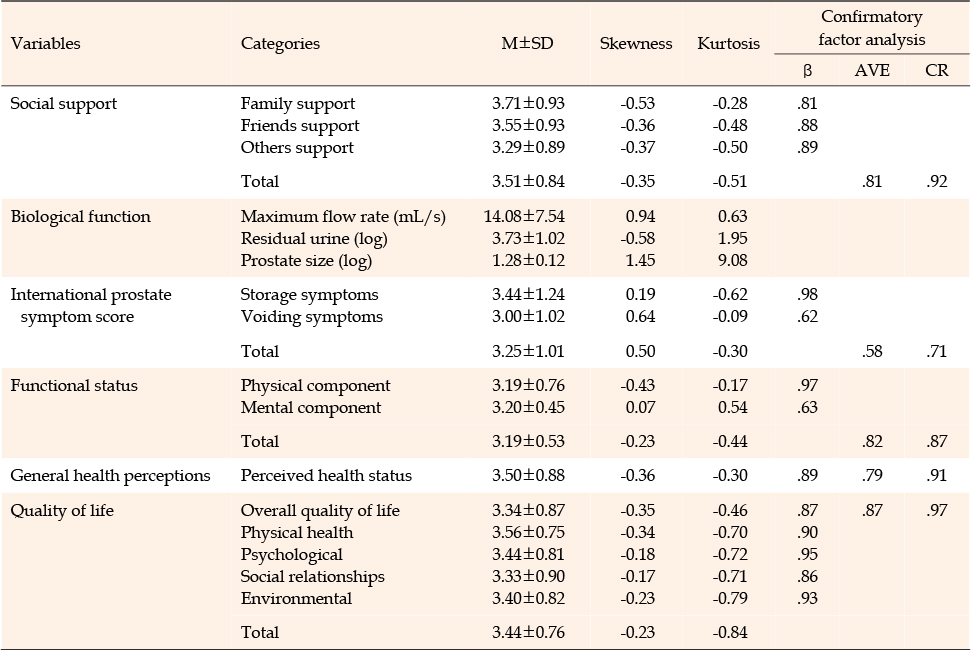
Table 2
Descriptive Statistics of the Measured Variables (N=217)
In assessing the suitability of the research model, we examined the χ2 (df=168) value in conjunction with other fit indices. This is because the χ2 value is significantly affected by both the sample size and the complexity of the model [19]. The results revealed a χ2/df value of 2.02, which aligns with the recommended levels. The other fit indices were as follows: GFI=.90, RMSEA=.07, NFI=.91, IFI=.95, TLI=.93, CFI=.95. These results suggest that the research model was appropriately fitted [23] (Table 3).

Table 3
Suitability of the Research Model (N=217)
The estimation of model parameters revealed that 15 out of 28 paths were significant, whereas 13 paths were not (Figure 1).
Age had a direct effect on the maximum flow rate (β=-.01, p=.019) and sleep duration (β=.16, p<.020). It also had a direct impact on residual urine (β=.11, p=.005), prostate size (β=.05, p<.007), and the IPSS (β=.02, p=.007). Caffeine consumption directly affected the IPSS (β=.06, p=.013). Prostate size and sleep duration both had direct effects on the IPSS (β=.07, p=.009 and β=-.40, p<.001, respectively). Social support directly influenced functional health (β=.73, p=.001), as did perceived health status (β=.88, p<.001). The IPSS directly affected quality of life (β=.50, p<.031), as did functional health status (β=.38, p<.001). Perceived health status also had a direct effect on quality of life (β=.71, p<.001). Moreover, both age and functional health had a direct effect (β=.02, p=.019) and an indirect effect (β=.07, p=.005) on quality of life, yielding a significant total effect (β=.09, p=.024). Social support and quality of life demonstrated an indirect effect (β=.46, p<.001), and the indirect effect of functional health on quality of life through perceived health status was statistically significant. In conclusion, the factors that significantly influenced quality of life were perceived health status, IPSS, and functional health status, in that order. The independent variables explained 89.7% of the variance in quality of life (Table 4).
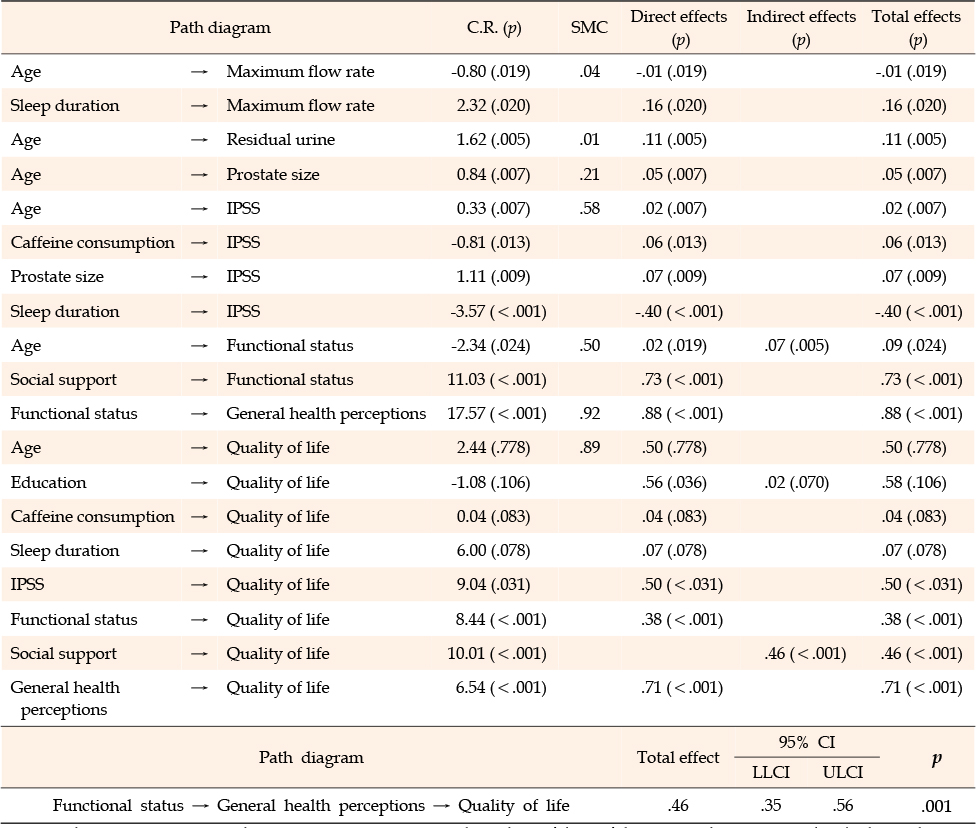
Table 4
Direct, Indirect and Total Effects for the Research Model (N=217)
This study aimed to explain and predict the factors influencing quality of life in middle-aged men suffering from prostatic hyperplasia. Our approach was grounded in Wilson and Cleary's conceptual model of health-related quality of life [8] and informed by prior research. We developed a theoretical model and collected data from middle-aged men with prostatic hyperplasia to evaluate the model's appropriateness and the validity of the proposed hypotheses. In this section, we explore the correlations between the study findings and the variables.
The first major factor identified in this study that influenced quality of life in middle-aged men with prostatic hyperplasia was perceived health status. Specifically, the results of this study show that perceived health status had a significant impact on quality of life.
Given that no previous studies have directly examined the inclusion of perceived health status in the context of prostatic hyperplasia, a review of related research findings indicates that perceived health status significantly impacts the quality of life of uterine cancer patients [40]. It also suggests that perceived health status is a predictive factor for health-related quality of life in cervical cancer patients [41], a finding that aligns with the results of this study. Moreover, it was established that self-efficacy for exercise improves in line with perceived health status during the stages of exercise behavior change in patients with rheumatoid arthritis [42]. The study also verified that perceived health status positively affects self-care behavior in cancer patients undergoing chemotherapy [43]. These findings underscore the relationship between perceived health status, quality of life, and related variables, thereby reinforcing the results of this study. Therefore, it is posited that strategies to positively alter perceived health status are necessary to enhance the quality of life of middle-aged men with prostatic hyperplasia. Additionally, in studies focusing on middle-aged men seeking medical attention due to worsening symptoms of prostatic hyperplasia, it should be noted that their health perception may be assessed as low due to a skewed perception of symptoms at the time of seeking medical care, potentially leading to the omission of confounding factors. This consideration should also be addressed in future studies.
The second major factor influencing quality of life in middle-aged men with prostatic hyperplasia, as identified in this study, was the IPSS. This conclusion aligns with previous research findings, which suggest that as lower urinary tract symptoms intensify, they negatively affect the quality of life [44]. This supports earlier studies demonstrating that a deterioration in the quality of life is associated with worsening lower urinary tract symptoms, leading to increased anxiety and depression [45]. Furthermore, among men with prostatic hyperplasia, a significant correlation was found between symptoms and quality of life [4]. As lower urinary tract symptoms worsen, the quality of life decreases [18]. There was also an inverse correlation between lower urinary tract symptoms and quality of life [11]. Prostate symptoms have been identified as a key factor affecting the quality of life, with family cohesion indirectly influencing these symptoms [18]. An inverse correlation was found between prostatic hyperplasia symptoms and quality of life, corroborating many previous studies, and these results confirm factors that influence the quality of life [19]. However, it is worth noting that in other research, urinary incontinence symptoms were found not to significantly impact the quality of life [46], unlike the present study. A limitation of this study is that it was conducted over a specific period and at a single institution. Additionally, given that lower urinary tract symptoms, which are prominent among middle-aged men with prostatic hyperplasia, worsen during the cold winter season due to increased sympathetic nerve activity, which causes contraction of the muscles surrounding the prostate and increases urethral pressure [5], it is difficult to generalize the results. Based on these findings, this study identified variables affecting symptoms to include age, caffeine consumption, prostate size, and sleep duration. Therefore, targeted interventions and symptom education are crucial.
The third factor that influenced quality of life in middle-aged men with prostatic hyperplasia was functional health. When compared to previous research, functional health (as measured by the physical health index) has been identified as a factor that influences the quality of life in patients with prostatic hyperplasia [4]. This factor has also been reported to influence the quality of life in patients with liver cirrhosis [47], which supports the findings of this study. Additionally, in patients with benign prostatic hyperplasia, lower urinary tract symptoms are associated with the educational level and sleep duration in individuals with functional health (as measured by the mental health index) [13]. This supports the current study, which found a significant relationship between male lower urinary tract symptoms and functional health (as measured by the mental health index) [48]. For individuals transitioning from middle age to the elderly stage, maintaining physical and mental health is essential for leading an independent and meaningful life, and is strongly linked to life satisfaction [49]. The alignment of this study with previous research underscores the need for a comprehensive understanding of this condition, which can lead to both physical and psychological complications. It also highlights the importance of professionals in the field having accurate knowledge to counsel and educate individual patients.
This study found that perceived health status, symptoms, and functional health significantly impact the quality of life in middle-aged men with prostatic hyperplasia, corroborating previous research findings. However, there is a scarcity of studies conducted on subjects with prostatic hyperplasia in both domestic and international settings, which complicates direct comparisons with existing research. Therefore, additional studies are necessary to comprehend the relationships between various factors that influence the quality of life among subjects with prostatic hyperplasia. It is important to note that the subjects in this study were selected for convenience from the outpatient Department of Urology at a general hospital in U city, Gyeonggi Province. The results of this study must be interpreted and generalized carefully considering this limitation.
The significance of this study lies in its exploration and validation of various factors influencing quality of life in individuals with prostatic hyperplasia, as this topic has not previously been thoroughly considered in South Korea. The results of this study are anticipated to enhance the quality of life for individuals with prostatic hyperplasia and may serve as a foundation for future research and nursing interventions for this population.
This study aimed to identify the factors that influence quality of life in middle-aged men with prostatic hyperplasia. The model used to assess quality of life was found to be appropriate for the subjects of this study. The findings showed that perceived health status had the most significant effect on the quality of life for these men, followed by the International Prostate Symptom Score and functional health. Together, these variables accounted for 89.7% of the variation in quality of life. The results suggest that benign prostatic hyperplasia, which is marked by lower urinary tract symptoms, can lead to a range of physical and mental health problems, ultimately impacting quality of life. As such, it is crucial to implement measures and interventions to address these issues. Based on the results of this study, it is anticipated that interventions will be developed that focus on physical and mental health, educational programs, coping strategies, and more, all aimed at improving the quality of life for middle-aged men with benign prostatic hyperplasia. Additionally, considering the strong correlation between prostate health and seasonal and temperature changes, it is recommended to conduct research during different seasons for comparison. Given the recent strengthening of privacy protection laws, which can limit surveys related to sensitive topics such as sexual health, it is also recommended that future studies investigate sexual health in patients with prostatic hyperplasia.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - MHN and YSH.
Data collection - MHN.
Analysis and interpretation of the data - MHN and YSH.
Drafting and critical revision of the manuscript - MHN and YSH.
This article is based on a part of the first author's doctoral thesis from Shinhan University in 2022.
 E-SUBMISSION
E-SUBMISSION