
Purpose
This descriptive phenomenological study explored the lived experiences of patients recovering from Coronavirus Disease-2019 (COVID-19).
Methods
Using a purposive sampling method, participants were recruited from the Korean Psychological Association’s Mental Health and Wellness Center in G city, South Korea, from May 5 to December 30, 2020. The interviews were analyzed using Colaizzi’s seven-step method. Data saturation was reached after interviewing 14 participants.
Results
The experiences of patients recovering from COVID-19 were clustered into 4 main themes and 10 subthemes:, namely, the patients’ 1) stigmatization, leading to anxiety, fatigue, and concern about neighbors; 2) negative emotions: anger and helplessness; 3) coping strategies under pressure: increased gratitude, self-reflection, and self-efficacy; and 4) ways of overcoming internalized stigma: personal growth and hope for the future.
Discussion
The results suggest that the positive and negative emotions of patients recovering from COVID-19 are interwoven and coexist against the background of the pandemic. Improvement of social networks, development of coping skills, and psychological growth play an important role in alleviating the psychological burden of recovering patients.
This descriptive phenomenological study explored the lived experiences of patients recovering from Coronavirus Disease-2019 (COVID-19).
Using a purposive sampling method, participants were recruited from the Korean Psychological Association’s Mental Health and Wellness Center in G city, South Korea, from May 5 to December 30, 2020. The interviews were analyzed using Colaizzi’s seven-step method. Data saturation was reached after interviewing 14 participants.
The experiences of patients recovering from COVID-19 were clustered into 4 main themes and 10 subthemes:, namely, the patients’ 1) stigmatization, leading to anxiety, fatigue, and concern about neighbors; 2) negative emotions: anger and helplessness; 3) coping strategies under pressure: increased gratitude, self-reflection, and self-efficacy; and 4) ways of overcoming internalized stigma: personal growth and hope for the future.
The results suggest that the positive and negative emotions of patients recovering from COVID-19 are interwoven and coexist against the background of the pandemic. Improvement of social networks, development of coping skills, and psychological growth play an important role in alleviating the psychological burden of recovering patients.
On June 22, 2021 the World Health Organization (WHO) reported weekly (June 14~20, 2021) global numbers of just over 2.5 million new cases and over 64,000 deaths from Coronavirus Disease-2019 (COVID-19) [1]. The COVID-19 is caused by a new virus strain, Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), first identified in Wuhan’s atypical pneumonia group in December 2019 [2]. Many patients recovering from COVID-19 experience neurobiological changes and psychological and social difficulties [3]. Systematic reviews and meta-analysis results showed the prevalence of stress (29.6%), anxiety (31.9%), depression (33.7%), and insomnia (33.7%) among the general Asian and European populations [4].
Many recovering and recovered COVID-19 patients experience psychological and social problems [5]. Confinement and loss of usual routines, such as shopping and reduced social and physical contact with others, were frequently shown to cause boredom and a sense of loneliness [6, 7]. Scholars have noted that the pandemic will lead to unprecedented mental health problems, as recovering COVID-19 patients may be under greater psychological pressure than the general population, owing to disease-related uncertainties and potential future financial burdens [8, 9]. Scholars have pointed out the need for exploratory treatment that focuses on improving individuals’ understanding of the source of problems, for them to live a more rewarding life [10]. A previous study also reported that healthcare providers provide appropriate psychological treatment to patients in both the current and post-pandemic periods [11].
Patients who have recovered from COVID-19 and have returned to their communities may experience life dissatisfaction and psychological discrimination [12]. Patients infected with COVID-19 experience lifestyle changes, delayed social readjustment, and alienation from colleagues during treatment [13, 14]. Although researchers have demonstrated that COVID-19-infected patients experience psychological exhaustion, COVID-19 is a novel disease and to date, researchers have conducted limited phenomenological studies and follow-up treatments to understand the lived experiences of recovering patients, having published few qualitative studies on the psychological experiences of patients with COVID-19 [15, 16]. Therefore, further research on the psychological experiences of recovering and recovered COVID-19 patients is needed. Phenomenological approaches to qualitative research can help patients experiencing psychologically traumatic COVID-19-related events obtain a vivid awareness of the recovery process [17].
Through semi-structured interviews, we explored the lived experiences of COVID-19 patients during their recovery process to provide a basis for understanding the psychological experiences of recovering COVID-19 patients.
We employed Husserl’s descriptive phenomenological method to explore the lived experiences of patients recovering from COVID-19. Husserl’s phenomenological process is inherently inductive, emphasizing on the depth of an individual’s lived reality and the discovery of their unique experiences [18].
Data were collected through face-to-face, semi-structured, in-depth interviews until theoretical saturation was reached. Participants were recruited from May 5 to December 30, 2020. This study was conducted at scheduled times in a separate, restricted room affiliated to the G Center and the Korean Psychological Association. The interviews were conducted by a researcher who previously worked as a nurse in a COVID-19 isolation ward in D city. The said researcher has obtained a Level 2 clinical psychologist certificate issued by the Korean Ministry of Health and Welfare. During the interview, empathy and interviewing skills were used to prompt participants to give a complete account of their lived experiences with COVID-19. We determined the interview outline by seeking experts’ opinions and recruiting three recovered patients for the pre-interview. The semi-structured interviews were based on the SAFER-R model which consists of Stabilization, Acknowledgment, Facilitate understanding, Encouragement, Recovery, and Referral (SAFER-R) [19], modified by a psychiatrist. Face-to-face or telephone consultations were conducted. Based on a prior phenomenological study [20], face-to-face counseling was conducted for up to three sessions, ranging from 40 to 70 minutes per person. Data saturation is taken as a signal to stop participant recruitment and end the research [21]. Similar to a previous study [22], the potential risks of quarantine experiences were weighed carefully against the possible psychological distress faced by quarantined patients. Patients confessed that they still recalled being quarantined and were significantly more inclined to have trauma-related mental health disorders. This led to the cooperation of interdisciplinary mental health professionals to provide better mental health support prior to a face-to-face interview conducted by one of the authors. We went through the following process to collect information, select participants, and obtain written consent. First, we identified the personal information of confirmed COVID-19 patients from the mental healthcare center in G city. Next, we sent psychological support guidance materials with informed consent forms and obtained written consent from the participants.
The semi-structured interviews began with open-ended questions, followed by probing questions to elicit more information from the participants. All interviews were recorded using audio recorders with the participants’ consent. The interviewer summarized the interview content and asked the participants to confirm them. The interviewer wrote debriefing notes for each interview. The participants were interviewed until data saturation was reached, which was the point when the data no longer yielded new information, codes, or themes. The authors completed data collection in the 14th interview, after which the content of the interviews yielded repetitive information.
This study was reviewed and approved by the Ethics Committee of K University (IRB No. KNU-2020-0045). The researcher explained the purpose of the study, methods, and related rights to the participants, confirmed their willingness to participate, and obtained their signatures on an informed consent form. All collected data were kept confidential and anonymous. A mental health disaster evaluation was conducted to assess the mental state of participants, and all participants were advised that they were free to stop participating at any time without any disadvantages.
The recordings were transcribed and analyzed following Colaizzi’s [17] phenomenological seven-step method, whereby interviewers: 1) listened to the interviews about the lived experiences of recovered COVID-19 patients and reviewed the interview transcripts; 2) objectively extracted significant statements; 3) formulated meanings from the significant statements; 4) organized the commonalities of the meanings to form theme clusters; 5) integrated the themes into a description; and 6) summarized the fundamental structure. Using a purposeful sampling method, 14 research participants were recruited, and no participants deviated during the experiment.
To improve transferability, credibility, dependability, and confirmability, and maintain rigor in the study, we followed Lincoln and Guba’s four criteria [21]. To confirm transferability (i.e., applicability of the findings in different settings), research participants were asked to read the study results to verify their applicability to their own experiences. We repeatedly listened to the recorded interviews and transcribed them according to the participants' statements. We read and checked for accuracy several times by comparing recorded interviews with transcripts and confirming the precision of transcripts by research participants. The present study also used the member-checking technique, following Lincoln and Guba [21], to ensure credibility. First, interdisciplinary researchers reviewed the interview transcripts and provided ideas to rephrase, interpret, and confirm participants' experiences. Second, interdisciplinary researchers discussed the findings to analyze themes and expressions that influenced the findings. Third, for a final check, the members shared supplementary feedback on the analysis (credibility). To ensure field data dependability, we composed an audit trail with one psychiatrist, two phenomenological research professors, one clinical psychologist, and one counseling psychologist, and then analyzed recorded decisions, working out, and inquiries (dependability). To uphold confirm-ability, a neutral attitude was maintained by avoiding involvement in interactions with the participants and excluding prejudices (confirmability).
In total, data obtained from 14 participants were used for the analysis (seven women and seven men respondents). Most participants were aged between 25 and 40 years, well-educated, and married. The quarantine period ranged from two to five months, with an average quarantine period of three months. Five respondents reported that they had exhibited symptoms of COVID-19, and twelve respondents reported that they had exhibited symptoms of Post-Traumatic Stress Disorder (PTSD) after COVID-19 infection. Twelve respondents practiced religion, and two did not (Table 1). We explored the psychological experience of COVID-19 recovery using phenomenological methods, and the results are represented by 4 themes and 10 subthemes (Table 2).
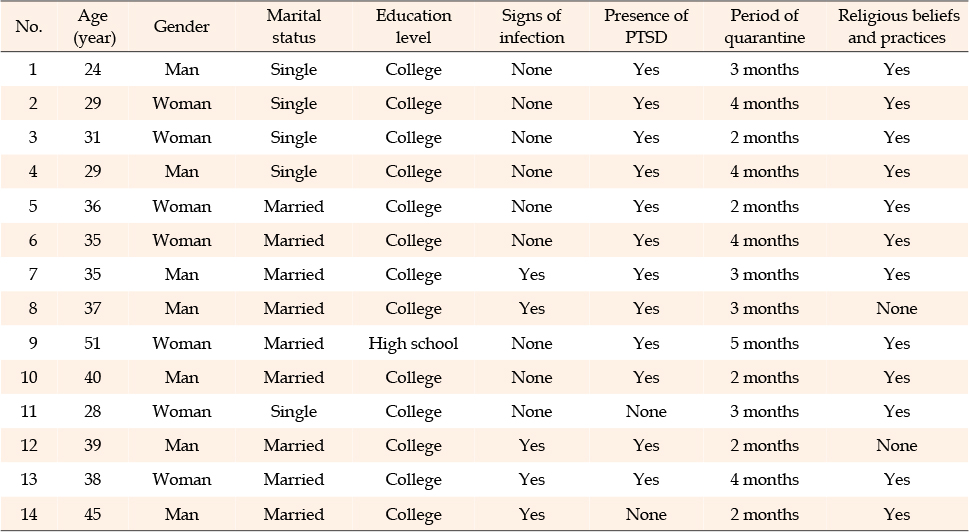
Table 1
General Characteristics of Participants (N=14)
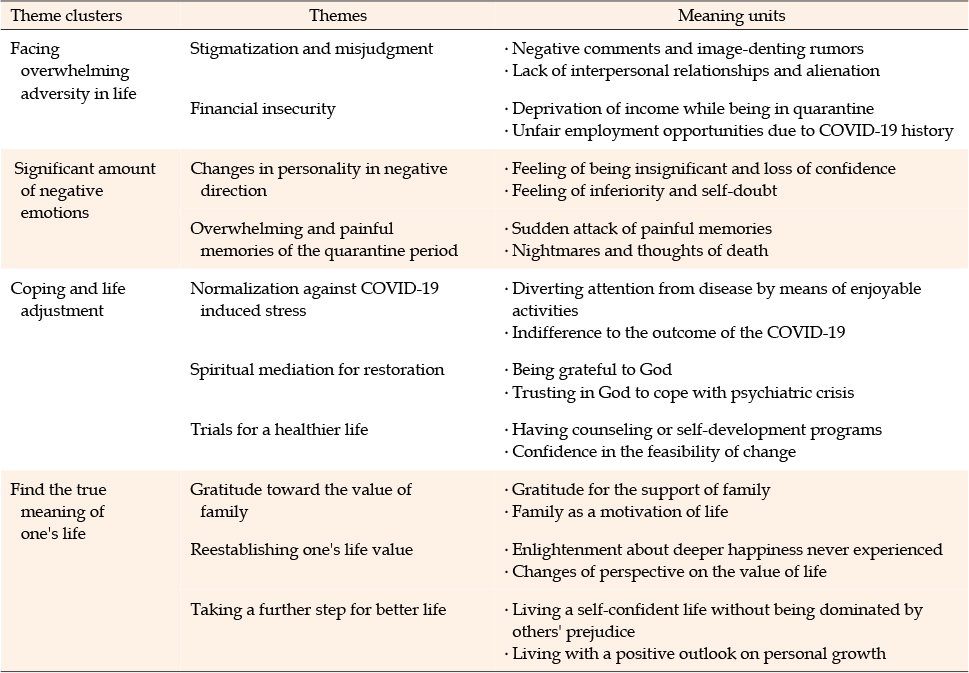
Table 2
Experiences of COVID-19 Patients in the Recovery Process
Participants reported experiencing stigmatization and misjudgment for having mental health consequences. They experienced being socially stigmatized for contracting COVID-19 and felt alienated from acquaintances after their release from quarantine.
People do not approach me because of the prejudice that COVID-19 is a scary and contagious disease that spreads quickly. (P8)
I met my middle school classmate after I was discharged from the hospital, and her attitude toward me has changed since she found out that I was infected with COVID-19. Therefore, I felt alienated by the people around me. (P3)
Participants suffered from insufficient income while under quarantine and were concerned about revealing their history of infection during job hunting. Participants, already stigmatized for COVID-19 infection, felt distressed due to being rejected at their new jobs, and to avoid further stigmatization, were hesitant to disclose their infection.
I’ve been quarantined for a long time, and I’m worried that I’ve not enough money to use after I’m released from quarantine. (P5)
I am looking for a new workplace, but I have been rejected by most companies. This is because I revealed that I was infected with COVID-19, and some people then thought of me negatively at my workplace. (P3)
Participants reported that they had undergone personality changes since they were stigmatized by social prejudice against people infected with COVID-19. Most participants said that they became introverted after their diagnosis. They felt insignificant and lost confidence. Some also experienced feelings of inferiority and self-doubt.
I was disappointed that there was no contact with my friends after being infected with COVID-19. Personality wise, I seem to have become more of an introvert as I spend more time alone. (P10)
I was mentally exhausted. I was discouraged and had lost confidence in living. It felt like I was insignificant. (P5)
Most participants confessed that they still recall being quarantined, and said it was difficult to talk about their experience in the quarantine facility which they were unable to escape from. For most participants, the memory of the quarantine facility evoked a severe fear.
The quarantine facility was located in the mountains and was completely isolated. I often had nightmares. Many bad thoughts occurred to me, and despair overcame me. To be honest with you, I wanted to die whenever the painful memories emerged. (P1)
Tears began to flow as I could do nothing but take medicine and get my blood pressure checked periodically in the isolation room. Whenever I faced a medical staff, I felt scared, and painful emotions emerged in the quarantine facility. (P7)
Participants shared that conditions normalized after getting through the disease by regulating their emotions while facing stressful events. Patients went through the disease period by carrying out a regular routine of appropriate practices and receiving psychological counseling to divert their attention away from their disease status or being indifferent to its outcome.
To control the negative emotions, I passed the time with jokes, making phone calls, and web browsing with a hands-free device deeming as if it was a normal day. (P2)
I tried to share my concerns with counselors or close friends to deliberately feel indifferent to stressful situations. (P1)
Most participants in this study had religious beliefs and practices. They confessed that trusting God was an alternative to relieve the stress caused by the disease crisis. Spiritual mediation allowed participants to reconfirm their identity and endure loss and disruption by strengthening their reasons for existence.
I was angry that I was infected with COVID-19. However, when I thought of the phrase "May God's grace be with you all" in the Bible, instead of thinking about my illness, I tried to focus on the good days I had planned for the future, and kept promising myself that hard times would not last long. (P2)
When I woke up in the morning, I thanked God for being alive, breathing, and being able to return home to meet my family and friends after quarantine release. (P12)
Through professional counseling and self-development, participants learned to cope with the after-effects of the disease by developing healthier habits or participating in self-development programs. Through professional counseling and healthy habits, participants had faith in themselves to defeat the disease and hoped for a positive future.
I became more interested in health, so I got into the habit of eating breakfast and eating organic food. Now, I exercise for an hour every day. I decided not to get infected again. (P13)
These days, I regularly take wellness programs and seek counseling to overcome hard times. I had counseling today. I believe these days will pass and become memories. (P9)
Participants received support from their families while recovering and preparing to return to their daily lives. They said that having family support was a significant motivation for successful recovery. They were able to overcome difficulties and rebuild their lives with the help of their families.
I appreciate the support of my family when I was infected with COVID-19. Living with my family is an important reason for my life. (P6)
While I was in the isolation room, my family comforted me and sent me a lot of packages containing things that I needed. I appreciate their dedication. (P3)
Participants were aware of the complexity and difficulty of returning to daily life after COVID-19 infection and were embracing changes in their lives. They reported valuing the moments of happiness that they previously overlooked. Despite the difficulties experienced by the patients, the disease was a catalyst for reassessing their life’s meaning.
Instead of thinking about my illness, I tried to focus on the good days before my illness and reminded myself that bad days would pass and become a memory. (P14)
I acknowledge that I was infected with COVID-19 once. Having COVID-19 does not mean that I am disabled, so it is important that I live my life with my own identity. (P4)
The participants gave themselves hope by coping with the disease with optimism, living with self-confidence without being dominated by others' prejudice, and trusting the good days they had planned for. They grew internally and attempted to overcome negative views and biases, allowing them to start their post-COVID-19 lives anew.
My dream is to save money and run my own store without relying on others. I will live my new life with gratitude every day. (P10)
I seem to have grown internally after the COVID-19 outbreak. Now, I can cope with difficulties without being dominated by negative societal biases and take another step toward a worthy life. (P13)
This study explored the lived experiences of recovering COVID-19 patients and provided basic data for developing a psychological intervention plan for COVID-19 validators by identifying the inherent meaning and nature of the lived experiences of recovering patients. We summarized our findings based on a cluster of themes.
Theme 1 concerns participants facing overwhelming adversity in life. Participants were psychologically burdened by negative social biases and were unable to accept that they were infected with COVID-19. In this regard, previous studies have shown widespread discrimination against people infected with COVID-19 [20, 22]. A possible explanation is that society holds negative views toward COVID-19 patients because the outbreak is a life-threatening situation. We also found that participants experienced alienation and financial losses due to unfair employment opportunities, which emphasizes the need to educate the general public to avoid spreading misinformation and misbeliefs about COVID-19. Doing so will play a crucial role in reducing COVID-19-related stigmatization. Moreover, subsidies are necessary to alleviate patients’ financial burden and restore them to society.
Theme 2 concerns the significant negative emotions associated with COVID-19. Most people isolated or quarantined during COVID-19 infection experience acute mental illness while recovering from a life-threatening experience [22]. In this study, participants experienced isolation while recovering from COVID-19 [23]. The loss of one’s usual routine and reduced social and physical contact with others were frequently shown to cause fear of the outside world, distressing the participants [24]. This study showed that most participants experienced fear and anxiety related to COVID-19 manifested through sudden attacks of painful memories and feelings of guilt [23, 24]. Thus, it is important that public health officials use a therapeutic communication approach because it is likely that psychological support could progressively decrease feelings of fear, worry, and suicidal impulses [25]. In this regard, a phone line or online service run by healthcare providers and specifically set up for those recovering from COVID-19 could provide information to help reassure patients, subsequently decreasing negative emotional states.
Theme 3 concerns coping and life adjustment. We found that participants sought to shift their focus away from the painful situation caused by the disease through positive thinking and normalization; participants tried to find alternative strategies for coping with adversity [25, 26]. According to the participants' experience, normalization was a their attempt to relieve stress from the disease through a regular routine of appropriate practices and a confidence-development program, which empowered them to have more control over their negative emotions. Spiritual mediation is known to play an intermediary role in facilitating psychological recovery in the event of stress [27]. In this study, we found that spirituality served as a medium for recovering participants by giving both religious and non-religious participants an opportunity to reaffirm their identity and relatedness. Most participants confessed that evangelism through a pastor, Bible study, and exercise helped them cope better with stressful life events. Therefore, it is necessary to strengthen spirituality by reinforcing relationships with significant acquaintances through self-reflection and outdoor activities.
Theme 4 concerns finding the true meaning of one’s life. Our study found that family members play an important role in supporting patients. Participants reflected on their own values and found positive power through family [27, 28]. Gratitude and support from family served as a driving force for participants to reconfirm their motivation in life by strengthening their reason for existence [27]. Thus, it is important for healthcare providers to encourage family support to help patients gain hope. Additionally, this study showed that COVID-19 patients seek to reestablish their own value by changing their perspective on the value of life. Changing perspectives help patients address harmful conditions and discover new pathways [28]. This study showed that participants grew internally and attempted to overcome negative social biases and find the true meaning of their lives. Positive outlook and self-confidence play important roles in reducing psychological trauma and enhancing personal growth [29]. This study revealed that finding happiness in what already exists but is hidden, significantly contributes to stress moderation and reconstruction of one’s life. These results demonstrate that it is important to find happiness in matters that have been overlooked to take a further step into a new life without being dominated by social prejudice.
This study has several limitations. First, owing to the pandemic regulations, we were unable to collect data from multiple centers; therefore, our findings may not be representative of all COVID-19 recovered cases. Exploration of the lived experiences of recovering COVID-19 patients who were quarantined at different centers is recommended for a more comprehensive understanding of the nature of patients who recovered from COVID-19. Finally, because this was a short-term study, the long-term experience of the research subjects is a promising avenue for future exploration.
The main contribution of this study is the exploration of participants’ vivid experiences as they recovered from COVID-19, which was conducted rigorously with the help of cooperative and interdisciplinary researchers. By describing the lived experiences of patients recovered from COVID-19, this study also offers a new direction to understand the psychological state of patients recovered from COVID-19 so that treatment can begin in a timely manner. Our results provide useful information for exploring psychological responses and presenting new directions for improving the handling of psychological resistance. Based on these findings, we recommend strengthening multidimensional support, providing adequate rationale, and facilitating patient support. Further, mental health professionals should be prepared to cope with the mental health-related consequences of patients in the post-COVID era.
Our research results provide a basis for understanding the psychological experiences of recovering COVID-19 patients and demonstrate that recovering COVID-19 patients experience physical, psychological, and social suffering, as well as lifestyle changes. We found that while negative emotions prevailed initially, coping strategies and psychological growth were important tools for recovering patients to maintain mental health after quarantine.
The holistic care model considers mental, environmental, and social factors comprehensively rather than just symptoms of an illness. Clinicians should apply the holistic care model to provide better healthcare by understanding the lived experience of recovering COVID-19 patients.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - KHS and PJW.
Data collection - PJW.
Analysis and interpretation of the data - KHS and PJW.
Drafting and critical revision of the manuscript - KHS and PJW.
 E-SUBMISSION
E-SUBMISSION