Abstract
-
Purpose
This study aimed to identify a clinically meaningful cut-off score on the Pressure Ulcer Scale for Healing tool for objectively determining healing in adult inpatients with pressure injury.
-
Methods
A retrospective analysis was conducted using electronic health records from adult inpatients at a tertiary hospital in South Korea. Pressure Ulcer Scale for Healing scores were calculated based on wound size, exudate amount, and tissue type. Receiver operating characteristic curve analyses were performed, and optimal cut-off scores were identified using the Youden Index. Stratified analyses by pressure injury stage were also conducted to evaluate predictive performance.
-
Results
A total of 20,476 pressure injuries were analyzed, of which 5,873 were classified as healed. Although all stages were initially included, stage 1 pressure injuries demonstrated limited discriminative ability (area under the curve=0.612) and were therefore excluded from cut-off derivation. For stage 2 or higher pressure injuries, the optimal cut-off score was 3.5, yielding an area under the curve of 0.721, with a sensitivity of 59.8% and a specificity of 72.0%.
-
Conclusion
The identified threshold for stage 2 or higher pressure injuries demonstrated meaningful discriminative ability for determining wound healing status. Application of this criterion may support more objective and consistent clinical decision-making when using the Pressure Ulcer Scale for Healing in nursing practice.
-
Key Words: Pressure ulcer; Wound healing; Nursing assessment
INTRODUCTION
A pressure injury (PI) involves localized damage to the skin and underlying tissues that is primarily caused by prolonged pressure or shear force [
1]. PI development or progression prolongs hospitalization and increases the burden on both patients and healthcare systems. According to a recent systematic review, the occurrence of pressure ulcers extended hospital length of stay by an average of 12.9 days [
2]. Nurses play a pivotal role in preventing PI, identifying early signs of skin breakdown, and facilitating wound healing through evidence-based interventions [
1,
3]. As PI prevention and management are core components of independent nursing practice, accurate clinical judgment is essential for improving patient outcomes. Therefore, consistent and objective assessment using reliable tools is crucial for accurately evaluating wound healing and supporting effective nursing decision-making [
4].
Various tools have been developed to objectively evaluate and monitor PI healing, including the Bates-Jensen Wound Assessment Tool (BWAT), the Photographic Wound Assessment Tool (PWAT), and the Pressure Ulcer Scale for Healing (PUSH). The BWAT provides a comprehensive evaluation across 13 wound-related parameters [
5]. However, limited reliability evidence and variation in evaluation time across wound sites hinder its feasibility in busy clinical settings [
6]. The PWAT enables objective and reproducible wound assessment through the use of standardized photographic images [
7]. However, its clinical feasibility may be constrained by requirements for consistent image quality and appropriate imaging equipment [
8].
Given these limitations, a simpler and more clinically applicable tool is necessary for the routine evaluation of PI healing. PUSH, developed by the National Pressure Injury Advisory Panel (NPIAP), assesses wound healing using three components—wound size, exudate amount, and tissue type—thereby enabling a streamlined and consistent evaluation process in clinical practice. Previous validation studies have demonstrated the effectiveness of PUSH in monitoring PI healing [
9,
10], and a recent systematic review reported comparatively higher levels of evidence for its validity and responsiveness relative to other wound assessment instruments [
8].
PUSH evaluates PI healing based on three components, allowing changes in the total score to reflect either improvement or deterioration [
11]. Because PI healing is an important indicator of nursing practice quality and patient outcomes [
12], accurate assessment of healing status is essential. Although previous studies have validated PUSH and examined healing trajectories through reductions in score [
11], a score of 0 may not always represent the only state of complete healing. According to the international clinical practice guideline issued by the NPIAP, a PI is considered to have healed when complete epithelialization has occurred with no open areas [
1]. However, in clinical practice, even when full epithelialization is observed, nurses may experience difficulty documenting a wound size of zero because of subtle pigmentation differences or the presence of thin, newly formed epithelial layers. Accordingly, clinically healed wounds may not consistently receive a PUSH score of 0 in real-world practice.
Therefore, identifying a clinically meaningful cut-off score that reflects documentation patterns in routine clinical settings may enhance the interpretability of PUSH scores and improve objectivity in wound healing assessment. This study aims to determine an objective and practical cut-off point that can support consistent nursing assessment and enhance the clinical utility of PUSH in PI management.
METHODS
1. Study Design
This retrospective study was conducted at a tertiary general hospital in South Korea. Data were extracted from the hospital’s electronic health record (EHR) system. The study period spanned from January 1, 2022, to December 31, 2024, and focused on nursing documentation related to PI management, including wound assessments and documentation of healing status. The study is reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines.
2. Study Population
This study included adult inpatients aged 19 years or older who had PIs either present at the time of admission (community-acquired) or that developed during hospitalization (hospital-acquired). For the purpose of determining the cut-off PUSH score for wound healing, patients were categorized into two groups: those whose nursing records explicitly documented the wound as “healed,” and those without such documentation, for whom the most recent PUSH score prior to discharge was used as a proxy indicator of non-healed status.
Patients were excluded if they were younger than 19 years of age, discharged on the same day as admission, or if the PI occurred in a location outside the general ward or intensive care unit. These cases were excluded because patients in non-inpatient settings are not consistently evaluated using standardized wound assessment protocols, which makes it difficult to determine the timing and origin of the injury, ensure accurate staging, and distinguish PIs from other wound types. In addition, cases in which the onset and healing dates of the PI were recorded as occurring on the same day were excluded, as these were considered likely to reflect documentation errors. A total of 20,476 PIs were included in the final analysis.
3. Data Collection
Data required to calculate the PUSH score were extracted from the hospital’s EHR system. The EHR system contained structured and coded wound assessment fields aligned with the PUSH tool, allowing nurses to document wound size, exudate amount, and tissue type using predefined categories (e.g., none, light, moderate, heavy for exudate amount).
A single researcher, a registered nurse with more than 10 years of clinical experience and formal training in wound assessment, reviewed the extracted data and computed the total PUSH score based on the documented values. Because the PUSH tool applies explicit scoring criteria, the researcher verified the individual item values and calculated the summed scores without subjective interpretation.
When a patient had multiple PIs, each wound was analyzed as an independent case. Cases were included only when complete data for all three PUSH components were available; records with missing values were excluded because total scores could not be calculated.
Healing status was also obtained from structured EHR fields. In the system, wounds documented as “healed” were coded as such by nurses as part of routine clinical documentation practices. For the receiver operating characteristic (ROC) analysis, this variable was used as the state indicator, with “1” representing healed wounds and “0” representing non-healed wounds.
4. Ethical Considerations
This study was approved by the Institutional Review Board of Samsung Medical Center prior to data collection (IRB No. SMC IRB 2025-02-130). Given the retrospective nature of the study, the requirement for informed consent was waived by the IRB. To ensure confidentiality, all personally identifiable information was either deleted or encrypted during the data extraction process.
5. Data Analysis
All statistical analyses were performed using IBM SPSS ver. 28.0 (IBM Corp., Armonk, NY, USA), with the significance level set at p<.05.
For continuous variables, independent-samples t-tests were used to compare differences between the healed and non-healed groups. Categorical variables were analyzed using chi-square tests. The normality of the final PUSH score was assessed using the Kolmogorov–Smirnov test, and as it violated the assumption of normality, the Mann–Whitney U test was additionally performed.
To determine the optimal cut-off value of the PUSH score for predicting wound healing, ROC curve analysis was conducted. The area under the curve (AUC) was calculated to evaluate the discriminatory power of the PUSH score, and the optimal cut-off point was identified using the Youden Index, which maximizes the sum of sensitivity and specificity.
RESULTS
1. Participant Characteristics
A total of 20,476 PIs were included in the analysis. Among these, 5,873 cases (28.7%) were classified as healed and 14,603 cases (71.3%) as non-healed, based on documented healing status in the EHR. Participant characteristics are summarized in
Table 1.
Patients in the healed group were younger than those in the non-healed group (p<.001), and the proportion of male patients was higher in the healed group. Hospital-acquired PIs were more common overall, and their proportion was significantly higher in the non-healed group. PIs associated with intensive care unit stays accounted for a larger proportion of healed cases than non-healed cases.
Stage distribution also differed between groups, with stage 1 more frequently observed among healed PI, whereas stage 1 and stage 2 were both common in the non-healed group. The most frequent anatomical sites were the coccyx and the ear, with coccygeal PIs more common in the non-healed group and ear-related PIs more frequent in the healed group.
Taken together, these findings indicate meaningful baseline differences between the healed and non-healed groups with respect to demographic characteristics, care setting, and wound-related features.
2. Distribution and Trends of PUSH Scores
The distribution of PUSH scores differed between the healed and non-healed groups. Overall, the healed group demonstrated lower PUSH scores with a narrower distribution, whereas the non-healed group exhibited higher scores with greater variability. Specifically, the mean PUSH score was lower in the healed group than in the non-healed group, indicating a more favorable wound status among healed cases. These findings suggest distinct score patterns between groups and support the relevance of PUSH scores in reflecting wound healing status.
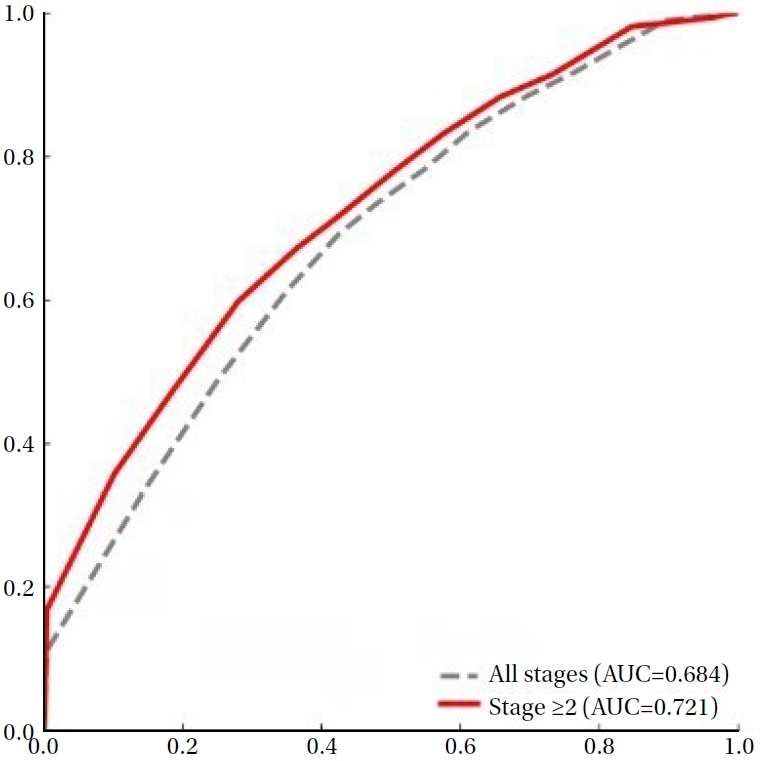
3. ROC Curve Analysis
The predictive performance of the PUSH score for identifying PI healing was evaluated using ROC curve analysis. Across all PI stages, the PUSH score demonstrated acceptable discriminatory ability, with an AUC of 0.684 and an optimal cut-off value of 4.5 as determined by the Youden Index (
Figure 1). Stage-specific analyses showed increasing discriminative performance with greater PI severity, with the highest AUC observed in stage 3 injuries.
To account for clinical variation and the high prevalence of stage 1 PI, additional stratified analyses were performed. When analyses were restricted to stage ≥2 cases, the AUC increased to 0.721, and further increased to 0.738 among stage ≥3 cases, indicating enhanced predictive utility in more advanced wounds. These findings suggest that PUSH scores are more informative for wounds involving tissue loss and may serve as a useful tool for supporting clinical decision-making in PI management. Detailed ROC results and cut-off values by PI stage are summarized in
Table 2.
DISCUSSION
This study identified a clinically meaningful cut-off score of 3.5 on the PUSH tool for predicting healing in stage ≥2 PI. Although the PUSH tool is widely used to monitor wound progression in clinical practice [
9], a specific threshold indicating wound healing has not been clearly established. The present finding provides objective evidence to support more consistent and clinically interpretable use of PUSH scores in the inpatient setting.
This study aimed to establish a clinically interpretable healing threshold for PIs that can be meaningfully applied in clinical settings. To place the proposed healing cut-off within an appropriate clinical context, stratified analyses by PI stage were conducted (
Table 2), with interpretation guided by stage-specific clinical characteristics and documentation patterns.
Stage 1 PIs were not considered appropriate for defining a healing cut-off. Clinically, stage 1 PIs present as non-blanching erythema without overt tissue damage and frequently resolve without formal intervention [
13]. From a documentation perspective, healing of stage 1 injuries is often not explicitly recorded in retrospective EHR–based data, increasing the risk of misclassification. Consistent with prior research that excluded stage 1 PIs from predictive analyses to enhance classification validity [
14], this study omitted stage 1 injuries to improve reliability in determining true healing status.
Conversely, defining a cut-off based solely on stage ≥3 PIs was also considered inappropriate. Although stage ≥3 PIs tended to demonstrate better discriminatory performance, such severe wounds account for a relatively small proportion of cases encountered in routine clinical practice. As a result, thresholds derived exclusively from stage ≥3 PIs are difficult to generalize to the broader inpatient population.
In contrast, stage ≥2 PIs represent wounds that are commonly encountered, require ongoing clinical assessment, and necessitate active wound management. These injuries are also more consistently documented in clinical records, providing a stable and clinically meaningful basis for interpretation. Within this clinically relevant context, the present study identified a PUSH cut-off score of 3.5 for stage ≥2 PI.
Previous research has primarily reported average PUSH scores for healed and unhealed wounds rather than identifying a specific healing threshold. For example, one study reported baseline mean PUSH scores of 7.00±0.48 and 13.2±2.11 for healed and unhealed PI, respectively [
14], demonstrating that complete wound closure did not necessarily correspond to a PUSH score of zero. This observation supports the rationale for the present study by emphasizing the need for a clinically interpretable cut-off score rather than assuming that wound resolution equates to a score of zero.
The present study differs from prior research by explicitly defining a clinically interpretable healing cut-off and by grounding this threshold in a broader and more representative clinical context. Whereas earlier studies were restricted to narrower stage ranges—typically including only stage 2, 3, and 4 PI—and small sample sizes, the current analysis incorporated a wide spectrum of PI, including unstageable and deep tissue injuries, using a large real-world inpatient dataset. This broader inclusion more closely reflects routine clinical practice and strengthens the generalizability and robustness of the proposed cut-off.
Nevertheless, several limitations should be acknowledged when interpreting these findings. First, this study employed a retrospective design and relied solely on nursing documentation, which may vary in completeness and accuracy. Second, only cases explicitly documented as “healed” were classified as healed; therefore, wounds that were nearly healed but not recorded as such may have been misclassified, potentially introducing selection bias. Third, the analysis was conducted in a single tertiary hospital and included only adult inpatients aged 19 years or older, which may limit generalizability to other healthcare settings or patient populations. Finally, the PUSH score was applied retrospectively rather than in real time, which may not fully reflect its use in routine clinical practice.
Future research may build on these findings through prospective, multicenter studies to validate the proposed cut-off across diverse clinical settings. In addition, predictive modeling approaches incorporating patient characteristics and baseline wound parameters—such as logistic regression or other multivariable methods—could be applied to estimate healing probability at earlier stages of care [
15,
16]. Building on the cut-off identified in the present study, such approaches may further support clinical decision-making by offering earlier prognostic insight.
Despite these limitations, this study advances understanding of PI healing by establishing a statistically and clinically meaningful PUSH cut-off score for stage ≥2 PI. By grounding this threshold in a large real-world inpatient dataset and routine documentation practices, the present study moves beyond descriptive reporting of PUSH score trajectories and provides a practical reference for assessing healing status. This contribution supports a more objective, consistent, and evidence-based interpretation of PUSH scores and facilitates wider integration of standardized PI assessments into routine nursing practice.
CONCLUSION
This study established a clinically meaningful PUSH cut-off score of 3.5 for identifying healing in stage ≥2 PIs. Stratified analyses demonstrated that stage ≥2 PIs represent the most appropriate population for applying this threshold. By providing an objective criterion for interpreting PUSH scores, these findings support more consistent PI assessment and may enhance clinical decision-making in practice.
-
CONFLICTS OF INTEREST
The authors declared no conflict of interest.
-
AUTHORSHIP
Study conception and design acquisition - JL and SP; data curation and analysis - JL and SP; funding acquisition - SP and JH; investigation - JL; project administration and supervision - JL, SP, and JH; resources and software - JL; validation - JL and SP; visualization - JL; and drafting and critical revision of the manuscript - JL, SP, and JH.
-
Funding
This study was supported by the research fund of the Department of Nursing, Samsung Medical Center in 2025 (No. SMC-NSD-2025-14).
-
ACKNOWLEDGEMENT
None.
-
DATA AVAILABILITY STATEMENT
This study used electronic health records from Samsung Medical Center. The data are not publicly available due to institutional regulations but may be available upon reasonable request to the corresponding author with approval from the Institutional Review Board.
Figure 1.Receiver operating characteristic curves for Pressure Ulcer Scale for Healing scores in predicting pressure injury healing in all stages vs. stage ≥2. AUC=area under the curve.
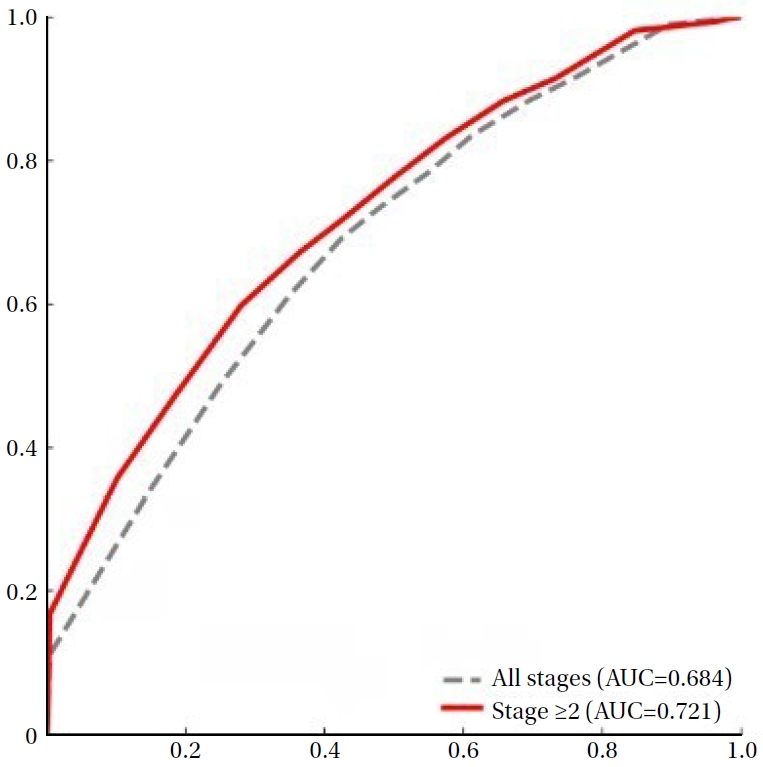
Table 1.Comparison of Participant Characteristics between Healed and Non-healed Pressure Injuries
|
Variables |
Healed (n=5,873) |
Non-healed (n=14,603) |
p-value |
|
M±SD or n (%) |
|
Age (year) |
66.24±14.24 |
68.63±13.63 |
<.001 |
|
Sex |
|
|
<.001 |
|
Female |
1,718 (29.3) |
5,115 (35.0) |
|
|
Male |
4,155 (70.7) |
9,488 (65.0) |
|
|
PI origin |
|
|
<.001 |
|
Hospital-acquired |
4,336 (73.8) |
11,844 (81.1) |
|
|
Community-acquired |
1,537 (26.2) |
2,759 (18.9) |
|
|
Ward type |
|
|
<.001 |
|
General ward |
4,039 (68.8) |
12,300 (84.2) |
|
|
Intensive care unit |
1,834 (31.2) |
2,303 (15.8) |
|
|
PI stage |
|
|
<.001 |
|
Stage 1 |
3,073 (52.3) |
5,389 (36.9) |
|
|
Stage 2 |
1,496 (25.5) |
4,753 (32.5) |
|
|
Stage 3 |
90 (1.5) |
611 (4.2) |
|
|
Stage 4 |
6 (0.1) |
91 (0.6) |
|
|
Unstageable |
328 (5.6) |
1,446 (9.9) |
|
|
Deep tissue injury |
880 (15.0) |
2,313 (15.8) |
|
|
PI location |
|
|
<.001 |
|
Coccyx |
949 (16.2) |
4,924 (33.7) |
|
|
Ear |
2,374 (40.4) |
3,362 (23.0) |
|
|
Buttock |
557 (9.5) |
1,623 (11.1) |
|
|
Trochanter |
232 (4.0) |
983 (6.7) |
|
|
Initial PUSH score |
4.64±3.24 |
6.21±3.70 |
<.001 |
|
Final PUSH score†
|
3.62±3.18 |
5.96±3.76 |
<.001 |
Table 2.Receiver Operating Characteristic Curve Analysis of Pressure Ulcer Scale for Healing Scores by Pressure Injury Stage
|
PI stages |
AUC (95% CI) |
Cut-off |
Sensitivity (%) |
Specificity (%) |
Youden Index |
|
Stage 1 |
0.612 (0.600–0.624) |
4.5 |
71.2 |
46.8 |
0.180 |
|
Stage 2 |
0.708 (0.692–0.723) |
3.5 |
63.4 |
67.0 |
0.303 |
|
Stage 3 |
0.781 (0.733–0.830) |
7.5 |
78.9 |
64.0 |
0.429 |
|
Stage 4 |
0.532 (0.240–0.824) |
9.5 |
50.0 |
78.0 |
0.280 |
|
Unstageable |
0.705 (0.673–0.737) |
4.5 |
57.0 |
72.1 |
0.291 |
|
Deep tissue injury |
0.729 (0.709–0.748) |
5.5 |
72.5 |
60.8 |
0.333 |
|
All stages |
0.684 (0.676–0.692) |
4.5 |
69.2 |
57.5 |
0.267 |
|
Stage ≥2 |
0.721 (0.711–0.732) |
3.5 |
59.8 |
72.0 |
0.318 |
|
Stage ≥3 |
0.738 (0.722–0.753) |
4.5 |
62.6 |
71.6 |
0.341 |
REFERENCES
- 1. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised national pressure ulcer advisory panel pressure injury staging system: revised pressure injury staging system. J Wound Ostomy Continence Nurs. 2016;43(6):585-97. https://doi.org/10.1097/WON.0000000000000281
- 2. Hasan B, Bechenati D, Bethel HM, Cho S, Rajjoub NS, Murad ST, et al. A systematic review of length of stay linked to hospital-acquired falls, pressure ulcers, central line-associated bloodstream infections, and surgical site infections. Mayo Clin Proc Innov Qual Outcomes. 2025;9(3):100607. https://doi.org/10.1016/j.mayocpiqo.2025.100607
- 3. Cordina J, Rolls K, Sim J. Nurses’ clinical decision-making about pressure injury prevention in hospital settings: a scoping review. J Adv Nurs. 2025;81(9):5763-92. https://doi.org/10.1111/jan.16776
- 4. Kottner J, Cuddigan J, Carville K, Balzer K, Berlowitz D, Law S, et al. Prevention and treatment of pressure ulcers/injuries: the protocol for the second update of the international Clinical Practice Guideline 2019. J Tissue Viability. 2019;28(2):51-8. https://doi.org/10.1016/j.jtv.2019.01.001
- 5. Bates-Jensen BM. The pressure sore status tool a few thousand assessments later. Adv Wound Care. 1997;10(5):65-73.
- 6. Bates-Jensen BM, McCreath HE, Harputlu D, Patlan A. Reliability of the Bates-Jensen Wound Assessment Tool for pressure injury assessment: the pressure ulcer detection study. Wound Repair Regen. 2019;27(4):386-95. https://doi.org/10.1111/wrr.12714
- 7. Houghton PE, Kincaid CB, Campbell KE, Woodbury MG, Keast DH. Photographic assessment of the appearance of chronic pressure and leg ulcers. Ostomy Wound Manage. 2000;46(4):20-6, 28-30.
- 8. Smet S, Probst S, Holloway S, Fourie A, Beele H, Beeckman D. The measurement properties of assessment tools for chronic wounds: a systematic review. Int J Nurs Stud. 2021;121:103998. https://doi.org/10.1016/j.ijnurstu.2021.103998
- 9. Gardner SE, Frantz RA, Bergquist S, Shin CD. A prospective study of the Pressure Ulcer Scale for Healing (PUSH). J Gerontol A Biol Sci Med Sci. 2005;60(1):93-7. https://doi.org/10.1093/gerona/60.1.93
- 10. Choi EP, Chin WY, Wan EY, Lam CL. Evaluation of the internal and external responsiveness of the Pressure Ulcer Scale for Healing (PUSH) tool for assessing acute and chronic wounds. J Adv Nurs. 2016;72(5):1134-43. https://doi.org/10.1111/jan.12898
- 11. Stotts NA, Rodeheaver GT, Thomas DR, Frantz RA, Bartolucci AA, Sussman C, et al. An instrument to measure healing in pressure ulcers: development and validation of the Pressure Ulcer Scale for Healing (PUSH). J Gerontol A Biol Sci Med Sci. 2001;56(12):M795-9. https://doi.org/10.1093/gerona/56.12.m795
- 12. Monaco D, Iovino P, Lommi M, Marano G, Zaghini F, Vellone E, et al. Outcomes of wound care nurses' practice in patients with pressure ulcers: an integrative review. J Clin Nurs. 2021;30(3-4):372-84. https://doi.org/10.1111/jocn.15583
- 13. Shi C, Dumville JC, Cullum N. Skin status for predicting pressure ulcer development: a systematic review and meta-analyses. Int J Nurs Stud. 2018;87:14-25. https://doi.org/10.1016/j.ijnurstu.2018.07.003
- 14. Gunes UY. A prospective study evaluating the Pressure Ulcer Scale for Healing (PUSH Tool) to assess stage II, stage III, and stage IV pressure ulcers. Ostomy Wound Manage. 2009;55(5):48-52.
- 15. Berezo M, Budman J, Deutscher D, Hess CT, Smith K, Hayes D. Predicting chronic wound healing time using machine learning. Adv Wound Care (New Rochelle). 2022;11(6):281-96. https://doi.org/10.1089/wound.2021.0073
- 16. Cho SK, Mattke S, Gordon H, Sheridan M, Ennis W. Development of a model to predict healing of chronic wounds within 12 weeks. Adv Wound Care (New Rochelle). 2020;9(9):516-24. https://doi.org/10.1089/wound.2019.1091


 E-SUBMISSION
E-SUBMISSION
