1Department of Nursing, Dongju College, Busan, Korea
2Department of Nursing, Dong-A University, Busan, Korea
© 2018 Korean Society of Adult Nursing
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/ by-nc/3.0), which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Characteristics of Study Participants (N=240)
| Characteristics | Categories | n (%) or M± SD |
|---|---|---|
| Gender | Male | 173 (72.1) |
| Female | 67 (27.9) | |
| Age (year) | 20~29 | 11 (4.6) |
| 30~39 | 33 (13.7) | |
| 40~49 | 69 (28.8) | |
| 50~59 | 78 (32.5) | |
| ≥60 | 49 (20.4) | |
| 51.00±11.54 | ||
| Marital status | Married | 173 (72.1) |
| Other | 40 (16.7) | |
| Unmarried | 27 (11.2) | |
| Living with | Spouse and child | 141 (58.8) |
| Alone | 38 (15.8) | |
| Spouse | 28 (11.7) | |
| Other | 33 (13.7) | |
| Education level | Junior high school | 39 (16.2) |
| High school | 113 (47.1) | |
| ≥ College | 88 (36.7) | |
| Religion | No | 159 (66.3) |
| Yes | 81 (33.7) | |
| Occupation | Office worker | 81 (33.7) |
| laborer | 51 (21.3) | |
| Other | 40 (16.7) | |
| Service/Trader | 68 (28.3) | |
| Monthly household income (10,000 won) | <100 | 26 (10.8) |
| 100~199 | 72 (30.0) | |
| 200~299 | 73 (30.4) | |
| ≥300 | 30 (12.5) | |
| None | 39 (16.3) | |
| Smoking | Yes | 181 (75.4) |
| No | 59 (24.6) | |
| Type of chronic liver diseases | Chronic hepatitis | 128 (53.3) |
| Alcoholic liver disease | 44 (18.3) | |
| Nonalcoholic liver disease | 11 (4.6) | |
| Liver cirrhosis/liver cancer | 57 (23.8) | |
| Years since diagnosed | <3 | 107 (44.4) |
| 3~5 | 67 (28.1) | |
| 6~9 | 40 (16.6) | |
| ≥10 | 26 (10.8) | |
| 52.04±51.88 (month) | ||
| Current symptom(s) (multiple selection) | Fatigue, weakness | 136 (56.7) |
| Indigestion | 71 (29.6) | |
| None | 60 (25.8) | |
| Insomnia | 58 (24.2) | |
| Oral dryness | 54 (22.5) | |
| Anorexia | 53 (22.1) | |
| Myalgia | 46 (19.0) | |
| Abdominal distension | 27 (11.3) | |
| Edema | 22 (9.6) | |
| Pain in right upper quadrant | 15 (6.5) | |
| Gum bleeding | 13 (5.4) | |
| Itching | 11 (4.6) | |
| Nausea, vomiting | 11 (4.6) | |
| Other | 34 (14.2) |
Characteristics of Study Participants (Continued) (N=240)
| Characteristics | Categories | n (%) or M± SD |
|---|---|---|
| Information related to liver disease | Medical personnel | 119 (49.6) |
| Media (TV, internet) | 66 (27.5) | |
| None | 41 (17.1) | |
| Other | 14 (5.8) | |
| Number of hospitalization in the past | None | 86 (35.8) |
| 1~3 times | 87 (36.3) | |
| ≥4 times | 67 (27.9) | |
| Treatment experience (multiple selection) | Antiviral drugs | 100 (41.7) |
| Arterial embolization | 17 (7.1) | |
| Chemotherapy | 14 (5.8) | |
| Radio-frequency ablation | 7 (2.9) | |
| Liver transplant | 3 (1.3) | |
| Comorbidities (multiple selection) | None | 150 (62.5) |
| Hypertension | 57 (23.8) | |
| Diabetes mellitus | 41 (17.1) | |
| Other | 5 (2.1) | |
| Drinking with | Coworkers/friend | 190 (79.2) |
| Other | 25 (10.4) | |
| Alone | 25 (10.4) | |
| Have been advised about alcohol abstinence | Yes | 165 (68.8) |
| No | 75 (31.3) | |
| Attempted alcohol abstinence | Yes | 148 (61.7) |
| No | 92 (38.3) | |
| Necessity of alcohol abstinence education | Necessary | 195 (81.2) |
| Unnecessary | 45 (18.8) | |
| Frequency of drinking per week | 2.01±1.15 | |
| Amount of drinking (glass/each time) | 8.85±4.72 |
Descriptive Statistics of Measured Variables (N=240)
| Variables | Range | M± SD | Skewness | Kurtosis | Standardized estimate |
|---|---|---|---|---|---|
| Alcohol abstinence behavior | 3~21 | 6.45±5.01 | |||
| To stop drinking within the last two weeks | |||||
| Stopped drinking | 1~7 | 1.97±1.65 | 1.75 | 1.77 | .95 |
| Tried my best | 1~7 | 2.00±1.46 | 1.74 | 1.74 | .95 |
| Drinking refusal self-efficacy | 1~7 | 2.48±1.90 | 0.98 | -0.43 | .83 |
| Alcohol abstinence intention | 4~28 | 15.07±4.06 | |||
| To stop drinking within two weeks | |||||
| Will intend | 1~7 | 3.59±1.14 | 0.56 | -0.31 | .94 |
| Will do my best | 1~7 | 3.77±1.17 | 0.32 | -0.63 | .86 |
| Will aim to stop drinking | 1~7 | 3.62±1.12 | 0.50 | -0.32 | .92 |
| Will refuse a chance to drink | 1~7 | 4.09±1.17 | -0.05 | -0.71 | .67 |
| Alcohol abstinence attitude | 4~28 | 16.32±3.47 | |||
| Bad/good | 1~7 | 4.33±0.97 | -0.56 | 0.66 | .67 |
| Not important/important | 1~7 | 3.92±0.75 | -0.17 | 1.48 | .63 |
| Option/essential | 1~7 | 3.80±0.67 | -0.98 | 0.19 | .72 |
| Hard/simple | 1~7 | 4.27±1.08 | -0.22 | -0.28 | .70 |
| Alcohol abstinence subjective norms | 3~21 | 12.57±3.09 | |||
| Normative belief | 1~7 | 4.23±1.11 | 0.14 | -0.74 | .91 |
| Motivation to comply | 1~7 | 4.21±1.01 | 0.25 | -0.52 | .95 |
| Positive normative belief | 1~7 | 4.13±0.97 | 0.24 | -0.51 | .87 |
| Alcohol abstinence perceived behavioral control | 4~28 | 12.34±3.69 | |||
| Control belief | 1~7 | 3.06±0.94 | 0.39 | -0.65 | .92 |
| Self-efficacy | 1~7 | 3.13±0.84 | 0.24 | -0.87 | .83 |
| Positive control belief | 1~7 | 3.14±0.95 | 0.41 | -0.52 | .96 |
| Control power | 1~7 | 3.01±0.96 | 0.40 | -0.56 | .91 |
Fitness Indices of Hypothetical and Modified Model (N=240)
| Model | x2 (p) | df | x2/df | GFI | AGFI | RMSEA (LO HI) | NFI | TLI | CFI | PNFI |
|---|---|---|---|---|---|---|---|---|---|---|
| Criteria | >.05 | <3.0 | ≥.90 | ≥.90 | (≤.05 ≤.08) | ≥.90 | ≥.90 | ≥.90 | >.60 | |
| Hypothetical model | 241.65 | 130 | 2.56 | .84 | .85 | .06 | .88 | .84 | .87 | .62 |
| (<.001) | (.05 .07) | |||||||||
| Modified model | 240.31 | 131 | 1.78 | .86 | .90 | .05 | .88 | .92 | .87 | .70 |
| (<.001) | (.04 .06) |
GFI=goodness-of-fit index; AGFI=adjusted goodness-of-fit index; NFI=normed fit index; RMSEA=root mean square error of approximation;
TLI=Tuker-Lewis index; PNFI=parsimony normed fit index; CFI=comparative fit index; LO=low; HI=high.
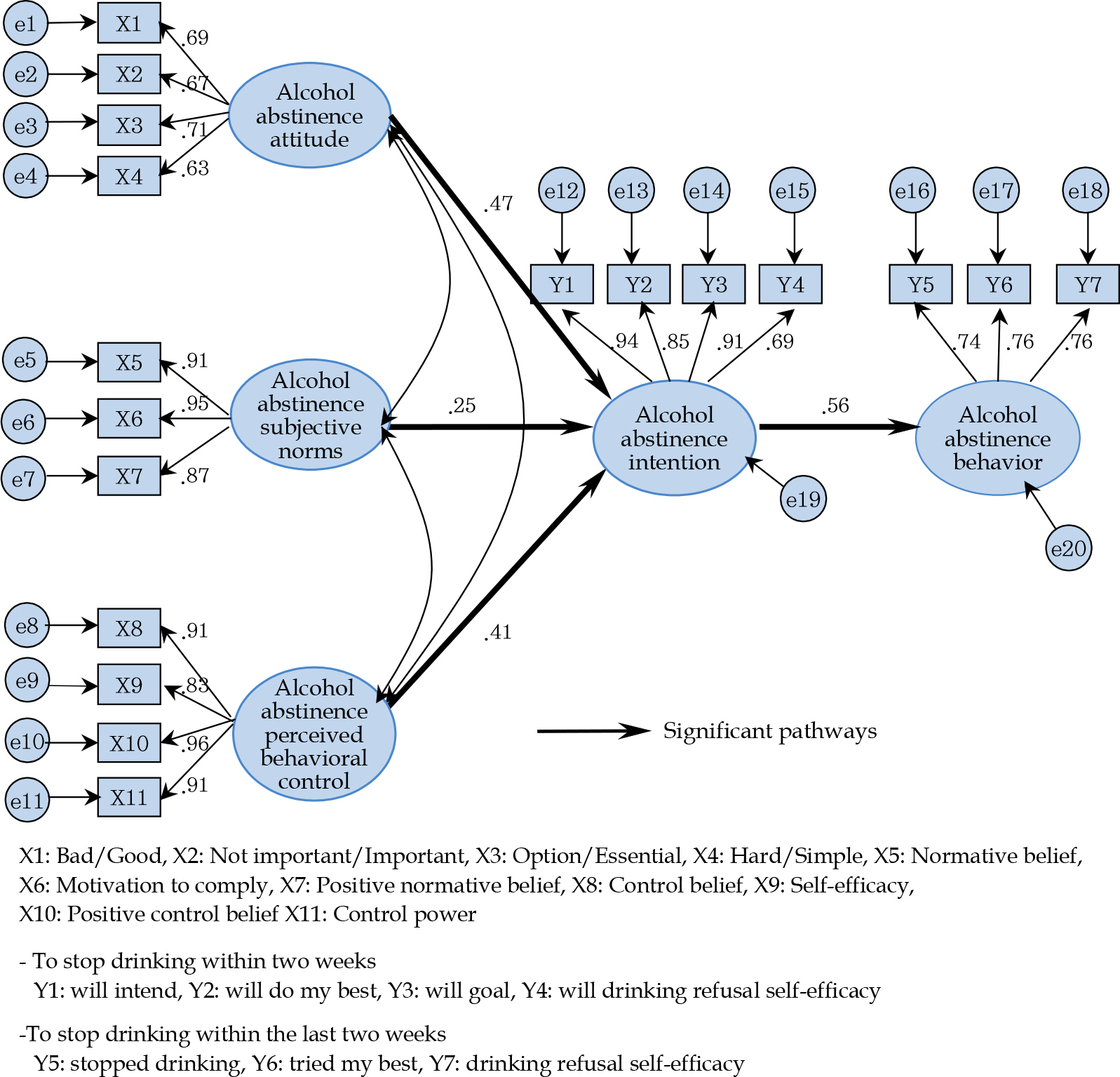
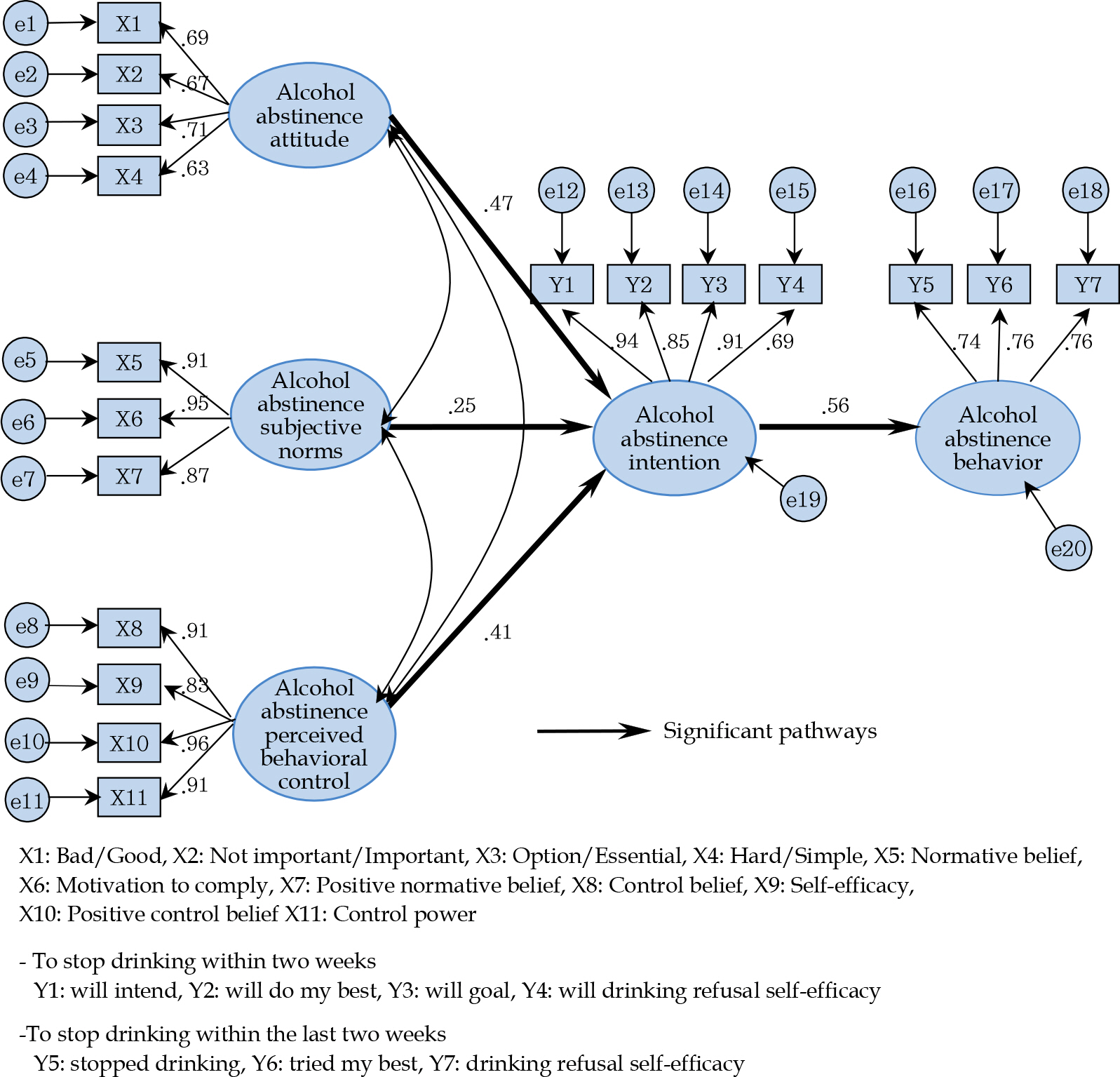
Direct, Indirect, and Total Effect Analysis of Modified Models (N=240)
| Endogenous variables | Exogenous variables | Direct effect | Indirect effect β | Total effect | SMC |
|---|---|---|---|---|---|
| β (p) | (p) | β (p) | |||
| Alcohol abstinence behavior | Alcohol abstinence intention | .56 (.021) | - | .56 (.021) | .32 |
| Alcohol abstinence behavior | Attitude | - | .27 (.016) | .27 (.016) | - |
| Subjective norms | - | .15 (.009) | .15 (.009) | ||
| Perceived behavioral control | - | .23 (.005) | .23 (.005) | ||
| Alcohol abstinence intention | Attitude | .47 (.015) | - | .47 (.015) | .46 |
| Subjective norms | .25 (.012) | - | .25 (.012) | ||
| Perceived behavioral control | .41 (.005) | - | .41 (.005) |
SMC=squared multiple correlation.
GFI=goodness-of-fit index; AGFI=adjusted goodness-of-fit index; NFI=normed fit index; RMSEA=root mean square error of approximation; TLI=Tuker-Lewis index; PNFI=parsimony normed fit index; CFI=comparative fit index; LO=low; HI=high.
SMC=squared multiple correlation.
 E-SUBMISSION
E-SUBMISSION