
Purpose
This study aimed to identify the characteristics and efficacy of Intermittent Pneumatic Compression (IPC) interventions for preventing Venous Thromboembolism (VTE) in critically ill patients.
Methods: The CENTRAL, Embase, OVID, CINAHL, KMbase, KoreaMed, and KoreaScience databases were searched from January 7 to 11, 2023. The search included all records from the inception of each database up to January 2023, with publication language restrictions to English and Korean. Three reviewers independently carried out the entire process, which included data search, quality assessment, and data extraction.
Results: Out of 1066 articles, six Randomized Controlled Trials (RCTs) were included. One of the four studies that reported on the incidence of DVT, and one of the six studies that measured the incidence of Pulmonary Embolism (PE), found that IPC alone was effective in reducing the incidence of DVT and PE. One of the four studies that reported on VTE incidence demonstrated a significant reduction in VTE incidence with a triple intervention of IPC, anticoagulants, and elastic compression stockings compared to a combined intervention of anticoagulants and graduated compression stockings. Four studies that reported data on the incidence of bleeding reported no effect on reducing bleeding.
Conclusion: Our findings suggest that IPC interventions may reduce the incidence of DVT as a preventive strategy in critically ill patients. Further RCTs are necessary to evaluate the effect of IPC interventions on DVT prevention in this patient population and to provide robust evidence for critical care nursing.
This study aimed to identify the characteristics and efficacy of Intermittent Pneumatic Compression (IPC) interventions for preventing Venous Thromboembolism (VTE) in critically ill patients.
The CENTRAL, Embase, OVID, CINAHL, KMbase, KoreaMed, and KoreaScience databases were searched from January 7 to 11, 2023. The search included all records from the inception of each database up to January 2023, with publication language restrictions to English and Korean. Three reviewers independently carried out the entire process, which included data search, quality assessment, and data extraction.
Out of 1066 articles, six Randomized Controlled Trials (RCTs) were included. One of the four studies that reported on the incidence of DVT, and one of the six studies that measured the incidence of Pulmonary Embolism (PE), found that IPC alone was effective in reducing the incidence of DVT and PE. One of the four studies that reported on VTE incidence demonstrated a significant reduction in VTE incidence with a triple intervention of IPC, anticoagulants, and elastic compression stockings compared to a combined intervention of anticoagulants and graduated compression stockings. Four studies that reported data on the incidence of bleeding reported no effect on reducing bleeding.
Our findings suggest that IPC interventions may reduce the incidence of DVT as a preventive strategy in critically ill patients. Further RCTs are necessary to evaluate the effect of IPC interventions on DVT prevention in this patient population and to provide robust evidence for critical care nursing.
Critically ill patients are susceptible to thrombus formation and embolism due to factors such as advanced age, prolonged immobility related to disease severity or sedative use, and vascular damage from central venous catheters or other invasive procedures. The incidence of Deep Vein Thrombosis (DVT) in this population is approximately 15~30% [1, 2].
DVT primarily affects the lower extremities, with blood clots forming in the deep veins and obstructing blood flow [3]. DVT is the leading cause of Pulmonary Embolism (PE); in recent times, DVT and PE together are referred to as Venous Thromboembolism (VTE) [3]. When VTE occurs in the popliteal vein, it is classified as proximal VTE, whereas its occurrence in the calf vein is termed distal VTE. DVT often presents without symptoms or may manifest as edema, tenderness, and fever. However, these symptoms can be difficult to distinguish from those of other conditions. Additionally, post-thrombotic syndrome, which is challenging to treat, may develop following DVT. Therefore, preventing the formation of venous thrombi is highly important [3, 4].
The American College of Chest Physicians and the American Society of Hematology have issued guidelines recommending the use of anticoagulants for thrombus prevention in critically ill patients without contraindications [5, 6]. However, in cases where there is active bleeding or a high risk of bleeding, Intermittent Pneumatic Compression (IPC) is advised as an alternative until the bleeding risk diminishes [5, 6]. The efficacy of anticoagulants, such as Unfractionated Heparin (UFH) or Low-Molecular-Weight Heparin (LMWH), in thromboprophylaxis has been well-documented [1]. Nonetheless, their use may be limited due to concerns about bleeding or the potential for bleeding. In the realm of critical care nursing, IPC is frequently chosen for its low bleeding risk and its ability to address Virchow's triad, making it a viable option for preventing VTE either alone or in conjunction with anticoagulants [7].
However, there is a lack of studies on the thromboprophylactic effects of IPC, the available evidence is inconsistent, and the efficacy of IPC remains uncertain. Only one previous meta-analysis [1] has examined the thromboprophylactic efficacy of anticoagulants and included the effects of mechanical thrombosis prevention. Limpus et al. [8] conducted a systematic review of two Randomized Clinical Trials (RCTs) comparing IPC with LMWH in trauma patients, revealing no significant difference in the incidence of DVT between the two interventions. A prior network meta-analysis comparing IPC, a control group, and LMWH [9] suggested a trend toward reduced DVT risk, but the difference was not statistically significant.
However, other studies [10, 11] have reported that IPC was effective in reducing the incidence of VTE and DVT compared to the control group. However, there was no significant difference when compared to LMWH. Additionally, combining IPC with LMWH did not yield any extra benefits, and the bleeding rate was higher with LMWH. These findings suggest that IPC is relatively safe and is widely recognized and selected in critical care nursing [9, 12]. Nonetheless, there is a lack of robust evidence to guide clinical practitioners regarding the thrombosis prevention effects of IPC.
The evidence-based clinical practice guidelines of the American College of Chest Physicians [6] recommend strategies for VTE prevention. These recommendations are based on two RCTs that compared the combined effect of IPC and an anticoagulant with that of an anticoagulant alone in patients undergoing major orthopedic surgery [5]. Consequently, it is important to determine the effectiveness of IPC in critically ill patients. This includes assessing the thromboprophylactic effect of IPC alone on VTE prevention in general inpatients, as well as its potential additional benefits when used in conjunction with anticoagulants. Previous secondary analyses of the efficacy of IPC in preventing VTE [9, 11] were limited by the small number of RCTs and non-RCTs or observational follow-up studies available, as there were few primary RCTs on the subject. Therefore, further research is required to provide robust evidence for the use of IPC in clinical practice. This study aimed to evaluate the characteristics and efficacy of IPC interventions for VTE prevention in critically ill patients. To achieve this, we conducted a systematic review of RCTs that implemented IPC interventions to prevent thrombosis in this patient population.
We selected the study subjects according to Participants, Intervention, Comparison, Outcome, Setting, and Study Design (PICOS-SD) framework as follows: 1) participants: adults (at least 19 years old) who are hospitalized in Intensive Care Units (ICUs); 2) intervention: IPC alone or a combined intervention; 3) comparison: pharmacologic thromboprophylaxis, Compression Stockings (CS), or their combinations; 4) outcomes: the incidence rate of DVT (Proximal DVT [P-DVT], Distal DVT [D-DVT]), PE, and VTE as primary outcomes, as well as bleeding as the secondary outcome; 5) setting: ICUs; and 6) study design: RCT. The exclusion criteria were 1) studies in which the subjects were not critically ill or under the age of 19, 2) studies that did not report thrombus-related variables, and 3) studies that did not use an RCT design.
This study did not apply for IRB approval because only the literature was used as a research subject, and a protocol was not prepared.
This study was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions [13] and prepared according to the PRISMA reporting guidelines [14]. We conducted the data search from January 7 to January 11, 2023. Based on the COre, Standard, Ideal (COSI) model [15] presented by the U.S. National Library of Medicine, we used the international core databases, including Ovid-Medline, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL); as Korean databases, we used Korean Medical Database (KMbase), KoreaMed, and KoreaScience. We used the Cumulative Index to Nursing and Allied Health Literature (CINAHL) as a standard international database. As Korean standard databases, we used DBpia, the Journal of Korean Academy of Nursing, Journal of Clinical Nursing Research, Korean Journal of Adult Nursing, Journal of Korean Academy of Fundamentals of Nursing, and Journal of Korean Critical Care Nursing. Google Scholar was searched using the snowball method. The search strategy was established using Medical Subject Headings (MeSH) and EMTREE terms, and search functions such as Boolean operators and truncation were used. Table 1 shows the search terms used. We used the RCT search filter of the Scottish Intercollegiate Guidelines Network. No restrictions were placed on the year of publication and the language. In addition, we included full texts and abstracts to minimize selection bias.
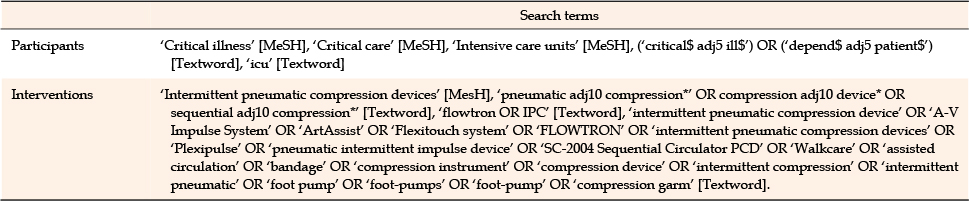
Table 1
List of Search Terms
We managed the retrieved data using the EndNote 20 program. After removing duplicate literature, we reviewed the titles and abstracts to select studies. We then reviewed the full texts to determine the subjects for the systematic review according to the literature selection and exclusion criteria. The literature selection process was conducted independently by three researchers, and any disagreements were resolved by consensus through discussions based on the selection and exclusion criteria.
The methodological quality of the included study was assessed using the Cochrane Risk-of-Bias tool for randomized trials (RoB 2.0) [16]. This tool evaluates five domains: randomization process, deviations from the intended intervention, missing outcome data, measurement of the outcome, and selection of reported results. Responses to each question within these domains are categorized as "yes," "probably yes," "probably no," "no," or "no information." Based on these responses, the risk of bias is classified as "low," "some concerns," or "high" according to the tool's evaluation algorithm. Ultimately, the final quality assessment criteria of RoB 2.0 classify the risk of bias to be "low," "some concerns," or "high" [16]. The methodological evaluation of the quality of the selected studies was performed independently by three researchers. In the event of disagreement, a consensus was reached through review and discussion.
We extracted data using a collection sheet designed by our research team. We examined the characteristics of the included studies, such as the author's name, publication year, country of origin, selection and exclusion criteria for participants, number of participants, age, gender, Injury Severity Score (ISS), Body Mass Index (BMI), length of ICU stay, and duration of ventilator use or intubation. We analyzed the characteristics of the interventions, including the type of IPC intervention, device application mode, sleeve type, and the timing and duration of application. Additionally, we assessed the control characteristics. Outcome measures were identified, including the incidence rates of DVT (P-DVT, D-DVT), PE, VTE, and bleeding.
In this study, the number of RCTs that reported thromboprophylaxis interventions with IPC was very small. The reported interventions and controls varied, as did the outcomes, which restricted our ability to calculate a combined estimate of effect size through quantitative analysis. Consequently, we conducted a systematic analysis of the types of interventions and their effects, with a focus on individual outcomes. Furthermore, we reported the incidence rates of DVT (P-DVT, D-DVT), PE, and VTE as primary outcomes and bleeding as secondary outcomes.
The systematic literature search yielded a total of 1,072 articles, and six articles were added through hand searching. We removed 161 duplicate articles, and three researchers reviewed the titles and abstracts, which led to the exclusion of 896 out of 911 articles. We selected 15 articles to review according to the inclusion and exclusion criteria. Finally, we included six articles—one [A1] was an abstract and five were full texts [A2-A6]—and excluded nine articles. For the abstract [A1], we emailed the author to request the full text but were not able to reach them, so we decided to use the abstract. The final included studies are listed in Appendix 1 (Figure 1).
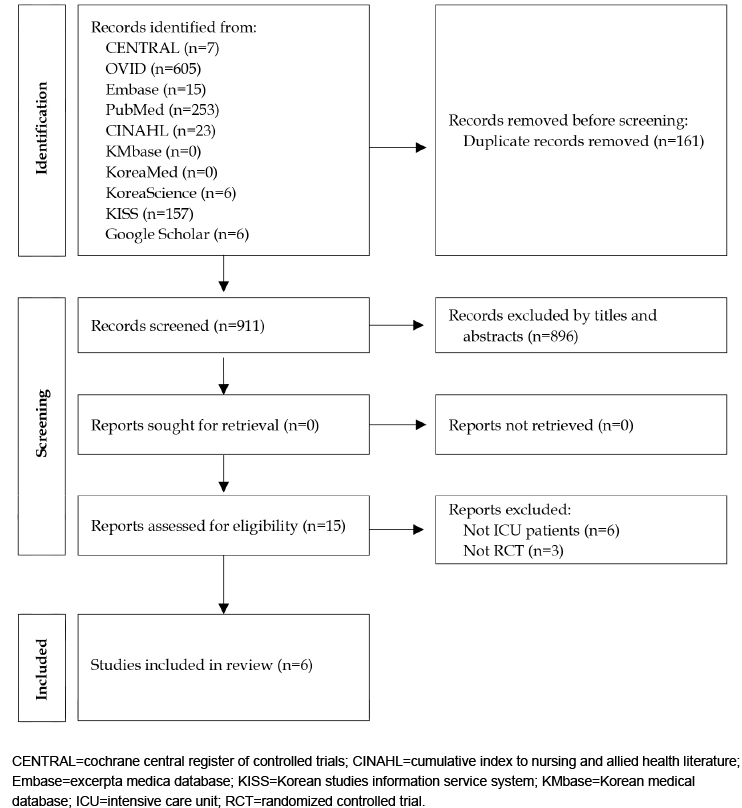
Figure 1
PRISMA flow of study selection process.
Since only the abstract was available for one of the six studies, it was judged to have a high level of overall bias due to the high risk of bias in "deviations from the intended intervention" and "missing outcome data." Four studies showed a low overall risk of bias, and the remaining study was judged to have "some concerns" (Figure 2).
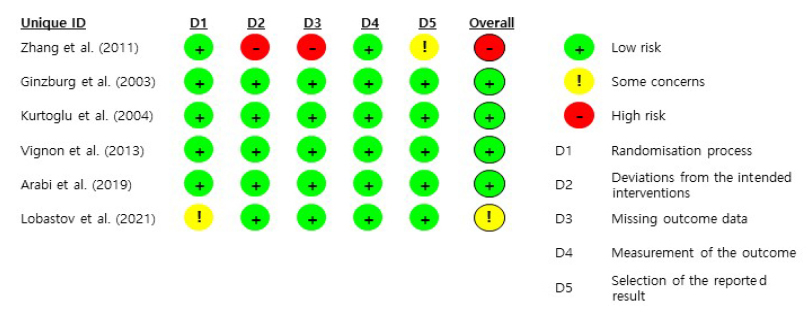
Figure 2
Risk of bias.
The six studies aimed at preventing thrombogenesis in critically ill patients were conducted in the years 2003 [A2], 2004 [A3], 2011 [A1], 2013 [A4], 2019 [A5], and 2021 [A6]. These studies took place in various countries, including multiple countries [A5], China [A1], the United States [A2], Turkey [A3], France [A4], and Russia [A6]. The settings for these studies were ICUs, encompassing general ICUs [A4,A5], trauma ICUs [A2,A3], medical ICUs [A1], and surgical ICUs [A6]. The sample sizes varied, ranging from 120 to 2,003 participants, with a total of 1,762 individuals in the experimental groups and 1,778 in the control groups.
The age range of participants was 37.1~68.8 years, with the proportion of men varying from 36.8% to 74.6%. Both the experimental and control groups exhibited similar levels, although one study did not report these figures [A1]. The average BMI of participants was comparable to that of the experimental group, falling between 16.4~29.0 kg/m2 [A3-A5]. Of the three studies that omitted BMI data, Ginzburg et al. [A2] specifically included only participants with a BMI under 25 kg/m2. The severity of the disease, as measured by the ISS or the Acute Physiologic and Chronic Health Evaluation II (APACHE II), was reported in three studies [A2,A3,A5]. Ventilator use duration was documented in only one study [A5]. The average length of ICU stay reported in five studies ranged from 5.0 to 10.7 days, with no significant difference between the experimental and control groups [A1-3,A5,A6] (Table 2).
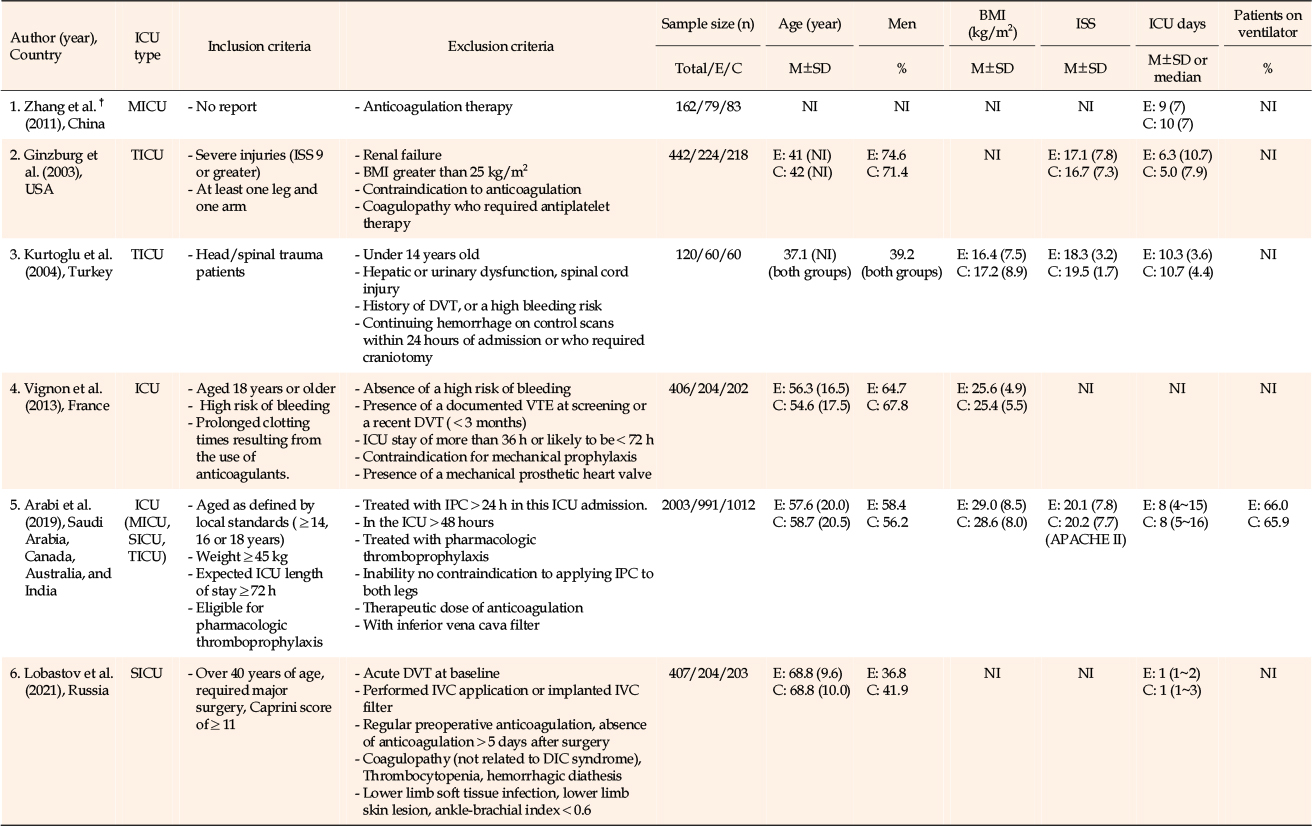
Table 2
Characteristics of Trials and Subjects (N=6)
The types of IPC interventions were categorized as follows: IPC alone [A1,A3,A4], IPC combined with Graduated Compression Stockings (GCS) [A2], IPC combined with an anticoagulant [A5], and IPC combined with both an anticoagulant and GCS [A6].
Regarding the types of IPC intervention and control groups, single interventions were categorized as either IPC alone compared with a control group [A1] or IPC alone compared with an anticoagulant [A3,A4]. Combined interventions were defined as IPC and GCS used together and compared with GCS alone [A2], IPC and an anticoagulant used together and compared with an anticoagulant plus Elastic Compression Stockings (ECS), or a comparison involving an anticoagulant and ECS used together [A6]. Two types of compression stockings were identified: graduated and elastic. In all four studies, LMWH was employed as the anticoagulant [A3-A6].
The mode of application for IPC was sequential compression in three studies [A3,A5,A6], while the remaining three studies did not report the mode used. Regarding the sleeve type of the IPC, four studies used thigh-length sleeves [A2,A3,A5,A6], one study used knee-length sleeves [A4], and one study did not report the sleeve type [1].
The initiation of IPC application varied across studies: it occurred immediately after admission to the ICU in two studies [A2,A4], within 24 or 48 hours of ICU admission in another two [A3,A5], prior to surgery in one study [A6], and was not reported in one study [A1].
The duration of IPC application ranged from 6 days [A2,A3,A5] to 28 days [A5] in cases where DVT or PE was suspected or confirmed. Two studies did not report the duration of IPC application [A1,A4]. The daily duration of IPC application varied, with some studies specifying continuous use throughout the day [A2], 22 hours [A5], 18 hours [A6], or 16 hours [A3]. This information was not reported in two of the studies [A1,A4] (Table 3).
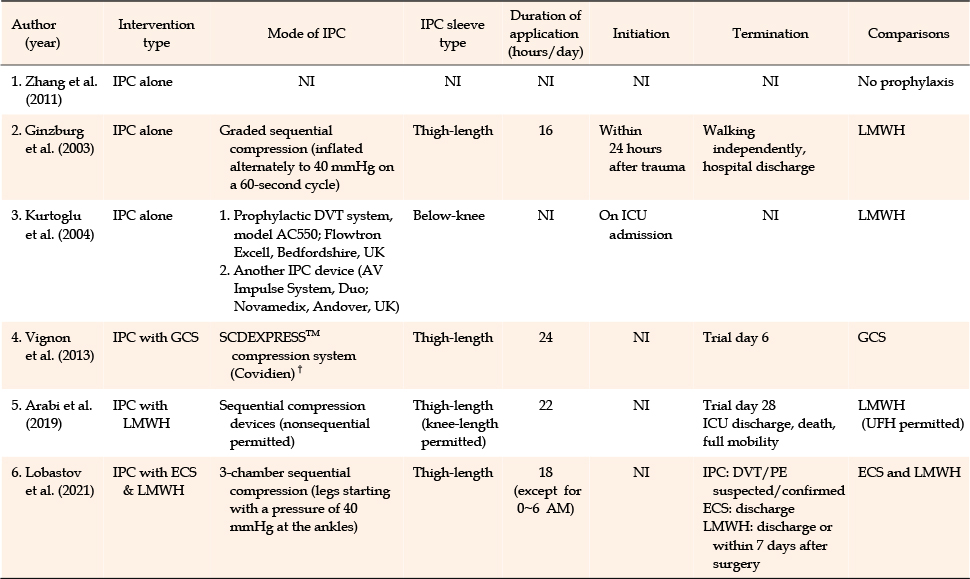
Table 3
Details of Interventions (N=6)
One of the four studies [A1-A3,A5] that reported occurrences of DVT noted a statistically significant decrease in the group using IPC alone compared to the control group [A1]. No significant efficacy was observed in two studies [A2,A3] when compared to LMWH alone, and one study [A5] evaluated the additional effects of combining IPC with LMWH.
No significant effect on P-DVT was observed in either of the studies that compared the additional effects of combining GCS with LMWH [A4,A5], or in the study that compared the additional effects of combining IPC with GCS and LMWH [A6]. Among the two studies [A4,A6] that reported on the occurrence of D-DVT, one study [A6] found a statistically significant reduction with the combined intervention of anticoagulants and GCS. However, the other study [A4] found no significant effect when comparing the additional effects of GCS alone or in combination.
In one out of six studies of PE [A1], IPC alone demonstrated a significant reduction in PE incidence compared to the control group. No difference in PE incidence was observed when comparing IPC with LMWH [A2,A3], IPC combined with LMWH versus LMWH alone [A5], or IPC combined with LMWH versus a triple intervention of IPC, LMWH, and ECS compared to a combined intervention of anticoagulants and GCS [A6].
One of the four studies that reported VTE incidence [A2,A4-A6] showed a significant reduction in VTE incidence after a triple intervention of IPC, anticoagulants, and ECS, compared to a combined intervention of anticoagulants and GCS [A6]. No effect on VTE incidence was observed when IPC was combined with LMWH [A2], IPC with GCS was combined with GCS [A4], or IPC and LMWH were combined with LMWH [A5]. Doppler ultrasound was utilized to diagnose DVT in five studies [A1-A3,A5,A6], while one study employed compression ultrasound for diagnosis [A4] (Table 4).
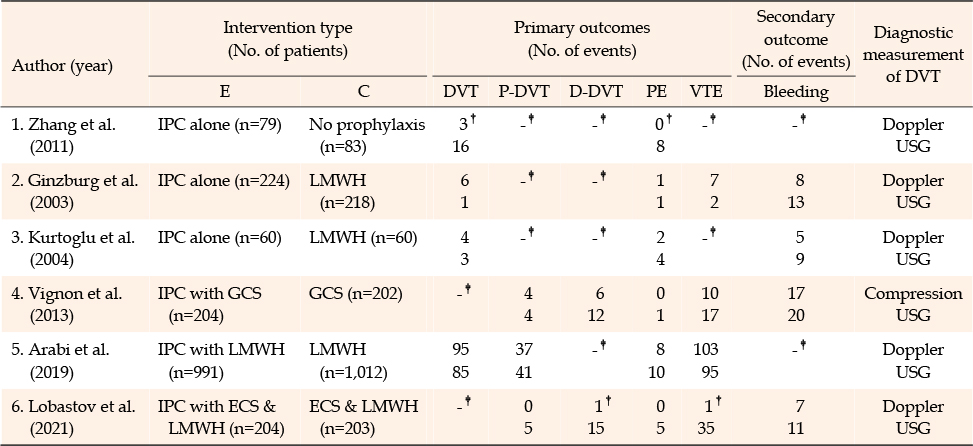
Table 4
Details of Outcomes (N=6)
This study aimed to investigate the characteristics of IPC interventions for thromboprophylaxis in critically ill patients and to analyze their effectiveness. In this section, we discuss the results of the six finally selected RCTs in the sequence of participants, interventions, and outcomes.
The risk factors for VTE are known to include age, BMI, surgery, trauma, cancer, chemotherapy, lower extremity surgery, pelvic fractures, severe infections, inflammatory bowel disease, severe cardiopulmonary disease, stroke, spinal cord injury, immobility due to paralysis, oral contraceptive use, pregnancy and childbirth, anticoagulant disorders, and obesity [6, 17]. The studies reviewed here exhibited inconsistencies due to varying inclusion and exclusion criteria related to bleeding risk factors or VTE risk factors associated with anticoagulant use. Furthermore, the studies differed in terms of disease type, severity, age, and BMI of the participants. These factors can influence the outcomes. Therefore, it is necessary to validate the effectiveness of thromboprophylaxis in a controlled setting, where participant selection or exclusion criteria are standardized, using tools that assess the risk based on severity evaluation criteria or VTE [18, 19, 20, 21].
Anticoagulants, such as warfarin, UFH, and LMWH, are recommended to reduce the risk of VTE in acute or critically ill patients. However, their use is limited by an increased risk of bleeding, which can counterbalance the benefits of thromboprophylaxis [6, 17]. Mechanical thromboprophylaxis, which addresses most elements of Virchow's triad without raising the risk of bleeding, is advised for use either alone or in conjunction with anticoagulants [6, 7]. Among the mechanical thromboprophylaxis options for preventing VTE in critically ill patients who are at risk of bleeding from anticoagulant use, IPC is regarded as the most appropriate and cost-effective choice [22]. The thrombosis prevention guidelines for non-surgical critically ill patients [5] also suggest the use of IPC when anticoagulation is contraindicated or when there are concerns about bleeding.
Our findings identified the following types of IPC interventions: IPC alone, IPC combined with GCS, IPC combined with LMWH, and IPC combined with both ECS and LMWH. IPC alone was compared with either a control group or LMWH, while the combined interventions were compared in a manner that allowed for the assessment of additional effects beyond those of the individual interventions. A previous study [23] reported on the effectiveness of IPC alone and anticoagulant therapy alone in inpatients, as well as the combined use of IPC and LMWH. A retrospective study of ICU patients [24] analyzed the use of IPC alone, LMWH alone, and the combination of IPC and LMWH. Additionally, we identified existing systematic reviews and meta-analyses [9, 10, 11] that compared IPC alone and LMWH alone with a control group, as well as studies comparing IPC alone directly with LMWH alone.
Meanwhile, our findings indicate that the sleeve-type IPC device was utilized in both thigh and calf configurations. A previous non-RCT [25] comparing the effectiveness of calf-thigh and foot types in patients undergoing hip replacement surgery demonstrated that the calf-thigh type was more effective at reducing postoperative thigh edema than the foot type. Future research should focus on comparing the effectiveness of IPC devices according to sleeve type in critically ill patients.
Next, we will discuss the effectiveness of IPC interventions based on the prevention of the risk of developing DVT, PE, and VTE, which are primary outcomes, and the risk of bleeding as a secondary outcome. The impacts on DVT incidence will be discussed in the following three categories.
First, the risk of DVT when using IPC alone was reduced compared to the control group [A1]; however, there was no significant difference when compared to the LMWH group [A2,A3]. The effectiveness of IPC alone in lowering the incidence of DVT in acutely ill patients has been confirmed in surgical patients [26], and its significant thromboprophylactic efficacy has also been established in stroke patients through large-scale, multi-organ RCTs [27]. A systematic review and meta-analysis examining the efficacy and safety of IPC and anticoagulants in neurosurgery patients found that both IPC and anticoagulants were significantly effective in preventing DVT, with comparable efficacy between the two [10]. Our findings align with a study [24] that analyzed the DVT prevention effects of IPC application by reviewing the medical records of 500 medical-surgical ICUs. Another meta-analysis [11] reported on the DVT prevention effect of IPC in ICU patients. Park et al. [9] suggested that IPC alone may reduce the tendency for DVT incidence, but the efficacy in reducing DVT incidence was not definitive; the effect of IPC in lowering the risk of DVT incidence in critically ill patients was not as pronounced as that of prophylactic anticoagulants.
Second, our findings showed that there was no significant difference in the incidence of either proximal or distal DVT when comparing the combined use of IPC and GCS with the use of GCS alone [A4]. A meta-analysis examining the effect of mechanical thromboprophylaxis on DVT in stroke patients [28] found that the included studies were unable to draw definitive conclusions regarding the benefits and risks due to limitations such as small sample sizes, diverse intervention methods, and varying DVT diagnostic techniques. In 2009, a multicenter RCT conducted across 64 centers in the UK, Italy, and Australia involved 2,518 patients who were immobilized and hospitalized within one week of an acute stroke [27]. The study reported that the incidence of DVT in patients who were administered thigh-level GCS did not significantly differ from that in the control group [27]. Additionally, the GCS group experienced a higher occurrence of skin damage, including ulcers, blisters, and skin necrosis, leading to the conclusion that thigh-length GCS provided no benefit to patients hospitalized for acute stroke [27]. Previous studies analyzing 326 medical records of critically ill patients found no difference in the incidence of DVT when comparing interventions with IPC, GCS, or elastic bandages [29]. However, when the venous blood flow rate was examined to compare the thromboprophylactic effects of CS and IPC in neurosurgical ICU patients, it was suggested that IPC might be more effective in preventing DVT than CS [30]. Furthermore, two meta-analyses [10, 31] confirmed that IPC is more effective than GCS in preventing DVT. Fernando et al. [32] reported that LMWH was effective in reducing the incidence of DVT in critically ill patients compared to the control group. In contrast, the effects of UFH, IPC, and mechanical pressure (both IPC and GCS) did not differ significantly. Additionally, the study could not confirm the thromboprophylactic effect of combining mechanical pressure with anticoagulant interventions.
Third, there was no observed difference in the incidence of DVT and P-DVT between the combined intervention of LMWH and IPC compared to LMWH alone [A5]. Similarly, no difference in P-DVT incidence was found when comparing the combined use of ECS and LMWH to LMWH alone, although differences in D-DVT incidence were noted. Furthermore, the additional benefit of combining IPC with anticoagulants could not be established. A previous meta-analysis [23] indicated that adding anticoagulants to IPC did not significantly affect the reduction of DVT incidence. However, another study suggested that incorporating IPC with anticoagulants decreased the incidence of DVT in surgical patients [33]. In summary, the efficacy of IPC alone in preventing DVT in critically ill patients was confirmed, and it was found to be as effective as LMWH. However, the study could not confirm either the added benefit of combining IPC with anticoagulants or its relative superiority to GCS. These conclusions are tentative due to the small number of studies included, the variability in participant characteristics and conditions, and the differences in the types of interventions across studies. Consequently, the generalizability of these results is limited until further research is available.
The efficacy of IPC alone in preventing PE was established in comparison with a control group [A1]. However, no significant difference was observed in the incidence of PE between the IPC and LMWH groups [A2,A3], indicating neither an additional benefit of LMWH nor an enhanced effect from the triple intervention involving IPC [A6]. Previous systematic reviews and meta-analyses [23, 33] have been unable to confirm the benefit of adding anticoagulants to reduce the risk of PE in inpatients, although the supplementary effect of IPC has been verified. In contrast, no difference in PE prevention was noted among critically ill patients [24]. Therefore, while the efficacy of IPC in preventing proximal DVT and PE has not been conclusively demonstrated, one study [3] did find that IPC significantly reduced the occurrence of proximal DVT and PE. Consequently, further research is necessary to determine the thromboprophylactic impact of IPC on proximal DVT and PE.
The efficacy of interventions to reduce the incidence of VTE was confirmed in one study that compared a triple intervention of IPC, LMWH, and ECS with a combined intervention of anticoagulants and GCS [A6]. However, no difference in VTE incidence was observed between the combined use of IPC and GCS [A4] and the combination of IPC and LMWH [A5]. A previous study [34] reported that IPC was as effective as anticoagulants in preventing VTE in surgical patients. Furthermore, combining anticoagulants with IPC could reduce the risk of VTE more than anticoagulants alone, and IPC was associated with a lower risk of major bleeding compared to anticoagulants [34]. Meta-analyses [10, 11] investigating the efficacy of IPC in preventing VTE in critically ill patients found no difference between IPC and LMWH, nor was there an additional effect when IPC was added to LMWH. However, this study included research that demonstrated effectiveness in preventing VTE, leading to results that differed from previous studies [10, 11]. Since the criteria for VTE occurrence varied across studies, further research with clearly defined indicators is necessary to validate these findings.
For the secondary outcome, which was the prevention of bleeding, there was no significant difference in efficacy between IPC and LMWH [A2,A3]. In a comparison of a triple intervention involving IPC, LMWH, and ECS with a combined intervention of IPC and ECS, there was a trend toward reduced bleeding with the addition of IPC, but the difference was not statistically significant [A4,A6]. A previous study [23] confirmed the effectiveness of combining IPC with anticoagulants for all patients requiring thromboprophylaxis; however, the addition of an anticoagulant increased the risk of bleeding compared to using IPC alone. No increase in bleeding risk was observed when IPC was combined with anticoagulants, as opposed to anticoagulant therapy alone. Other studies [9, 24] found no significant difference in bleeding risk between IPC and LMWH in critically ill patients, although IPC was associated with a lower risk of bleeding than LMWH in some reports [10]. Haykal et al. [11] noted that due to insufficient data, conclusions regarding the incidence of bleeding from IPC and LMWH interventions should be reserved until more empirical evidence is available.
Considering the bleeding risk associated with anticoagulants, our findings revealed that IPC alone is effective for thromboprophylaxis, showing no difference in efficacy compared to LMWH. Therefore, this study is significant as it confirms the value of both anticoagulants and IPC as thromboprophylaxis interventions in critical care nursing.
This study systematically reviewed six RCTs that assessed the impact of IPC alone or in combination with other interventions on DVT, PE, VTE, and bleeding as a thromboprophylactic strategy in ICU patients. The interventions included three studies of IPC alone, one study of IPC with GCS, one study of IPC with anticoagulants, and one study combining IPC, GCS, and anticoagulants. Additionally, the comparison groups in the three studies of IPC alone consisted of one with no prophylaxis and two with anticoagulants. Consequently, this study was limited by the inability to derive pooled estimates from the meta-analysis to confirm quantitative efficacy.
Based on our findings, we make the following recommendations: First, considering the application of IPC and the administration methods of LMWH, as well as the diagnostic methods for DVT, PE, and VTE, we propose a systematic review and meta-analysis that includes non-RCT studies in addition to the limited number of RCTs. Second, we suggest further research into the various application modes of combined interventions with anticoagulants and IPC as a thromboprophylactic strategy for patients who require thrombus prevention but are at high risk of bleeding or are contraindicated for anticoagulant use. Third, there is a need for a study to compare the application modes of IPC devices and the efficacy of thromboprophylaxis according to the type of sleeve used. Fourth, we recommend a study to compare and validate the effectiveness of thromboprophylaxis using IPC against that of a foot pump. Fifth, we advocate for research to verify the efficacy of IPC alone or in combination with other interventions, taking into account patient severity, the presence of risk factors, and the assessment of VTE risk.
This study systematically reviewed RCTs that evaluated IPC interventions for thrombus prevention in critically ill patients. The effectiveness of IPC alone in preventing thrombus formation was established, and additional benefits were observed when IPC was combined with anticoagulants and GCS. However, these effects were each demonstrated in only a single study, and no significant differences in effectiveness were noted when comparing anticoagulants or GCS with IPC alone. The findings suggest the potential for using IPC as a thromboprophylactic strategy in critically ill patients who are at an increased risk of bleeding or for whom anticoagulants are contraindicated. Consequently, there is a need for studies that consider the unique characteristics of critically ill patients and RCTs that assess the thromboprophylactic efficacy of IPC, either as a standalone intervention or in combination with other treatments.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - RS, KNY, and KY-H.
Data collection - RS, KNY, and KY-H.
Analysis of the data - KNY.
Interpretation of the data - RS and KNY.
Drafting of the manuscript - RS, KNY, and KY-H.
Critical revision of the manuscript - RS-A, and KY-H.
A1. Zhang C, Zeng W, Zhou H, Zheng BX, Cheng JC, Li XY, et al. The efficacy of intermittent pneumatic compression in the prevention of venous thromboembolism in medical critically ill patients. Chinese Critical Care Medicine. 2011;23(9):563-5.
A2. Ginzburg E, Lopez J, Jackowski J, Brown M, Hameed SM. Randomized clinical trial of intermittent pneumatic compression and low molecular weight heparin in trauma. British Journal of Surgery. 2003;90(11):1338-44. https://doi.org/10.1002/bjs.4309
A3. Kurtoglu M, Yanar H, Bilsel Y, Guloglu R, Kizilirmak S, Buyukkurt D, et al. Venous thromboembolism prophylaxis after head and spinal trauma: intermittent pneumatic compression devices versus low molecular weight heparin. World Journal of Surgery. 2004;28(8):807-11. https://doi.org/10.1007/s00268-
A4. Vignon P, Dequin PF, Renault A, Mathonnet A, Paleiron N, Imbert A, et al. Intermittent pneumatic compression to prevent venous thromboembolism in patients with high risk of bleeding hospitalized in intensive care units: the CIREA1 randomized trial. Intensive Care Medicine. 2013;39(5):872-80. https://doi.org/10.1007/s00134-
A5. Arabi YM, Al-Hameed F, Burns KEA, Mehta S, Alsolamy SJ, Alshahrani MS, et al. Adjunctive intermittent pneumatic compression for venous thromboprophylaxis. The New England Journal of Medicine. 2019;380(14):1305-15. https://doi.org/10.1056/NEJMoa1816150
A6. Lobastov K, Sautina E, Alencheva E, Bargandzhiya A, Schastlivtsev I, Barinov V, et al. Intermittent pneumatic compression in addition to standard prophylaxis of postoperative venous thromboembolism in extremely high-risk patients (IPC SUPER): a randomized controlled trial. Annals of Surgery. 2021;274(1):63-9. https://doi.org/10.1097/SLA.0000000000004556
 E-SUBMISSION
E-SUBMISSION