
Purpose
This meta-analysis was conducted to analyze the effect of Diabetes Mellitus (DM) on the risk of Parkinson Disease (PD).
Methods
Original prospective observational studies were searched through PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), ProQuest, Web of Science, Science Direct, Koreanstudies Information Service System (KISS), and DBpia published up to March 2020. The Relative Risks (RRs) were calculated using the random-effects model.
Results
An integrated analysis of ten large population-based cohort studies, involving 10,730,117 participants, showed that patients with DM had a 30% higher risk of PD than those without DM (pooled RR=1.30, 95% Confidence Interval [CI]=1.14~1.48). Subgroup analyses based on the characteristics of the studies were conducted, and the association between DM and PD was significant in studies conducted in Asia (RR=1.30, 95% CI=1.01~1.69) and Europe (RR=1.45, 95% CI=1.09~1.94), and for patients with DM durations less than ten years (RR=1.31, 95% CI=1.27~1.37) and stroke (RR=1.16, 95% CI=1.03~1.31). Each study included in the analysis had methodologically good quality and showed no evidence of publication bias.
Conclusion
DM resulted in a significantly increased risk of PD; therefore, prevention and early detection of PD in patients with DM should be encouraged.
This meta-analysis was conducted to analyze the effect of Diabetes Mellitus (DM) on the risk of Parkinson Disease (PD).
Original prospective observational studies were searched through PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), ProQuest, Web of Science, Science Direct, Koreanstudies Information Service System (KISS), and DBpia published up to March 2020. The Relative Risks (RRs) were calculated using the random-effects model.
An integrated analysis of ten large population-based cohort studies, involving 10,730,117 participants, showed that patients with DM had a 30% higher risk of PD than those without DM (pooled RR=1.30, 95% Confidence Interval [CI]=1.14~1.48). Subgroup analyses based on the characteristics of the studies were conducted, and the association between DM and PD was significant in studies conducted in Asia (RR=1.30, 95% CI=1.01~1.69) and Europe (RR=1.45, 95% CI=1.09~1.94), and for patients with DM durations less than ten years (RR=1.31, 95% CI=1.27~1.37) and stroke (RR=1.16, 95% CI=1.03~1.31). Each study included in the analysis had methodologically good quality and showed no evidence of publication bias.
DM resulted in a significantly increased risk of PD; therefore, prevention and early detection of PD in patients with DM should be encouraged.
Diabetes Mellitus (DM) is a chronic metabolic disease characterized by high serum glucose levels that lead to multi-organ disorders that affect the eyes, kidneys, nerves, heart, and blood vessels [1]. In particular, amylin, which is a hormone secreted from pancreatic beta-cells, forms a neurotoxic polymer in the brains of patients with DM and is associated with neurodegenerative diseases [2]. Parkinson Disease (PD) is a progressive and incurable neurodegenerative disorder caused by a deficiency in the active neurotransmitter dopamine. It shows the typical symptoms of tremors at rest, stiffness, a mildly bent forward posture, slower conscious movement, and a lack of facial expression known as the masked face, which affects approximately ten million individuals globally [3]. In Korea, the number of PD patients under 65 years old has more than doubled over the past ten years to 4,193 in 2019 [4]. However, the causes of PD are not yet clear; therefore, they are difficult to prevent. In addition, if DM is present when PD is diagnosed, the burden of the disease increases. Evidence from a literature review shows that the symptoms of PD are worse and develop faster in patients with DM [5].
Pagano et al. [6] found that DM is associated with Parkinson's-like pathology and affects the markers of Parkinson's pathology. In individuals with DM but without PD, dopamine transporter binding was significantly reduced in the corpora striata of their brains, which implies associations with PD [6]. Santiago and Potashkin [7] also asserted associations between DM and PD since the two neurodegenerative chronic diseases share "remarkably similar dysregulated pathways". Exposure to environmental risk factors is combined with inherited susceptibility, "mitochondrial dysfunction, endoplasmic reticulum stress, inflammation, and alterations in metabolism may lead to insulin resistance and, ultimately, DM and/or neurodegeneration [7]".
The link between PD and DM has been investigated in several meta-analyses. Cereda et al. [8] conducted a metaanalysis on the risk of PD associated with DM and reported discrepancies between cohort and case-control studies. While cohort studies showed a significant increase in the risk of developing PD in DM, case-control studies showed the opposite results, although they were not statistically significant. Lu et al. [9] also conducted a meta-analysis and reported that the probability of PD in DM patients in case-control studies was significantly reduced by 25%. However, Yue et al. [10] argued in their meta-analysis of cohort studies that the risk of PD in patients with DM was 38% higher than that in patients without DM. As such, the link between DM and PD has been continuously studied but without a clear conclusion. Cohort studies can provide a powerful basis for causality better than case-control studies can, because exposure to risk factors is identified before outcomes [11]. Therefore, in this study, we included only cohort studies to further clarify the temporal sequence between DM and PD. One prior meta-analysis [10] only analyzed cohort studies, but more than half of the included studies assessed exposure or outcome using self-reported data. All but one of the cohort studies included in the previous meta-analysis studies [8, 10] were conducted in the United States or Europe. However, three of the four cohort studies that were published after 2016 and added to the current analysis had been conducted in Asia. In addition, all four studies utilized objective data, such as medical records, when ascertaining exposures and outcomes. Thus, we attempted to estimate the robust pooled effect of DM on the risk of PD by only using cohort studies, geographically expanded samples, and objectively evaluated data. These may also provide better internal and external validities [12].
The purpose of this meta-analysis with large population-based cohort studies is to investigate whether DM at baseline is a risk factor for PD. In addition, this study updates the results of existing meta-analyses [8, 10] by including cohort studies published thereafter. This may help indirectly manage PD, an incurable neurodegenerative disease, by managing relatively well-known DM on the prevention and management of diseases in terms of disease prevention. The results of this study could benefit nurses in clinical and community settings during their daily practice with patients with DM. The results could inform nurse researchers and educators to develop better management strategies for DM patients to prevent and detect PD early.
This is a meta-analysis of cohort studies on DM and its association with PD as a risk factor in adults. Studies to be analyzed were searched and selected in the following three steps: setting up the literature search criteria, searching databases using keywords, and selecting studies followed by quality assessment using the Meta-analysis of Observational Studies in Epidemiology (MOOSE) reporting guidelines [13].
A literature search was performed to retrieve studies published, regardless of publication type, in English or Korean up until March 2020. The electronic databases queried were PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), ProQuest, Web of Science, and Science Direct for studies published in English; the Koreanstudies Information Service System (KISS) and DBpia were queried for studies published in Korean. The search was performed using the following Medical Subject Headings (MeSH): "Parkinson's disease OR Parkinson disease" AND "diabetes mellitus OR diabetes". We also scanned the reference lists of the included studies and relevant reviews retrieved from the search. The reference management software EndNote X9 (Clarivate, Philadelphia, PA) was applied to the retrieved studies to remove duplicates. Furthermore, titles and abstracts were screened independently by the researchers of this meta-analysis to identify potentially eligible studies, and later, full texts were reviewed to determine the final list of studies. The final lists of selected studies from all the researchers were compared, and no discrepancies were found.
The criteria for searching and selecting studies for this meta-analysis were based on the Participants, Interventions, Comparisons, Outcomes, Timing, Setting, and Study Design (PICOTS-SD) frame in Cochrane's guidelines [14]. The eligibility criteria for the study included in this analysis were as follows:
• Participants were adults who were diagnosed with either type 1 or type 2 DM but did not have PD at the beginning of the study.
• Interventions were not applicable to this analysis and, therefore, were ignored.
• The comparisons were conducted with adults without DM and PD at the beginning of the study.
• The outcomes were the occurrence of PD after a certain time period from the beginning of the study and had to be reported as a Relative Risk (RR) or a Hazard Ratio (HR) and 95% Confidence Interval (CI).
• The outcome was assessed at least one year after the beginning of the study.
• The outcome was compared between participating adults and adults without DM and PD and was represented by statistical measures such as RR or HR.
• Hospital (both outpatient clinics and wards) and community settings were included.
• The study design was a longitudinal prospective or retrospective design.
When a study met any of the criteria listed below, it was excluded from this analysis.
• It assessed the effects of several risk factors on PD after controlling for the effects of DM.
• It assessed effects of DM on pathophysiological or molecular biological aspects of PD.
• It assessed the effects of DM in patients who were already diagnosed PD.
• The study design was either a case -control study, systematic review, or meta-analysis.
The researchers independently extracted data regarding study characteristics such as the name of the first author, year of publication, country or origin of the population studied, study design, follow-up period, age of the population studied at baseline, diagnostic criteria for DM and PD, sample size, frequency of PD observed, risk of PD estimates (HR or RR) and corresponding 95% CIs, and adjusted variables. If a study provided several HRs or RRs, those after adjusting for the greatest number of confounding variables were included in the current analysis. When complete information was not available in the identified studies, the respective study investigators were contacted for additional information.
Comprehensive Meta-Analysis (CMA) Version 3 software (Biostat, Englewood, NJ, USA) was used for statistical analysis. The association between the two chronic diseases was estimated using the pooled adjusted RRs and corresponding 95% CIs after adjusting for as many confounders as possible. The extent of homogeneity across the primary studies was assessed using the Cochrane’s Q test (reported with χ2 and p values) and Higgins I2 value [15]. An I2 value of up to 25% indicated low heterogeneity, around 50% indicated moderate heterogeneity, and≥75% indicated high heterogeneity [15]. A meta-analysis was performed using the random effects model. The level of significance for all analyses in this study was determined using a two-tailed p value of <.05 with 95% CIs.
The methodological quality of the primary studies for this meta-analysis was assessed using the Newcastle-Ottawa Scale (NOS) version used for cohort studies [16]. The scale contained eight items categorized into three perspectives: selection of study groups (four items), comparability of groups (one item), and ascertainment of the outcome of interest (three items). For each item, zero or a maximum score of one was awarded depending on the level of quality. An exception to this rule was the comparability item; a maximum score of two could be awarded if a study controlled for participants’ age, gender, and other factors. A study score of three or four in the selection domain, one or two in the comparability domain, and two or three in the outcome domain indicates good quality in methodology. Each of the three researchers independently conducted the quality assessment of the studies included in the analysis, and the final assessment scores were reached after discussing a few discrepancy items.
Publication bias was assessed using a funnel plot, trim and fill analysis, and Egger’s regression test [17]. A sensitivity analysis was performed to assess the influence of each study on the overall results of the current meta-analysis. Finally, the quality of the current study was assessed using A MeaSurement Tool to Assess Systematic Reviews - version 2 (AMSTAR2), which was designed for nonrandomized or observational studies [18].
The literature search identified a total of 403 potentially eligible studies in English or Korean language from electronic databases (402 studies in English and one in Korean), and no additional studies were added after scanning reference lists from the identified studies. Of these, 311 duplicates were removed first, and 23 studies were removed after reviewing the titles and abstracts. The researchers thoroughly reviewed the full texts of the remaining 69 studies for eligibility and finally selected ten studies [19, 20, 21, 22, 23, 24, 25, 26, 27, 28] for this meta-analysis. The reasons for excluding the 59 studies were inappropriate study designs (n=27), such as intervention studies, case-control studies, systematic reviews, and meta-analyses. Wrong study purposes (n=32) included factors such as assessing the effect of DM in patients with PD, assessing the effects of several risk factors after controlling for the effect of DM, or assessing the effects of DM on pathological and molecular biological aspects of PD (Figure 1).
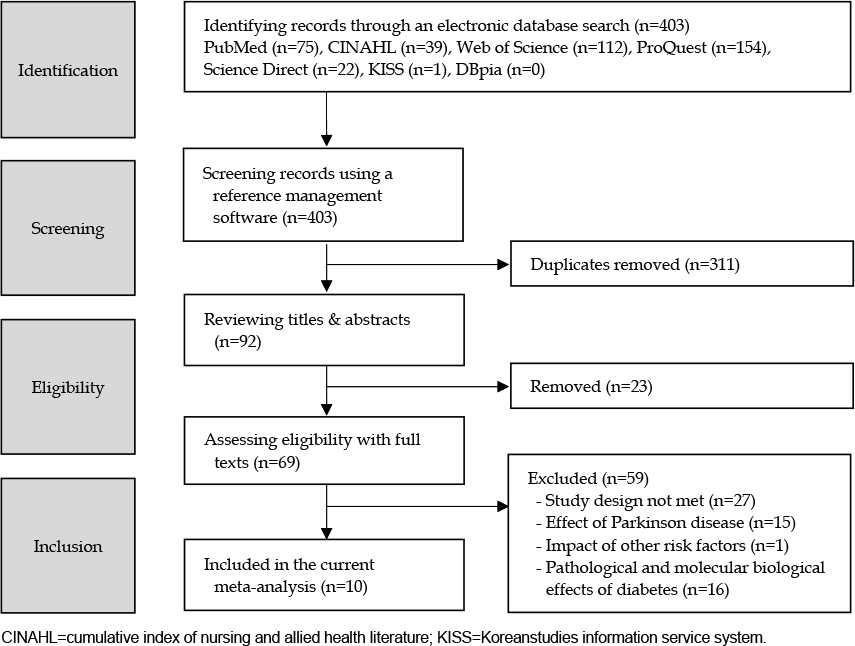
Figure 1
Flow diagram of study selection.
Only an abstract was published for the study by Kim [22]. Therefore, the author was contacted, and the original data presented in the abstract was acquired. Similarly, the study by De Pablo-Fernandez et al. in 2014 [29] was also published as an abstract only and included in a previous meta-analysis [10]. However, our efforts to obtain the original report of the abstract from the authors were not successful. Instead, a recent publication [19] by the same author, including the data presented in the abstract [29], was included in the current study. Several discrepancies were found between the two previous meta-analyses [8, 10] and the current study. These discrepancies were related to follow-up periods [27], frequencies of PD occurrence [20], number of participants [25], and risk ratio for PD [24, 27].
Methodological qualities of the ten selected cohort studies [19, 20, 21, 22, 23, 24, 25, 26, 27, 28] were assessed using NOS [16], and the studies scored more than three in the selection domain, two in the comparability domain, and more than two in the outcome domain, which indicates good quality. All ten studies were large population-based cohort studies and published in English between 2007 and 2018. A total of four of the ten studies were conducted in the USA, four in Asia (one in Korea and three in Taiwan), and two in Europe (England and Finland). Among the ten studies, six were conducted prospectively, and four were conducted retrospectively. There were wide-ranging follow-up durations, and only the three Taiwan-based studies by Lee et al. [23], Sun et al.[26], and Yang et al. [28] identified PD within less than ten years from the beginning of the study (five, nine, and seven years, respectively). In the remaining seven studies, the monitoring period was more than ten years, ranging from 11 years [22, 27] to 23 years [20]. All the primary studies identified PD in the participants following the criteria of the International Classification of Diseases, except for one study by Driver et al. [20] that only used self-reports by participants (Table 1). A total of 10,730,117 adults participated in the analysis. Among these participants, 2,730,624 had DM and 7,852,397 did not have DM, and the DM status of the remaining 147,096 participants was not reported in the article [24]. The HRs and RRs of each primary study are presented in Table 1. The chosen risk of PD in each study was the one that was adjusted for as many confounding factors as possible.
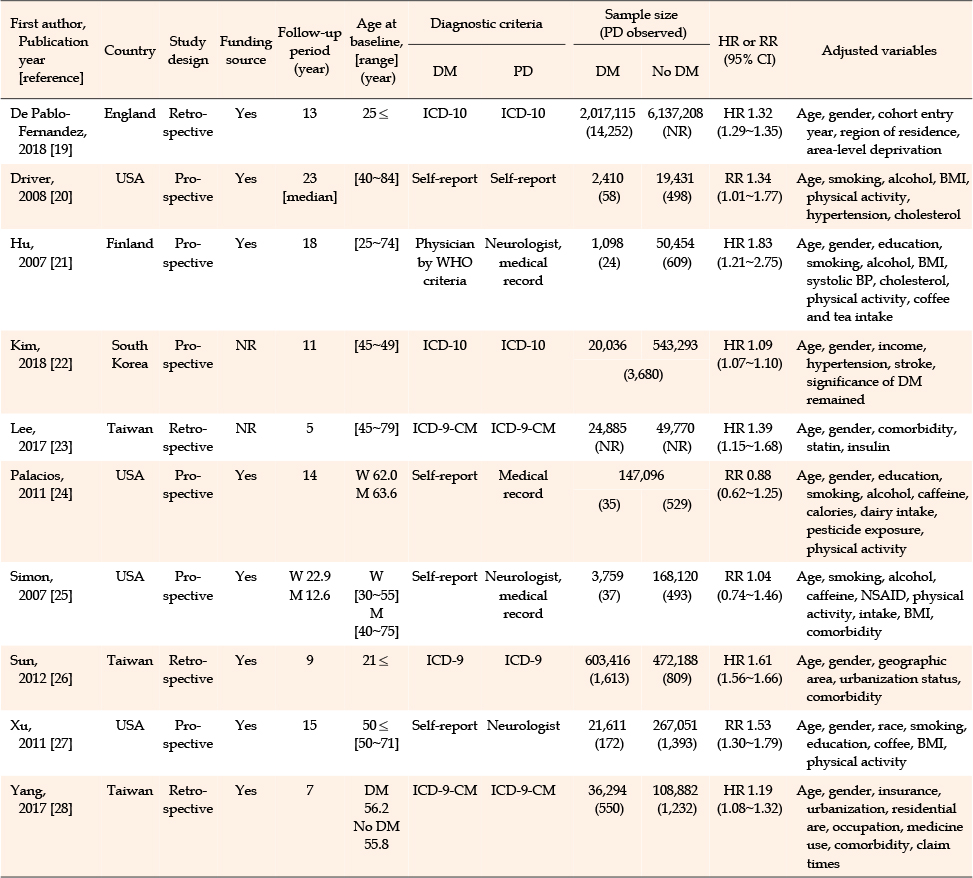
Table 1
Characteristics and Outcomes of the Primary Studies
The association between DM and PD was estimated using pooled adjusted RRs and their corresponding 95% CIs. The results showed that the risk of PD in participants with DM was significantly higher (by 30%) than that in participants without DM (RR=1.30, 95% CI=1.14~1.48, p<.001) (Figure 2).
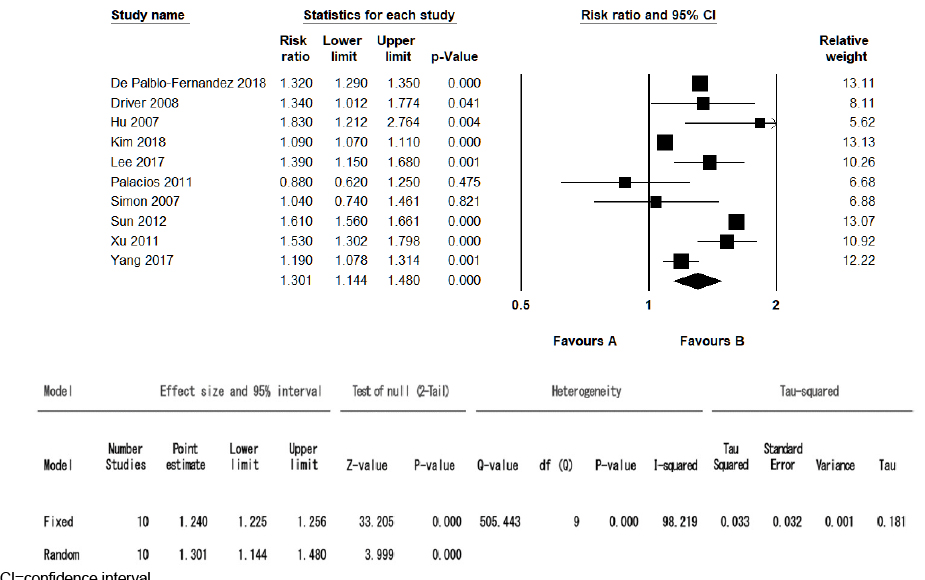
Figure 2
Forest plot and heterogeneity tests.
Homogeneity across the ten primary studies was assessed using the Q test and I2 value. The results showed that the effect sizes of the ten studies were heterogeneous (Q=505.44, df=9, p<.001, I2=98.2%). However, the forest plot showed RRs in a similar direction, and only two studies [24, 25] contained a lower limit of 95% CI below one (Figure 2).
Since the Q test and I2 value showed high heterogeneity across the ten primary studies, subgroup analyses were performed to explore possible sources of heterogeneity based on the study characteristics such as country, gender, duration of DM, and comorbidities (Table 2).
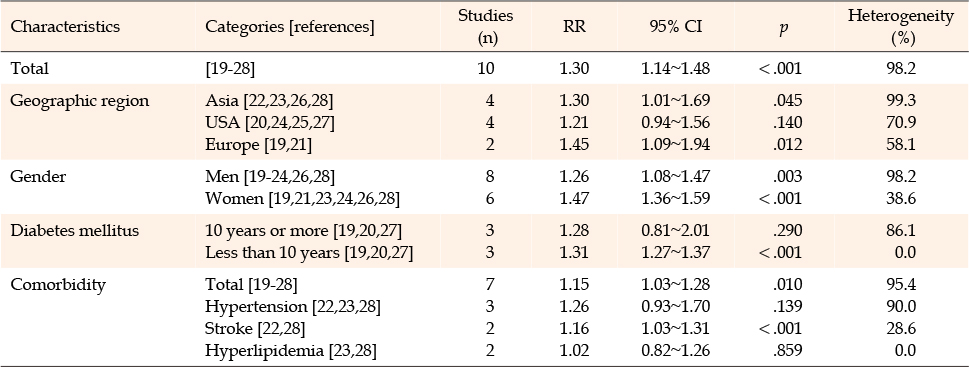
Table 2
Overall and Subgroup Analysis
When the studies were grouped into three based on geographical regions, the pooled adjusted RR from studies conducted in Asia (RR=1.30, 95% CI=1.01~1.69, p=.045) and Europe (RR=1.45, 95% CI=1.09~1.94, p=.012) showed that DM was a statistically significant risk factor for PD, but the RR from four studies conducted in the USA did not (RR=1.21, 95% CI=0.94~1.56, p=.140). The subgroup analysis based on participants’ gender showed that DM was a statistically significant risk factor for PD in men (RR=1.26, 95% CI=1.08~1.47, p=.003) and women (RR=1.47, 95% CI=1.36~1.59, p<.001). Furthermore, the subgroup analysis based on the duration of DM revealed that having DM for less than ten years was a statistically significant risk factor for PD (RR=1.31, 95% CI=1.27~1.37, p<.001) but having DM for over ten years was not (RR=1.28, 95% CI=0.81~2.01, p=.290). Lastly, in the subgroup analysis based on comorbidities such as hypertension, hyperlipidemia, and/or stroke, DM was a statistically significant risk factor for PD (RR=1.15, 95% CI=1.03~1.28, p=.010). However, in a separate analysis for each comorbid condition, only stroke was a significant risk factor (RR=1.16, 95% CI=1.03~1.31, p<.001). In summary, countries in Asia or Europe, having DM for less than ten years and comorbidities, such as stroke, showed significant effect sizes.
Publication bias was assessed using a funnel plot, trim and fill analysis, and Egger's regression test. The funnel plot showed that effect sizes were placed almost symmetrically around the top of the funnel. The trim and fill analysis resulted in a maintained estimated effect size without inserting additional papers, which indicates that publication bias is less likely. Egger’s regression test result was not significant (p=.622), which also indicates no publication bias.
To verify the consistency of the results of this study, a sensitivity analysis was performed to identify changes in effect size after each individual study was removed. The mean effect size from the ten studies was 1.30 (95% CI = 1.14~1.48), and the effect sizes from nine studies, excluding one at a time, ranged between 1.26 and 1.35, which were not far from the overall mean effect size of the ten studies. The 95% CIs from the nine studies were also similar to the overall 95% CI from the ten studies (Figure 3). The rating of overall confidence was found to be high when the current study was critically appraised using AMSTAR 2.
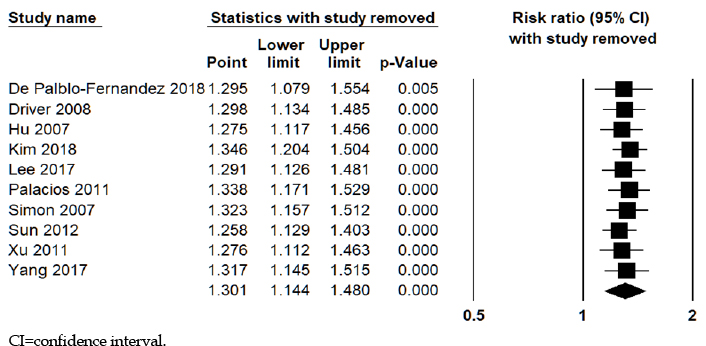
Figure 3
Sensitivity analysis.
This meta-analysis was performed to analyze the effect of DM on the risk of PD in ten large cohort studies. The overall effect size of the ten cohort studies was estimated to be 1.30. In other words, DM increased the risk of developing PD by 30%. The overall effect size was similar to those reported in the two previous meta-analyses: 1.37 (95% CI=1.21~1.55) in a study by Cereda et al. [8] with four cohort studies and 1.38 (95% CI=1.18~1.62) in a study by Yue and colleagues [10] with seven cohort studies. The results of our study supported the concluding remarks of the two previous studies [8, 10], which indicated that DM was a risk factor for PD development. In addition, Santiago and Potashkin [30] showed that the two diseases are highly interconnected at the molecular level by a network biological analysis. Previous studies have suggested that insulin resistance causes neurodegeneration [7]. This implies that DM and PD are biologically and functionally related, supporting the findings of previous and current studies. However, inconsistent results have been reported in these studies. As also noted in the Santiago and Potashkin study [30], this is thought to have resulted from sometimes self-reported DM diagnoses and the impact of reactions among drugs to treat DM and PD.
All ten primary studies analyzed the data from credible sources. Among the ten studies, six used national databases: English National Hospital Episode statistics and mortality data in England [19], the Nationwide Social Insurance Institution's drug register database in Finland [21], and National Health Insurance databases in Korea and Taiwan [22, 23, 26, 28]. The remaining studies used data from the American Association of Retired Persons database with over 40 million members in the USA [27], a nutrition cohort with over 140,000 adults followed for 14 years in the USA [24], a cohort of over 20,000 male physicians followed for more than 23 years in the USA [20], and data from the Nurse's Health Study (121,046 women) and the Health Professional Follow-up study (50,833 men) [25]. These data sources had large sample sizes and considerably long monitoring periods, which were highly likely to confer representativeness to the data and validity of the results [31].
The levels of heterogeneity in the current and two previous meta-analyses were inconsistent. Although the heterogeneity was low (I2=34.3%) in the first meta-analysis [8] and relatively high (I2=71.2%) in the second meta-analysis [10], it was considerably high (I2=98.2%) in the current study. One reason for this inconsistency is the large number of primary studies and their sample sizes [15]. Only four and seven cohort studies were included in the first and second meta-analyses, respectively [8, 10]. However, ten were included in our study. The sample size was over eight million in the study by De Pablo-Fernandez et al. [19] and over one million in Sun et al.'s study [26]. Another source of heterogeneity is the differences between the sample characteristics and study design of the primary studies [32]. Including studies conducted in Asia may have contributed to the high heterogeneity. One Korean study [22] and three Taiwanese studies [23, 26, 28] were added to the first meta-analysis. The data sources of all four studies conducted in the USA were self-reports of participants, while the data sources were government-controlled national databases in the remaining studies. Self-reporting might have led to diagnostic and reporting errors, particularly underreporting. As such, subgroups based on geographical regions of studies were found to be significantly heterogeneous. In summary, the high heterogeneity in this study was understandable from a design-related practical standpoint. In addition, from a statistical standpoint, high heterogeneity did not mean that the pooled effect was not significant from a statistical standpoint, since the 95% CI of the pooled RR did not stretch below one and all the studies turned out to be good [33]. We are confident that the positive effect we found was robust.
Several subgroup analyses revealed interesting results. First, the subgroup analysis based on geographical regions revealed the source of heterogeneity in the current study. In the four studies conducted in the USA, the RR was not significant, while the RRs from studies conducted in Asia and Europe showed an association between DM and PD. Among the four studies from the USA, two showed association [20, 27], while the others did not [24, 25]. Data extracted from three [20, 25, 27] out of four studies [20, 24, 25, 27] in the USA were reported incorrectly in the meta-analysis by Cereda et al. [8]. Yue et al. [10] also reported incorrectly extracted data [24, 27]. Second, the results of the subgroup analysis according to sex were similar to those reported in the study by Yue et al. [10]. RRs for men and women were significant, and the RR for women was slightly higher than that for men. Third, a DM duration of less than ten years was found to be a risk factor for PD in the current study and the study by Yue et al. [10]. The reason for a DM duration of less than ten years, rather than one greater than ten years, is a significant risk factor for PD is unclear. The reason for this might be ascertainment bias, as many of the authors of the primary studies indicated. Patients with DM are more prone to other diseases and are, therefore, likely to be in contact with their healthcare providers more often than patients without DM. Hence, increased surveillance might have led to the detection of PD more often in this group. However, the long-term effect of increased surveillance might have decreased because DM and PD are age-related chronic diseases, and diabetes-associated comorbidities exacerbate PD symptoms. Additionally, this may have resulted from the longterm use of anti-diabetic drugs, such as metformin, eliciting neuroprotection [30]. Further prospective investigations are required to clarify the etiological role of DM. Fourth, a subgroup analysis based on comorbid status was performed only in the current study. When patients with DM had comorbid hypertension, stroke, and hyperlipidemia combined, the risk of PD was higher. However, when each comorbid status was considered separately, only stroke was a risk factor for PD. Perhaps this finding, in which stroke acted as a risk factor for PD, resulted from a similar path on which the two are based. If ischemic stroke-induced cerebrovascular changes affect subcortical white matter, basal ganglia, thalamus, and upper brain stem related to PD, it could result in vascular parkinsonism [34]. In summary, the risk of PD in patients with DM was similar in men and women and significantly higher in patients with DM for less than ten years and those with stroke. However, the results need to be interpreted with caution because the number of studies in each subgroup analysis was small, ranging only from two to seven. In addition, the number of cohort studies included in the analysis to estimate the pooled effect was small. The possibility of bias in the publication bias test was less likely, but it could not be ruled out completely. Details of individual patients, such as history of using anti-diabetic drugs and DM severity, were not identified. Therefore, this was not considered in estimating the pooled effect on causality between DM and PD. Subsequently, a systematic literature review is required to cover all related papers for a broad understanding of the effect of DM on the risk of PD. Moreover, an additional meta-analysis is needed considering the details affecting causality between DM and PD to increase clinical applicability in patients. However, the current study has complemented power compared to previous meta-analyses with the advantage of larger populations, longer follow-ups, and a larger number of primary studies. These findings can serve as a basis for nursing practice. Based on these findings, it is necessary to educate patients and their families about the association between DM and PD, especially for patients with DM durations of less than ten years and those who have suffered from strokes, and to develop and apply nursing intervention programs to reduce PD incidence risk. In addition, it is necessary to identify PD outbreaks as early as possible to prevent the worsening of symptoms. Based on the results of this study, the education and application of interventions for DM patients could increase disease insights and self-care activities. This consequently reduces the risk of PD outbreaks, suggesting that DM patients continue to live independently.
In conclusion, although the mechanism of the association between DM and PD has not yet been clearly demonstrated, the association was found globally in ten population-based cohort studies and consistently confirmed with three meta-analyses, including the current one. In addition, further studies should focus on causality or mechanisms that underlie DM and PD to elucidate the clarity of the association.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - YS, YY and KJH.
Data collection - YS and YY.
Analysis and interpretation of the data - YS, YY and KJH.
Drafting and critical revision of the manuscript - YS, YY and KJH.
 E-SUBMISSION
E-SUBMISSION