
Purpose
As the rate of older people visiting Emergency Departments (EDs) increases, nurses are responsible for identifying patients at risk of poor outcomes and providing preventive interventions. The aim of this study was to identify the factors associated with the mortality of older adults hospitalized through EDs.
Methods
The study design was a retrospective correlational design using the electronic medical records from a tertiary hospital in Korea. Data were collected from January 3 to March 6, 2016 through the hospital information center based on elderly patients admitted from January 1, 2011 to August 31, 2015. The study variables included general and admission characterstics, disease characteristics, and mortality of older patients visiting EDs.
Results
Of the 9,896 patients, the mortality rate was 7.4%; highest in patients aged over 86 years, men, or those hospitalized from nursing homes. Older adults arriving by private ambulance were 2.36 times more likely to die than walk-ins, and 1.38 times more likely for those using the 119 government emergency ambulance. Older patients hospitalized for more than four weeks were 2.17 times more likely to die than those hospitalized for less than a week.
Conclusion
Based on the study findings ward nurses will be able to early detect older patients at risk of poor outcomes and make better clinical decisions to improve the quality of nursing care. Nurses can propose health policies such as stricter management of the private ambulance service and considering the most efficient length of hospital stay for older adults hospitalized through EDs.
As the rate of older people visiting Emergency Departments (EDs) increases, nurses are responsible for identifying patients at risk of poor outcomes and providing preventive interventions. The aim of this study was to identify the factors associated with the mortality of older adults hospitalized through EDs.
The study design was a retrospective correlational design using the electronic medical records from a tertiary hospital in Korea. Data were collected from January 3 to March 6, 2016 through the hospital information center based on elderly patients admitted from January 1, 2011 to August 31, 2015. The study variables included general and admission characterstics, disease characteristics, and mortality of older patients visiting EDs.
Of the 9,896 patients, the mortality rate was 7.4%; highest in patients aged over 86 years, men, or those hospitalized from nursing homes. Older adults arriving by private ambulance were 2.36 times more likely to die than walk-ins, and 1.38 times more likely for those using the 119 government emergency ambulance. Older patients hospitalized for more than four weeks were 2.17 times more likely to die than those hospitalized for less than a week.
Based on the study findings ward nurses will be able to early detect older patients at risk of poor outcomes and make better clinical decisions to improve the quality of nursing care. Nurses can propose health policies such as stricter management of the private ambulance service and considering the most efficient length of hospital stay for older adults hospitalized through EDs.
The population aged 60 years or over numbered 962 million worldwide in 2017, more than twice as large as it was in 1980, and the number of older persons is expected to double again by 2050 [1]. The increasing rate of older population in Korea is the fastest in the world from 6.0% in 2005 to 14.9% in 2019, and expected to reach 39.8% in 2050 [1, 2]. As health issues such as chronic illness management, falls, and sudden crises have been on the rise in our aging society, the national long-term care insurance system was implemented in 2008 [3]. However, the visiting rate of older adults to Emergency Departments (EDs) has risen from 15.2% in 2005 [4] to 23.9% in 2016 [5]. In Australia, 22.0% of emergency medical center users were older adults [6] while the United States had an increase of 23.3% in 2016 [7].
Approximately 90.0% of older adults have at least one chronic disease, and 51.0% have more than three [8]. Moreover, the severity of disease process in older adults is relatively higher than that in the younger population, and their symptom characteristics are atypical, so it is not easy to identify which disease has caused the symptoms, resulting in more complicated tests being required [9, 10]. These matters result in longer stays in hospital for older patients, leading to physical and psychological hardship and poor outcomes [11]. In fact, the current in-hospital mortality rate of older patients admitted through EDs is high, ranging between 5.1% and 18.4% in Korea [12, 13] and 8.9% to 11.4% in other countries [14, 15]. In-hospital overall mortality in elderly patients also varies by disease from 3.0% to 11.6% [16, 17]. Although the mortality rate of hospitalized elders in Korea does not differ much from that of Western countries, the factors affecting mortality will be different because the lifestyle and the health care delivery system differ.
Therefore, it is necessary to investigate the characteristics of older patients who have been hospitalized through EDs and experienced worse outcomes. Among previous studies in Korea, most have focused on specific populations such as suicide attempts [18], homeless older adults [19], and older patients with trauma, [20] or clinical test results related to mortality in EDs [21] rather than their prognostic or disease characteristics. As elderly people are admitted to hospitals through EDs due to chronic illness management or sudden accidents, and show a high mortality rate and medical expenses compared to younger adult patients [20, 22], it is necessary to study the relationships between the characteristics of older patients and mortality to improve their health outcomes. Based on the literature review of previous studies on the mortality or characteristics of elderly patients in EDs, mortality-related variables were identified as 1) general characteristics of gender [14, 23], age [24], and health insurance [25]; 2) admission characteristics of admission process [25]; mode of arrival [9], level of consciousness [25, 26], and emergency severity [9, 14]; and 3) disease characteristics of main symptom [23, 25], main diagnosis [14], treatment department [26], admission unit [26], and length of hospital stay [14]. Because older adults tend to find it difficult to communicate their problems directly and consider the economic situation of their family more than they actively participate in their own clinical decision-making [27], ward nurses's α early identification of risk factors and appropriate responses may have a positive impact on the outcome of medical treatment.
Therefore, this study was conducted to investigate the relationships between the mortality of older patients hospitalized via EDs and their influencing characteristics, in order to make better clinical decisions and improve the quality of nursing services.
The aim of this study was to identify factors that are associated with the mortality of older adults who have been hospitalized via EDs, by their general, admission, and disease characteristics.
The study used a retrospective correlational design to investigate the factors associated with the mortality of older patients by analyzing their general, admission, and disease characteristics based on Electronic Medical Records (EMRs).
This study included the EMRs of 9,896 elderly patients who were hospitalized through the ED of a tertiary hospital in Korea from January 1, 2011 to August 31, 2015. Inclusion criteria were patients aged 65 years or older, patients hospitalized through the ED, and patients alive before hospitalization. Older adults who were repeatedly hospitalized were excluded to prevent the results from being affected by selection bias as most were cancer patients undergoing chemotherapy. The detailed number of patients of the accessible population was not provided by the hospital information center due to hospital management issues. The ED, which was the study site, has more than sixty beds and around 180 patients visit daily. The post hoc power of this study was 98.9% with a total of 9,896 in the sample size.
Admission characteristics included admission process, mode of arrival, level of consciousness, and emergency severity. The admission process was divided into admission from home, transfer from other hospitals or nursing homes, and admission through the outpatient department. The mode of arrival included walk-ins (own car), 119 government emergency ambulance, and private ambulance. The level of consciousness was classified into the following categories: alertness, lethargy, stupor, and unconsciousness based on the medical records.
The emergency severity was measured by the modified version of the Emergency Severity Index (mESI) accounting for the medical situation in Korea [28, 29]. The tool classifies the severity into five levels depending on the patient's symptoms, vital signs, and the number of emergency medical resources needed. The severity of mESI is classified as 1=urgent (if there is an imminent threat to life and immediate intubation or cardiopulmonary resuscitation is needed), 2=emergent (if resuscitation is not immediately required but there is urgent need of intervention to improve vitality), 3=moderate-emergent (if many additional medical resources are required), 4=non-emergent (if only one additional medical resource is required), and 5=stable (if there is no additional health care expenditure). The weighted kappa value of the mESI was 0.70 in the reliability evaluation between the physician and nurse groups [28].
Disease characteristics consisted of main symptom, main diagnosis, treatment department, admission unit, length of hospital stay, and medical outcome. The main symptom was measured by 14 items based on the Enforcement Regulation of Emergency Medical Service Act Article 2 no. 1 [30] and classified by legal criteria based on urgency of symptoms including eight acute symptoms: a. acute altered mental status, b. acute cardiopulmonary disorder, c. acute metabolic disorder and poisoning, d. surgical emergency condition or serious burns, e. acute hemorrhage, f. ophthalmological emergency symptom, g. allergy, and h. psychiatric emergency symptom; and six subacute symptoms: i. subacute mental change, j. subacute cardiopulmonary disorder, k. subacute surgical disorder and fracture, l. subacute hemorrhage, m. childbirth or genderual abuse, and n. choking.
The main diagnosis was measured by 17 items from the 7th Korean Standard Disease Sign Classification List [31], and the contents were as below: a. Infectious or parasitic disease, b. neoplasms, c. blood-forming or immune mechanism, d. endocrine, nutritional, and metabolic diseases, e. mental and behavioral disorders, f. neurological diseases, g. ophthalmological diseases, h. circulatory diseases, i. respiratory diseases, j. gastrointestinal diseases, k. skin diseases, l. musculoskeletal diseases, m. genitourinary diseases, n. congenital malformations, o. abnormal clinical and laboratory findings, p. injury or poisoning, and q. factors influencing health status.
The length of hospital stay was the number of days from the date of admission to ED to the day of discharge from hospital. The medical outcome was the results of the medical treatment which were divided into discharge and death based on the outcome records of the hospital discharge summary.
General characteristics included gender, age, and type of insurance. The types of insurance were national health insurance, medical aid, and private insurance.
First, we requested data which met the selection criteria from the hospital information center. The information center provided a data set collected from the EMRs of 9,896 older adults hospitalized through ED. The data set included the general and admission characteristics of the participants based on the nursing information records, and the disease characteristics and death and discharge information based on the initial medical record and discharge summary.
The study was approved by the Institutional Review Board (IRB) of the study hospital (IRB approval number SMC2015-08-083-001) before data collection. The study identification number was used for the participants's α medical records for anonymity. All data were managed by assigned research codes so that personal health information could not be identified. Each database group (general, admission, and disease characteristics databases, and death and discharge database) was stored separately so that the personal information could not be traced. The collected data were used only for research purposes.
Data were analyzed using SPSS for Windows version 22.0 (IBM Corp., Armonk, NY, USA). A Chi-squared test was used for the comparison of mortality and discharge rates according to general, admission, and disease characteristics of older adults hospitalized through ED. Factors associated with mortality of older patients were analyzed using logistic regression analysis. The model fit of the prediction model was assessed by performing a Hosmer-Lemeshow goodness-of-fit test. Effect size was measured using the Nagelkerke R2.
Of the 9,896 older adults hospitalized through ED, 731 (7.4%) died. The mortality rate was higher in men (χ2=19.62, p<.001) and in those aged 86 years or older (χ2=20.22, p<.001). Most patients (95.6%) had national health insurance (χ2=4.90, p=.086), and there was no difference in mortality according to the type of insurance (Table 1).
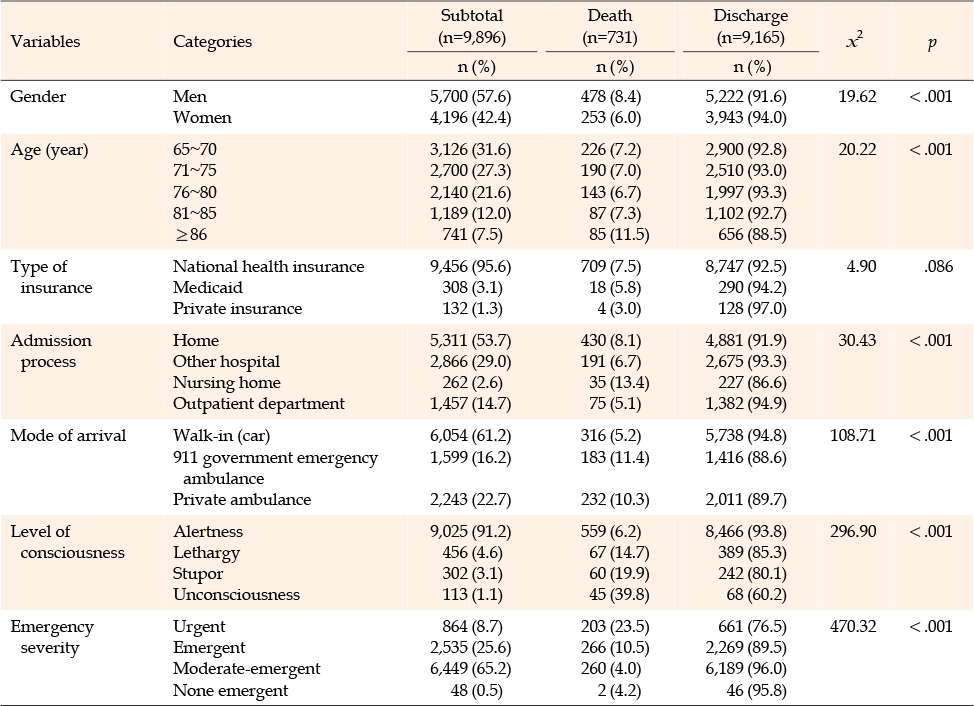
Table 1
Mortality and Discharge Rates by General and Admission Characteristics (N=9,896)
In the admission characteristics, the mortality rate was higher for those admitted from a nursing home (χ2=30.43, p<.001), using the emergency transportation systems (χ2=108.71, p<.001), unconscious state (χ2=296.90, p<.001), and urgent status (χ2=470.32, p<.001) at admission (Table 1). In the disease characteristics, subacute surgical disorder and fracture (27.4%) was the most frequent of the main symptoms, followed by acute cardiopulmonary disorder (25.1%) while neoplasm (27.9%) was the most frequent in main diagnoses, followed by circulatory disease (26.2%). The mortality rate was higher in patients with cardiopulmonary symptoms of the main symptoms (χ2=160.41, p<.001), neoplasm of the main diagnosis (χ2=234.76, p<.001), internal medicine of the treatment department (χ2=148.80, p<.001), intensive care unit of the admission unit (χ2=238.72, p<.001), and a hospital stay of more than two weeks (χ2=120.42, p<.001) (Figure 1).
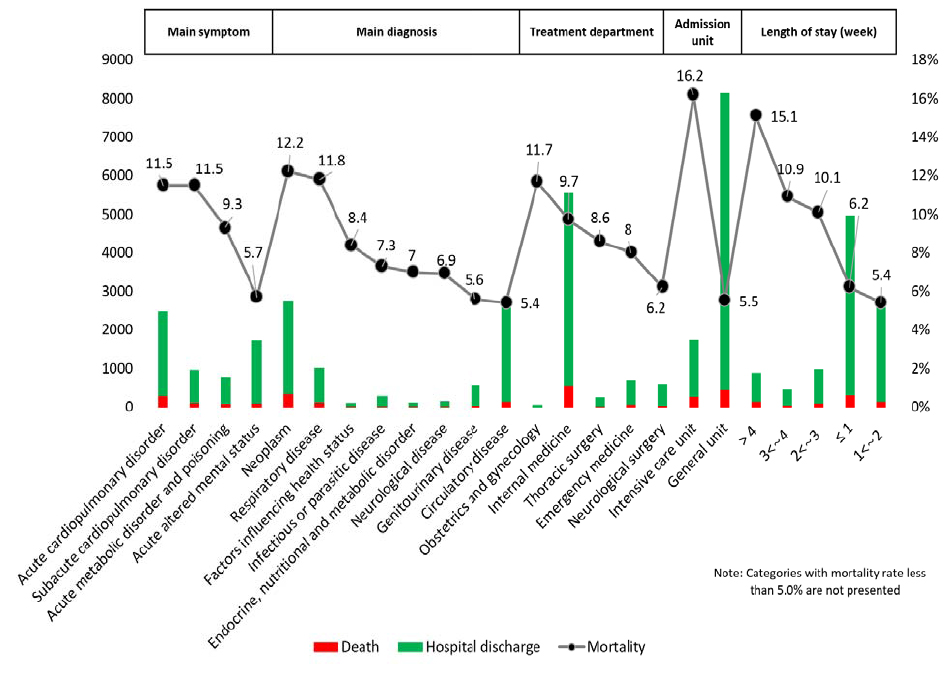
Figure 1
Mortality and hospital discharge rate by disease characteristics.
Variables that were found to cause significant differences or have a significant correlation with mortality of older patients were selected as independent variables in the logistic model. Logistic regression analysis was used to examine the factors associated with mortality of older patients. The Hosmer-Lemeshow test for general characteristic factors model, which included gender, age, and type of insurance, revealed a good fit (χ2=5.14, p=.162). The Nagelkerke2 effect size was .01. Of the general characteristics, the mortality of older patients was 0.68 times lower in women than men (B=−0.39, p<.001). Patients aged 86 years or older were 1.80 times more likely to die than those aged 65~70 years (B=0.59, p<.001)(Table 2).
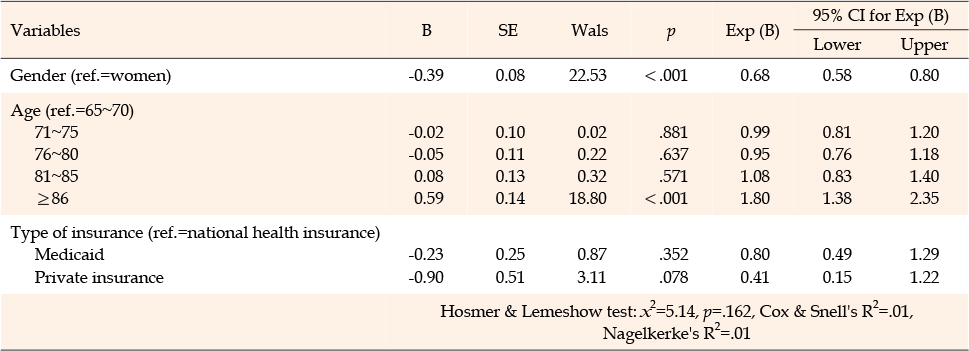
Table 2
General Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
In the admission characteristic factors model, which included admission process, mode of arrival, level of consciousness, and emergency severity, the Hosmer-Lemeshow test also revealed a good fit (χ2=4.31, p=.229), and the Nagelkerke2 effect size was .12. Among the admission characteristics, patients arriving from other hospitals were 0.57 times less likely to die than those from home (B=−0.57, p<.001). Patients who arrived by private ambulance were 2.36 times more likely to die than walk-ins (B=0.86, p<.001), while those who arrived via the 119 government emergency ambulance were 1.38 times more likely to die (B=0.32, p=.005). Patients in an unconscious state at admission were 2.92 times more likely to die than those who were alert (B=1.07, p<.001), while those in stupor were 1.52 times (B=0.42, p=.011) and those in lethargy were 1.41 times (B=0.34, p=.022) more likely to die. Patients in an emergent status at admission were 0.49 times less likely to die than those in urgent state (B=−0.73, p<.001), while those in the moderate-emergent category were 0.21 times less likely to die (B=−1.56, p<.001)(Table 3).
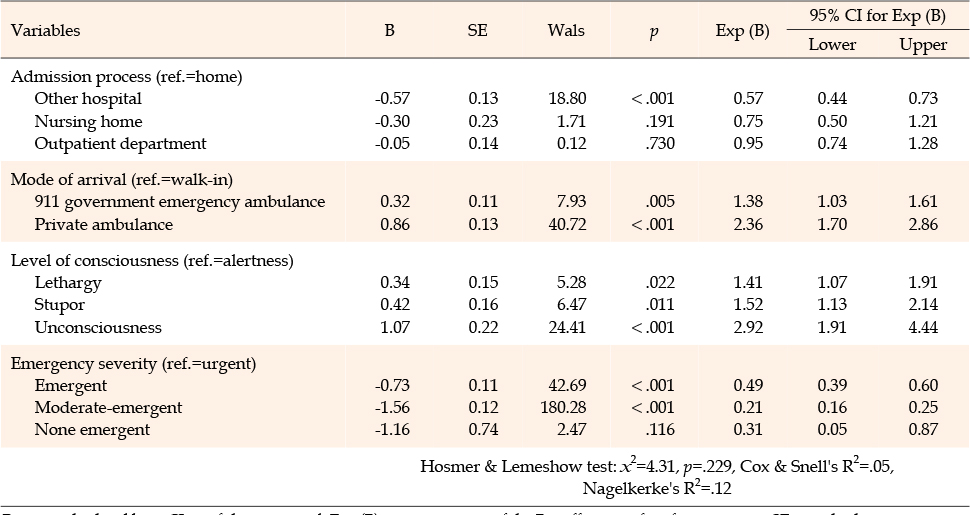
Table 3
Admission Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
In the disease characteristic factors model, which included main symptom, main diagnosis, treatment department, admission unit, and length of hospital stay, although the Hosmer-Lemeshow test did not reveal a good fit (χ2=26.10, p<.001), the sample size was sufficient [32] with 99.9% of post hoc power in this study. The Nagelkerke2 effect size was .16. Older patients with a main symptom of acute hemorrhage were 0.60 times lower likely to die than those with acute altered mental status (B=−0.51, p=.029). Patients with neoplasms as a main diagnosis were 2.34 times more likely to die than those with infectious diseases (B=0.85, p<.001), while those with gastrointestinal diseases were 0.48 times less likely to die (B=−0.74, p=.023). Older patients treated from the department of internal medicine were more likely to die than those from neurology, general surgery, or urology. Patients admitted to the intensive care unit were 3.26 times more likely to die (B= 1.18, p<.001); patients hospitalized for more than four weeks were 2.17 times more likely to die than those hospitalized for less than a week (B=0.77, p<.001), while those hospitalized for 3~4 weeks were 1.55 times higher (B=0.44, p=.010), and those for 2~3 weeks were 1.35 times higher (B=0.30, p=.018) (Table 4).
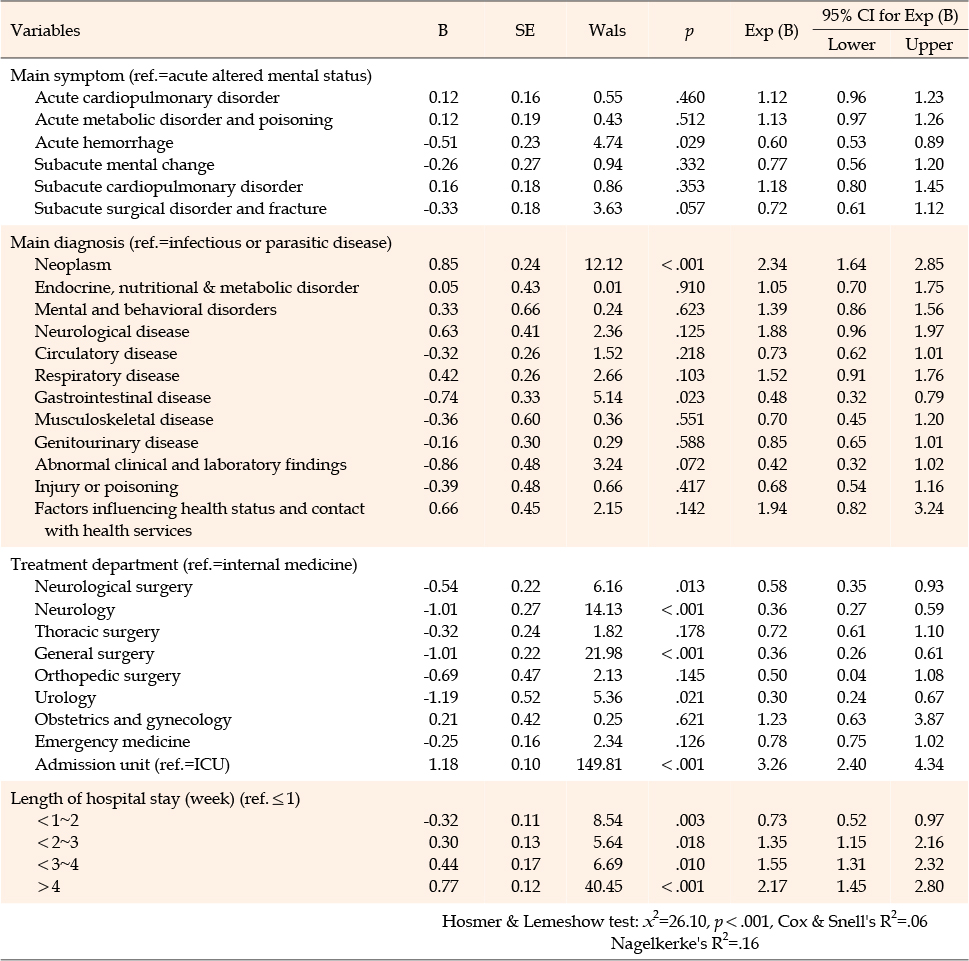
Table 4
Disease Characteristic Factors Associated with Mortality in Older Patients (N=9,896)
Identifying older adults at risk of poor outcomes as well as establishing preventive strategies for improving the quality of nursing care is important for those hospitalized through ED. The risk factors of their mortality identified in this study will help nurses predict changes in the condition of the elderly and plan preventive care.
In terms of the characteristics of the study participants, among the 9,896 older adults hospitalized through ED the most frequent main symptom was subacute surgical disorder and fracture (27.4%) followed by acute cardiopulmonary disorder (25.1%). In a previous study approximately 28.7% of older adults reported falling at least once, and 37.5% of those who fell reported being hospitalized at least once [33]. Therefore, our study findings suggest that programs to prevent falls resulting in fractures for older adults are very urgent.
The highest risk factors from the general and admission characteristics in this study were men, the oldest, private ambulance use, unconscious state at admission, and urgent status of severity on admission. In a previous retrospective study of older patients in ED, factors associated with mortality were highest for men, neoplasms, and ambulance utilization [34]. In this study, the mortality of older patients arriving by private ambulance was the highest among the identified factors. In Korea, the total number of 119 government emergency systems was 1,384 with 9,103 trained staff while private ambulance services were 892 with 1,161 trained staff in 2017 [35]. Moreover, in the study of the emergency response abilities of ambulance staff from private ambulance services, the scores were low at 66.09 of 100 points in emergency treatment, 63.75 points in consciousness confirmation, 69.33 points in airway management, 59.44 points in respiratory, and 64.00 points in circulation [36]. Based on current evidence, the emergency care training programs for private ambulance employees need to be stricter to improve their emergency response capabilities and, for the safety of patients, legal control over the transfer of patients or expansion of the 119 government emergency system should also be improved. It is also proposed that medical personnel accompany patients in private ambulances used for transfer to other hospitals.
The significant risk factors from the disease characteristics in this study were patients with acute altered mental status, and those with neoplasms, affiliated to internal medicine, transferred to intensive care unit, and hospitalized for more than four weeks. The average length of hospital stay across Organization for Economic Cooperation and Development (OECD) countries was around eight days, whereas Korea had the longest stays with over 16 days [37]. The reason for this may be that the national health insurance covered most medical costs. In this study 98.7% of older adults had national health insurance or Medicaid. In a study of older patients, increasing length of stay in Intensive Care Unit (ICU) is associated with higher mortality within a year for both mechanically ventilated and non-mechanically ventilated patients [38]. The evidence of the present study suggests that clinical decision-making for older patients needs to consider the evidence that a longer stay in hospital with aggressive medical treatment may not reduce their mortality rate. Therefore, it is recommended that the condition and quality of life of elderly patients is considered rather than continuing ICU treatment over a protracted period.
As nurses play an important role in patient assessment, it is necessary to accurately understand elderly patients and predict their prognosis in order to plan professional nursing services based on the study findings.
The study has several limitations. First, as there is a difference in the severity of patients by the size and level of the ED, the results of the study may apply more to tertiary hospitals. For future study, hospitals of various sizes and locations should be included. Second, the study used retrospective data from EMRs which could not measure prospective changes in patients' outcomes by nursing interventions that consider the risk factors of mortality. Therefore, we propose a prospective study of older patients hospitalized through ED for further studies. Nevertheless, this study contributed to the planning of strategies which will reduce the mortality rate of older adults by identifying the current problems in the emergency care system. Third, as discharge included cases transferring to other hospitals such as long-term care or rehabilitation hospitals, those may have been relieved in an emergency status, but still treated. Finally, the study data was relatively old based on the current emergency care system, although the contents of training and transportation systems outlined in the Emergency Medical Service Act have not been changed for more than ten years.
The study findings provide important prognostic information regarding the association between characteristics of older patients hospitalized through EDs and their mortality. Among the general and admission characteristics, the mortality rate was the highest in men, older adults aged over 86 years, and those who arrived via private ambulance service. Among the disease characteristics, the mortality rate was greatest in older patients with neoplasms, and those who had been hospitalized for more than four weeks. Nurses are at the forefront of identifying changes in patients's α health conditions. Based on the results of this study, ward nurses will be able to identify older patients at risk of poor outcomes and make better clinical decisions to improve the quality of nursing care. Nurses may use the study findings to develop tools to assess elderly patients admitted via ED and develop clinical protocols. In addition, the results of the study suggest stricter management of private emergency services, and future studies for the most efficient length of hospital stay for older patients hospitalized through EDs.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - LJA.
Data collection - LJE.
Analyzing the data - LJE and LJA.
Drafting and critical revision of the manuscript - LJE and LJA.
This article is a revision of the first author's master's thesis from Kyung Hee University.
 E-SUBMISSION
E-SUBMISSION